
Abstract
Objective
This research aims to investigate the relapse rates of major depressive disorder (MDD) within primary care and evaluate the efficacy of relapse prevention therapies. Despite primary care being the common point of contact for MDD patients, there are limited studies around this.
Methods
We included randomized controlled trials and observational studies examining MDD relapse incidence and the effect of pharmacological and non-pharmacological interventions in preventing relapse in primary care. Databases; Medline via Ovid, EMBASE, The Cochrane Library, PsycInfo (ebsco), and Clinical Trials.gov were searched from their inception until September 7, 2022. Joanna Briggs Institute (JBI) appraisal instrument for methodological quality assessment was used. A proportional data analysis estimated the MDD relapse incidence. Therapy effectiveness results were shown as odds ratios with 95% confidence intervals, with heterogeneity explored via subgroup analysis.
Results
Out of the reviewed studies, 35 met the eligibility criteria. Quality appraisal scores varied between 73% and 96%. MDD relapse incidence was divided into subgroups, revealing that both pharmacotherapy and non-pharmacotherapy led to a similar decrease in relapse rates with combination therapies showing further reduction in relapse. Subgroup analyses by study design, follow-up length, date of study and quality of study also yielded noteworthy findings.
Conclusion
Our findings showed that MDD relapse rates in primary care settings can be effectively reduced by pharmacotherapy, non-pharmacotherapy, or combination therapy. Some psychological interventions might also reduce relapse likelihood. More studies are needed on individual and combined treatments over longer periods to understand their long-term impacts on MDD relapse in primary care.
Plain Language Summary Title
How Often Depression Returns and How Well Treatments Work in Primary Care: A Review of Studies
Plain Language Summary
This study looked at how often people depression experience return of symptoms, when they are treated in primary care settings, such as family doctor clinics, and how well different treatments work to prevent this return of symptoms. Even though primary care is where many people with depression first seek help, there hasn't been much research on how to best prevent this return of symptoms in this setting. To gather information, the study looked at and summarized the studies that were published around this topic following a standard procedure. The study found that both medication and non-medication treatments were beneficial in reducing the chances of return of depression symptoms. Furthermore, using a combination of treatments was even more beneficial. The study also found interesting results when looking at different factors like the type of study and follow-up duration. In conclusion, this study suggests that various treatment options can effectively reduce return of depression symptoms in primary care. This includes medications, psychological therapies, or a combination of both. However, more research is needed to better understand how these treatments work over longer periods and their long-term effects people with depression.
Background
Major depressive disorder (MDD) is the leading cause of disability worldwide with the lifetime prevalence ranging from 2% to 21% of adults experiencing 1 or more episodes of depression. 1 According to the 2019 Global Burden of Diseases, Injuries, and Risk Factors Study, both depressive and anxiety disorders ranked among the top 25 leading causes of global burden, with MDD being the most disabling of the 2 disorders.2,3 Previous research has demonstrated that depression negatively impacts work productivity3 and leads to increased healthcare resource utilization.4,5
Guideline-recommended treatments for MDD include pharmacologic and psychotherapeutic interventions using a collaborative model of care. Although acute phase treatment (defined as 8–12 weeks of treatment) 6 has been well established and effectively alleviates depression symptoms, the risk of relapse remains a significant issue. 7 MDD is highly recurrent, 8 making relapse prevention 1 of the most critical challenges in managing the disorder. 9 Studies suggest that 30–85% of patients experience MDD relapse despite antidepressant therapy,10,11 with risk factors including residual symptoms (odds ratio (OR) 2.77, 95% confidence interval (CI) [2.08–3.68]), a history of previous relapse (OR 1.69, 95%CI [1.28–2.24]), a history of or current comorbid anxiety disorder (OR 1.74, 95%CI [1.37–2.22]), a history of child maltreatment or abuse (OR 1.5, 95%CI [1.27–1.77]). 12 Thus, the relapse of depressive symptoms after successful acute MDD treatment is not only common but also a considerable clinical concern.
Frank et al. 13 proposed a definition of MDD relapse, conceptualizing it as a return of symptoms satisfying the full syndrome criteria for an episode occurring during remission. A systematic review examining the evidence surrounding these concepts and definitions found that specific duration thresholds separating remission from recovery were not meaningful in clinical practice. 14 In light of this finding and guided by clinical guidelines, 6 we consider both relapse and recurrence as relapse in this study.
The risk of relapse can be minimized by continuing antidepressant use after acute treatment. Numerous treatment guidelines advise patients with an MDD episode to continue antidepressant therapy for 4–12 months after successful acute phase treatment to prevent relapse and to maintain full therapeutic doses for up to 2 years or more for those at an increased risk of MDD relapse. Nonpharmacological interventions, such as cognitive behavioral therapy (CBT), have also been explored for relapse prevention and found to be beneficial. 15
Primary care has been defined as the provision of integrated, accessible healthcare services by clinicians who are accountable for addressing a large majority of personal healthcare needs, developing a sustained partnership with patients, and practicing in the context of family and community. 16 The majority of people with mental health problems are managed in primary care. 17 Despite primary care being the most frequent point of contact for MDD patients seeking healthcare services, studies examining MDD, therapy, and other critical factors within the primary care context are relatively scarce. The majority of work exploring the scope of the problem of depressive relapse has been done in secondary care settings and is likely to be of limited applicability to primary care, 12 which is where the vast majority of patients with depression are managed. For instance, there are few investigations into MDD relapse therapy in primary care settings. A systematic review by Prieto-Vila et al. 18 explored relapse risk factors in MDD patients, but the review only encompassed randomized controlled trials (RCTs) involving psychotherapy. Furthermore, only a few studies have aimed to meta-analyze both pharmacotherapy and non-pharmacotherapy in MDD relapse in primary care. Sim et al. 11 separately examined pharmacotherapy and non-pharmacotherapy interventions for MDD relapse, including various interventions and pooling heterogeneous designs. However, their studies were drawn from mixed healthcare settings and were not specific to primary care. Another meta-analysis by Gili 19 identified a small number of RCTs examining relapse prevention, specifically focusing on primary care samples. Since both studies were published in 2015, more primary care studies, including RCTs, have emerged.
