
Abstract
The field of early intervention in psychosis has grown quickly over the last 15 years. While these developments have important repercussions for the way psychoses are considered and treated, affective psychoses in general, and bipolar disorders in particular, have been neglected by this movement, despite the obvious need for early intervention treatment strategies [1]. However, before such interventions can be developed and implemented, much remains to be explored and certain basic concepts need clarification. In particular, while characterization of the bipolar spectrum of disorders has received extensive attention, much less has been achieved in the definition of the various phases leading from the onset of first symptoms to the full-blown disorder
As a first step, it might prove useful to apply the concepts of ‘prodrome’ and ‘onset’ to bipolar disorders; in a similar way they have been used for psychosis in general and schizophrenia in particular. The ‘prodrome’ can be defined as the period of disturbance, which represents a deviation from a person's previous experience and behaviour, prior to the development of the florid features of a disorder. The ‘onset’ on the other hand can be more difficult to define in bipolar spectrum disorders. For example, it might become clear only much later and retrospectively that an initial depressive episode was actually the first manifestation of a bipolar I disorder. As a first approach, it might prove useful to draw an analogy between first-episode (FE) mania and FE psychosis. The first psychotic episode must occur for the clinician to make the diagnosis of a psychotic disorder (and is absolutely necessary, for example, for schizophrenia to be diagnosed) and gives coherence to earlier manifestations of the illness once they can be put in the frame of the prodromal phase. Similarly, the first manic episode marks the diagnosis of a bipolar I disorder. What happens during the premanic phase—episodes of subthreshold or threshold depression, hypomania, or anxiety syndromes for example—could in such a concept be considered as the initial prodrome to bipolar I disorders and become a key target for early intervention. However, key challenges in the area are that, like in prodromal schizophrenia, potential early symptoms of bipolar disorder such as depression (which appears to be the most common initial presentation of bipolar disorders [2]) and anxiety are both widespread and of low specificity and that they are additionally more likely to follow an intermittent rather than a continuous pattern. In addition, mild mania, while specific, is ego syntonic, rarely distressing and consequently seldom reported. Moreover, such definitions have limitations, and are difficult to apply to other disorders of the bipolar spectrum, such as bipolar II disorders for example. They might nevertheless allow the exploration of the initial phase of the illness and be further refined and adapted at a second stage.
Importantly, it must be mentioned that ‘early intervention in bipolar disorders’, the focus of this paper, is different from ‘intervention in early-onset bipolar disorders’, a controversial subset of bipolar disorders with onset during childhood that may also justify specific treatment strategies but that will not be discussed in the present publication.
Current guidelines for treatment in the early phase of bipolar disorders
To our knowledge, none of the official guidelines for treatment of bipolar disorders make mention of specific strategies for the early phase of the illness. The following elements only can be gathered from the most recent version of the ‘Practice Guidelines for the treatment of patients with bipolar disorder’ published by the American Psychiatric Association [3]:
Mood stabilizers (lithium or valproate) should be used during the acute manic phase and continued for at least 6 months after a single manic episode, or 18 months in children and adolescents.
Antipsychotic medication should be used in association with mood stabilizers according to the severity of the episode and/or the presence of psychotic symptoms.
Need for ongoing antipsychotic treatment should be reassessed on entering maintenance treatment; antipsychotics should be discontinued unless they are required for control of persistent psychosis or prophylaxis against their recurrence. While maintenance therapy with atypical antipsychotics is sometimes considered, there is as yet no definitive evidence that their efficacy in maintenance treatment is comparable to that of agents such as lithium or valproate. This recommendation is likely to change given the recent publication of evidence that atypicals indeed do have maintenance efficacy: olanzapine has been shown to have comparable efficacy to lithium [4], and has been reported to be superior to placebo in prevention of mania, depression and overall relapse in randomized designs [5–7].
Some recent publications [8–11] have proposed guidelines for the treatment of FE psychosis, but some of the proposed strategies still need validation through randomized controlled trials.
