
Abstract
Objective
This exploratory correlational study explored the demographic, clinical, and offence-type characteristics of people with documented past-year contact with the criminal justice system (CJS) in Toronto, Canada who died by suicide. We aimed to compare demographic and clinical factors among individuals with CJS contact who died by suicide to those without recorded CJS contact who died by suicide.
Methods
Coroners’ final death reports from all recorded suicide deaths in Toronto between 1 January 1998 and 31 December 2020 were retrieved by research staff and coded at the Office of the Chief Coroner (OCC) of Ontario. A series of bivariate analyses and binary logistic regression analyses were performed to compare demographic and clinically relevant characteristics between these groups. Descriptive statistics relating to demographic, clinical, and offence-type characteristics were reported.
Results
A total of 5,288 people died by suicide, of whom 251 (4.7% of all suicides) had recorded CJS contact prior to death. Assault, physical assault, impaired driving, serious/death threats, and sexual assault were the most common criminal charges among those in the CJS contact group. When compared with the no recorded CJS contact group, the CJS contact group was slightly younger (M = 40.0, SD = ±13.4 vs. M = 47.5, SD = ±18.1, p < 0.001), had a higher proportion of males (85.6% vs. 69.9%, p < 0.001), more commonly experienced interpersonal (36.3% vs. 14.5%, p < 0.001) and/or relationship break-up/breakdown stressors (16.7% vs. 7.5%, p < 0.001), and substance misuse or substance use disorders (37.5% vs. 18%, p < 0.001).
Conclusions
Our findings highlight that younger men with interpersonal stressors and/or substance misuse characterize suicide decedents with recorded CJS contact in Toronto, Canada. Suicide prevention efforts and strategies should consider the profile differences among those navigating the CJS.
Plain Language Summary Title
Criminal Justice System Contacts among Suicide Decedents in Toronto
Plain Language Summary
Why was the study done? Having contact with the Criminal Justice System (e.g., police encounter, being charged with a criminal offense, imprisonment) can be a stressful experience that may impact an individual's mental health, including the risk of suicidal ideation, self-harm, and suicide death. There is little research in Canada exploring the impact of Criminal Justice System contact on those who have died by suicide. What did the researchers do? This study examines a sample of 5,288 suicide deaths in Toronto, Canada between 1998 to 2020 according to contact with Criminal Justice System. We compared groups with and without contact according to variables of interest such as sex, age, marital status, and living circumstances, life stressors, mental health history, and suicide method. What did the researchers find? We found that approximately 5% of suicide deaths had a known recent contact with the Criminal Justice System as a significant stressor. Those with contact were more likely to be young, males, with interpersonal conflict and/or relationship breakup stressors, and substance misuse/use disorders. Violent criminal offences (e.g., assault or sexual assault) were most commonly reported. What do the findings mean? This study identifies the profile of those with Criminal Justice System contact who die by suicide including demographic and legal offence factors. These results should inform future suicide prevention efforts in the Criminal Justice system.
Introduction
Suicide is a major public health problem in Canada. 1 It is the 13th leading cause of death (suicide rate of 9.2 per 100,000 individuals) with more than 3,500 people dying by suicide annually. 2 There are more than 1,100 suicides per year in Ontario, Canada's largest province, with a suicide rate of 7.52 per 100,000 individuals. 2 Contact with the criminal justice system (CJS) is a stressful life event that often carries a social stigma. 3 Research on mental health and the CJS shows that having contact with the system may negatively impact mental wellbeing and further exacerbate underlying mental illnesses;4-6 it is important to acknowledge that being convicted of a criminal offence is itself, also a stressful life event. Feeling separate from others, psychological pain, and feeling trapped are all thought to influence suicide outcomes7-9 and these reactions may all occur in response to CJS contact.
