
Abstract
Objectives
Non-suicidal self-injury (NSSI) is a common behaviour in youth with mental disorder and in the general population. While NSSI is an important predictor of suicide attempts, not all youth with NSSI experience this outcome. The objective of this study is to report on the overlap between NSSI and suicidal ideation or attempt among Canadian youth self-reporting these behaviours in the general population to define a group of youth who engage in NSSI alone. This group of youth may represent a unique clinical phenotype.
Methods
We used data from 14–17 year olds (N = 2,576) from the 2014 Ontario Child Health Study, a province-wide, cross-sectional, epidemiologic study of child health and mental disorder. Based on their responses to questions about past year experiences of suicidal thoughts and behaviours including NSSI, 6 mutually exclusive groups were created reflecting their differing profiles of suicidal thoughts and behaviours. These groups were compared to each other on socio-demographic and symptom characteristics.
Results
A total of 9.2% of youth reported NSSI, and half of these youth endorsed NSSI alone (without suicidal ideation or attempts). Both groups had significantly more females. Compared to other groups of youth endorsing suicidal thoughts and behaviours, the NSSI alone group had lower symptoms of mental disorder in all domains except for social anxiety symptoms. They also had the lowest perceived need for help of all groups.
Conclusions
About half of youth who self-harm do so without suicidal intent, and some for as long as 1 year during adolescence. Further prospective study of youth with NSSI alone is needed, to determine symptom stability as well as incident more risky suicidal behaviour before recommendations regarding the appropriateness of minimal medical or psychological intervention for youth who engage in this behaviour can be considered. There also are important sex differences in NSSI that deserve additional prospective study.
Introduction
A meta-analysis of prevalence studies of suicidal thoughts and behaviours in adolescents found a 12-month prevalence of 14.2% for suicidal ideation (SI), 14.2% for deliberate self-harm, and 4.5% for suicide attempts up to age 20. 1 Lifetime prevalences are higher in all studies, and age differences are important in adolescence with past year estimates of suicidal thoughts and behaviours being higher for youth 15 and older.2,3 Between 20% and 25% of youth report self-harm without any intent to die1,4 that is, they engage in non-suicidal self-injury or NSSI. 5 This group is the main focus for this paper.
The challenge for research in the field of NSSI, in particular, and self-harm more generally, is that one-third to one-half of youth who endorse NSSI also endorse experiencing SI at, or around, the same time.6–9 Few studies have reported the proportion of youth who engage in NSSI and do not report suicidal ideation or attempts during a defined interval.10,11 While Scott et al. 10 explored NSSI and suicidal ideation as prospective predictors of suicide attempts in adolescents, they did not examine an “NSSI-alone” subgroup (i.e., NSSI without any history of suicidal ideation) due to an insufficient sample size. Voss et al. 11 were able to investigate the prevalence estimates for lifetime NSSI and its co-occurrence with suicidal thoughts and behaviour. In this study, it was reported that 11.7% of adolescents and young adults aged 14–21 years engaged in NSSI-alone without the co-occurrence of suicidal behaviour (i.e., ideation and attempts) as a lifetime estimate. It was also noted that individuals reporting NSSI-alone were more likely to be female, while those with NSSI with associated suicidal thoughts or behaviour only were more likely to be male (Voss et al. 11 ).
Ascertaining whether an NSSI-alone group exists and persists for youth is important as such a group may not be at increased risk for other suicidal behaviour, compared to youth with no history of self-harm. If this finding were substantiated, it may facilitate a different approach to intervention such as increased focus on behaviour modification for NSSI.
The practical or clinical implications of identifying a group of adolescents with NSSI-alone would be bolstered by evidence supporting distinct correlates among youth with NSSI-only compared to youth endorsing NSSI with suicide ideation, plans, and attempts. The most consistently supported correlates of self-harm—irrespective of intent—include prior self-harm,8,12 substance abuse, 13 anxiety, 13 depressive symptoms,13,14 friends or family who also engage in self-harm, 15 and female sex. 13 Andover et al. 16 provided a comprehensive review of studies that have sought to identify risk factors for NSSI/self-harm that may be distinct from those for suicide attempts. They note that the majority of risk factors are common to both behaviours (NSSI and attempts) whereas risk factors for suicidal ideation may be different, a finding replicated by Kokaliari et al. 17 It is important to note that the NSSI in these studies could not be clearly identified to be NSSI-alone (without concurrent suicidal ideation).