Current pharmacological treatment of the early phase of bipolar disorders in naturalistic settings
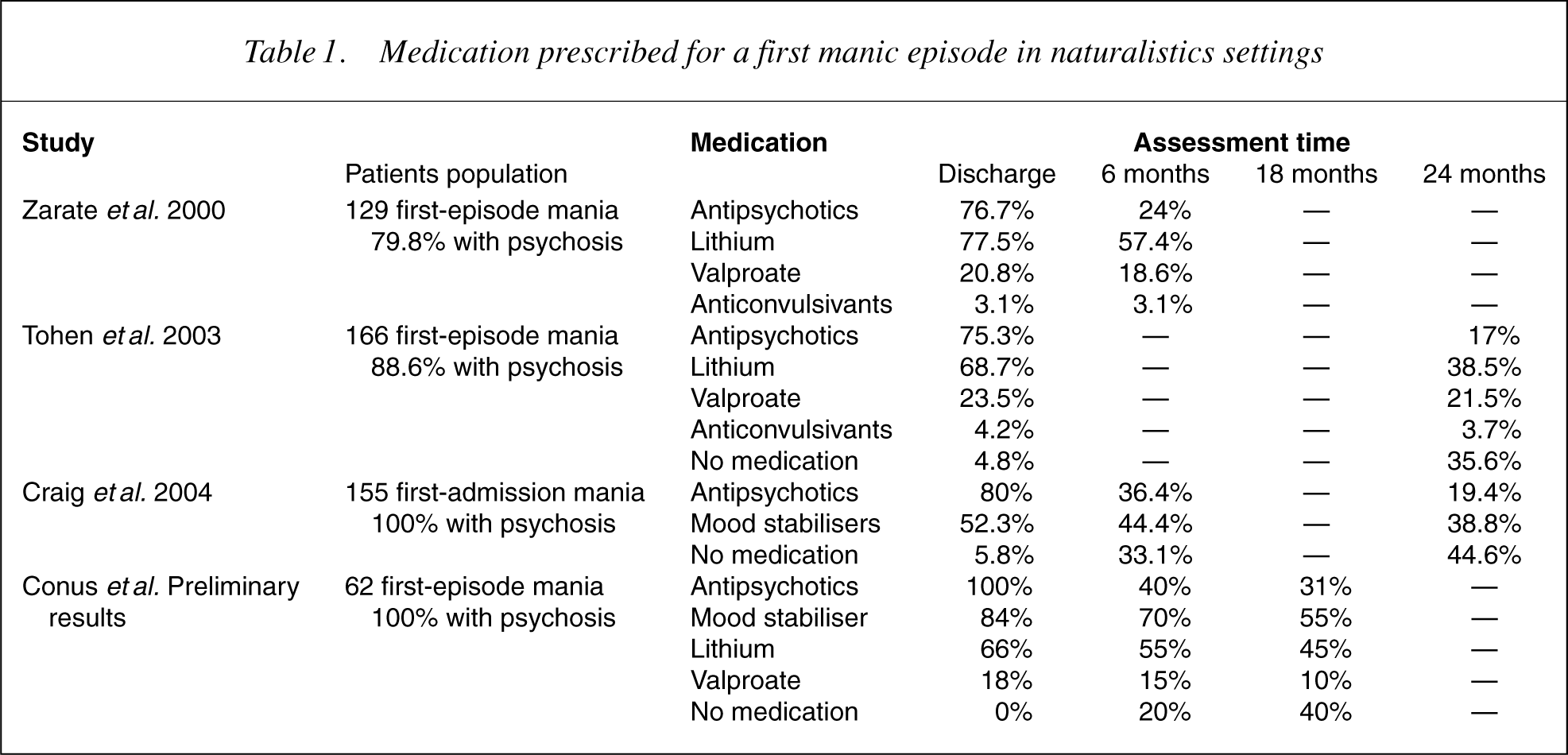
Various groups have explored treatment of the first manic episode in a naturalistic setting [12–14]. Results of these studies and preliminary data collected from the files of patients treated at EPPIC between 1998 and 2000 [15] are summarized in Table 1. Caution should be applied when comparing their results because of two reasons: (i) while all studies focus on FE mania, the proportion of patients presenting concurrent psychotic symptoms varies between cohorts, and (ii) authors provide different levels of detail about medication. Nevertheless, these results provide valuable information regarding current practice in the treatment of FE mania in a naturalistic setting and about the effect of various treatment strategies by evaluating their impact on outcome. The main conclusions that can be derived from these studies are the following:
Mood stabilizers are commonly not prescribed in patients with FE mania with psychotic features: this is illustrated in the Suffolk County cohort of Craig etal. [14], where only 53.3% of patients were prescribed a mood stabilizer at the time of discharge, despite the presence of clear manic symptoms in 84% at the time of admission. Treatment with mood stabilizers is often terminated very early: In the study by Craig etal. [14], only 44.4% of patients were still on mood stabilizers after 6 months. Antipsychotics are frequently prescribed during FE mania: These studies show that 75–100% of FE mania patients receive antipsychotic medication and still take them at the time of discharge. After 6 months, 25–40% are still receiving this medication and 15–17% after 24 months. While this might be in part related to a bias of the sample toward psychotic mania, Zarate and Tohen [12] found no differences in terms of antipsychotic exposure whether or not patients presented psychotic features. Similarly, Samellas etal. [16] have recently shown that the best predictor of antipsychotic prescription at discharge after a manic episode was prescription of antipsychotic medication early in the episode rather than intensity of symptoms or aggressive behaviour. Similarly to what has been observed in more established illness, adherence to treatment is rather poor after a first manic episode. For example, Craig etal. [14] found that 43% of patients at 6 months and 58.7% at 24 months were using mood-stabilizing medication less that 25% of the time.
