
Abstract
Objective:
To evaluate the feasibility and preliminary efficacy of a digital dialectical behaviour therapy (d-DBT) skills intervention in suicidal psychiatric inpatients.
Methods:
A parallel arm, assessor-blinded, randomized controlled trial (RCT) was conducted to compare d-DBT to standard care among psychiatric inpatients. Participants included adults admitted for suicidality (i.e., suicidal ideation or suicide attempt). The intervention group received a d-DBT intervention encompassing 5 online modules completed over 5 to 10 days, covering mindfulness, emotion regulation, and distress tolerance skills. Participants received an initial orientation but no formal therapy sessions. Daily check-ins were available for technical-related queries. Feasibility outcomes included recruitment, adherence (≥3 modules completed), retention, and acceptability (client satisfaction questionnaire-8). Efficacy outcomes included suicidality (Columbia-Suicide Severity Rating Scale [C-SSRS] total score), psychological distress (K10), emotion regulation (Difficulties in Emotion Regulation Scale-16 [DERS-16]), and clinical global impression (CGI). Linear regression models analysed group differences.
Results:
A total of 65 participants were recruited, of which 42 were randomized, with high d-DBT adherence rates in the intervention arm (75%). The d-DBT intervention demonstrated significant reductions in C-SSRS scores (Cohen's −1.0) compared to standard of care. No significant group differences were observed in K10, DERS-16, or CGI. High acceptability and satisfaction were reported among participants randomized to d-DBT. Challenges and limitations included maintaining follow-up postdischarge and the small sample size.
Conclusion:
d-DBT is feasible to implement through an RCT and may reduce suicidality and improve mental health among psychiatric inpatients. The study highlights the importance of developing accessible, evidence-based interventions for this population. Future research should focus on long-term efficacy and expanding the intervention's appeal and accessibility.
Introduction
Suicide is a devastating public health issue that profoundly impacts individuals and communities. Suicidality, a broad term encompassing suicidal ideation, plans for suicide, and suicide attempts, represents a critical global health crisis. 1 Approximately 3.2 million cases of intentional self-harm and approximately 842,000 suicides occur globally each year, leading to a loss of nearly 35 million years of life. In Canada, the gravity of this issue is underscored by suicide ranking as the ninth leading cause of death across all age groups, with a particularly high incidence among those aged 10 to 44 years. 2 In Ontario, suicide data from 2008 to 2012 reveal a total of 5,650 suicide deaths, many by individuals diagnosed with mood, substance use, or personality disorders. 3 According to Statistics Canada, in 2019, there were 4,500 suicide deaths. The literature further shows that the majority of these individuals had sought mental health care in various forms in the years and even months leading up to their suicide. 2 This underscores the need for effective and timely interventions during critical interactions with the healthcare system.
Patients admitted to psychiatric inpatient settings represent a particularly high-risk group, exhibiting high rates of suicidal ideation associated with various mental health disorders. 4 Furthermore, suicidal psychiatric inpatients are at a high risk of suicidal behaviour postdischarge. 5 Despite the urgent need for effective interventions, the current therapeutic landscape for treating suicidality is notably limited and focuses primarily on managing risk and targeting underlying mental health conditions. Previous studies have investigated various treatment modalities for reducing suicidality in psychiatric inpatients such as brief psychotherapeutic interventions, brain stimulation modalities, and novel pharmaceutical compounds such as ketamine.6–9 In routine clinical practice, however, there is limited focus on interventions that specifically target suicidality, despite evidence that this may be a more effective approach. 10 One reason for this is that many of these interventions with independent antisuicidal properties are not widely available. Furthermore, many existing treatments, such as lithium and electroconvulsive therapy, have demonstrated efficacy in reducing suicidality; however, their use is often limited by significant side effects and barriers to access, including patient preferences, provider availability, and systemic constraints. In addition, most clinical trials in psychiatry systematically exclude patients with moderate to high suicidality. This raises critical questions about the applicability of the existing evidence base to highly suicidal patients.