The aim of this study is to estimate the extent of overlap between NSSI-alone and suicidal ideation (SI) or suicide attempt (SA) among Canadian youth self-reporting these behaviours in the general population to describe the characteristics of a group of youth who engage in NSSI-alone.
Sex differences in the prevalence or features of suicidal behaviours and NSSI-alone are also important to consider. A study of sex differences in suicidal behaviours across adolescence identified that girls are 1.7 times more likely to have SI (girls: 15%; boys: 9%) and 2.9 times (girls = 6%; boys = 2%) more likely to make a SA than boys. 18 Boys are more likely to die by suicide beginning in adolescence, and this sex difference is apparent beginning at age 14 (sex ratio of 1.89). 19 A recent meta-analysis of 120 studies of NSSI prevalence identified a significantly greater effect size for sex of NSSI (female > male OR = 1.5, 95% CI, 1.35 to 1.65), which was even larger in clinical samples. 20 Sex differences in NSSI did not vary as a function of age (adolescent vs. adult) meaning that adolescent girls were also 1.5 times more likely to engage in NSSI as boys. 20 Again, it is important to note that the behaviour NSSI in these studies is not distinguished as being NSSI-alone.
Objectives
Using a representative sample of youth aged 14–17 years in Ontario, the study objectives are to:
Determine the past-12-month prevalence of non-suicidal self-injury (NSSI), SI, and SA, overall and by sex (male, female). Estimate the overlap between past 12-month NSSI and SI and SA. Establish 6 mutually exclusive groups of youth (unaffected, NSSI-alone, SI alone, NSSI and SI, SI and SA or NSSI and SI and SA—the “complex group”) and determine the extent to which these groups are distinguished by clinical and socio-demographic correlates.
Methods
We used data from the 2014 Ontario Child Health Study, 21 a province-wide, cross-sectional, epidemiologic study of child health and mental disorder. A probability sample of 6,537 households (58.8% response) with 10,802 4 to 17 year olds participated. The sampling frame was the 2014 Canadian Child Tax Benefit (CCTB) file. Households were selected based on a complex 3-stage survey design that involved cluster sampling of residential areas and stratification by residency (urban, rural) and income (areas and households cross-classified by 3 levels of income (<20th; 20th to 80th; >80th percentiles). Detailed accounts of the survey design, content, training, and data collection are available elsewhere. 22
Measures
Suicidal Thoughts and Behaviours
The 2014 OCHS
21
asked youth a series of questions about suicide. We used these questions to classify individuals according to the following criteria:
Suicide ideation (SI): Youth who said “yes” to the question “In the past 12 months, did you ever seriously consider taking your own life or killing yourself” were coded as suicide ideation present (1). Those who said no were coded as suicide ideation absent (0). Youth who answered “yes” were also asked questions about suicide attempts. Suicide attempt (SA): Youth who said “yes” to SI and “yes” to the question “In the past 12 months, did you actually try to take your own life?” were coded as SA present (1). Those who said “yes” to suicide ideation and “no” to SA were coded as SA absent (0). Those who said “no” to SI were not asked about attempts and so were also coded SA absent (0). It should be noted that the youth were only asked about SAs if they endorsed SI, thus all youth who endorsed SA in the past 12 months also endorsed SI during this time period.
Non-suicidal self-injury (NSSI)
Youth who said “yes” to the question “In the past 12 months, did you ever deliberately harm yourself but not mean to take your life?” were coded as NSSI present (1). Those who said “no” were coded as NSSI absent (0).