Medication prescribed for a first manic episode in naturalistics settings
Critical issues in the approach of pharmacological treatment of the early phase of bipolar disorders
On the basis of these observations, three critical issues deserve attention in the current pharmacological approach of the early phase of bipolar disorders: (i) failure to prescribe mood stabilizers in the early phase of bipolar disorders, (ii) use of antipsychotic medication and (3) non-adherence to treatment. They will be discussed briefly below.
Failure to prescribe mood stabilisers in the early phase of bipolar disorders
Various studies converge to show that there is on average a very long delay between the onset of a bipolar disorder and the introduction of a mood-stabilizing medication [17–19]. For example, Post etal. [19] report an ‘average of 10 years between first symptoms meeting diagnostic threshold and first treatment’ (p 317), and Baethge etal. [18] found an average mean latency of 9.3 years between first medical contact for the mood disorder and start of treatment with mood stabilizer.
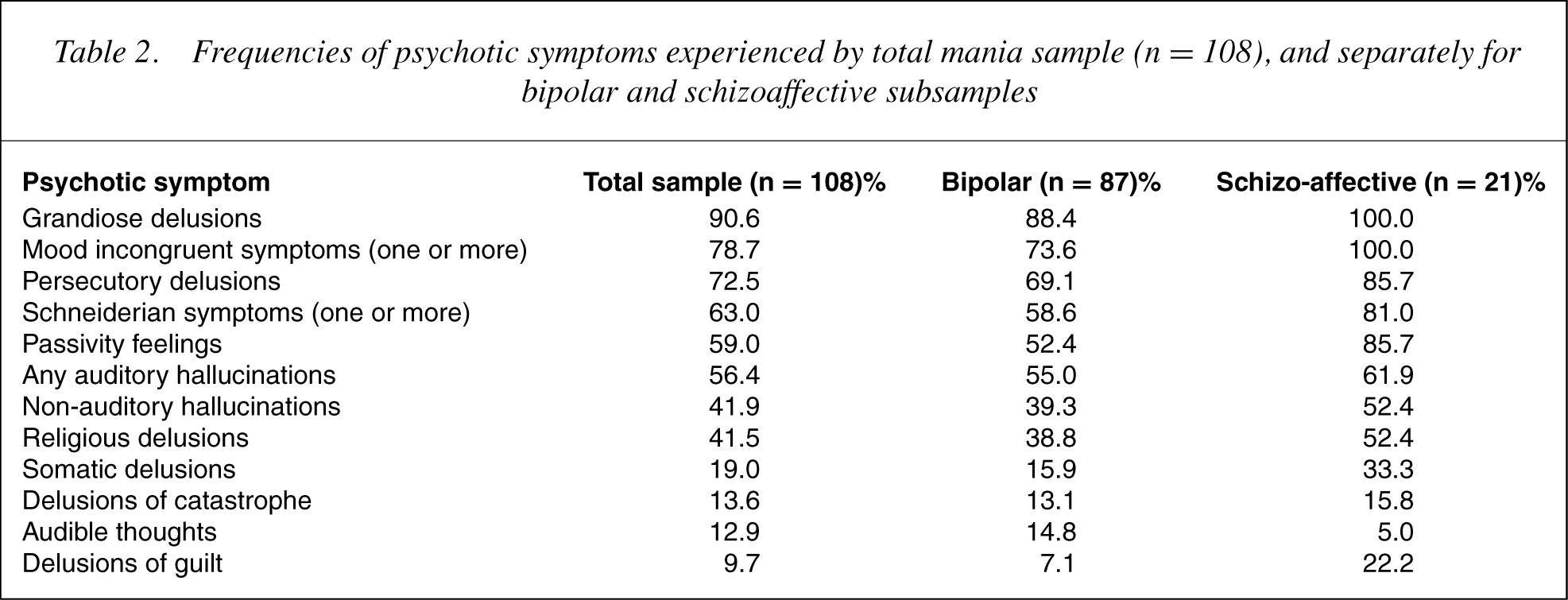
This latency is partly due to the fact that index episode of illness is typically depressive, and as a consequence, the most common initial diagnosis is of unipolar depression [20]. Another major reason for such a latency is the failure to identify mania in young patients, which can be explained by various factors. First, clinical presentation of mania is frequently atypical in adolescents and young adults, with high rates of mixed episodes, as evidenced by irritability, increase in energy and flight of ideas rather than euphoria and grandiosity [21, 22]. Mild mania is uncommonly a source of distress and therefore seldom a focus of clinical attention. Disruptive behaviour in mania can overlap phenomenologically with personality disorders. There is also a higher rate of comorbidity and overlap with manifestations of other disorders, such as ADHD, anxiety, substance use disorder and antisocial behaviour [22]. Finally, younger patients present with a higher rate of psychotic symptoms [23], more often of a mood-incongruent nature [24]. In a sample of 108 FE psychotic mania patients treated at EPPIC between 1987 and 1995, Conus etal. [25] found high rates of moodincongruent psychotic symptoms, persecutory delusions and Schneiderian symptoms, not only in those with a diagnosis of schizoaffective disorder, but also in those with a diagnosis of bipolar disorder (see Table 2). Such an atypical presentation leads to high rates of misdiagnosis, most often with schizophrenia, but also with conduct disorders, ADHD, antisocial or borderline personality disorder.