The current approach to treating suicidal patients in hospitals favours pharmaceutical and somatic treatments, with limited use of psychotherapeutic interventions. This is the case despite evidence supporting the effectiveness of psychosocial interventions such as dialectical behaviour therapy (DBT) in reducing suicidality. 10 However, findings on DBT's effectiveness remain somewhat mixed, particularly outside of populations with borderline personality disorder.11–13 Variability in study populations, treatment fidelity, and methodological limitations may contribute to these inconsistencies.11,14 Recent systematic reviews highlight the ongoing challenges but potential in identifying effective psychotherapeutic interventions for suicidality in inpatient settings. 7
Despite growing evidence supporting psychosocial treatments such as DBT, accessibility remains a major barrier, particularly in hospital settings where trained personnel, structured programs, and sustained engagement are often lacking. Many individuals face significant obstacles in accessing these therapies due to a scarcity of trained therapists, high costs, stigma, and logistical challenges related to the length and intensity of DBT-based interventions.15,16 These barriers are particularly pronounced in acute inpatient settings, where short hospital stays and competing clinical demands limit opportunities for structured psychotherapeutic interventions. Without scalable and accessible alternatives, many patients at high risk for suicidality remain unable to benefit from evidence-based psychosocial treatments.
More recently, digital interventions have emerged as a promising solution to bridge this treatment gap in mental health care. 15 These digital platforms offer a novel approach to delivering psychological treatments, with cost-efficiency, ease of dissemination, scalability, and reduced stigma being key advantages. 16 While preliminary evidence suggests that digital interventions may help reduce suicidality, their feasibility and acceptability in psychiatric inpatient settings remain underexplored.17,18 Most existing studies have focused on community-based samples, leaving a critical gap in understanding how digital DBT could be tailored and effectively implemented for high-risk inpatient populations. The present study aims to evaluate the feasibility and effectiveness of a digital DBT skills intervention for suicidal psychiatric inpatients admitted to a large academic health center in Toronto, Ontario.
Methods
The study was approved by the Centre for Addiction and Mental Health (CAMH) research ethics board and registered on Clinicaltrials.gov (identifier NCT05045677) on September 16, 2021.
Study Design
This was a parallel arm, assessor-blinded, randomized controlled trial (RCT) comparing the efficacy of a digital DBT (d-DBT) skills intervention to standard care among psychiatric inpatients. The study was structured to allow for integration within the operational framework of a busy tertiary psychiatric care facility focused on acute clinical care. This healthcare environment is very dynamic, where patient presentations and needs undergo frequent fluctuations. Drawing upon insights from previous clinical trials involving inpatient psychosocial interventions, our primary aim was to develop an intervention that emulates the flexibility and authenticity of real-world clinical practices. 19 During the study, participants continued to consult with their usual inpatient psychiatric team. The study was completed over five consecutive days at any point during a participant's inpatient admission, after obtaining consent and confirming eligibility. If after consent the admission was determined to be less than 5 days, participants were permitted to complete the digital intervention in less than 5 days. Participants were also offered the opportunity to complete the modules in more than 5 days if it was deemed necessary based on inpatient care needs. The minimum acceptable number of modules completed was a priori decided to be 3 out of 5 to account for participants that may be discharged from the hospital prior to completing the modules.
Participants
Included participants were aged 18 years and above, presenting with any Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) diagnosis per the clinician-administered Mini-International Neuropsychiatric Interview (MINI). 20 Eligible participants were admitted to CAMH for suicidality (defined as a nonzero Columbia-Suicide Severity Rating Scale [C-SSRS] score), 21 willing to consent, anticipated admission greater than 5 days at the time of referral, and deemed suitable for participation in a psychotherapeutic intervention. Exclusion criteria included the inability to complete d-DBT due to severe psychiatric symptoms (e.g., severe agitation, cognitive impairment, and disorganized thought form) and concurrent convulsive therapies given concerns about cognitive side effects.
Study Groups
The intervention group received the d-DBT intervention plus standard inpatient care.
The d-DBT intervention included five online modules covering mindfulness, emotion regulation, and distress tolerance skills and was delivered on a study-issued tablet. Each module was approximately 30 to 60 min in length and was accompanied by an optional worksheet to encourage on-unit practice of the relevant skill. This digital intervention is a modified version of the d-DBT skills intervention developed by Drs Wilks and Linehan, and previously evaluated in outpatients with suicidality and severe alcohol use.
22
The original intervention was administered weekly and intended for outpatients, thus the present intervention was adapted to be administered daily for psychiatric inpatients (e.g., changing language from “last week” to “yesterday,” reducing the number of skills learned given a shorter time frame). The addiction module was removed as substance use was not an inclusion criterion in the present study. The intervention was structured into 5 modules, each focusing on a core skill area.
The comparator group received standard inpatient care alone, including psychiatric review, medication management, and multimodality psychosocial group interventions.
Participants received a brief orientation from study staff on navigating the intervention. Daily check-ins were available to address technical issues, but no formal therapy sessions were included. An unblinded study team member conducted these daily check-ins with all participants, regardless of treatment allocation, to provide support and ensure engagement with the intervention.
