
Abstract
Objective
Posttraumatic stress disorder (PTSD) and alcohol use disorder (AUD) commonly co-occur. Momentary alcohol cognitions may represent in-the-moment, modifiable risk factors to target in interventions for comorbid PTSD and AUD. However, the role of such cognitions in risk for problematic drinking as it emerges in response to individuals’ fluctuating PTSD symptoms across their daily lives remains unknown. The present study aimed to test whether state-level PTSD-alcohol expectancies and/or drinking motives modulate in-the-moment associations between PTSD symptoms and alcohol outcomes.
Method
Frequent drinking adults with current PTSD (n = 54) reported on their posttraumatic symptoms and alcohol cognitions, craving, and consumption during four momentary surveys each day for 14 days (3,024 observations) in an ecological momentary assessment design. Multilevel moderation analyses tested whether in-the-moment PTSD-alcohol expectancies and/or drinking motives moderated relations of PTSD symptoms with alcohol craving and consumption.
Results
Findings demonstrated a significant interaction between PTSD symptoms and coping drinking motives on in-the-moment alcohol craving. Specifically, greater experience of PTSD symptoms related more strongly to craving for alcohol during events in which drinkers endorsed higher levels of coping drinking motives. There were no additional interaction effects for drinking motives or PTSD-alcohol expectancies on either alcohol craving or consumption.
Conclusions
Coping drinking motives appear to convey strong in-the-moment risk for PTSD-related alcohol craving yet not subsequent alcohol consumption. Future research should delineate concurrent alcohol risk and possible protective processes active in the presence of PTSD symptoms to help identify targets for interventions tailored to the unique risk processes maintaining comorbid PTSD and AUD.
Posttraumatic stress disorder (PTSD) and alcohol use disorder (AUD) commonly co-occur 1 and relate to more severe PTSD and AUD symptomatology. 2 Effective interventions for comorbid PTSD/AUD exist 3 although, notably, remain limited by challenges with accessibility, retention and adherence.4,5 Clinical interventions that reduce systemic barriers to access and offer readily available, personalized trauma-informed care could increase the reach of PTSD-related drinking support. 5 Research should identify treatment approaches accessible to individuals with comorbid PTSD/AUD and tailored to the unique processes that maintain PTSD-related drinking.
Alcohol cognitions are widely implicated in PTSD-related drinking6–9 and represent modifiable, common targets of psychosocial interventions for comorbid PTSD/AUD. 3 Alcohol cognitions that may promote PTSD-related drinking include beliefs about the effects of alcohol on PTSD symptoms (PTSD-alcohol expectancies) and/or reasons for drinking alcohol (drinking motives). Expectancies represent anticipated effects of alcohol consumption, 10 including on specific PTSD symptoms. 11 Drinking motives are theorized to translate such expectancies into drinking decisions, comprising reasons for drinking in response to perceived internal/external incentives.10,12 Limited research suggests trait-level alcohol expectancies and motives could modulate PTSD-related drinking. Specifically, greater posttraumatic symptoms have related to riskier drinking only among individuals endorsing moderate or high levels of positive PTSD-alcohol expectancies.8,13 Trauma and posttraumatic symptoms also have related to greater alcohol problems only among individuals highly motivated to drink to cope with general negative affect or depression as well as to enhance positive affect or social experiences.14,15 However, such moderating roles have not been universally supported.16,17 Prior research demonstrates more consistent support for moderating roles of alcohol cognitions in PTSD-related drinking when assessing cognitions more dynamically and/or proximally to posttraumatic symptoms, 18 such as through daily naturalistic assessments 9 and laboratory trauma paradigms. 19 Findings might suggest that state-level alcohol cognitions create conditions under which PTSD symptoms are more likely to lead to problem drinking, although such processes remain currently unexplored despite their possible intervention implications.
Ecological momentary assessment (EMA) designs could delineate in-the-moment associations of state-level alcohol cognitions with PTSD-related drinking in naturalistic settings. Alcohol cognitions likely emerge dynamically in response to traumatic distress and precede behavioral responses such as alcohol use. For example, when encountering a trauma cue, beliefs that alcohol can help distract from trauma-related memories may increase alcohol craving and consumption. Such dynamic risk processes remain underexamined 18 such that it is unknown whether alcohol cognitions confer risk for drinking in the presence of PTSD symptoms in daily life and, if so, which state-level alcohol cognitions might contribute to such risk.
The present study examined whether momentary alcohol cognitions modulate in-the-moment associations of PTSD symptoms with alcohol craving and consumption. Frequent drinking adults with PTSD reported their PTSD symptoms, alcohol cognitions and alcohol outcomes four times daily for 14 days. Greater PTSD symptoms were hypothesized to relate to greater in-the-moment alcohol craving and consumption more so in the presence of alcohol-promoting momentary PTSD-alcohol expectancies and drinking motives.