Given the aforementioned limitations of the previous literature, we conducted a systematic review and meta-analysis to (1) investigate the incidence rate of relapse episodes for all intervention groups in patients with MDD in primary care settings, and (2) evaluate the effectiveness of pharmacotherapy and/or non-pharmacotherapy interventions to prevent relapse.
Methods
Study Design
A systematic review was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) and MOOSE (Meta-analysis of Observational Studies in Epidemiology) guidelines during all stages of design, implementation and reporting.20,21 The systematic review was registered in the PROSPERO international prospective register of systematic reviews (protocol number CRD42021290452).
Eligibility Criteria
This review included RCTs and nonrandomized controlled trials (non-RCTs), assessing the incidence rate of relapse episodes in adult patients with MDD and the effectiveness of pharmacotherapy and/or non-pharmacotherapy interventions in primary care setting in preventing relapse. Specific study designs that were eligible included (a) RCTs, (b) non-RCTs, or other quasi-experimental studies, (c) cohort studies (CS), (d) case-control studies (CCS), nested case-control or case-cohort studies. Other study designs were excluded from this review, such as systematic reviews and meta-analyses, case series, case reports, or cross-sectional studies because temporality between exposure and outcome was uncertain. 22
Inclusion criteria for the study population were as follows: (a) adults aged 18 years and older; (b) adults with any type of depressive disorders confirmed by any validated depression scale or by the ICD-10 or the DSM-IV-TR criteria; (c) interventions that included pharmacotherapy, non-pharmacotherapy, psychotherapy or sequential therapy used in MDD. There was no restriction on the type of comparison among intervention; (d) authors’ definition of a primary care setting. Primary care setting could include general practitioner or family physician, nurse practitioner, pharmacists, or mental health worker.
The primary outcome of interest was the incidence of a relapse, measured by any validated depression scale, or changes in the severity of depressive symptoms, as assessed against diagnostic criteria (such as the ICD-10 or the DSM-IV-TR). We excluded studies that included patients with treatment-resistant depression, inpatients and patients who did not receive an intervention or an exposure for depression therapy.
Data Sources and Searches
The search strategy was carried out in collaboration with a research librarian (AF) experienced in systematic reviews from the date of the databases’ inception to September 7, 2022. We searched the following 5 biomedical databases: Medline via Ovid, EMBASE, The Cochrane Library, PsycInfo (ebsco) and Clinical Trials.gov.
The search was developed in Ovid Medline using MeSH Terms and keywords and was subsequently translated into the other databases, using each database's controlled vocabulary and keywords. There were no restrictions on language in the search; however, only English language studies were included. Grey literature such as information produced on all levels of government, academics, business, and industry in electronic and print formats not controlled by commercial publishing was also searched. Duplicate studies were removed using Endnote ×9 and imported into Covidence for screening. See Supplement File 1 for the specific search strategy used in each database and a list of the grey literature sources.
Study Selection
Two reviewers (WAA, SD) independently scanned study titles, abstracts, and keywords of every non-duplicate record retrieved from the literature search. Following title/abstract screening, 2 reviewers independently screened the full text of the included articles. Relevant studies were identified using the software Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). Discrepancies were resolved by consensus of the 2 reviewers. If consensus was not achieved, a third reviewer was consulted.
Data Extraction and Quality Assessment
Data were extracted by 1 reviewer (WAA) onto a predesigned form that included first author, contact details, journal citation, year of publication, study design, funding, sample size, data set used, study location and duration, duration of follow-up, study population characteristics, statistical analysis used, depression diagnosis tool used, relapse definition, the study-specific measure of association, and type of intervention and exposure. Studies with confirmed inclusion criteria were assessed for methodological quality using the standardized critical appraisal instrument from the Joanna Briggs Institute (JBI) Meta-Analysis of Statistics Assessment and Review Instrument. 23 The instrument chosen for review was dependent on the study design of each study included. Each criterion was allocated a score (Yes = 2, No = 0, Unclear = 1), giving a total possible score of 26 for RCTs, a score of 22 for cohort studies and a score of 20 for case-control studies. These scores were then converted to a percentage24,25 for ease of interpretation and comparison. Guided by previous studies using a similar approach in quality assessment,24,25 the quality of each review was ranked based on the following criteria: 0–33% of criteria met (low quality), 34–69% of criteria met (medium quality), and 70% or more of criteria met (high quality). The study selection process was conducted independently by 2 reviewers (WAA, SD). Any disagreements were resolved through discussion, or with a third reviewer (JH). Moreover, included studies that had more than 2 treatment arms, were shown in the forest plots as “author, year, arm—portrayed as a number [1,2,3, etc.].”
Data Synthesis and Analysis
Characteristics of included studies were described and stratified by study design. To estimate the incidence of MDD relapse in this study, we conducted a proportional data analysis. When pooling proportions for meta-analysis, a transformation of the data is required. To transform the data, we used the logit transformation.26,27 This method is used to calculate the weighted summary proportion under the random-effects model. Random effects models were used to pool results from included studies for the outcome. 28 The resultant meta-analysis gives a pooled proportion with a 95% CI both for the fixed and the random-effects model, and lists the proportions (expressed as a percentage), with their 95% CI, found in the individual studies included in the meta-analysis. The results were graphically presented in a forest plot. For the effectiveness of therapies, the results were expressed as an OR with corresponding 95% CI. Heterogeneity was assessed using the Chi-Squared test and measured using the I-squared statistic as recommended by the Cochrane handbook. We followed the guide provided by the Cochrane handbook on the interpretation of heterogeneity. 28 We considered heterogeneity to be “not important” if the I-squared statistic was between 0% and 40%; “moderate heterogeneity” if the I-squared statistic was between 30% and 60%; “substantial heterogeneity” if the I-squared statistic was between 50% and 90%; and “considerable heterogeneity” if the I-squared statistic was between 75% and 100%. Heterogeneity was explored using subgroup analysis.28,29 Meta-analysis was conducted for all treatment arms combined to measure the incidence summary proportion. Meta-analysis was also conducted for subgroups of pharmacotherapy, non-pharmacotherapy and combination therapy. Furthermore, subgroup metanalysis was conducted according to the study design. Finally, we meta-analyzed the OR for the effectiveness of therapies into subgroups of pharmacotherapy, non-pharmacotherapy and combination therapy. Studies that included multiple interventions or more than 1 study arm, were noted with “a number” after the same author's name (e.g., Author X, Year −1; Author X, Year −2; Author X, Year −3; etc). To avoid double counting of the reference groups, we used a “combination method” and a “splitting method.”30,31 Subgroup analysis was done to explore heterogeneity. Incidence was pooled into the following subgroups: study design (RCT, Cohort studies), intervention group (Pharmacological, nonpharmacological, both), length of follow-up (<1 year, 1–2 years, > 2 years), date of study (1990–2000, 2001–2005, 2006–2010, 2010–2015, ≥2016), intervention type, quality of study (≥85% score). Analysis was conducted using R package 4.2.2. (R.app GUI 1.79, S. Urbanek & H.-J. Bibiko, © R Foundation for Statistical Computing, 2021).