Outcomes
The primary outcome was feasibility and acceptability of implementing the intervention by participants and inpatient clinical staff. Feasibility outcomes included recruitment, adherence to modules (completing at least 3 of 5 modules), retention, and completeness of outcome measures at each time point. Acceptability was informed by the client satisfaction questionnaire-8 (CSQ-8) and a user-experience questionnaire (UXQ).23,24 The CSQ-8 is an 8-item measure evaluating participants’ satisfaction with the intervention, with total scores ranging from 8 to 32, where higher scores indicate greater satisfaction. The UXQ is an 11-item measure designed to capture perceptions of the intervention's ease of use, serviceability, and overall user experience. Each item is scored from 0 to 10, with total scores ranging from 10 to 110, where higher scores indicate greater usability. We also invited participants to provide a narrative description of their experience with the intervention. We grouped relevant feedback into themes and presented representative quotes.
Secondary outcomes included a change in suicidal ideation score as measured by the C-SSRS, as well as a change in clinical global impression (CGI), 25 emotion regulation (brief Difficulties in Emotion Regulation Scale-16 [DERS-16]), 26 and psychological distress (Kessler psychological distress scale (K10)). 27 DSM-5 diagnoses were confirmed by the clinician-administered MINI for DSM-5 version 7.0.2 (MINI).
Changes in secondary outcomes were assessed postintervention completion and again at 4 weeks postdischarge. If participants were discharged 1 week after completing the study period, secondary outcomes were assessed again at the time of discharge.
Randomization and masking
Participants were randomized into the study using a random permuted block method. A research assistant external to the study managed the randomization of subjects. Outcome assessors were masked to allocation; however, given the nature of the trial and intervention, participants and inpatient staff were unblinded. Outcome assessors were trained research assistants.
Statistical Analysis
A sample of 40 subjects, 20 per group, is deemed sufficient to assess the feasibility and acceptability of an intervention. 28 For the primary outcome of feasibility and acceptability, data from all participants were included. For secondary outcome measures, we report results only for those participants who completed the intervention. We did not conduct an intention-to-treat (ITT) analysis given the exploratory nature of the study and small sample size. Analysis of variance was conducted to examine the differences in baseline clinical and demographic variables across the intervention groups. Linear regression models were used to analyse the impact of the intervention on various secondary outcome measures. Initial models (unadjusted) evaluated the relationship between postintervention outcomes and the intervention. Subsequently, adjusted models were developed which incorporated relevant baseline symptom scores, age, sex, and primary diagnosis as control variables. Cohen's d was calculated for each outcome measure to quantify the intervention's effect size. Statistical analysis was conducted in RStudio version 2023.12.0+369.
Role of Funding Source
The funder of the study had no role in the study design, data collection, data analysis, data interpretation, or writing of the manuscript. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
Participant Flow and Recruitment
Clinical teams on the inpatient units notified study staff of potential participants who were admitted with suicidality and were interested in the study. A total of 65 patients were recruited from May 4, 2022, to January 31, 2023, of whom 42 were randomly assigned to one of two treatment groups. Of the total sample (i.e., both groups), 85% completed the intervention period and 29% completed the follow-up period 4 weeks postdischarge (see Figure 1). The first 2 participants recruited were removed after allocation due to an initial technical issue with launching the digital intervention. Reasons for participant withdrawal during the intervention period included early discharge prior to completion of at least 3 modules, inability to engage with the intervention, and, in 1 instance, participant dislike of the intervention.
