
Abstract
Objective
The implementation of Integrated Youth Services (IYS) can help ensure that youth are adequately supported. The objective of this analysis was to provide a model for the planning and costing of IYS throughout Canada over a 15-year period.
Methods
To estimate resource allocation for IYS, we determined the number of hubs and hub staffing requirements by service level and jurisdiction, backbone support and infrastructure requirements by jurisdiction. A needs-based analytic framework for planning was employed to estimate the number of hubs required. The optimal mix of hub staffing requirements was determined based on prior literature. The costs of running each hub were estimated using publicly available data and internal documents from existing IYS agencies. Finally, the cost of setting up IYS hubs, IYS virtual care and respective backbone support throughout Canada was estimated and projected over 15 years and the cost-savings of IYS were calculated.
Results
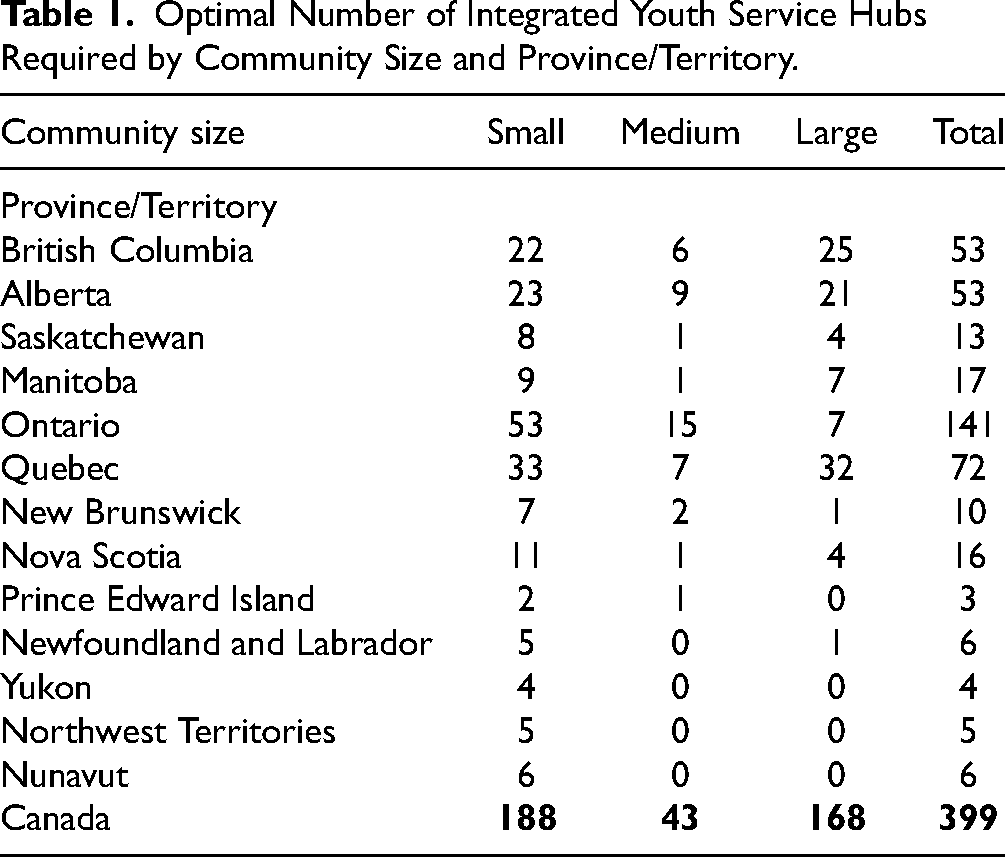
At maturity, it was estimated that 399 hubs—188 small, 43 medium, 168 large—across Canada would be required to address youth mental health and substance use needs. The cost of implementing IYS initiatives across Canada would vary between $4,349,126 (for less populous jurisdictions) and $248,950,524 (for more populous jurisdictions), for a total annual cost of $676,633,388 (excluding costs of infrastructure). It was estimated that the implementation of IYS hubs would lead to cost-savings of $2.1 billion annually and have the potential to be cost-effective.
Conclusion
The implementation of IYS hubs can provide good value for money, in the form of high client satisfaction, earlier supports with improved youth outcomes and decreased health care costs. Future work should address gaps in data availability on mental health and substance use-related needs of youth with neurodevelopmental disorders, youth experiencing homelessness, youth in congregate living and foster care, and Indigenous youth.