Methods
This manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines. 20
Participants
Eligible participants were 18–65 years of age, English language proficient, consumed alcohol 4+ times per week over the past month, and met criteria for past-month PTSD. Participants with cognitive impairment that could interfere with assessment completion or those seeking treatment for the effects of a prior stressful event and/or substance/alcohol use were excluded; participants seeking treatment were provided with referral support. Through study recruitment, 405 individuals completed eligibility screening, and 108 met provisional eligibility criteria assessed during eligibility screening. There were 84 individuals scheduled for an enrollment session, 70 individuals completed the session, and 16 participants were excluded from analyses for not meeting criteria for past-month PTSD as assessed during the enrollment session. Participants in the final sample (n = 54) were, on average, 35 years of age (range = 21–54 years; Table 1).
Demographic Characteristics of Sample.
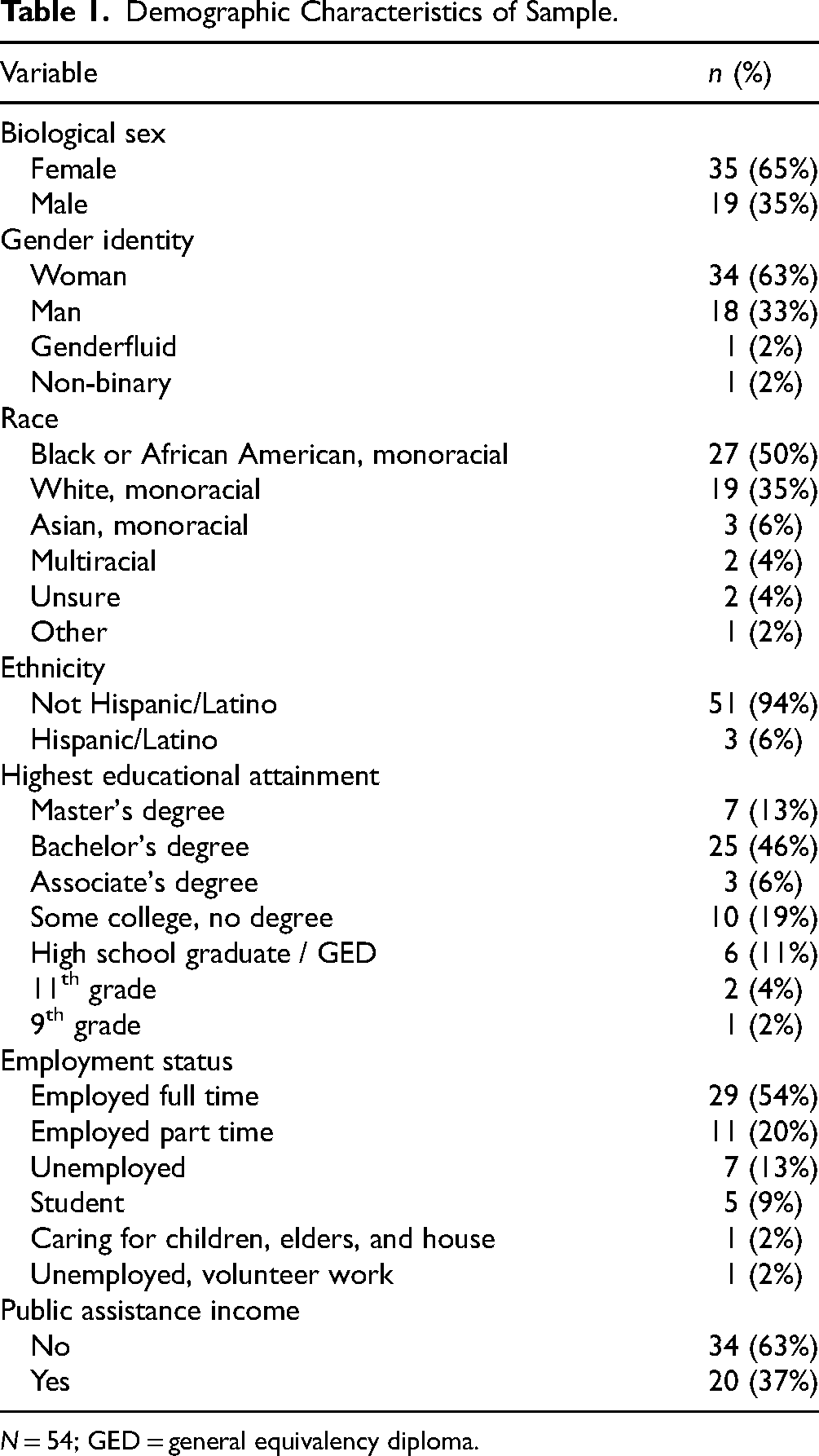
N = 54; GED = general equivalency diploma.