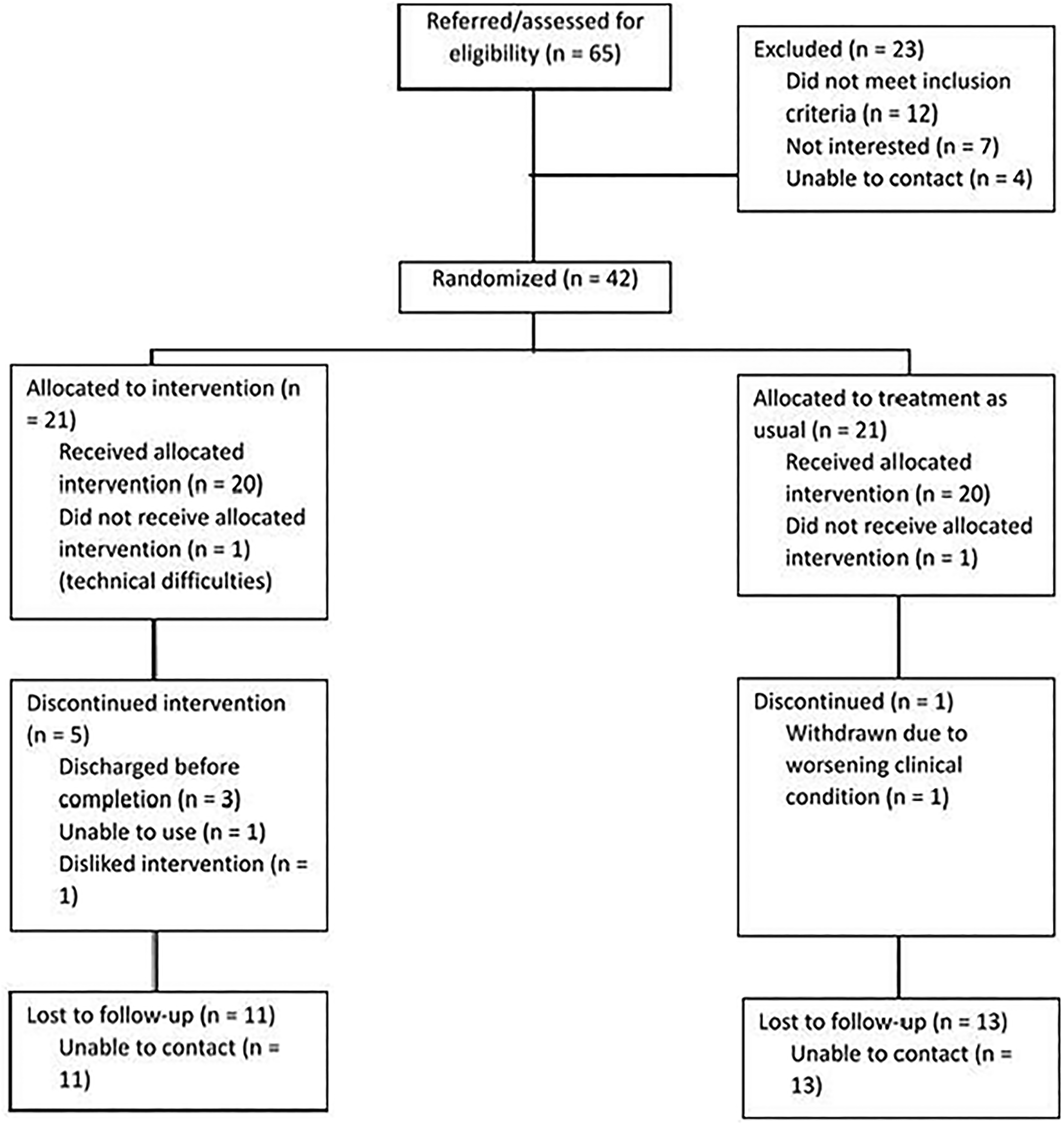
Consort.
Baseline Data
Table 1 describes the baseline demographic and clinical variables of the sample. The most common primary diagnosis was major depressive disorder with a high degree of psychiatric comorbidity, with an average of 5 (SD = 2) MINI diagnoses. The mean baseline C-SSRS score was 22.3 for the entire sample with no significant difference between groups. There was no significant difference between groups on all baseline clinical or demographic variables.
Baseline Demographic Data.