Introduction
Mental health and substance use (MHSU) problems commonly emerge in adolescence and early adulthood,1,2 providing critical opportunities for early detection and intervention at these key developmental stages.1,3 Roughly 20% of Canadian youth experience MHSU disorders; despite effective treatments, only 22–30% receive help.4–6 Few youth receive timely access to services due to long wait times, and fewer receive a full course of effective treatment.3,7,8 Barriers to receiving care include fragmented services and systems, lack of developmentally and culturally appropriate services, over-emphasis on illness-based and medical models, and services that fail to consider preferences and perspectives of youth and families.3,8,9 Moreover, barriers and inequities have been exacerbated by the impact of the COVID-19 pandemic on health systems. Inadequately addressed MHSU problems in adolescence and early adulthood translate to poor adult health and worse social and economic outcomes, with great personal, family and societal costs.1,10 Accordingly, there is an urgent need for targeted efforts to significantly improve youth MHSU service integration, quality and outcomes.
In the mid-2000s, significant youth MHSU system reform was initiated globally with the introduction of headspace and Orygen Youth Health in Australia, Jigsaw in Ireland, Forward Thinking Birmingham in the United Kingdom, and One Stop Shops in New Zealand.3,8,9 Efforts to develop Integrated Youth Services (IYS) have also been initiated throughout Canada. Services include MHSU health care interventions, primary care, youth and family peer supports, culturally specific wellness services, care navigation, education, employment and training support, and other community and social supports, as well as other services as identified by community need. Services are brought together into an integrated service delivery model, grounded in a commitment to address historical system deficits through, for example, providing ready access to developmentally appropriate evidence-based or evidence-generating services through the transition to young adulthood (See Lancet Psychiatry Commission on Youth Mental Health, McGorry et al., 2024 for a comprehensive discussion of the model). IYS target youth with a range of needs but MHSU health service components typically include early intervention services and services for youth with identified needs not yet connected to specialized treatments. Additionally, prevention and health promotion services and specialised services may be offered within IYS settings depending on community resource availability and local system planning. Accordingly, IYS services generally align with tiers 2 and 3 of the Canadian National Treatment Strategy's tiered model of prevention and treatment services, with some reach into tiers 1 and 4. 11 Currently, all provinces/territories have developed or are considering developing an IYS network or approach. Moreover, the Canadian Institutes of Health Research have identified IYS as a key element of youth MHSU system transformation 12 and recently announced a $59 million investment in supporting IYSs to operate as Learning Health Systems. 13 Given the expanding role of IYS in youth MHSU health system transformation, it is important to understand what would be required to address youth MHSU concerns by making IYS available throughout Canada. To date, there has been an absence of modeling to demonstrate the number of IYS centres required to meet the MHSU needs of youth in each province/territory. Similarly, cost estimates of running hubs are lacking.
The goal of this study was to propose an IYS Pan-Canadian Planning Model (IYSPPM) and provide an overview for planning and costing IYS throughout Canada over a 15-year period by considering available data on youth population needs in Canada and existing evidence from Canadian and international contexts.
Methods
Setting and Study Design
The development of the IYSPPM occurred over six months through extensive examination of Canadian and international evidence, consultation with 12 key informants across six organisations/initiatives, review of available IYS administrative data, and internal and external reports from multiple Canadian IYS initiatives. Several factors should be considered regarding resource allocation: population to be served, number of individuals at risk for a given condition, level of service planned and productivity of inputs (i.e., staff/professionals). The IYSPPM uses prevalence of unmet need, community size, level of IYS service (or hub size), productivity of IYS hubs by level of service, required workforce inputs to deliver IYS to youth and families, infrastructure required for service delivery and workforce required to provide implementation.