Results
Trial Flow
We identified 4,267 potentially relevant citations and retrieved 672 papers for full-text review (Figure 1). Of these full-text review studies, 35 studies met the eligibility criteria and were included in this systematic review.
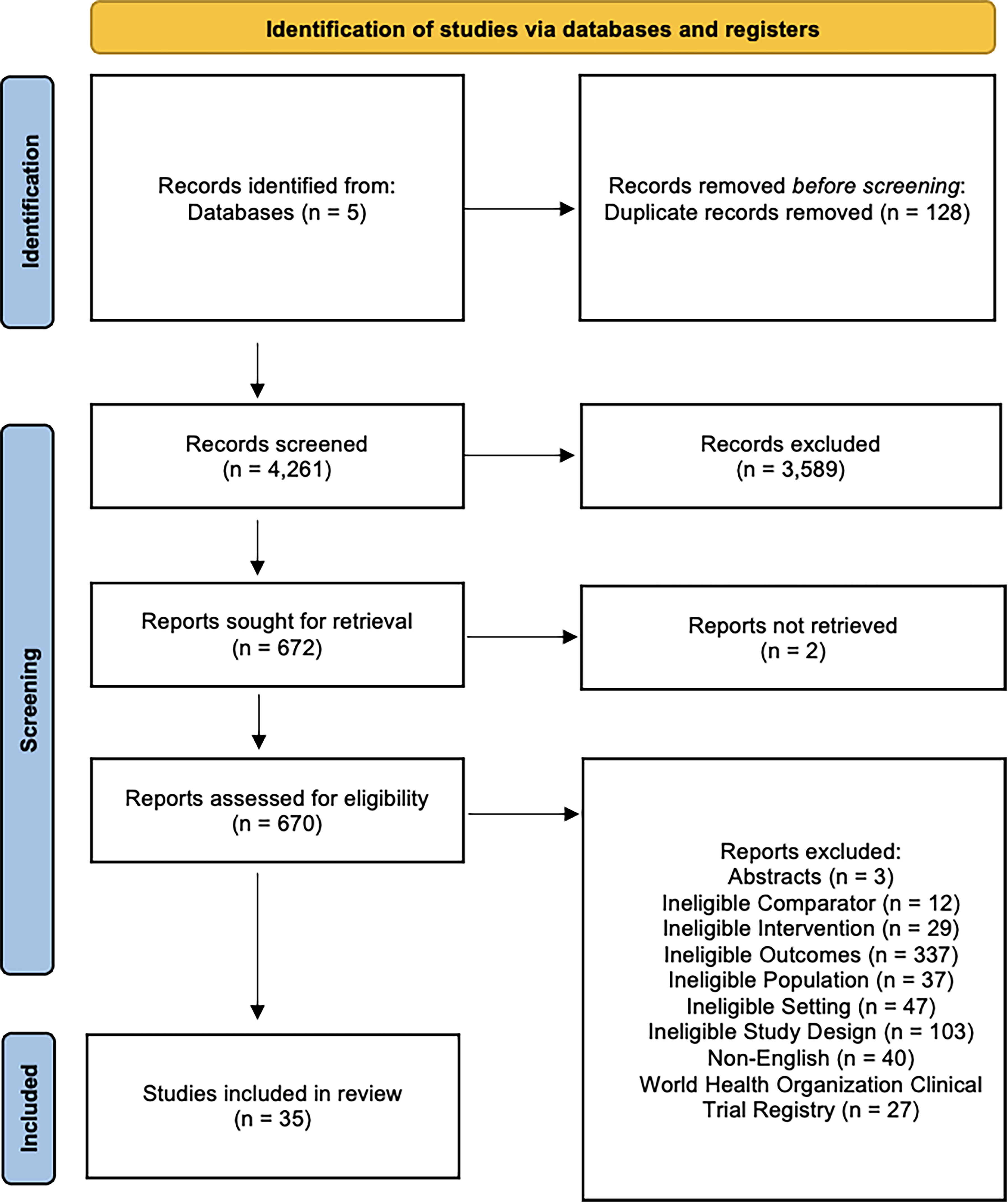
PRISMA flow diagram.