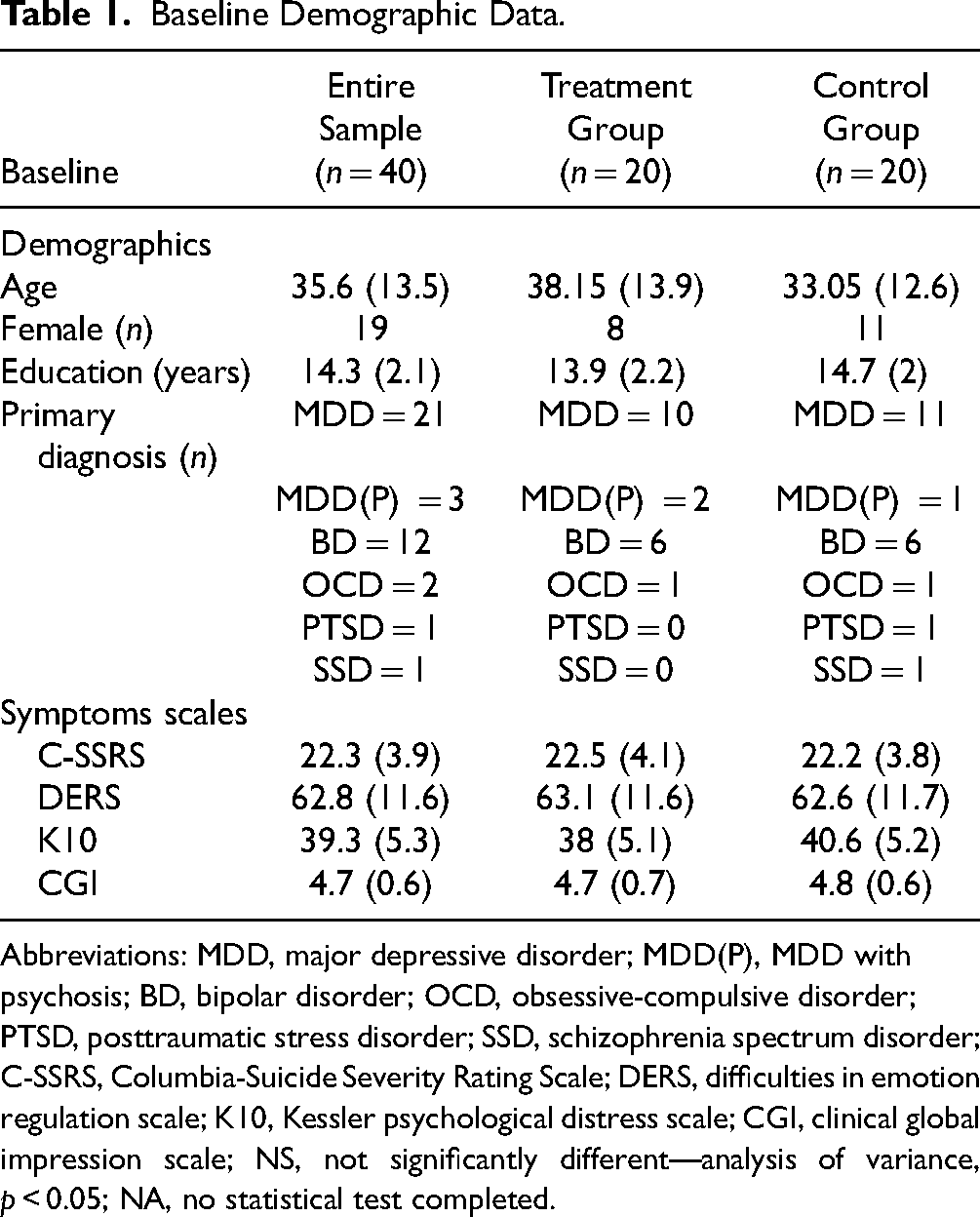
Abbreviations: MDD, major depressive disorder; MDD(P), MDD with psychosis; BD, bipolar disorder; OCD, obsessive-compulsive disorder; PTSD, posttraumatic stress disorder; SSD, schizophrenia spectrum disorder; C-SSRS, Columbia-Suicide Severity Rating Scale; DERS, difficulties in emotion regulation scale; K10, Kessler psychological distress scale; CGI, clinical global impression scale; NS, not significantly different—analysis of variance, p < 0.05; NA, no statistical test completed.
Feasibility and Acceptability
In total, 15 out of 20 (75%) participants allocated to the intervention arm adhered to the d-DBT intervention and were retained through to the primary postintervention endpoint. The UEQ indicated moderate to high acceptability (mean = 76.9, SD = 19.1), while the CSQ-8 demonstrated high satisfaction (mean = 26.6, SD = 1.8). These findings suggest a positive reception of the intervention. Participants provided primarily positive narrative feedback which is summarized in Table 2.
Feedback From Participants.

A combination of direct quotes written down on feedback or a summary of statements expressed to the research team recorded during the feedback session.
Clinical outcomes measures
C-SSRS scores were significantly lower postintervention in those receiving d-DBT compared to participants receiving treatment as usual (Table 3). This remained significant when controlling for baseline C-SSRS score, age, diagnosis, and gender (Table 4). There was no significant difference between groups in postintervention K10, DERS, or CGI in the unadjusted or adjusted models (Table 4). Cohen's d was large for the C-SSRS (−1.03) and effect sizes were moderate for the K10 (−0.57), DERS (−0.43), and CGI (−0.50) postintervention (Table 3). We were unable to complete regression models for the 4-week postdischarge outcomes given the high rates of loss to follow-up.
Postintervention Scores of Secondary Outcome Variables.