Analysis
Determining the Number of Hubs Required
Based on a previous needs-based model for resource planning in radiation oncology
14
and using the workforce planning framework by Birch and colleagues, which incorporates population health needs, levels of service to respond to health needs, and provider productivity to determine future requirements of levels and mix of healthcare providers,
15
a needs-based assessment for IYS hubs in each province/territory was performed. The number of hubs required was calculated, using the following formula, which describes current need of hubs (N) as a function of the size of the population (P) multiplied by three factors that relate population to need:

Statistics Canada 2021 Census data were used to determine P, the youth population aged 12–25 years old by province/territory. 16 Community size—defined as small (population between 1,000 and 29,999), medium (population between 30,000 and 99,999) and large urban (population of 100,000 or more)—was incorporated into the model to ensure IYS service planning reflected differences in the distribution of the youth population across urban and rural centres of various sizes. The proportion of the total population for each community size within each province/territory was then used to estimate the proportion of the youth living in each community.
H, level of health (or illness) in the population, was defined as the number of youth with unmet need for service. This approach, as opposed to using prevalence data of mental health disorders, has the benefit of reflecting existing adequate service utilisation. H/P reflects the percent of individuals with unmet need for service. This value was estimated separately for MH- and SU-related needs using data from the Canadian Community Health Survey 17 and prior existing work,4–6,18–23 and added to estimate total unmet need for service. Further information can be found in the Appendix.
Q represents the quantity of services delivered, while Q/H represents the quantity of service provided for a specific health state. For IYSMPP, Q/H represents a planning goal—the targeted quantity of service to be provided to youth with unmet need. Given the multifactorial drivers of youth contact with service even when perceived unmet needs are present, IYSMPP estimates Q/H to be 65% for in-person services and 10% for virtual services, for a total initial target of service contact of 75% in the first 15 years, reflecting continued non-engagement in service for some youth with unmet needs, and alternative services sought by other youth. These estimates were based on Canadian and international MHSU system planning initiatives.24–29 Further information can be found in the Appendix.
To account for service level by community size (i.e., small, medium, large), values of Q/N were estimated for different hub sizes. These values were calculated based on the median of a range of actual and target volumes at Foundry British Columbia and Youth Wellness Hubs Ontario (YWHO) in communities of varied sizes, and data from headspace 30 and Jigsaw. 31 Ranges and medians can be found in Appendix Table A1. Virtual service modelling was guided by evidence gathered from Foundry internal documents. The resource requirements were then expressed as hub service level equivalents, for ease of comparison to in-person resource estimates (see Appendix Table A2 for these values).
Determining the Hub Staffing/Workforce Requirements
Understanding the optimal mix of staff is crucial to ensure efficient resources use. To determine this, a rapid review of existing youth mental health models of care was undertaken. Two scoping reviews,8,9 a review in World Psychiatry, 3 publicly available documents from Foundry, YWHO, ACCESS Open Minds (Canada), headspace (Australia), Orygen (Australia), Jigsaw (Ireland), and internal documents from ACCESS Open Minds, Foundry, and YWHO were used for this purpose.
Estimating the Costs of Operating Hubs
To estimate the costs of running each hub, publicly available data on compensation rates for required roles and internal documents from Foundry and YWHO, annual staffing costs were determined (see Appendix Table A3). Additionally, 25% non-labour expenses were estimated to cover operating costs. The backbone/central office organisation is responsible for successful implementation of the IYS model. The costs of setting up these organisations include both labour (i.e., staff expenses) and non-labour (i.e., operating/administration expenses, data system subscription expenses) costs. Backbone/central office organisations should be in place 18–24 months before hub development and implementation begins. Currently, only British Columbia (BC), Ontario and Manitoba have backbone/central office organisations in place. The costs of backbone/central office organisations were based on existing values from YHWO (backbone/central office) and by pro-rating the cost of running each organisation by the number and size of IYS hubs they support. Projections were made at the 5-, 10- and 15-year mark to understand how implementing hubs and virtual services would occur over time.
In-person IYS hubs require spaces that are large enough to facilitate integration of a range of services, can accommodate primary care services and are amenable to youth-friendly service delivery. Using Foundry internal documents, capital costs for construction (only) were calculated at $348/sq. ft (this excludes costs of furniture and appliances [average $216,000], primary care equipment, technology, signage, or professional fees like interior design, architectural, geotechnical, permits etc.). The estimated capital costs for in-person hubs by level of service/hub size can be found in Appendix Table A4.