Suicide and the Criminal Justice System
Existing literature has primarily focused on the role of imprisonment on risk of suicide, related outcomes such as self-harm, and prevention.10-14 Studies globally have estimated that suicide deaths are 3-fold higher among incarcerated males than in the general population. 10 Factors such as psychiatric history, previous suicide attempts, and suicidal ideation during imprisonment are associated with increased suicide risk.10,13 The rate of prison suicide in Canada (in both provincial and federal custody) is elevated compared to the general Canadian population.10,15 A study examining lived experiences of suicide attempts during imprisonment demonstrated that factors such as the inadequacy of suicide risk assessments, the dehumanization of people inside jails and prisons, and lack of human connection or interactions while incarcerated, among others, influenced the suicide decision-making process in custody. 12 Suicide is also the second leading cause of death (after accidents) in the period post-release from custody. 16
Some studies have explored the association between more general CJS involvement and mental health. Results from a Danish population study identified that having any type of CJS history could increase suicide risk up to 2-fold for men and more than 3-fold for women, 17 and, in a US self-report population study, the suicide attempt risk was higher among those with recent arrest (RR = 1.80). 18 A study in the Canadian province of Manitoba, found the presence of a mental disorder in 39% of those accused of a crime reported compared to 26% in the general population. Several studies have examined the impact of police encounters on mental health,12,19,20 including 1 suggesting that the risk of suicide attempt increased after experiencing police violence and use of force, regardless of the race or ethnicity of the person involved. 21 People with current CJS involvement (i.e., either facing legal charges or currently on probation/parole) were more likely to present with a lifetime suicide ideation history if they also reported high thwarted belongingness, a key risk factor for suicide in the general population.22-23 Finally, there is limited specific literature exploring general CJS involvement and suicide death.24-30 US data identified being involved in multiple legal cases and court types, domestic-related violence charges, sexual-based offences, and driving offences as significant predictors of suicide death. 24 In fact, it was found that interpersonal violence perpetrators accounted for 6% of suicide deaths in North Carolina and that these suicides tended to occur in men with alcohol-related problems. 24
There remains a gap in the literature on the role of CJS involvement in suicide deaths both internationally and in the Canadian context. As described above, much literature focuses on incarcerated populations, such as in jails, prisons, or juvenile correctional facilities. Demographic characteristics and additional risk factors for suicide remain largely unknown among those who have had contact with other aspects of the CJS, such as probation or court contacts and on bail. In this exploratory correlational study, we aimed to address that gap by identifying common criminal offences and the demographic and clinical characteristics of suicide decedents with CJS involvement in Toronto, Canada.
Methods
Data Retrieval
This exploratory correlational study used data from an ongoing study of coroner records in Toronto, Canada. 31 Trained research assistants, who hold Bachelor degrees (either BA or BSc), reviewed a total of 5,288 chart records of confirmed suicide deaths between 1 January 1998, to 31 December 2020 at the Office of the Chief Coroner (OCC) of Ontario. Data collection has spanned 2 decades with periodic measures of interrater reliability between successive coders to ensure good agreement.
Our database included the following variables: demographic information (age, sex, marital status, and living circumstances), life stressors (employment, financial and/or academic, relationship, interpersonal conflict, bereavement, recent medical/health, criminal justice, and immigration), known prior suicide attempt(s), history of self-harm, mental health history and details of the suicide method. Information in OCC charts were obtained from multiple sources, such as medical reports (e.g., last discharge summary, if available); interviews with next of kin, friends and family members; and police records (sometimes outlining previous criminal charges) if available. We examined all available data sources to identify evidence of CJS involvement. Note that our findings must be interpreted with a note of caution given potential missing data regarding CJS involvement in some cases, particularly if the involvement was very limited and/or in social isolated decedents without an involved next of kin.
Sample
Our initial data visualization and project conceptualization process is outlined in the supplementary document. We derived 2 mutually exclusive comparison groups from our sample: (1) CJS contact (CJS group) or (2) no CJS contact (n-CJS group). Cases included in the CJS group had to have at least 1 of the following criminal justice contacts in the 12-month period prior to death: evidence of being arrested and/or criminally charged, released on probation or on parole, subject to a current criminal court proceeding or with a court appearance imminent, having a warrant issued and/or wanted for a crime, criminally convicted and/or incarcerated, and evidence of a police encounter and/or mention that a charge may be pending. Individuals subject to civil (i.e., non-criminal) claims or where potential CJS involvement was ambiguous (e.g., “legal difficulties”) were excluded from the main analyses. We finally included all sample cases for post-hoc analysis as we were interested in exploring suicide death counts in relation to all legal stressors (i.e., both criminal and non-criminal).
For those in the CJS group, we also collected the types of offence(s) for which they were engaged in the system (i.e., offence charged and/or for which a conviction occurred). Offences are listed in the supplementary documents.
Statistical Analysis
Descriptive statistics for offences, demographic factors, and clinical-related information were reported. Bivariate analyses were performed using t-tests, 1-way ANOVA for continuous variables, and chi-square tests for categorical variables, respectively. Those variables that were significant in bivariate analyses were then input into binary logistic regression tests to identify independent associations with CJS involvement. For the suicide method analysis, if more than 1 suicide method was identified, then both methods were included in the analysis. A joinpoint regression analysis was also performed to identify trends over time. Toronto's population census data was collected through the Statistics Canada website to determine suicide rates per 100,000 individuals. These included census data from 1996, 2001, 2006, 2016, and 2021.32-34 The significance level was set at p < 0.05, and odds ratios (ORs) and 95% confidence intervals (CIs) were reported. A series of post hoc tests were performed including (1) a 2-control:1-exposure sensitivity analysis to identify specific group differences when controlling for demographic variables such as age, sex, marital status, and living circumstance; (2) a comparison according to the number of offences identified (i.e., 1 offence vs. multiple offences vs. unknown number offences vs. no offences) to identify potential differences according to offence count; and (3) a comparison according to whether the offence was violent (i.e., violent offence vs. non-violent offence vs. unknown violence level of offence vs. no offence) to identify potential differences based on the nature of an offence. We refer to violent offence(s) as any criminal charge that involves direct harm or threatening violence against a person (e.g., assault, sexual assault, murder). 35 If an individual had been charged with, or convicted of, committing any violent offence, they were assigned to the violent offence group regardless of whether they had also been charged with or convicted of a non-violent offence. Fisher's exact test was used throughout post-hoc analyses for cases with cell counts less than 5. All statistical analyses were performed using R-Studio Software version 4.3.3 (R Core Team, 2024), except joinpoint regression analysis which was performed using Joinpoint Regression Program Software version 5.2.0 (National Cancer Institute).