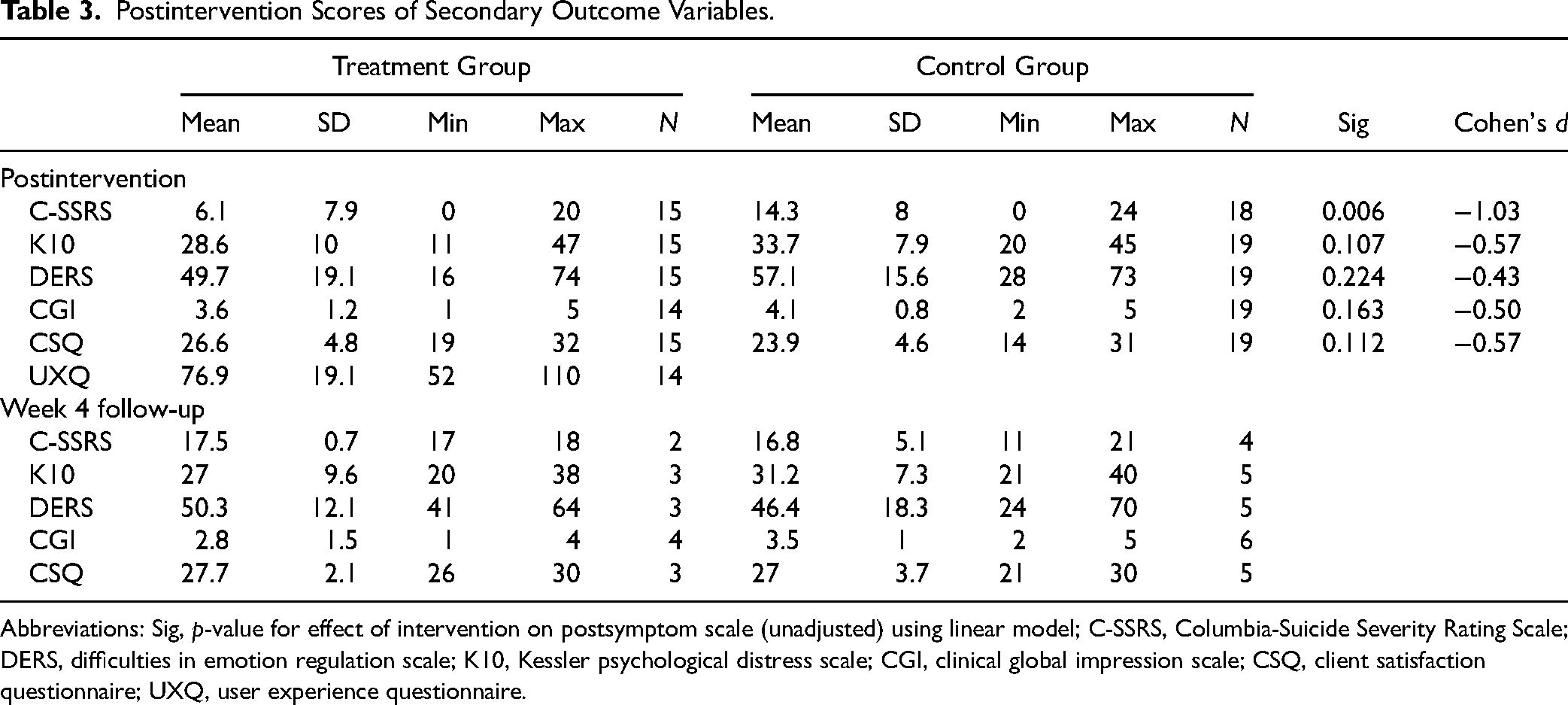
Abbreviations: Sig, p-value for effect of intervention on postsymptom scale (unadjusted) using linear model; C-SSRS, Columbia-Suicide Severity Rating Scale; DERS, difficulties in emotion regulation scale; K10, Kessler psychological distress scale; CGI, clinical global impression scale; CSQ, client satisfaction questionnaire; UXQ, user experience questionnaire.
Regression Models.