Estimating the Cost-Savings of the IYSPPM
According to ACCESS Open Minds, 32 on average, for every $1 invested, mental health prevention and early intervention programs can lead to reductions in health care costs of $1,985 in hospitalisations, $38 in emergency department visits, $604 in outpatient clinic services, $429 in specialist services, $47 in general practitioner visits, $1,263 in public residential services and $107 in prescription drugs per patient per year, when comparing individuals who received mental health prevention and early intervention programs to those who did not. Based on this, the cost-savings of implementing the IYSPPM were estimated, assuming these would be constant over time, and across IYS in-person and virtual models, when all IYS hubs are operating at full capacity across the country.
All costs were inflated to 2021 Canadian dollars (CAD) using Statistics Canada's consumer price index for health and personal care. 33
Results
Number of Hubs Required
The total number of hubs required to meet 75% of unmet MHSU needs of youth aged 12 to 25 years old was determined to be 399 across Canada. The number of hubs per province/territory ranged from a low of 3 (Prince Edward Island) to a high of 141 (Ontario) (see Table 1).
Optimal Number of Integrated Youth Service Hubs Required by Community Size and Province/Territory.
Hub Staffing/Workforce Requirements
Based on prior work and existing data,3,8,9,30–32,34 each hub should have the following staff mix to optimally deliver youth programs at maturity (hubs would likely reach this configuration by the 3rd year post-implementation): hub/centre/program manager, clinical supervisor, outcomes administrative assistant, social worker/therapist/mental health addiction clinician, clinical care coordinator/navigator, psychiatrist, psychologist, family