Results
Overall Comparison
Of 5,288 total suicide deaths recorded, 251 suicide deaths (4.7%) were identified as having prior CJS contact. The 5 most common legal offences perpetrated by decedents were assault (unspecified) (12.8%), physical assault (12.4%), impaired driving (12.0%), serious/death threats (9.2%), and sexual assault (6.8%) (see Table 1).
Frequencies of Offence for People Who Died by Suicide and Had Contact with the CJS in Toronto from 1998 to 2020 (N = 251).
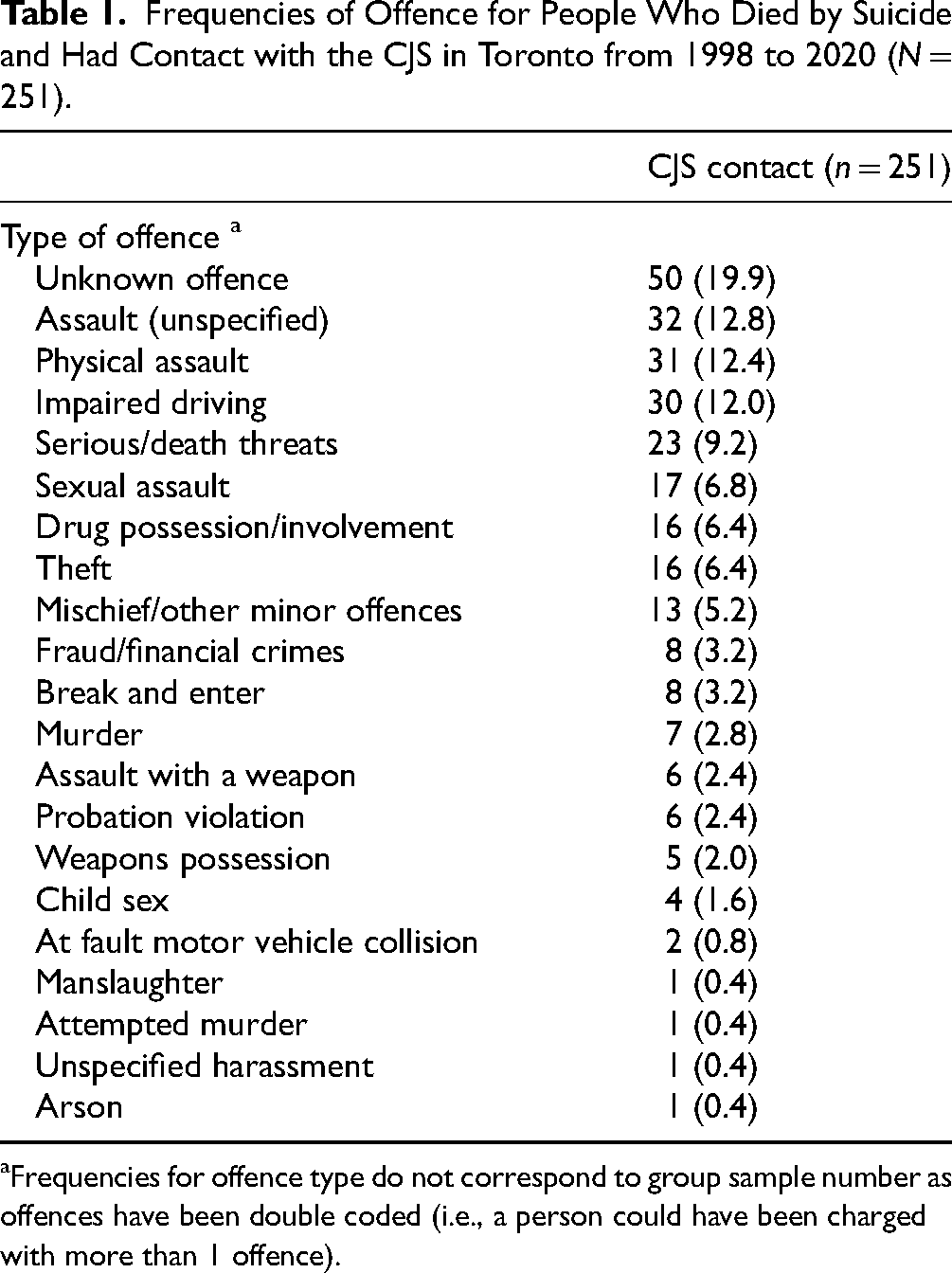
Frequencies for offence type do not correspond to group sample number as offences have been double coded (i.e., a person could have been charged with more than 1 offence).