Comparison groups
In addition to examining these thoughts and behaviours independently, these criteria were also used to create 6 mutually exclusive groups of youth for the examination of clinical and socio-demographic correlates. These groups were classified as follows:
Control group: This group reported having no SI or SA and no NSSI in the past 12 months. Non-suicidal self-injury (NSSI) alone: This group reported NSSI with no intercurrent SI or SA in the past 12 months. Suicide ideation (SI) alone: This group reported SI alone but no SA or NSSI in the past 12 months. Suicide ideation and NSSI (SI/NSSI): This group reported SI alone and NSSI but no SA in the past 12 months. Suicide ideation and suicide attempt (SI/SA): This group reported suicide ideation and SA but no NSSI in the past 12 months. Suicide ideation, NSSI, and suicide attempt (complex): This group reported SI with SA and NSSI in the past 12 months.
Mental Health Symptoms
Youth completed the OCHS Emotional–Behavioural Scales (OCHS-EBS) 21 which are dimensional measures of 6 DSM-V disorders (major depressive disorder (MDD); generalized anxiety disorder (GAD); social anxiety disorder; attention-deficit hyperactivity disorder (ADHD); oppositional-defiant disorder (ODD); and conduct disorder (CD)). The OCHS-EBS were presented in a self-administered checklist questionnaire with response options of “0 = never or not true,” “1 = sometimes or somewhat true,” and “2 = often or very true.” Items were summed to generate scale scores and have demonstrated satisfactory validity and reliability. Detailed information on the evolution, development, and psychometric properties of the scales are available.22,23
Other Clinical Correlates
Youth reported on their experiences with substance use (nicotine, cannabis or other illicit drugs, and heavy episodic drinking), peer victimization, and exposure to child maltreatment as described in a previous publication. 24 The use of any substances was collapsed into a binary classification (0 = no, 1 = yes) and similar binary classifications were established for report of being victimized by peers at least once or twice a month, and exposure to any form of child maltreatment.
Perceived Need for Professional Help
Perceived need was defined as positive responses to 2 sequenced questions that asked whether the youth thought that, in the past 6 months, they had any emotional or behavioural problems, and if yes, needed any professional help with these problems. Perceived need was coded as present (1) if the youth answered yes to both questions; and otherwise, absent (0).
Service Contact
Mental health-related service contact was assessed using 2 questions administered to the parent and the youth: (1) whether the youth had seen or talked to a medical doctor or other professional about mental health concerns; and (2) whether they had gone to a specific setting for mental health concerns in the past 6 months. Additional questions asked about the type of provider(s) seen and where this care occurred. Service contact was coded as present (1) when either the parents or the youth reported contact with at least 1 provider or in at least 1 service setting and otherwise, absent (0).
Socio-Demographic Correlates
Socio-economic and demographic characteristics of families and children were collected using standard Statistics Canada questions administered to the person most knowledgeable (PMK) on child sex (male or female), age (in years), number of biological parents in the home (2 vs. 1 or no biological parent), household income below the low income measure (based on the 2013 before tax cut-offs) and urban–rural residency (large urban, small–medium urban, and rural).
Sample for Analysis
Eligible for inclusion in the analysis were all youth aged 12 to 17 (n = 2,910) who were invited to complete a computerized self-complete questionnaire about themselves. Only cases with complete information on all variables of interest were included in the study (n = 2,576). We compared included cases with excluded cases (n = 334); there were no statistically significant differences in the socio-demographic characteristics, mental health symptoms, and service use.
Analysis
Prevalence estimates were calculated separately for each of SI, SA, and NSSI overall and broken down by sex. We also estimated the overlap between SI, SA, and NSSI. Finally, we examined the distribution of clinical and socio-demographic correlates among 6 mutually exclusive groups (controls, SI, SI + SA, NSSI-alone, NSSI + SI, and complex), testing for group differences. We used pairwise comparisons to examine group differences, using the chi-square test for categorical covariates and the F test for continuous covariates (age, income, mental disorder). Estimates were weighted using survey weights and replicate bootstrap weights with an adjustment factor to account for the study design. STATA software version 14.0 was used for all analyses.