Study Characteristics
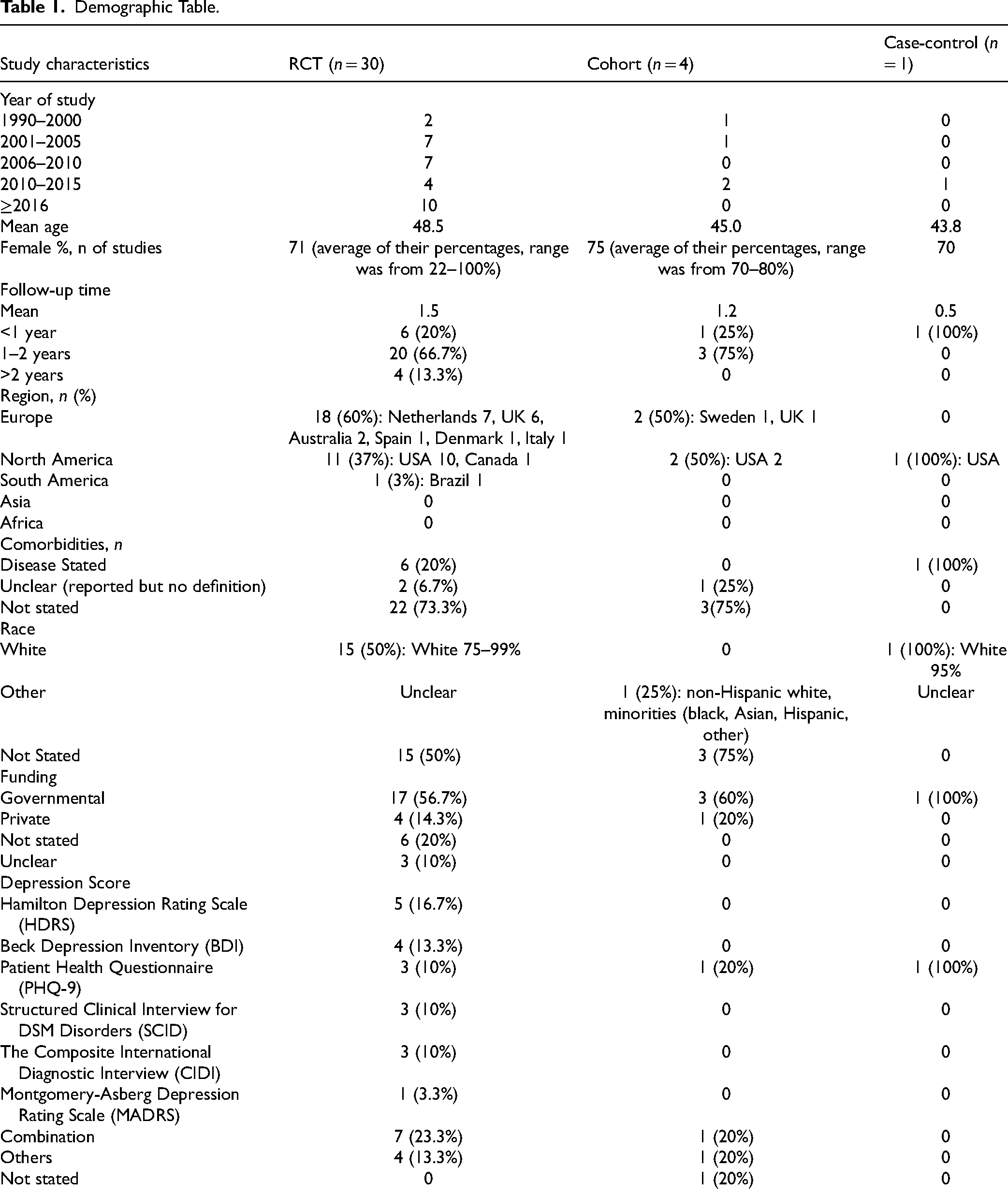
The 35 eligible studies were conducted in the USA (n = 13), the UK (n = 7), the Netherlands (n = 7), Sweden (n = 1), Australia (n = 2), Canada, Italy, Denmark, Spain, and Brazil (all n = 1).
Most studies included a majority of female participants, and adults of any age (mean ages 44–48 years) who identified as Caucasian. There were a variety of tools used to assess the outcomes of interest. Depending on the study, the presence and the severity of depressive symptoms were assessed through the Hamilton Depression Rating Scale (HDRS), Beck Depression Inventory (BDI), Patient Health Questionnaire (PHQ-9), Structured Clinical Interview for DSM Disorders (SCID), The Composite International Diagnostic Interview (CIDI), Montgomery-Asberg Depression Rating Scale (MADRS) or a combination of these tools. Of the studies excluded, 40 studies were in non-English language. The key characteristics of the studies are summarised in Table 1. Individual study characteristics are summarized in Table 2.
Demographic Table.
Individual Study Characteristics.

RCTs
Of the 35 included studies, 30 were RCTs. The majority of included studies evaluated psychological therapies: CBT;32–39 mindfulness-based cognitive therapy (MBCT);40–43 and interpersonal psychotherapy (IPT).44,45 The next largest group of studies evaluated pharmacologic therapies and methods; specific therapies;46–50 and method of therapy approach.51–56 There were also studies evaluating service-level programs such as prevention programs.57–59 Most of the comparators were “treatment as usual,” with some as “an active comparator” and a few interventions were compared to both, “active comparator” and “treatment as usual.” Follow-up times for the majority of the studies were between 1 and 2 years.
Observational Studies
We included 4 cohort studies and 1 case-control study. Included exposures were collaborative care management,60–62 method of therapy approach, 63 and mindfulness-based cognitive therapy. 64 Most of the controls were “treatment as usual”60–62,64 and 1 study included “active controls.” 63 Follow-up times for the majority of the cohort studies were between 1 and 2 years, with 6 months for the case-control study.
Risk of Bias
Overall, the reviewed studies were of sufficient quality to be synthesized in this review. Quality appraisal scores for RCTs ranged from 73% to 96%, except for 1 study that scored 69%. The quality appraisal scores for cohort studies ranged from 91% to 95%, and for the 1 case-control study quality score was 85%. Quality appraisal results are summarised in Details of included studies are shown in Supplement File 2.