Demographic Characteristics
Table 2 presents the demographic and clinical differences between the CJS and n-CJS groups. In comparison to the n-CJS group, decedents in the CJS group were younger (M ± SD = 40 ± 13.4 vs 47.5 ± 18.1, t(5248) = −6.5146, p < 0.001), more likely to be male (85.6% vs 69.2%; OR = 2.65, 95% CI = 1.88–3.85), more likely to have interpersonal conflict (36.3% vs 14.5%; OR = 3.37, 95% CI = 2.56–4.39), relationship breakup (16.7% vs 7.5%; OR = 2.47, 95% CI = 1.72–3.46), history of substance misuse/use disorders (37.5% vs 18.0%; OR = 2.73, 95% CI = 2.09–3.55), and to die by hanging (39.0% vs 32.2%; OR = 1.35, 95% CI = 1.03–1.74). Decedents in the CJS group were less likely to have depression (40.6% vs 51.4%; OR = 0.65, 95% CI = 0.50–0.84), medical stressors (2.4% vs 12.0%; OR = 0.18, 95% CI = 0.07–0.38), and were less likely to die by self-poisoning (12.4% vs 17.3%; OR = 0.68, 95% CI = 0.45–0.98).
Demographic and Clinical Data for People with or without Contact with the CJS in Toronto from 1998 to 2020 (N = 5251).
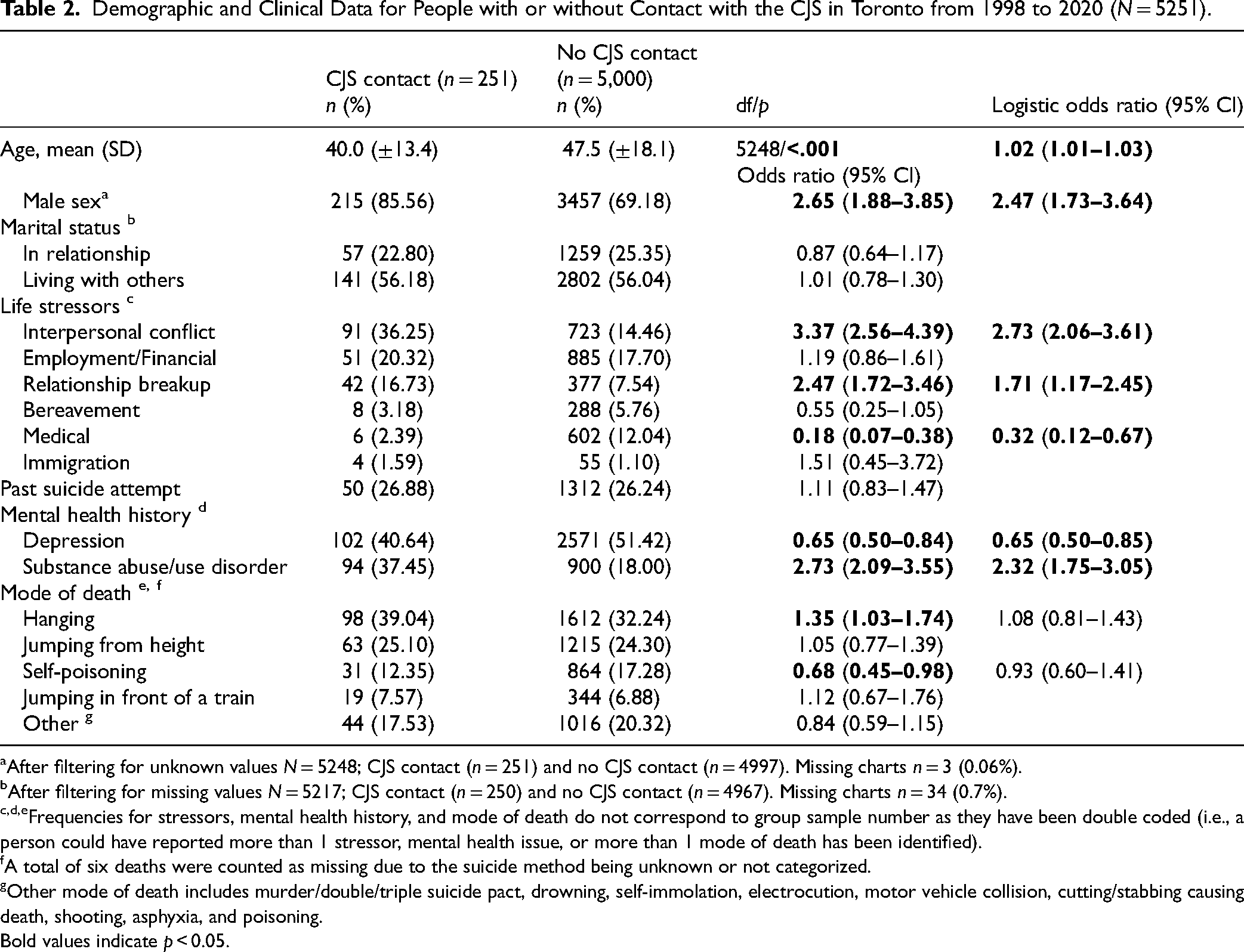
After filtering for unknown values N = 5248; CJS contact (n = 251) and no CJS contact (n = 4997). Missing charts n = 3 (0.06%).