Results
Table 1 shows the past 12-month prevalence of suicidal thoughts and behaviours and NSSI. Past year prevalence of SI was 8.6% (6.0% male, 11.4% female), SA was 4.8% (3.7% male, 5.9% female), and NSSI was 9.3% (4.3% male, 14.5% female). There were statistically significant sex differences in prevalence for SI and NSSI, but not for SA.
Past 12-Month Prevalence of Suicidal Thoughts and Behaviours, and NSSI Behaviours Overall and by Sex.
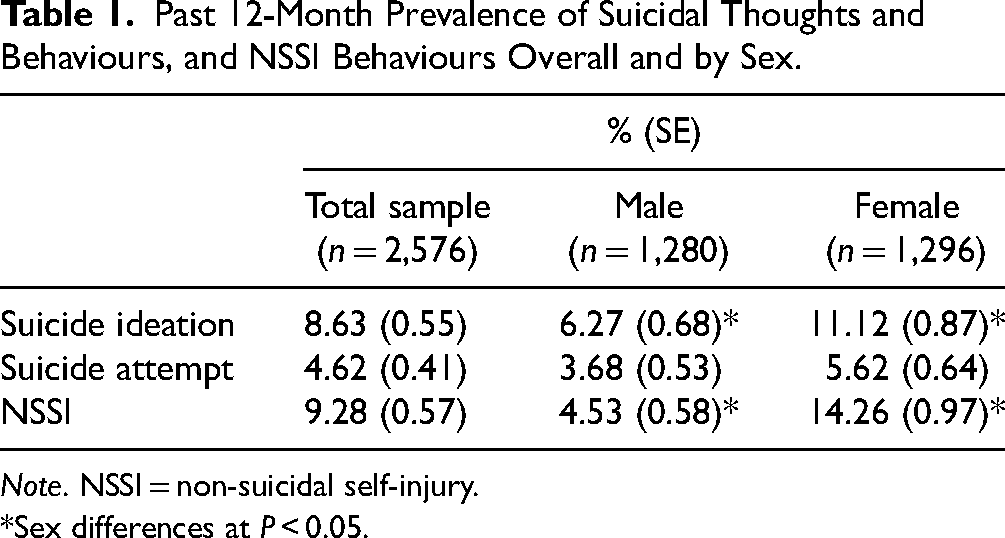
Note. NSSI = non-suicidal self-injury.
*Sex differences at P < 0.05.
Figure 1 shows the prevalence of 6 distinct groups of youth: control, NSSI-alone and the overlap between suicidal thoughts and behaviours and NSSI. The prevalence of NSSI-alone was 4.5% and this group was the largest of the distinct groups. NSSI with SI and/or SA was only slightly more prevalent (4.8%) than NSSI-alone. The next largest group was composed of youth with SI only (2.2%). Of youth who reported a SA (4.8%) two-thirds of this group also engaged in NSSI in the past 12 months.