Meta-Analysis
MDD relapse incidence rate:
MDD relapse incidence rate was meta-analyzed into the following subgroups:
Interventions
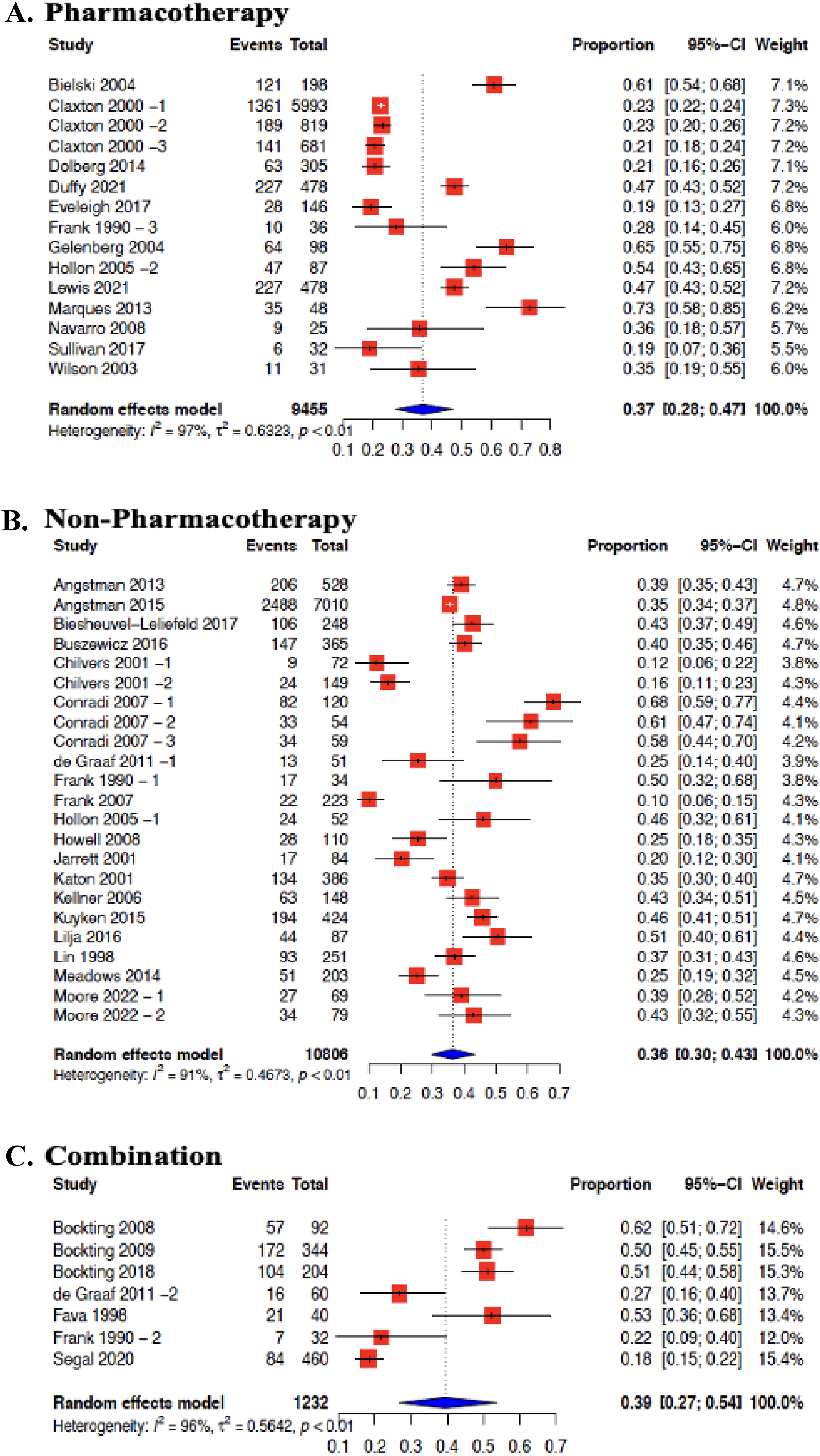
Incidence proportions were subgrouped into pharmacotherapy, non-pharmacotherapy and studies that included a combination of both group interventions. There were 13 studies that included pharmacotherapy that were meta-analyzed in this review (Figure 2 (A)). This resulted in an MDD relapse incidence rate of 37% (95% CI 28%–47%, I2 = 97%). Non-pharmacotherapies were reported in 19 studies, that were also meta-analyzed (Figure 2 (B)). These included studies showed an MDD relapse incidence rate of 36% (95% CI 30%–43%, I2 = 91%). Finally, 7 studies included a combination of both pharmacotherapy and non-pharmacotherapy interventions (Figure 2 (C)). These studies were meta-analyzed and resulted in an MDD relapse incidence rate of 39% (95% CI 27%–54%, I2 = 96%). There was “considerable heterogeneity” even after subgrouping by intervention. Pooling of MDD relapse incidence rate by specific intervention type was also done. However, this could only be done for CBT and MBCT interventions. The MDD relapse incidence rate for CBT was 42% (95% CI 32%–52%, I2 = 84%), and for MBCT was 32% (95% CI 20%–47%, I2 = 96%). There was “considerable heterogeneity” in these subgroups (Supplement File 3—Figure 4(A)).
Forest plot for MDD relapse incidence rate in primary care by intervention group: (A) pharmacotherapy; (B) non-pharmacotherapy; (C) combination.
Study design
Studies were also subgrouped according to study design. RCTs, including the different treatment arms within some included studies, were meta-analyzed. The MDD relapse incidence rate was 36% (95% CI 30%–42%, I2 = 93%). Cohort studies were also meta-analyzed to yield an MDD relapse incidence rate of 30% (95% CI 22%–40%, I2 = 98%). There was also “considerable heterogeneity” even after subgrouping by study design. (Supplement File 3—Figure 5(A)).
Length of follow-up
Incidence proportions were subgrouped according to length of follow-up of <1 year, 1–2 years, >2 years. The MDD relapse incidence rate for <1 year was 44% (95% CI 29%–62%, I2 = 96%). The MDD relapse incidence rate for 1- < 2 years was 31% (95% CI 26%–38%, I2 = 96%). And the MDD relapse incidence rate for ≥2 years was 41% (95% CI 32%–50%, I2 = 92%). There was “considerable heterogeneity” even after subgrouping by study design (Supplement File 3—Figure 6(A)).
Date of Study Publication
Incidence proportions were subgrouped according to the date of study publication. The MDD relapse incidence rate for studies published between 1990 and 2000, was 60% (95% CI 23%-39%, I2 = 88%). The MDD relapse incidence rate for; studies published between 2001 and 2005 was 37% (95% CI 24%-51%, I2 = 94%); studies published between 2006 and 2010 was 44% (95% CI 30%—60%, I2 = 94%); studies published between 2010 and 2015 was 35% (95% CI 23%-48%), I2 = 93%), and for studies published ≥2016 was 38% (95% CI 30%-46%, I2 = 93%). There was “considerable heterogeneity” in all subgroups (Supplement File 3—Figure 7(A)).
Study quality
To further explore heterogeneity, the incidence rate was pooled in studies that had a quality score of ≥85%. After pooling, the MDD relapse incidence rate was 37% (95% CI 30%–45%, I2 = 97%). There was “considerable heterogeneity” even after subgrouping by study quality (Supplement File 3—Figure 8(A)).