physician, nurse practitioner, peer support worker, Indigenous health worker, family peer support worker and youth outreach worker. The percentage of time required of each professional (i.e., the full time equivalent, FTE) will differ depending on the size of the hub (service level), which is reflective of community size; see Appendix Table A5 for the proposed FTE% for each hub type.
Costs of Operating Hubs
The costs to operate hubs vary by service level and ranged from $624 thousand/year for an extra-small hub to $1.9 million/year for a full-size hub at maturity. Appendix Table A6 provides annual service costs of virtual care by province/territory and virtual care IYS hub service equivalents. It was estimated that the annual cost of each backbone/central office organisation would vary between $579,600 (for provinces/territories with fewer than 7 hubs) and $6,641,250 (for provinces with more than 100 hubs; not shown). Building upon the core backbone/central office for in-person services, virtual care IYS services require additional dedicated staff with technical skills, operational, and competencies profiles required to support the level of service/size of the virtual care operations. Annual costs were estimated at $601,650 and $1,508,050 for smaller and larger virtual care IYS teams, respectively. Combining the cost of setting up IYS hubs, IYS virtual care and the respective backbone/central office organisations, it was estimated that the cost of implementing IYS initiatives across Canada by full implementation would vary between $4,349,126 (for less populous jurisdictions) and $248,950,524 (for more populous jurisdictions), for a total of $676,633,388 (see Table 2).
Combined Estimated Cost of In-person and Virtual Hub Services, Operations, and Backbone/Central Office Supports.