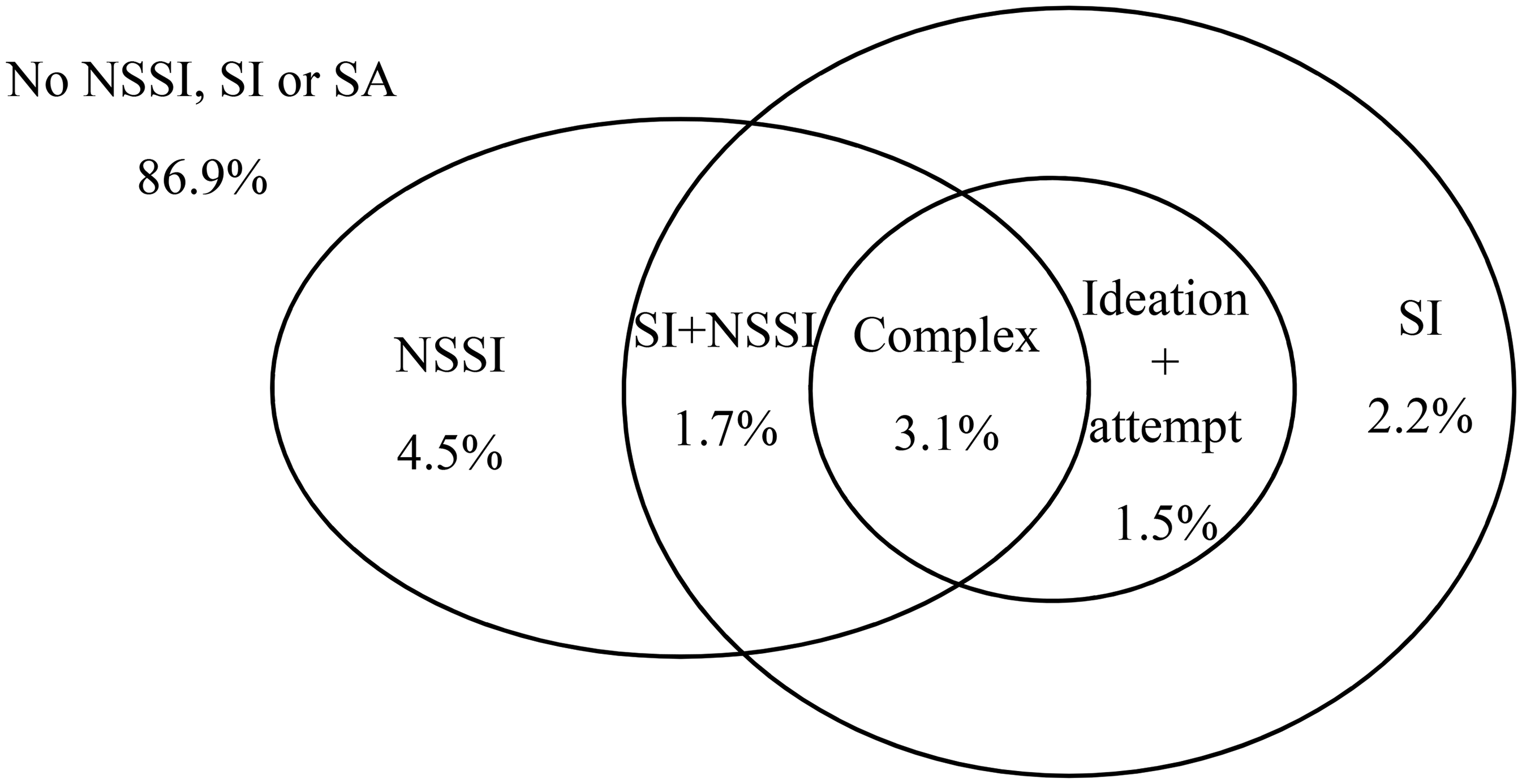
Groups of youth with distinct co-occurrence of suicidal thoughts and behaviours and NSSI.
Table 2 presents the distribution of socio-demographic and clinical correlates among the 6 mutually exclusive groups (control, SI, NSSI-alone, SI + NSSI, SI + SA, complex). Sample sizes for the groups are unweighted but all estimates are weighted. Perceived need for help and exposure to peer victimization was greater in all groups compared to the control group. There were statistically significant differences between the control group and other groups with respect to mental health service contacts. The complex group also reported more service contacts than the NSSI-alone and the NSSI + SI groups. Compared to the control group, the NSSI-alone group contained more females, were less likely to live with both biological parents, and were more likely to live in a small–medium urban area. Compared to the control group, the SI group contained more females and was more likely to live in a rural area. Compared to the control group, the SI + SA group was more likely to live in a small–medium urban area. Finally, the complex group had more females, were more likely to be older, and less likely to live with both biological parents than controls.
Socio-Demographic and Clinical Correlates of Non-Suicidal Self-Injury Behaviours and Suicidal Thoughts and Behaviours.