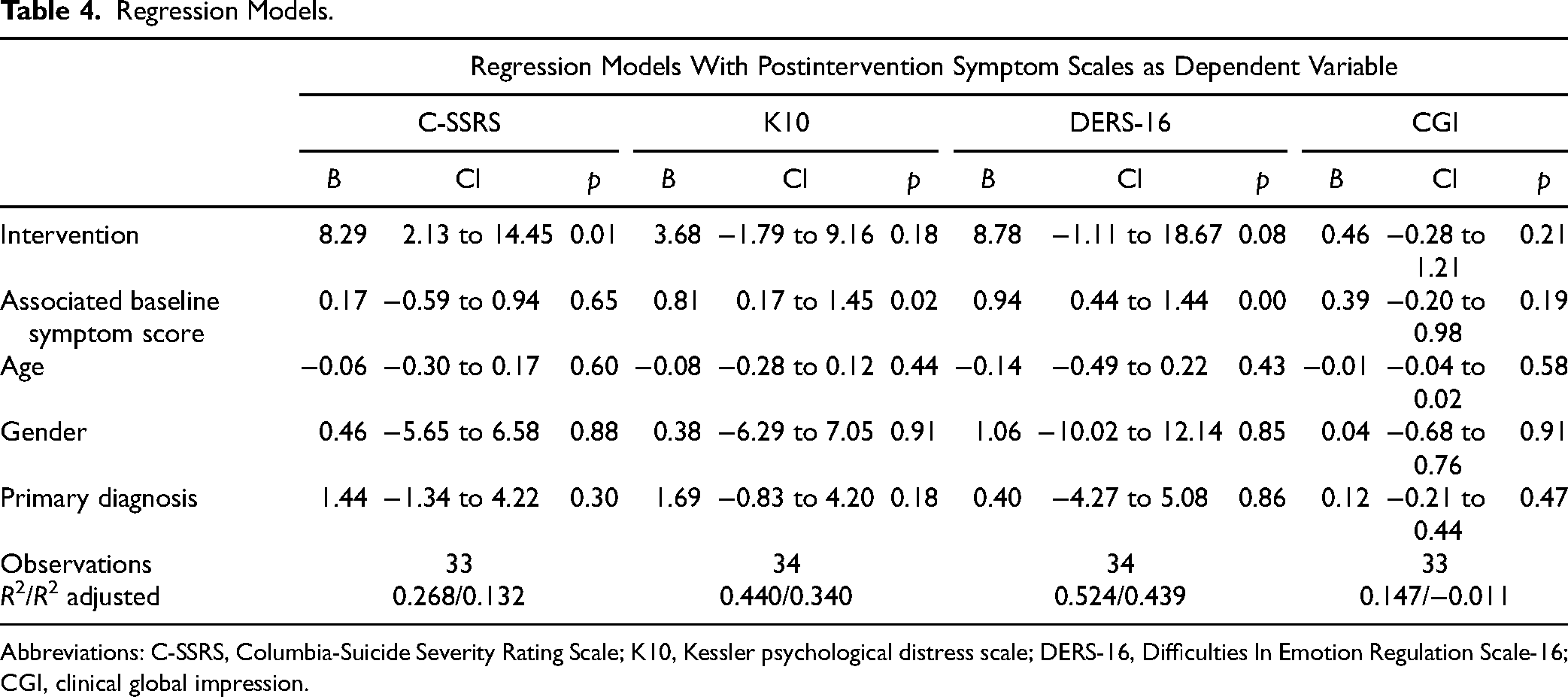
Abbreviations: C-SSRS, Columbia-Suicide Severity Rating Scale; K10, Kessler psychological distress scale; DERS-16, Difficulties In Emotion Regulation Scale-16; CGI, clinical global impression.
Adverse Events
There were no serious adverse events related to the study intervention. There were 2 nonserious unrelated adverse events, with 1 reported in each of the study arms.
Discussion
This RCT assessed the feasibility and preliminary efficacy of a d-DBT skills intervention for suicidal psychiatric inpatients. The high rate of participant referral and recruitment underscores the feasibility of interventional trials in a busy inpatient setting. The ease of recruitment not only reflects clinical teams’ recognition of the need for innovative therapeutic options, but also suggests their readiness to explore and adopt digital interventions. Importantly, the intervention's high completion rates and positive feedback from participants demonstrate its acceptability among a diverse patient population. We recruited and retained participants of a wide age range and diagnoses. This acceptance is crucial, considering the varied needs and backgrounds of psychiatric inpatients, and it highlights the potential for wider implementation of digital interventions in similar settings and for diverse patient populations.