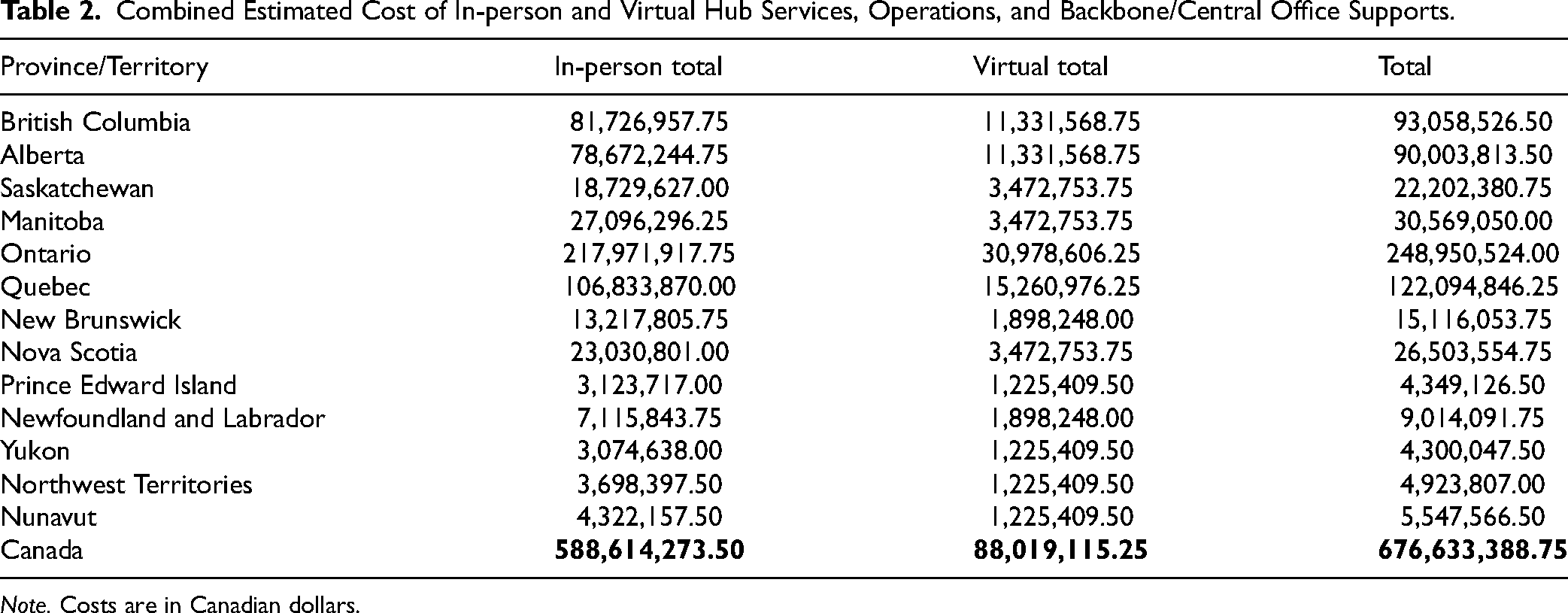
Note. Costs are in Canadian dollars.
At the time of the analysis, there were approximately 80 hubs in operation and one province-wide virtual IYS service (Foundry Virtual) being offered in Canada. The number of hubs implemented over time can be found in Figure 1; the costs of in-person and virtual IYS service and backbone/central office supports at the 5-, 10- and 15-year marks can be found in Table 3. This investment would serve 223,190 unique youth annually after 5 years, 342,342 unique youth annually after 10 years and 462,050 unique youth annually 15 years. After 5 years, there would be backbone/central offices in all provinces/territories with a total of 158 community based hubs and virtual services at an annual cost of $331.7 million; after 10 years, there would be 278 hubs at an annual cost of $505.3 million; and after 15 years (i.e., at full maturity), 399 hubs, 13 backbones/central offices and 13 virtual services at an annual cost of $676.6 million. The average cost of per youth served would be $1,475.
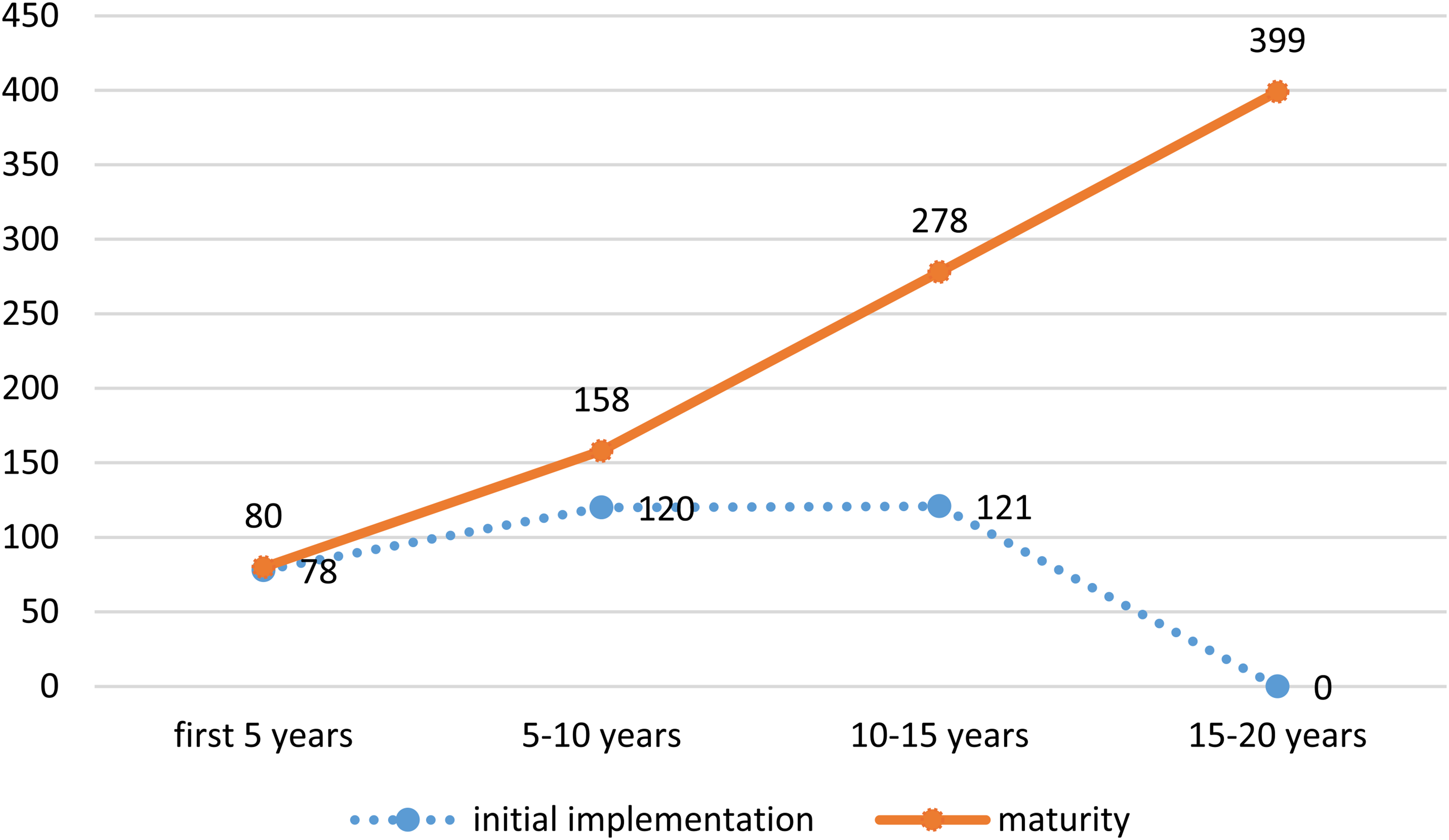
Number of in-person integrated youth service hubs in the stages of initial implementation and maturity over 5-year time blocks.
Costs of Operations and Backbone/Central Office Supports of Integrated Youth Service Services Over Time.

Note. Costs are in Canadian dollars.
Cost-Savings of the IYSPPM
At full capacity, it is estimated that mental health prevention and early intervention programs would produce cost-savings of $2,138,897,510.77 in avoided unnecessary health services/year across Canada (see Table 4).
Total Cost-Savings Associated With the Implementation of Integrated Youth Services Over Time.
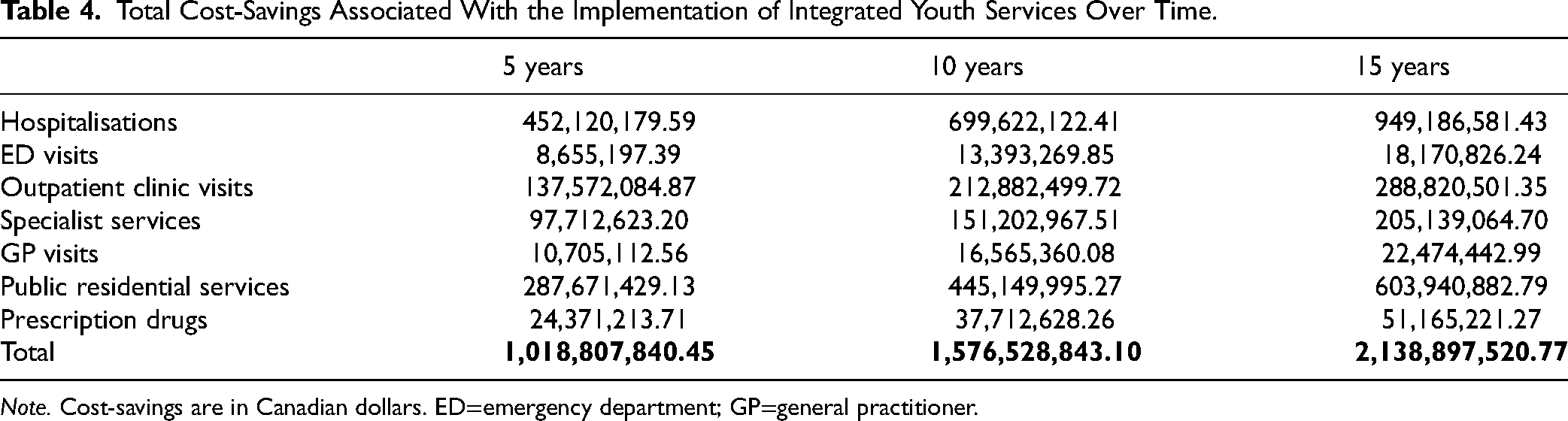
Note. Cost-savings are in Canadian dollars. ED=emergency department; GP=general practitioner.