2.Effectiveness of therapies in MDD relapse:
MDD relapse prevention was meta-analyzed into the following subgroups:
Interventions
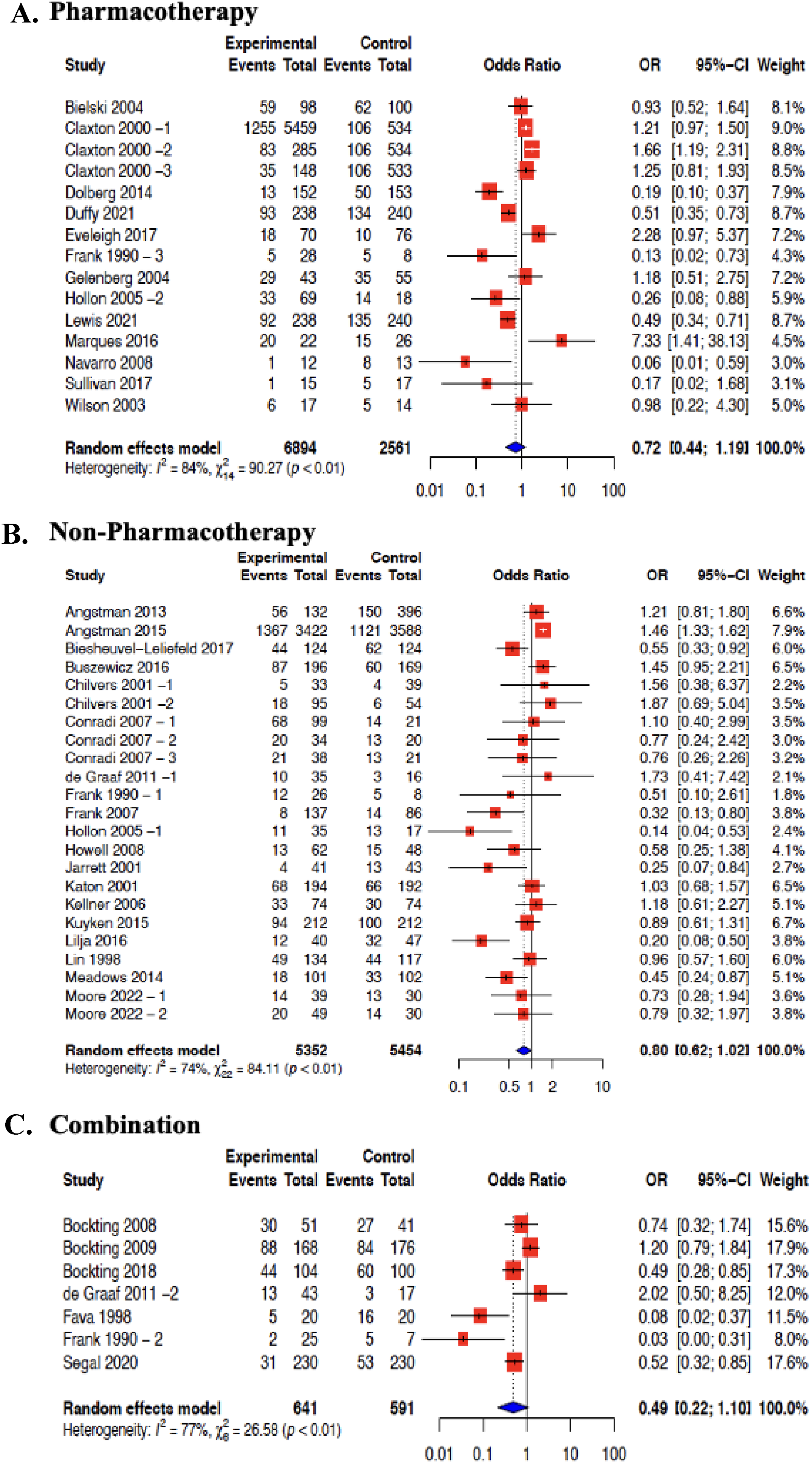
Effectiveness of pharmacotherapy interventions in 13 studies were meta-analyzed (Figure 3(A)). The average risk of MDD relapse was reduced by 28% (OR = 0.72; 95% CI 0.44 to 1.19, I2 = 84%). The effectiveness of non-pharmacotherapy interventions in 19 studies was also meta-analyzed (Figure 3(B)). The average risk of MDD relapse was reduced by 20% (OR = 0.80; 95% CI 0.62–1.02, I2 = 74%). The effectiveness of the combination of both pharmacotherapy and non-pharmacotherapy interventions was also meta-analyzed from 7 studies (Figure 3(C)). The average risk of MDD relapse was reduced by 51% (OR = 0.49; 95% CI 0.22–1.10, I2 = 77%) (Figure 3(A)). We also were able to meta-analyze studies that included a common intervention. CBT intervention effectiveness was pooled from 8 studies,32–39 and MBCT from 4 studies were meta-analyzed.40–43 All comparators were included within the same meta-analysis. Compared with all controls, the average risk of MDD relapse was reduced by 45% for CBT (OR = 0.55; 95% CI 0.30–0.99, I2 = 72%), and 35% for MBCT (OR = 0.65; 95% CI 0.45–0.94, I2 = 36%) (Supplement File 3—Figure 4 (B)).
Forest plot for prevention of MDD relapse in primary care by intervention group: (A) pharmacotherapy; (B) non-pharmacotherapy; (C) combination.
Study design
Studies were subgrouped according to study design and meta-analyzed. In RCTs, the MDD relapse was reduced by 44% (OR = 0.66, 95% CI 0.52–0.84, I2 = 69%). However, when cohort studies were meta-analyzed, the MDD relapse was not different between treatment and control groups (OR = 1.05, 95% CI 0.66–1.68, I2 = 79%). There was “substantial heterogeneity” in both groups (Supplement File 3—Figure 5(B)).