After filtering for missing values N = 5217; CJS contact (n = 250) and no CJS contact (n = 4967). Missing charts n = 34 (0.7%).
Frequencies for stressors, mental health history, and mode of death do not correspond to group sample number as they have been double coded (i.e., a person could have reported more than 1 stressor, mental health issue, or more than 1 mode of death has been identified).
A total of six deaths were counted as missing due to the suicide method being unknown or not categorized.
Other mode of death includes murder/double/triple suicide pact, drowning, self-immolation, electrocution, motor vehicle collision, cutting/stabbing causing death, shooting, asphyxia, and poisoning.
Bold values indicate p < 0.05.
Binary Logistic Regression
We included 8 significant variables from our bivariate analyses in our model. The collinearity assumption was not violated for the model, with variance inflation factor (VIF) less than 5 for all variables. The binary logistic regression analysis confirmed that when controlling for other variables and compared to people with n-CJS contact, those who had CJS contact and died by suicide were more likely to be younger (age: M = 40.0, SD = ±13.4 vs M = 47.5, SD = ±18.1; OR = 1.02, 95% CI = 1.01–1.03), male (OR = 2.47, 95% CI = 1.73–3.64), with interpersonal conflict (OR = 2.73, 95% CI = 2.06–3.61) and/or relationship breakup stressors (OR = 1.71, 95% CI = 1.17–2.45), and substance abuse/use disorders (OR = 2.32, 95% CI = 1.75–3.05). In contrast, they were less likely to be depressed (OR = 0.65, 95% CI = 0.50−0.85) or report medical stressors (OR = 0.32, 95% CI = 0.12−0.67).
Joinpoint Analysis Results
Suicide time trends of cases that reported CJS contact in Toronto between 1998 and 2020 are illustrated in Figure 1. Table 3 shows joinpoint regression analysis results for both type of analysis. A 2-joinpoint model was selected based on the proportion of cases with CJS contact and showed a significant decreasing trend from 2015 to 2017 (APC = −42.61, 95% CI = −54.33, −18.43), and a later significant trend increase from 2017 to 2020 (APC = 48.25, 95% CI = 7.56, 174.70). When analyzing rates per 100,000, a zero-joint point model was selected with a significant decreasing trend from 1998 to 2020 (APC = 3.92, 95% CI = −6.50, −1.76)). Additional counts and proportions for suicide deaths following CJS were added (see supplementary document, Figure 1).
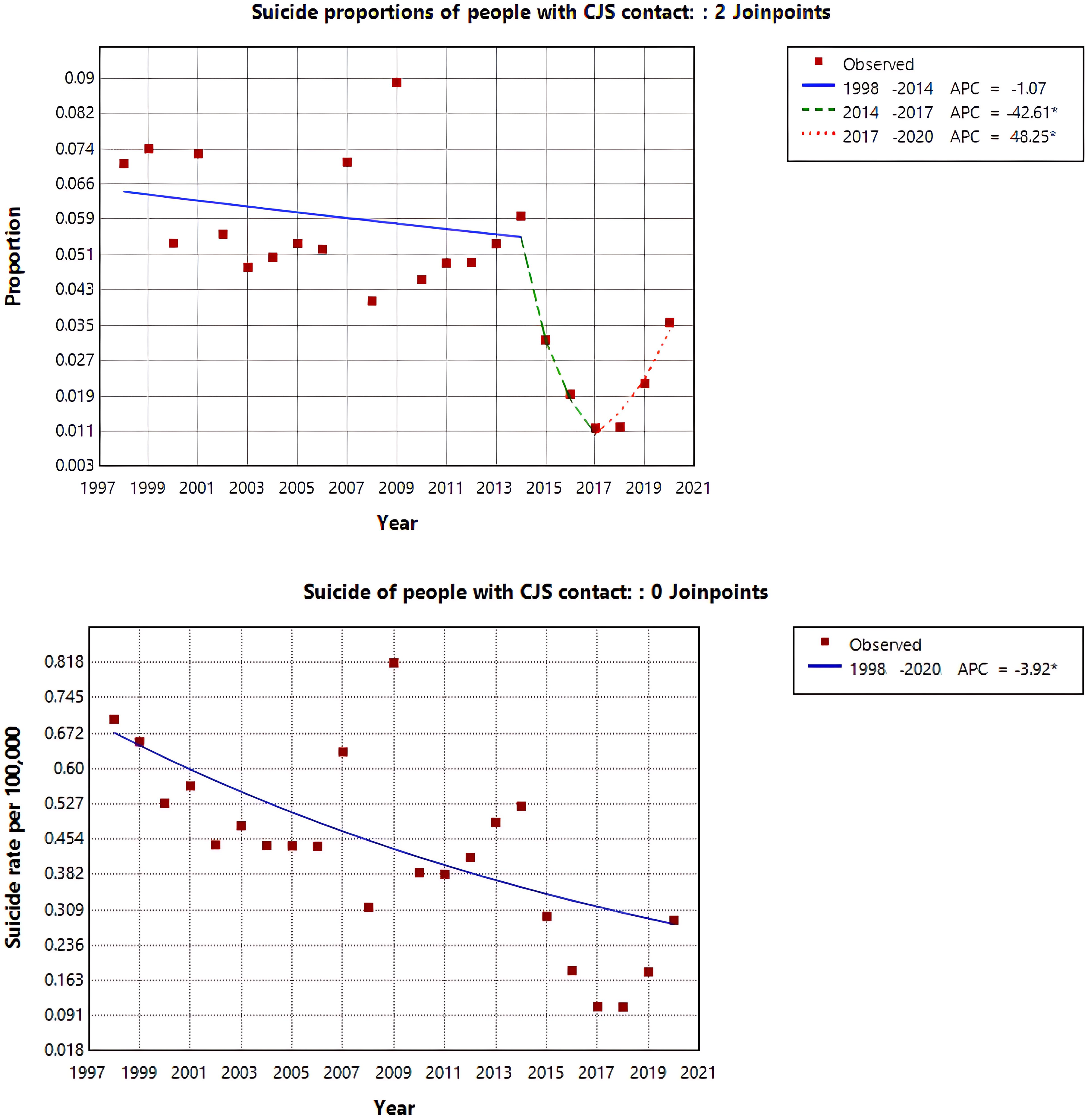
Joinpoint trend analysis of both proportions and suicide rates (per 100,000 population) for people with CJS contact in Toronto from 1998 to 2020.
Joinpoint Regression Analysis of Both Proportions and Suicide Rates (per 100,000 Population) for People with CJS Contact in Toronto from 1998 to 2020.
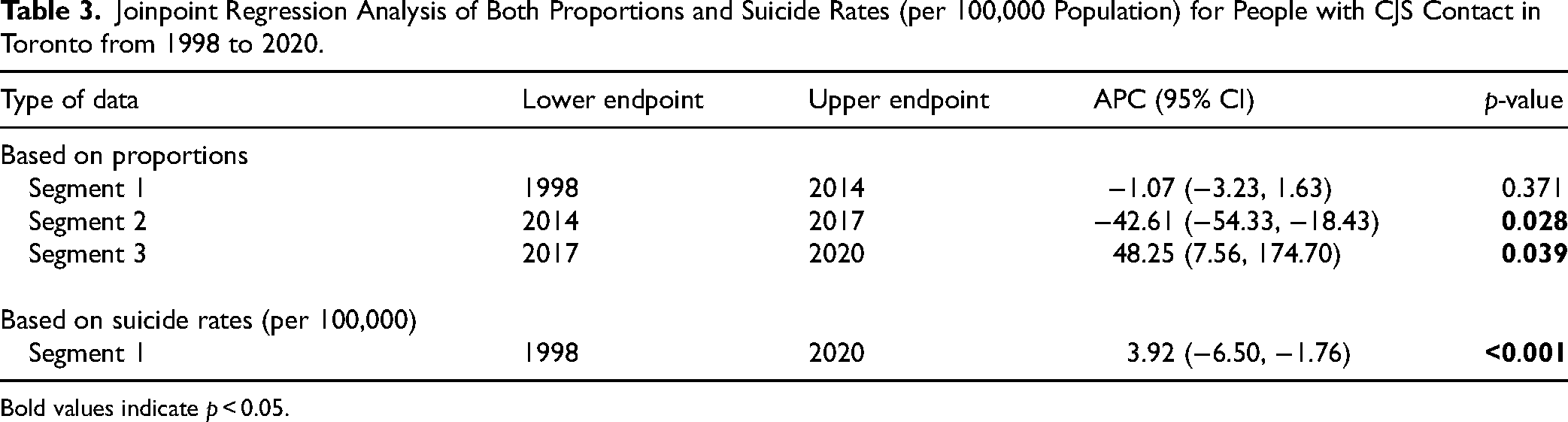
Bold values indicate p < 0.05.
Post Hoc Tests Results
Sensitivity analysis results are presented in Supplementary Table 1. When controlling for age, sex, marital status, and living circumstance variables, bivariate analyses confirmed that those who had CJS contact were more likely to report interpersonal conflict and/or relationship breakup stressors, and to have had substance use disorders. In contrast, they were less likely to report employment/financial stressors, medical stressors, and depression. Demographic and clinical characteristics according to the number of offences reported and violence of offence(s) are included in Supplementary Tables 2 and 3, respectively. In both instances, groups significantly differed according to age, sex, interpersonal conflict, relationship break-up, medical stressors, depression, substance abuse, and suicide method hanging. Comparing decedents with single to multiple charges/legal processes yielded results similar to the overall analysis. Those who were charged with 1 charge/legal process were mostly older males, with interpersonal conflict stressors, depression, and hanging as a suicide method. Those charged with multiple charges/ legal processes also reported more substance abuse-related problems.