Discussion
To date, there has been an absence of evidence around the planning and costing of a pan-Canadian IYS model. Based on a workforce planning framework and considering the optimal staff mix required, it is estimated that, in a best-case scenario, 399 hubs are required to address 75% of unmet youth MHSU needs across Canada. The costs to operate hubs by service level ranged from $624 thousand/year for an extra-small hub to $1.9 million/year for a full-size hub at maturity. These estimates align with reported costs of other IYS centres at full implementation, such as Jigsaw (Ireland) at $1,415,000 CAD (€1,000,000 in 2013) 34 and headspace (Australia) at $1,105,000 CAD ($1,200,000 AUD in 2015). 35 Combining the cost of setting up hubs, providing virtual care, and respective backbone/central office organisations (excluding infrastructure), implementing IYS initiatives across Canada will cost $676,633,388. This investment would serve 223,190, 342,342, and 462,050 unique youth after 5, 10, and 15 years, annually, respectively. At maturity, IYS hubs would produce cost-savings of $2.1 billion/year, suggesting, at minimum, an annual return on investment of $2 for every $1 invested. Prior research has shown that prevention and early intervention for mental health care programs, such as IYS, can produce cost-savings (i.e., lead to a reduction of costs by reducing unnecessary/avoidable care) and provide a return on investment between $2 and $10.3,36–38 Furthermore, some youth prevention programs have been found to be cost-effective (i.e., provide a demonstrable effect worth the investment made).39,40
Mental health prevention and early intervention programs, such IYS, can also provide value for money, that is, provide utility from every purchase/sum of money spent. The concept of value for money can be easily understood as “not paying more for a good/service than its quality or availability justify.” In relation to public spending, it implies a concern with economy (cost minimisation), efficiency (output maximization) and effectiveness (full attainment of intended results), though it must also support equity. Thus, in addition to examining the financial return on investment, it is important to understand other outputs provided by these programs. Youth One Stop Shops (New Zealand), Your Choice (New Zealand), Kapiti Youth Support (New Zealand), headspace (Australia), Jigsaw (Ireland), Foundry BC (Canada), ACCESS Open Minds (Canada), YWHO (Canada), @ease (Netherlands) and Community Health Assessment Team (CHAT) (Singapore) have been shown to provide many benefits for youth, such as timely access to services,3,36,37,41 provision of inclusive services,3,36,41 high levels of satisfaction with services and relationships with staff and environment,3,35,38,41 improved outcomes (e.g., reduced distress, improved mental health) and quality of life,3,36,41,42 and positive experiences with virtual care. 43 Moreover, there are benefits for providers, such as reduced burnout and greater work satisfaction.41,44 Overall, this analysis and existing evidence suggest that implementing IYS hubs can provide good value for money, in the form of decreased health care utilisation and costs but also high client satisfaction and earlier supports with improved youth outcomes.