Frequencies of psychotic symptoms experienced by total mania sample (n = 108), and separately for bipolar and schizoaffective subsamples
Consequences of delayed introduction of mood stabilizers are numerous. First, there is still a controversy regarding potential reduction of the effect of lithium, with increasing delay between onset of the disorder and start of the medication. Some authors have found a reduced response [19], while others [18, 26] did not. Whatever the case may be, most authors agree that delay in treatment is linked with poorer social adjustment, higher number of hospitalizations [27], increased risk of suicide, development of comorbidities, forensic complications and global impairment of the capacity to face developmental tasks [1]. In addition, Post's neurosensitization model suggests that an increased number of relapses poduces not only acute modifications, but also more permanent alterations in the neuronal activity possibly transduced at the level of gene expression, alterations that in turn might induce a higher tendency to relapse, and maybe a poorer response to medication [28]. Misdiagnosis may also lead to inadequate psycho-education, rejecting attitude, for example, in the case of a diagnosis of antisocial personality disorder, and inappropriate medication regimens, which in turn may have a negative effect on outcome. Untreated illness may interfere with the attainment of age-specific social, psychological and educational developmental goals [29]. Finally, the notion that mood stabilizers have a primary neuro-protective function is gaining currency [30]. There is ample neuro-imaging data regarding structural changes in bipolar disorder [31], and recent data suggest that atypical agents prevent structural changes in FE psychosis [32]. There is similarly data suggesting that lithium and valproate can prevent tissue loss in the amygdala in paediatric bipolar disorders [33]. Such a conceptualization of the occurrence of a reversible process in the early phase of bipolar disorders is another element supporting the need for early intervention.