Length of follow-up
Studies were also subgrouped according to length of follow-up of < 1 year, 1–2 years, >2 years. The MDD relapse reduction was higher with longer follows. Studies with <1-year follow-up, OR was 0.92 (95% CI 0.42–2.00, I2 = 87%); 1 to <2 years follow-up, OR was 0.80 (95% CI 0.60–1.07, I2 = 77%); and ≥2 years follow-up, OR was 0.54 (95% CI 0.36–0.80, I2 = 69%). There was “considerable heterogeneity” even after subgrouping by study design. Heterogeneity was reduced from “substantial” to “moderate” as the follow-up period increased (Supplement File 3—Figure 6(B)).
Date of study publication
Further subgrouping was according to the date of study publication. The OR for MDD relapse for studies published between 1990 and 2000, was 0.6 (95% CI 0.24–1.49, I2 = 78%); for studies published between 2001 and 2005, OR was 0.74 (95% CI 0.43–1.25, I2 = 58%); for studies published between 2006 and 2010, OR was 0.78 (95% CI 0.55–1.12, I2 = 44%); for studies published between 2010 and 2015, OR was 1.01 (95% CI 0.45–2.24, I2 = 89%); and for studies published ≥2016, OR was 0.63 (95% CI 0.44–0.90, I2 = 72%). Heterogeneity varied from “moderate” to “substantial” (Supplement File 3—Figure 7(B)).
Study quality
To explore heterogeneity even further, OR of MDD relapse was pooled in studies that had a quality score of ≥85%. After pooling, the MDD relapse OR was 0.87 (95% CI 0.66–1.16, I2 = 81%). There was “considerable heterogeneity” even after subgrouping by study quality (Supplement File 3—Figure 8 (B)).
Discussion
This review was based on 35 studies, including 30 clinical trials, 4 cohort studies, and 1 case-control study. Overall, the studies were of high methodological quality according to the JBI Checklist. Some studies (27 studies) reported relapse of depression in primary care as the main outcome, while others (9 studies) reported it as a secondary or tertiary outcome. The included studies encompassed a variety of pharmacological and non-pharmacological interventions and exposures, differing in their source of primary care population, methods, and quality.
Our aim was to measure the MDD incidence rate in primary care and effectiveness of therapies to prevent relapse. Subgrouping according to intervention group of pharmacotherapy, non-pharmacotherapy, and combination therapy, demonstrated an MDD relapse incidence rate of these subgroups as 37%, 36%, and 39% respectively. Heterogeneity varied within each subgroup. Our review indicated a decrease in MDD relapse with therapy, as pharmacotherapy, non-pharmacotherapy, and a combination of both therapies were shown to reduce MDD relapse in primary care (28%, 20%, and 51% decrease, respectively). The meta-analysis also demonstrated that specific psychological interventions (MBCT, CBT) delivered to adults with depression may reduce the risk of experiencing relapse by 34–40%, with moderate to substantial heterogeneity. 28 Reasons for heterogeneity might be clinical (variability in the participants, interventions), methodological (outcome measurement tools), statistical (consequence of clinical or methodological diversity, or both). 28
To facilitate analysis and explore heterogeneity, we presented the data in detail, and pooling results into different subgroups of intervention groups, study design, length of follow-up, study publication date, and studies that had a quality score of ≥85%.
Numerous reviews have investigated depression relapse, but only a handful have specifically focused on depression within a primary care context. To the best of our understanding, a single review conducted by Gili et al. 19 delved into depression relapse in primary care. This review recognized a small subset of studies targeting relapse prevention in primary care samples, indicating insignificant effect sizes for relapse. However, it limited its scope to RCTs reported until January 2014. In contrast, our research includes more recent studies and observational methodologies.
There have been other reviews studying depression relapse without specifically concentrating on primary care environments. Two reviews explored non-pharmacological interventions for depression relapse,7,15 yielding findings consistent with ours. Zhou et al. 7 identified psychotherapy as effective in preventing relapse, while Clarke et al. 15 suggested that psychological therapies might mitigate the risk of depression relapse after 1 year. Another review concentrated on risk factors for depression relapse, 12 finding childhood maltreatment, residual symptoms, history of recurrence, existing or past comorbid anxiety disorders, and rumination as potential relapse predictors. Furthermore, 1 study examined risk factors contributing to increased relapse following cognitive-behavioral therapy for depression, 65 identifying residual depressive symptoms and previous episodes as significant predictors. Another review showed that the impact of continuous antidepressant medication 66 had a consistent effect on relapse prevention, while another reviewed the sequential combinations of pharmacotherapy and psychotherapy, 67 linking it to reduced relapse risk. Unlike these preceding reviews, our study prioritizes depression relapse in a primary care context and does not restrict inclusion to clinical trials only.
Strengths and Limitations of This Review
Our review was conducted in accordance with PRISMA recommendations, 20 and possesses several methodological strengths. Firstly, we pre-registered a protocol to promote consistent conduct by the study team and ensure accountability and transparency of the completed review. Additionally, we conducted a comprehensive search of literature databases without focusing on specific interventions, ensuring all interventions within our inclusion criteria were captured. Two independent researchers scanned titles, abstracts, and full texts of studies for inclusion. 68 We used a validated critical appraisal tool, the JBI, to assess study quality. The majority of included studies were deemed high quality by our team.
However, our study has some limitations. The generalizability of these findings might be affected for various reasons. Firstly, the reviewed studies’ samples varied in participant numbers and clinical conditions and comorbidities. Most studies excluded patients with other psychiatric diseases, personality disorders, and alcohol and drug abuse, but many did not state the possible comorbidities of the included patients. If comorbidities were mentioned, they were often not clearly defined (study characteristics table). Moreover, while participants were all from primary care setting, most studies did not specify what constituted primary care (study characteristics table). Populations in included studies might have presented with comorbidities as they were primary care patients, potentially modifying the association between depression relapse and specific interventions and exposures. Exploring effect modification was beyond the scope of this study. Furthermore, we only included English-language studies, which might affect generalizability. However, only 6% of the full-text studies were non-English, and others have reported that excluding non-English studies does not substantially influence results. 69
Another limitation is the lack of uniformity and definition of diagnosis and tools used to identify depression relapse across studies, which may introduce bias. There is a lack of uniformity and reliability in depression measurement scales used in clinical practice, potentially causing bias. 70 Our review included a variety of tools to assess MDD relapse and therapy effectiveness in preventing relapse. Nevertheless, all included studies clearly specified the measuring tools used to assess the outcome and how it was captured.