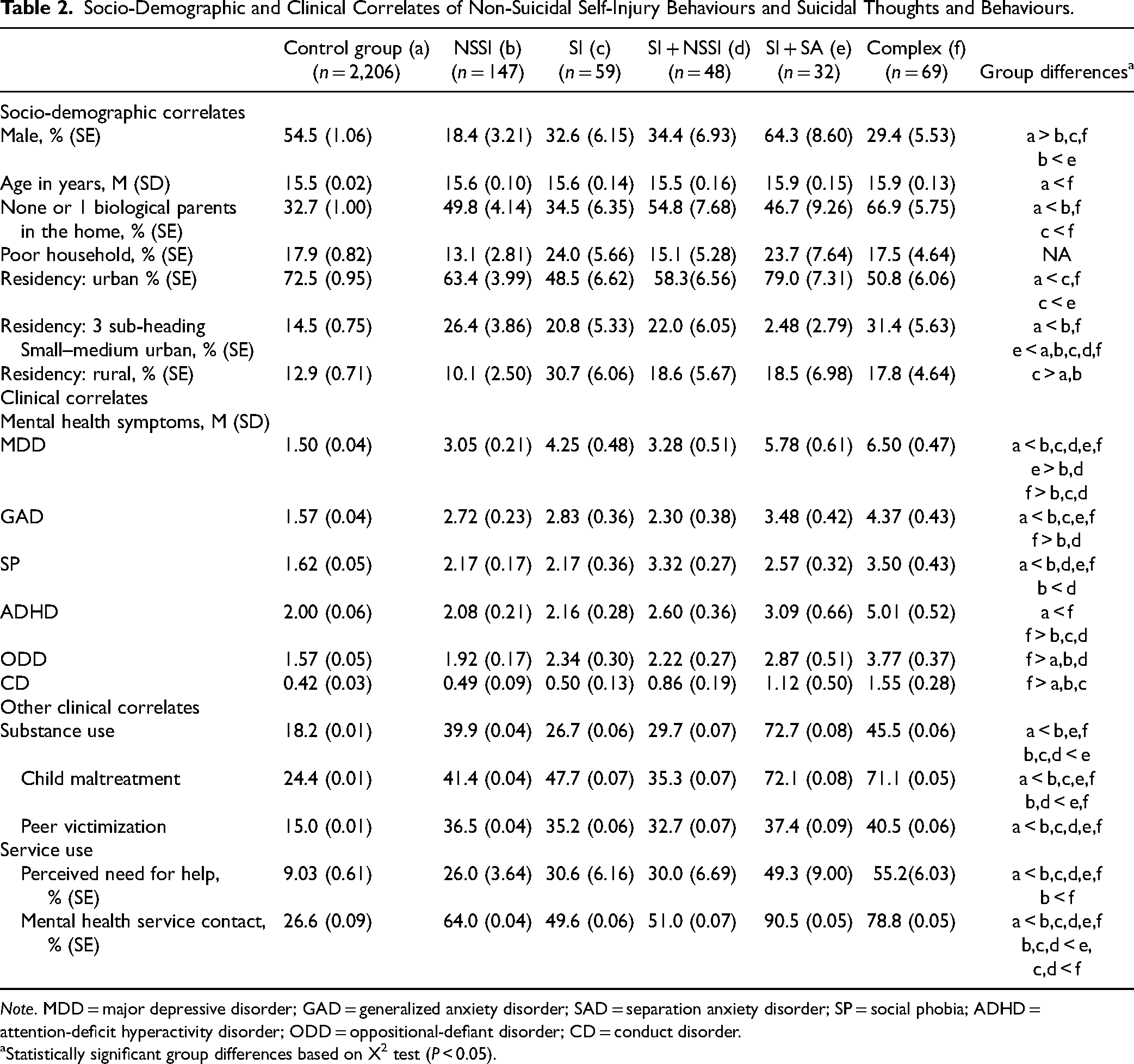
Note. MDD = major depressive disorder; GAD = generalized anxiety disorder; SAD = separation anxiety disorder; SP = social phobia; ADHD = attention-deficit hyperactivity disorder; ODD = oppositional-defiant disorder; CD = conduct disorder.