Use of antipsychotic medication in the early phase of bipolar disorders
According to the APA guidelines, antipsychotic medication should be used only during acute manic phases with psychotic features or in particularly sever manic or mixed episodes, in combination with lithium or valproate [3]. Despite the availability of various mood-stabilizing agents and their proven efficacy in acute and maintenance phases, and despite the availability of benzodiazepines to help control agitation in the acute phase, antipsychotics remain the most commonly prescribed adjunctive treatment for mania [1]. In their study, Zarate and Tohen [12] found that, while usually receiving lower doses, patients with FE mania were as likely as FE non-affective psychosis patients to receive antipsychotics. Moreover, they found that while 77% of them received antipsychotic medication at discharge, 25% still received it at 6-months' follow-up. In chronic populations, 6 months after hospitalization for a manic episode, 68–95% of patients who have been prescribed antipsychotics still receive it, and proportions of up to 67% have been observed during the maintenance phase.
This is a matter of concern for various reasons. First, bipolar patients have a high susceptibility to tardive dyskinesia with typical antipsychotics [34]. Moreover, if antipsychotics rather than benzodiazepines are used for acute behavioural control, they tend to be prescribed at high dosages that can induce extra-pyramidal syndromes and lead to prolonged alienation of patients from treatment. In addition, Craig etal. [14] found that patients who were prescribed typical antipsychotic medication ended up with poorer GAF score (Global Assessment of Functioning [35]) at outcome and less time in remission. Zarate and Tohen [12] also found a detrimental effect to maintenance of such medication after remission of mania (increased risk of side effects, dysphoria, depressive symptoms, shorter time to depressive relapse). Atypical antipsychotic constitute a promising alternative to typical neuroleptics for use in acute bipolar mania [36] while their use as mood stabilizers deserves more extensive research to support it [37]. However, despite to a lesser extent, individual atypical antipsychotic still have side effects such as somnolence, hyperprolactinemia, osteoporosis, dyslipidaemia, weight gain and diabetes and even extra-pyramidal side effects.
Non-adherence to medication
Non-adherence to medication is known to be an important problem in any medical or psychiatric condition and has been identified as one of the major risk factors for relapse in bipolar disorders. Basco and Rush [38] showed that the rate of non-adherence to mood stabilizers was close to 50%. Keck etal. [39] showed in a cohort of 101 patients hospitalized for acute mania that 64% of them were non-adherent to their medication in the month prior to admission. They also found that medication adherence was associated with higher rates and more rapid recovery [40].
In FE patients, the rate of non-adherence seems to be even higher, reported by some authors to be as high as 57% [41]. Among the 83 bipolar of a cohort of 109 FE affective patients, Strakowski etal. [42] reported that 41% were fully adherent, 26% partially and 33% totally nonadherent. Craig etal. [14] found that, at 6 months, 43% of patients were non-adherent to mood stabilizers. These numbers might be explained by various factors. First of all, denial is an associated feature of the illness. It is common for individuals to have a number of episodes before accepting the implications of the recurrent nature of the illness, and its implications. Furthermore, lifestyle change involved in prophylactic medication represents a major challenge, especially for young people. This underlines the need to develop specific psychosocial interventions aimed at the specific needs of this group of individuals [43].
The impact of non-adherence on the outcome of FE mania has not been well studied. Strakowski etal. [42] found that syndromal recovery was more likely to occur for patients with full adherence than for those with partial adherence. The impact of total non-adherence is more difficult to assess, non-adherent patients tending to drop out of the studies altogether. Moreover, non-adherence rarely occurs in isolation and is often combined with other poor prognostic factors such as substance abuse, and might then have an indirect as well as a direct effect on outcome. It is however possible that adherence may be a marker of other behaviours or illness characteristics modulating outcome.