Nonetheless, this analysis is not without limitations. Inputs used to determine unmet MHSU needs were obtained from the Canadian Community Health Survey, 17 which excludes individuals living on reserves, in some northern and/or remote communities, and in the territories, where substantial Indigenous populations reside. Several groups may have also been excluded due to their English/French language skills, living arrangements, access to communication devices and/or other factors. There is also potential underrepresentation of youth with neurodevelopmental disorders. Moreover, CCHS is based on self-report but was used because comprehensive point of contact utilisation and outcome data from existing models of care are largely unavailable. Finally, inputs were collected prior to the COVID-19 pandemic; evidence demonstrates significant negative impacts on youth MHSU since then. 9 There is much still to be learned to tailor IYS to respond to youth needs in varied contexts, including rural, remote, northern and Indigenous contexts. Moreover, IYS operate as learning health systems and while some associated costs, for example, hub level outcome assistant, backbone evaluation positions, and data systems have been considered, the full costs and savings associated with operating as a learning health system over time have not been included. Thus, the current estimates likely underestimate youth IYS-related needs. Additionally, this analysis does not capture the needs of all youth experiencing significant MHSU concerns, only those who identified needing service and experiencing at least some unmet needs. It is likely there are youth experiencing significant concerns who would not identify as needing service, though they would benefit from such. It is also possible this analysis includes youth who perceive themselves to need these services but would not meet criteria for significant MHSU concerns using standardized screening or assessment measures. Additionally, variability in the quantity of services provided for a specific health state and need complexity at presentation were not considered. This analysis does not capture youth not covered by the public health care system, such as newcomers/refugees and out-of-country post-secondary students. Lastly, the IYS service model assumes primary health care is available to youth; however, it does not consider unmet need for primary care services due to data limitations. Taken together, these considerations suggest that the potential IYS demand is likely underestimated, and the estimated number of hubs is a minimum required as it would only address 75% of youth's unmet need. The FTE staffing values were based on data from IYS initiatives in BC and Ontario; thus, these values may not be representative of the entire country. The cost-saving estimates are based on a single site from Alberta and may not be representative of other Canadian sites. Furthermore, while it is important to understand where hubs should be physically located to ensure maximum reach and equitable access to services, this was not addressed in this work. Additionally, it is important to note that workforce estimates do not include in-kind contributions from partner organisations who deliver services through IYS. The significant system-building roles IYS hubs and backbones/central offices have in the broader health system are also not captured. Future work should address these shortcomings, paying attention to gaps in data availability on MHSU-related needs of youth with neurodevelopmental disorders, youth experiencing homelessness, youth in congregate living and foster care, and Indigenous youth.
In sum, there is great need for more and better MHSU services for youth and their families across Canada, which has only increased and become more complex since the pandemic. IYS models have been effective in improving access to care and producing positive outcomes for youth in Canada and internationally. Evidence suggests IYS in Canada provide high client satisfaction, improved youth outcomes and decreased health care utilisation, and can lead to cost-savings of $2.1 billion at full capacity. The opportunity cost of not investing in IYS includes financial losses due to unnecessary medical costs and the missed opportunity to implement broader system improvement and change, and the IYS values of equity, inclusion and youth and family engagement. More importantly, delays in implementing IYS models nationally will exacerbate the access and quality issues that currently exist, potentially adding to youth and families heightened and prolonged distress that could have lifelong impacts with large personal, family and societal costs.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241301008 - Supplemental material for The Implementation of Integrated Youth Services in Canada: Planning and Costing of a Pan-Canadian Model: La mise en œuvre des services intégrés pour les jeunes au Canada : planification et établissement des coûts d’un modèle pancanadien
Supplemental material, sj-docx-1-cpa-10.1177_07067437241301008 for The Implementation of Integrated Youth Services in Canada: Planning and Costing of a Pan-Canadian Model: La mise en œuvre des services intégrés pour les jeunes au Canada : planification et établissement des coûts d’un modèle pancanadien by Jo L. Henderson, Claire de Oliveira and Steve Mathias in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
This analysis represents independent work partially funded by the Canadian Institutes of Health Research's Institute of Neurosciences, Mental Health, and Addiction. The views expressed are those of the authors and not necessarily those of the Canadian Institutes of Health Research. The authors would like to thank the following individuals for their support in preparing the report, which this manuscript is based on: Robyn Burgess at Foundry, Janine Luce, Maria Talotta, and Meaghen Quinlan-Davidson at Youth Wellness Hubs Ontario, Kyleigh Schraeder at the Canadian Institutes Health of Research, and Mackenzie Hilton at the Centre for Addiction and Mental Health.
Data Availability
The authors are happy to share all data collected for this article. These data will be available from the publication date. Please contact the corresponding author if you would like to see any data that are not included in the article or appendix.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Canadian Institutes of Health Research's Institute of Neurosciences, Mental Health, and Addiction.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.