Statistically significant group differences based on X2 test (P < 0.05).
When comparing the groups with any of SI, SA, or NSSI (i.e., excluding controls) to each other, there were fewer group differences on socio-demographic correlates but there were notable differences on some clinical correlates and social risk variables. In summary, when comparing the NSSI-alone group to other groups with NSSI and SI or SA, differences were most notable when the comparison group was the complex group. Complex group youth scored higher on MDD, GAD, ADHD, ODD, and CD scales and had higher rates of perceived need for help compared to the NSSI-alone group or the SI + NSSI group. The most notable difference was between the complex group and the SI-alone group. The complex group had elevated symptom scores, and was less likely to live with both biological parents. Youth with SI + NSSI had higher levels of social phobia symptoms than their peers with NSSI-alone. History of child maltreatment and higher service use were significantly more common in youth who endorsed SA than youth without SA. Substance use was more common among youth with any form of self-harm compared to youth with SI alone.
Discussion
This paper describes the prevalence of past year suicidal thoughts and behaviours, as well as NSSI in a representative sample of adolescents living in Ontario. Across ages 14–17, SI was reported by 8.6% (6.2% male, 11.1% female) of youth, with significantly more females being affected. This estimate of SI was lower than in the meta-analysis (range 11–17%). 1 The sex difference in SI is consistent with meta-analytic reviews. Lim et al. 1 did not distinguish clinical from epidemiologic samples and the clinical data likely inflated their estimates. An Ontario community study (Ontario Student Drug Use and Health Survey—OSDUHS) conducted in 2015 reported a 1 year prevalence of suicidal ideation of 12.4% (8.2% M, 16.9% F) among respondents who were slightly older than those in this study. 25
A total of 9.3% (4.5% M, 14.3% F) of youth in this study reported engaging in NSSI over the past year with significant sex differences. This 12-month estimate is also significantly lower than those from meta-analyses,1,4 many of which include clinical samples. A prior Ontario study with a clinical sample reported higher rates of NSSI in youth identifying 20.2% within a 12-month period. 3
SAs were reported by 4.6% of youth (3.7% M, 5.6% F) with no significant sex difference. Other studies using past year estimates have found a significant sex difference in report of SAs. The OSDUHS found a past year SA prevalence of 3% (1.5% M, 4.5% F) which was a significant sex difference. 25 Meta-analyses of adolescent studies have noted a small but significant sex difference with females reporting more SAs. 5 It is likely that our findings reflect general population estimates for SI, SA, and NSSI.
Our second objective was to identify how commonly youth engage in self-harm in the absence of any SI in a 12-month period, which we termed NSSI-alone. We found that 4.5% of youth engage in NSSI-alone, which is almost half of youth who report NSSI. This means that NSSI can occur over at least a 1-year period in adolescents and is not associated with suicidal thoughts or behaviours. This group is largely composed of females (81%). This is the first study to report the 1-year prevalence of NSSI-only. As age didn’t differ between these groups, it is unlikely that NSSI-alone in youth is an earlier occurring phenomenon among adolescents who then transition to later suicidal behaviours.
Our third objective tested whether youth reporting NSSI-alone may have fewer mental health symptoms, service use, and psychosocial adversity as compared to youth with SI and/or SAs. Youth with NSSI-alone had lower symptoms of mental disorder in all domains except for social anxiety symptoms. They also had the lowest perceived need for help, and similar rates of service use to youth with SI or NSSI + SI but less than those with report of SA.