Discussion
Our study explored suicide trends among people in Toronto, Canada with CJS contact identified by coroner investigations finding that younger age, male sex, interpersonal stressors (including conflict and relationship breakups), and substance misuse were all associated with CJS contact. We identified that approximately 5% (or 1 in every 20) of suicide decedents had a CJS stressor before death, which is a lower proportion when comparing to cities in the United States, 30 for example. CJS involvement, as well as the related conviction for crimes, can negatively impact mental health and/or the ability to cope with mental health challenges.4-6,15,16,19,20,24,25 Having contact with the CJS carries social stigma that can have wide-ranging impacts on numerous aspects of an individual's life (e.g., financial stability, employment security, interpersonal relationships, etc.) both before and after potential incarceration36,37 A prior Canadian study found that individuals who had experienced incarceration often prefer to lie about their criminal background in job applications due to concerns about discrimination, acts which themselves aroused feelings of guilt and shame. 37 People with CJS involvement frequently point to a lack of empathy in interactions with CJS personnel (e.g., lack of respectful treatment, mockery about mental wellbeing) as impacting their self-perception contributing to feelings of worthlessness, isolation, and a sense of entrapment that can contribute to self-harm. 12 The lack of consistent mental health assessments, interventions, and social supports in the context of CJS contact negatively impacts mental wellbeing.12,13 All of this can further hinder help-seeking behaviours among those who are known for having lower propensity to seek help, such as men. 38
We identified demographic factors that distinguished those who had CJS contact and died by suicide, such as being young, male, with interpersonal conflict and/or relationship breakup stressors, and substance abuse/use disorders. These results confirm prior evidence indicating that most CJS-related suicide deaths occurred among younger males,10,24,25 with interpersonal violence and/or substance abuse problems.10,13,20,24 These demographics also align with the known demography of those who are incarcerated in Canada. 15
Furthermore, we identified 4 violent (e.g., assault, physical assault, serious/death threats, and sexual assault) and 1 non-violent (e.g., impaired driving) offences as the most prevalent among suicide decedents with CJS involvement. Comparing to US findings, it is notable that none of the most represented offences were drug related, and this may owe to differences in substance laws between the countries. 24 However, these results align with previous studies where people with higher suicide risk and self-harm-related behaviours had been charged with 1 or more violent offence(s) (violent offence: 4.1% vs. non-violent offence: 2.0%), 39 mostly interpersonal violence (for example, domestic violence and sexual offences: 67%), 24 and offences such as murder and sexual assault. 13 Ontario's Criminal Justice (OJS) statistic reports (2024) 40 show that, in Toronto, the top 5 most reported criminal offences between 2012 and 2020 were theft (13.3%), failure to comply with a court order (12.7%), common assault (10.9%), major assault (9.1%), and breach of probation (5.2%), (see Supplementary document, Table 4). The prominence of assault matches our suicide decedent findings; however, there are obvious differences. Charges related to impaired driving, for example, appear much more frequent among those who had CJS involvement and died by suicide compared to OJS's statistics (CJS: 12% vs. OJS: ∼3.4%). These results are similar to previous studies indicating that people with CJS involvement who died by suicide were more likely to have 1 or more traffic violations and higher levels of traffic court involvement.17,24 These results suggest the importance of risk assessment and intervention for those who are accused and/or convicted of an impaired driving-related offence.
We found a higher prevalence of substance abuse and/or misuse among those with CJS contact, which may partly explain the high frequency of this specific charge in this group. Substances can also contribute to impulsivity which can moderate the transition from suicidal thoughts to behaviour 8 Post-hoc results comparing violent and. non-violent offence groups identified that those with a violent offence were slightly older males, with interpersonal conflict and/or relationship breakup stressors, similar to previous findings. 25 The high proportion of suicide decedents with violent offences may be then a reflection of deficits in coping with interpersonal conflict and/or relationship breakup stressors (i.e., pre-motivational phase).
We found higher death proportions with identified substance misuse problems among those with multiple charges. Among those with multiple charges/legal processes, there is a concern regarding a vicious cycle in which individuals with previous negative experiences with the system, and/or dealing with the stigma of being criminal charged, experience significant stress and use unhealthy coping mechanisms such as substance abuse/misuse which may, in turn, increase the likelihood of further CJS contact.