Engagement with the d-DBT intervention led to a significant decrease in C-SSRS scores postintervention. While the study was not adequately powered to assess intervention efficacy, these preliminary results suggest that a d-DBT intervention may be an effective and feasible approach to delivering DBT skills in high-risk patient populations. Notably, the preliminary effect size is large and symptom reductions occurred over a short period of time (5–10 days). This finding alongside moderate effectsizes in other outcome measures, suggests that d-DBT may improve overall mental health among a diverse group of psychiatric inpatients. Future RCTs adequately powered to detect treatment effects are warranted. These findings are consistent with previous studies investigating applications of psychotherapeutic interventions to reduce suicidality as well as the benefit of digital interventions to reduce suicidality in outpatients.8,25 They are also consistent with reviews suggesting that psychosocial interventions can affect inpatient treatments for suicidality.
Integrating clinical trials into an inpatient setting that is not specifically designated for research is logistically challenging due to competing demands. By aligning our study design as much as possible with the dynamic context of an inpatient facility, our core objective was to ensure the highest degree of adaptability. This approach permitted us to mirror the challenges and opportunities routinely encountered by clinicians, thereby enhancing the applicability of our findings to real-world clinical settings. In essence, our study aimed to bridge the gap between controlled research environments and the intricacies of real-world inpatient psychiatric care. These considerations underscore the importance of methodological considerations specifically for this patient population and unique setting. For example, despite good recruitment and retention for the study period, there was a substantial challenge in reconnecting with participants postdischarge. One explanation may be the fragmented nature of postdischarge community care in an urban centre such as Toronto. While we were able to integrate ourselves into the clinical setting for the inpatient units, it was more logistically challenging to stay connected with participants once they left the hospital.
While the primary aim was not an efficacy trial, the study's sample size limited statistical power for all secondary outcomes and precluded a formal ITT analysis with multiple imputations. Instead, we focused on effect size estimates and feasibility outcomes to guide future research. In assessing the narrative feedback from participants, some felt the intervention was too didactic or was not visually appealing. Future replications of this work should invite service users to help codevelop the application to help reach a broader audience. Another limitation, as discussed above was the poor follow-up at 4 weeks postdischarge. To address this limitation in future trials, strategies such as closer collaboration with outpatient services, the use of automated reminders, optional phone follow-ups, and integration of follow-up procedures into established discharge planning workflows should be considered. Additionally, increasing participant engagement during the inpatient phase and exploring the use of digital tools for remote assessments may help mitigate attrition and improve data collection during this critical postdischarge period. Future studies should also focus on evaluating long-term outcomes with larger and more diverse samples to better understand the sustained impact of digital DBT interventions on suicidality. Implementation of self-report measures of suicidality in addition to clinician-rated scales would also provide additional insight.
Conclusion
In conclusion, the current feasibility of RCT demonstrates not only the feasibility and acceptability of a digital DBT intervention in a psychiatric inpatient setting but also its potential efficacy in addressing suicidality among a diverse patient group. The largely positive feedback from participants and ease of recruitment signals a broader interest and readiness for innovative mental health treatments for this population. However, the challenges encountered in maintaining long-term follow-up emphasize the need for more robust methodologies in future research. Our study marks a step towards developing evidence-based, accessible interventions for a historically underrepresented and vulnerable population in mental health care.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251337607 - Supplemental material for A Digital Dialectical Behaviour Therapy Intervention for Acute Suicidality in Psychiatric Inpatients: A Feasibility Randomised Controlled Study: Intervention numérique en thérapie comportementale dialectique en cas de suicidabilité aiguë de patients hospitalisés en psychiatrie : Étude de faisabilité contrôlée à répartition aléatoire
Supplemental material, sj-docx-1-cpa-10.1177_07067437251337607 for A Digital Dialectical Behaviour Therapy Intervention for Acute Suicidality in Psychiatric Inpatients: A Feasibility Randomised Controlled Study: Intervention numérique en thérapie comportementale dialectique en cas de suicidabilité aiguë de patients hospitalisés en psychiatrie : Étude de faisabilité contrôlée à répartition aléatoire by Brett D.M. Jones, Mary E. Kittur, Michael S.B. Mak, Wei Wang, Juveria Zaheer, Shelley McMain, M. Omair Husain, Anne Sonley, David Gratzer, Benoit H. Mulsant, Daniel M. Blumberger and M. Ishrat Husain in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We thank Fahd Shaikh for assisting in organizing the data for analysis and Dr Chelsey Wilks for graciously providing us with the intervention and her input early in the development of the protocol. In 2022, BDMJ received The Rankin family and the Kevin Gordon Rankin Memorial Award, which contributed to the development of this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ORCID iDs
Trial Registration
The trial was registered on Clinicaltrials.gov (NCT05045677) on September 16th, 2021.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was funded by a resident research award from the Physicians' Services Incorporated Foundation (grant number R21-15).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.