Where do we go from here?
In summary, the pharmacological treatment of the early phase of bipolar disorders currently lacks specific guidelines, and most published guidelines do not really differentiate treatment strategies early in the course from those recommended for later stages. The important issues identified above regarding identification of the disorder, delayed prescription and unclear ideal duration of mood stabilizer treatment, high use of antipsychotic medication, and finally poor adherence to treatment, underline an urgent need for research and development in early intervention in bipolar disorders. In our opinion, various strategies could be applied to address these critical issues within the broader framework of early intervention strategies in psychiatry, and they will be discussed below.
Earlier identification of bipolar disorders
Earlier identification of the disorder would allow pharmacological treatment to be commenced sooner, with the potential to reduce the collateral damage caused by prolonged duration of untreated illness, and the introduction of medication during a phase where it may be more efficacious. Three strategies might have an impact on delayed identification of bipolar disorders:
a)
b)
c)
Development of specific guidelines for treatment
As Malla and Norman [56] pointed out, there is however more to early intervention than intervening early. Early case identification needs to go hand in hand with phasespecific treatment procedures in order to really improve outcome [57]. Pharmacological treatment of the early phase of bipolar disorders therefore needs to be studied in order to allow the development of phase-specific guidelines. Among other ideas, it would be useful to compare efficacy and effectiveness of mood stabilizers in FE mania as well as to define the ideal duration of prophylaxis after a first manic episode. Regarding antipsychotic treatment, studies are needed to (i) define the need for and the optimal duration of antipsychotic treatment both in psychotic and non-psychotic mania, (ii) compare typical and atypical antipsychotics in terms of safety as well as efficacy and (iii) compare the efficacy and effectiveness of various atypicals both in the acute and maintenance phase. Regarding this last issue, a file audit study recently conducted at the EPPIC that explored response to treatment in a non-randomized non-controlled naturalistic setting revealed that olanzapine had a higher efficacy than risperidone in FE affective (mainly manic) psychoses: lower Clinical Global Impression score [58] at the end of the trial, higher rate of global improvement on CGI scale and higher rate of remission of positive symptoms [59].
In addition, the development of methods to identify the prodrome for bipolar disorders would pave the way to explore possible biological mechanisms underlying the emergence and development of the disorder and evaluate potential preventive strategies such as neuroprotective agents, psychosocial interventions and primary prevention of secondary substance use disorder [46].
Psychological impact of a first manic episode
Finally, it must be emphasized the treatment of the early phase of bipolar disorders is much more than medication. Recent findings from our group have confirmed, in a cohort of 87 FE bipolar mania patients that, despite a generally good symdromic recovery, 41% failed to reach symptomatic remission after 12 months, and that only 39% returned to their premorbid level of functioning [60]. Patients who remained symptomatic suffered mainly from anxiety, presented symptoms of social phobia and important restriction of social interactions. In addition, as mentioned above, an important proportion of patients abused illicit substances and failed to adhere to medication. Therefore, there is an important need for the development of psychological and psychosocial interventions that would address the specific needs of young patients, through adapted psycho-education approaches and psychological interventions that would focus on engagement, development of insight, adherence to treatment, substance abuse comorbidity, anxiety, social phobia, selfesteem, vocational recovery strategies, and that would take into account the effect of illness on age-appropriate developmental tasks [43].
Conclusion
Currently, pharmacological treatment of the early phase of bipolar disorders is not really different from the treatment proposed for patients who have had many episodes of illness. A number of issues that deserve attention can be identified. Clinical research in these domains would allow the clarification of fundamental concepts and create the conditions for the development of treatments that would be tailored to stage of illness and the specific needs of patients; this could well have a positive impact on the evolution and outcome of the disorder. This kind of approach is long overdue.
Footnotes
Acknowledgements
Part of this work has been presented at the ‘Second National Working Meeting of Mental Illness: The Bipolar Spectrum Disorders’ organized by Professor José Luis Vázquez-Barquero in Santander, Spain, 25–27 November 2004.