There was a decrease in suicides among those with CJS contact per 100,000 population over the study period. Both Canada overall and Toronto specifically have seen a similar decreasing trend in police-reported crimes from 1998 to 2023,41,42 which may partly explain the reduction of cases observed in our results as well. Indeed, examining trends based on the proportion of CJS contact, we observe a significant decrease in the trend from 2015 to 2017, but a sudden increase from 2017 to 2020. This is similar to Toronto's crime statistics for the same period of time. 41
Finally, previous literature highlights evidence on potential cost-benefits of mental health interventions prior to, and after, CJS contact,30,43,44 and the positive impact of multi-program suicide prevention strategies in the reduction of suicide risk among those who are in custodial settings. 45 People with CJS involvement emphasize the importance of having access to fast and adequate mental health assessments, and dignity in their treatment as key elements to preserving their mental wellbeing while being processed in the system. 12 Following our demographic results, addressing environmental factors such as support navigating interpersonal conflict and/or relationship break-ups (especially among males), and encouraging help-seeking behaviour and treatment for substance abuse/misuse-related problems may reduce risk of both subsequent criminal offence incidence and suicide. Supporting individuals in their transition from CJS contact to society reintegration is fundamental to destigmatize and positively reconstruct an individual's identity,36,37 which could lead to feelings of inclusion and reduce hopelessness and entrapment. 4 Therefore, examining strategies that encourage the preservation and maintenance of mental and social wellbeing while navigating the CJS (at any stage) is key in the prevention of suicide. Lastly, governments and courts may consider routinely offering resources to those involved in the CJS encouraging social connection and coping skills. Such efforts would likely have a series of benefits including reducing the risk of suicide as well as recidivism. 46
Strengths and Limitations
Our study includes several strengths, most notably that it relied on records of detailed coroner investigations in one of North America's largest cities over a long-time span (23 years). It is also, to our knowledge, the first study rigorously examining suicide profiling in relation to CJS contact in Toronto. Nevertheless, our study has several limitations. First, coroners’ files may contain missing information based on the nature of data collection (e.g., unavailable next-of-kin interviews and/or inaccurate information shared by next of kin, missing police reports, missing criminal records). This may limit our understanding of whether a decedent had CJS involvement and for what reasons. These same issues may have led to missing demographic and/or clinical data. Therefore, our group comparisons must be interpreted with caution and require replication. Additionally, the fact that our data does not include ethnicity is an important limitation as research shows significant disparities between ethnic groups and CJS involvement. Our study also relied on cross-sectional data with limited information about the temporal relationship between stressors meaning that we were unable to comment on that aspect. Lastly, our sample included individuals who committed/had been convicted of serious criminal offences, and our study was not designed to disentangle the impact of CJS involvement from the stress of conviction for an offence.
Conclusion
This study identified the demographic, clinical, and offence-related/criminogenic characteristics of those who died by suicide and had CJS involvement in Toronto, Canada between 1998 and 2020. In general, suicide rates of those with CJS involvement decreased through the years, and the sample comprised mostly men with interpersonal conflict and/or relationship stressors. These results highlight key profile differences for the prevention of suicide in the context of CJS, especially among groups at increased risk of suicide. Future hypothesis-driven research including comparisons with living controls and/or psychological autopsies will further advance our understanding of this area. In the meantime, policymakers and clinicians engaged with the CJS should focus on efforts to mitigate suicide risk in young men with interpersonal and/or substance problems.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251342276 - Supplemental material for Criminal Justice System Contacts among Suicide Decedents in Toronto, 1998-2020: An Observational Study: Démêlés avec le système de justice pénale parmi les personnes décédées par suicide à Toronto, entre 1998 et 2020 : Une étude d’observation
Supplemental material, sj-docx-1-cpa-10.1177_07067437251342276 for Criminal Justice System Contacts among Suicide Decedents in Toronto, 1998-2020: An Observational Study: Démêlés avec le système de justice pénale parmi les personnes décédées par suicide à Toronto, entre 1998 et 2020 : Une étude d’observation by Daniel Sanchez-Morales, Samantha Mason, Prudence Po Ming Chan, Rohan Borschmann, Alexander Simpson, Lauren M. Weinstock, Jennifer M. Dmetrichuk, Ayal Schaffer, Rachel H.B. Mitchell, Rosalie Steinberg and Mark Sinyor in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We acknowledge and thank Andrew Stephen and the staff at the Office of the Chief Coroner of Ontario for their assistance with this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Sinyor and Dr. Mitchell's work were supported in part by Academic Scholars Awards from the Departments of Psychiatry at the University of Toronto and Sunnybrook Health Sciences Centre. Dr. Schaffer's work was supported in part by an Academic Scholar Award from the Departments of Psychiatry at Sunnybrook Health Sciences Centre. Dr. Weinstock receives research grant funding from the US National Institute of Mental Health (P50MH127512), the Warren Alpert Foundation, and book royalties from Oxford University Press; Australian National Health and Medical Research Council (NHMRC) Emerging Leadership Investigator Grant (grant number EL2; GNT2008073).
Research Ethics and Patient Consent
This project was approved by Sunnybrook Heath Science Center Research Ethics Board, project number #1980.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.