Based on our multi-group comparison (Table 2), some differential associations seem worthy of future research. The majority of youth reporting SAs engage in NSSI, whereas those with NSSI-alone are almost exclusively female. This may mean that girls with NSSI without SI or attempt are less likely than boys with this presentation to ever have a SA. Most boys with NSSI in this study also reported SAs or had SI, thus those boys presenting to services with NSSI-alone should be closely monitored for incident SI/attempts. Given that we were able to distinguish a group with NSSI-alone from one with NSSI and SI in the past year, these groups should be compared regarding the types and frequency of the self-harm behaviours they engage in, as these features may distinguish youth whose NSSI is more likely to progress to SAs. 26
Among the 3 groups labelled SI, SI + SA, and NSSI-alone, clinically significant differences were not apparent for age and family income. There was a trend where youth in groups endorsing either NSSI, SA, or both behaviours to be less likely to live with both parents. This difference is small but worthy of further study as youth with both NSSI and SAs have reported lower levels of parental support than youth engaging only in NSSI. 27 Clinical correlates did differ between these groups suggesting these groups may be clinically different and worthy of additional careful comparisons in larger studies. Youth with NSSI-alone had significantly fewer MDD, GAD, ODD, and ADHD symptoms than their peers with SI or SA. Several studies, mostly clinical, have shown a pattern of greater severity of symptoms or diagnoses in youth engaging in SAs and NSSI, however typically the comparison group is youth with SAs and no NSSI. 16 Our study found that conduct disorder symptoms were highest in the SA group, and depressive symptoms were higher in the youth with SI and attempts compared to youth with NSSI-alone. These data suggest that conduct and mood symptoms are important correlates of suicidal ideation and attempt as they are less common in youth with NSSI-alone. The association of conduct and mood symptoms with youth suicidal behaviours have been the most replicated disorder specific symptom associations28,29 in studies of different groups of youth with suicidal behaviours. Substance use was associated with any self-harm (NSSI or SA) and SA in particular was associated with exposure to child maltreatment. This suggests the other clinical correlates we studied were predictive of self-harm irrespective of suicidal intent.
Although we did not have data to confirm the presence of diagnostic criteria for NSSI disorder, this study suggests that a sizeable group of youth who self-harm do so without suicidal intent, and some for as long as 1 year during adolescence. Further prospective study of NSSI-alone is needed, to determine stability/predictive validity before recommendations regarding the appropriateness of minimal medical or psychological intervention for youth who engage in this behaviour can be considered. If this group is stable in this behaviour and it occurs with minimal harm or impairment, psycho-education about the function of NSSI and coaching on alternative emotion regulation strategies may be an indicated intervention. Indeed, some have argued that in some cases, NSSI-alone may be developmentally normative. 20 If NSSI-alone is stable, this has very important public health implications.
Strengths and Limitations
The OCHS represents a large, representative population sample which allowed for the dis-aggregation of groups central to this study. Data were collected cross-sectionally reflecting over the past year. This may have been a strength allowing us to collect more accurate estimates of suicidal behaviours and thoughts. While we were able to identify mutually exclusive groups over this year, some comparisons were constrained by small numbers and some estimates were suppressed due to confidentiality concerns. At the time of the study, Statistics Canada did not collect data on gender.
Additional studies are needed to confirm the validity and stability of NSSI-alone over time, and our findings. While past year recall may be more reliable than lifetime recall, 30 the sequencing of outcomes remains unclear. For example, where youth are grouped as having a complex presentation (NSSI + SI + SA), SI may have emerged before or after NSSI, suggesting different proximal causes. Given their breadth, it is difficult for epidemiologic studies to measure aspects of these outcomes such as their frequency or temporality with sufficient detail needed to corroborate clinically relevant phenotypes. In addition, we did not have information about severity/duration/frequency of self-harm beyond whether it happened during the past year.
Conclusion
Suicidal thoughts, behaviours, and NSSI are common in Ontario adolescents. We identified a group of self-harming youth who engage in NSSI-alone, constituting 4.5% of the sample of 14–17 year olds. This group was composed of predominantly girls who have lower levels of psychopathology, greater socio-economic advantage, and similar numbers of service contacts to youth with SI, despite the absence of SI in the past year. Longitudinal studies are needed to establish the persistent absence of SI and SA in this group of youth.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research Grant number 125941, Ministries of Education, Child and Youth Services and Health and Long-term Care, Government of Ontario.