It is important to mention that some of the included studies were not specifically designed to quantify depression relapse (9 studies), however, relevant data from these studies were included in our review and meta-analysis. Moreover, while statistical heterogeneity was observed in the meta-analysis, it is important to acknowledge that a portion of this variability may stem from clinical heterogeneity across studies. Differences in participant characteristics, intervention protocols, and outcome measurement methods likely contributed to variations in effect sizes. This can be seen in the summary of individual study characteristics in Table 2. These clinical differences, while contributing to statistical heterogeneity, provide valuable insights into the potential influence of real-world variations on the observed intervention effects. 28
Implications for Future Research
This review highlights significant concerns that future research should consider. More data should be specified in research on depression relapse when conducting clinical or observational trials. Our review revealed that most included studies did not specify comorbidities in included patients, standard depression relapse definitions, time to relapse, and adjustment of covariates and confounders in reporting estimates (particularly in observational studies). Understanding the role of these factors could improve our knowledge of depression relapse in primary care. Moreover, our review indicated a scarcity of well-designed studies, specifically observational studies, with long follow-up times to study depression relapse in primary care. Additionally, most studies included a majority of Caucasian participants. Future clinical trials should involve racialized communities to determine if there are outcome differences based on race. These findings highlight the potential of combination therapy, encompassing pharmacological and non-pharmacological approaches, as an effective strategy to prevent relapse in MDD. While current evidence supports its efficacy, practical implementation in primary care requires careful consideration of factors such as resource availability and individual patient preferences which may influence the feasibility of implementing combination therapies in primary care. Clinicians can draw on these results to guide decisions.
Conclusion
This review aimed to synthesize the best available evidence regarding MDD relapse incidence rate and the effectiveness of pharmacological and nonpharmacological therapies in adult patients in a primary care setting. Our findings indicate that various interventions could be used for MDD relapse in primary care, with pharmacotherapy, non-pharmacotherapy and a combination of showing preventive effects. Further research into specific pharmacological and non-pharmacological therapies, separately or in combination, with longer follow-up durations, is necessary to understand the long-term impact of these interventions on MDD relapse in primary care.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437251322401 - Supplemental material for Incidence of Major Depressive Disorder Relapse and Effectiveness of Pharmacologic and Psychological Interventions in Primary Care: A Systematic Review and Meta-Analysis: Incidence de la rechute du trouble dépressif majeur et efficacité des interventions pharmacologiques et psychologiques en soins primaires : revue systématique et méta-analyse
Supplemental material, sj-docx-1-cpa-10.1177_07067437251322401 for Incidence of Major Depressive Disorder Relapse and Effectiveness of Pharmacologic and Psychological Interventions in Primary Care: A Systematic Review and Meta-Analysis: Incidence de la rechute du trouble dépressif majeur et efficacité des interventions pharmacologiques et psychologiques en soins primaires : revue systématique et méta-analyse by Waseem Abu-Ashour, Stephanie Delaney, Alison Farrell, John-Michael Gamble, John Hawboldt and Joanna E. M. Sale in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437251322401 - Supplemental material for Incidence of Major Depressive Disorder Relapse and Effectiveness of Pharmacologic and Psychological Interventions in Primary Care: A Systematic Review and Meta-Analysis: Incidence de la rechute du trouble dépressif majeur et efficacité des interventions pharmacologiques et psychologiques en soins primaires : revue systématique et méta-analyse
Supplemental material, sj-docx-2-cpa-10.1177_07067437251322401 for Incidence of Major Depressive Disorder Relapse and Effectiveness of Pharmacologic and Psychological Interventions in Primary Care: A Systematic Review and Meta-Analysis: Incidence de la rechute du trouble dépressif majeur et efficacité des interventions pharmacologiques et psychologiques en soins primaires : revue systématique et méta-analyse by Waseem Abu-Ashour, Stephanie Delaney, Alison Farrell, John-Michael Gamble, John Hawboldt and Joanna E. M. Sale in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-3-cpa-10.1177_07067437251322401 - Supplemental material for Incidence of Major Depressive Disorder Relapse and Effectiveness of Pharmacologic and Psychological Interventions in Primary Care: A Systematic Review and Meta-Analysis: Incidence de la rechute du trouble dépressif majeur et efficacité des interventions pharmacologiques et psychologiques en soins primaires : revue systématique et méta-analyse
Supplemental material, sj-docx-3-cpa-10.1177_07067437251322401 for Incidence of Major Depressive Disorder Relapse and Effectiveness of Pharmacologic and Psychological Interventions in Primary Care: A Systematic Review and Meta-Analysis: Incidence de la rechute du trouble dépressif majeur et efficacité des interventions pharmacologiques et psychologiques en soins primaires : revue systématique et méta-analyse by Waseem Abu-Ashour, Stephanie Delaney, Alison Farrell, John-Michael Gamble, John Hawboldt and Joanna E. M. Sale in The Canadian Journal of Psychiatry
Supplemental Material
sj-pptx-4-cpa-10.1177_07067437251322401 - Supplemental material for Incidence of Major Depressive Disorder Relapse and Effectiveness of Pharmacologic and Psychological Interventions in Primary Care: A Systematic Review and Meta-Analysis: Incidence de la rechute du trouble dépressif majeur et efficacité des interventions pharmacologiques et psychologiques en soins primaires : revue systématique et méta-analyse
Supplemental material, sj-pptx-4-cpa-10.1177_07067437251322401 for Incidence of Major Depressive Disorder Relapse and Effectiveness of Pharmacologic and Psychological Interventions in Primary Care: A Systematic Review and Meta-Analysis: Incidence de la rechute du trouble dépressif majeur et efficacité des interventions pharmacologiques et psychologiques en soins primaires : revue systématique et méta-analyse by Waseem Abu-Ashour, Stephanie Delaney, Alison Farrell, John-Michael Gamble, John Hawboldt and Joanna E. M. Sale in The Canadian Journal of Psychiatry
Footnotes
Abbreviations
Availability of Data,Code,and Other Materials
Available through contacting corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.