Procedures
Potential participants were recruited in the United States through print and online advertisements. Potential participants completed telephone or online eligibility screening that assessed current age, drinking frequency, treatment seeking status and provisional past-month PTSD using the PTSD Checklist for DSM-5 (PCL-5). 21 Participants meeting provisional eligibility criteria were invited to an enrollment session either in-person at the research laboratory or online through the Zoom conferencing platform from July 2023 to November 2023. During the enrollment session, participants received an overview of study procedures, provided informed consent and completed questionnaires assessing demographics as well as alcohol use, problems and cognitions. Participants also reported on their lifetime experience of potentially traumatic events using the Life Events Checklist, 22 designating their “most distressing event” from those endorsed. Post-baccalaureate or higher trained researchers then administered the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) 23 to diagnose past-month PTSD. Diagnostic interviews were audio recorded with participant consent. Research staff focused the diagnostic interview on participants’ most distressing Criterion A event. 24 Several participants did not endorse a Criterion A trauma as their most distressing event and were queried about other endorsed events to focus on a Criterion A trauma when possible. Participants retained in the final sample represented only those endorsing a Criterion A trauma. Past-month PTSD was defined as at least one Criteria B and C symptom rated moderately or higher, two Criteria D and E symptoms rated moderately or higher, and Criteria F and G met. 23 Finally, research staff reviewed the momentary survey structure and assisted participants with setting up EMA software on their mobile device. Participants were compensated $40 on a reloadable debit card for the 2-h session and provided with a list of mental health resources.
Participants then completed a 14-day EMA using the ilumivu platform. Participants were instructed to complete four assessments each day25,26 through a combination of device- and user-generated assessments27–29 designed to capture a breadth of relevant daily experiences. Specifically, participants completed both user-generated (i.e., a self-initiated “on demand” survey) and device-generated (i.e., two random “daytime” surveys and a scheduled “morning” survey) assessments. The “on demand” survey aimed to capture salient, high-risk moments and was open throughout the day; participants were instructed to complete this survey when experiencing an urge to drink or distress related to a previous traumatic event. The two “daytime” surveys aimed to capture broad PTSD-related drinking risk processes and opened for 1 h daily at a randomized time between 1:00PM–5:00PM and 6:00PM–10:00PM in the participants’ time zone. The “morning” survey aimed to capture events since the previous evening assessment and opened daily from 8:00AM–12:00PM in the participants’ time zone. Surveys assessed PTSD symptoms, alcohol cognitions, alcohol craving and alcohol consumption since the last assessment. Surveys took approximately 5 min to complete. Participants who reported alcohol consumption that could result in an estimated blood alcohol content (eBAC) ≥ 0.30% (n = 2) received psychoeducation on alcohol overdose and appropriate referral resources. Research staff contacted participants periodically to encourage compliance and troubleshoot completion barriers. Participants were compensated up to $300 for the EMA phase based on a renumeration schedule of $10/day with up to $160 in bonuses to encourage compliance. Study procedures were approved by the University at Buffalo Institutional Review Board (#00005757).
Measures
PTSD symptoms
The PCL-5 21 assessed participants’ experience of 20 PTSD symptoms (e.g., “Feeling jumpy or easily startled”) during each momentary survey. Scale introductory language was modified to assess in-the-moment experiences (“Right now, how much are you bothered by:”), and participants responded using the original scale ranging from 1 (not at all) to 5 (extremely). Responses were summed to calculate a total score (within-level α = .98), with at least 70% of items required for scale computation.
Alcohol craving
Participants reported on urge to drink alcohol during each momentary survey using a single item (“To what extent do you feel an urge to drink an alcoholic beverage right now?”) with a 0 (no urge to drink at all) to 10 (very strong urge to drink) response scale.30,31
Alcohol consumption
Participants reported their alcohol use since the prior assessment (“Did you have a drink of beer, wine, wine cooler, or liquor since the last assessment?”) using “No” or “Yes” response options. Participants reporting any alcohol use responded to a subsequent item assessing alcohol quantity using a 1 (1 drink) to 10 (10 or more drinks) response scale. Participants were provided with a definition of a standard drink (i.e., 12-ounce can or bottle of beer, 5-ounce glass of wine, or drink containing one shot of liquor) at study enrollment. Responses were condensed into 0 (i.e., did not drink alcohol since last assessment; 66%), 1 (1 drink; 6%), 2 (2 drinks; 10%), 3 (3 drinks; 8%), and 4 (i.e., 4 or more drinks; 10%) to facilitate model convergence.
PTSD-alcohol expectancies
The PTSD-Alcohol Expectancy Questionnaire (P-AEQ) 11 assessed participants’ perceptions of alcohol's effects on their PTSD symptoms during the momentary assessments. The original 27 scale items randomly were administered in varying frequencies across the momentary surveys to reduce response burden. Participants responded using abbreviated “No” or “Yes” response options, with an additional “Not applicable” response option provided for several items (i.e., flashbacks, hallucinations, visual memories) that was recoded to missing for analyses. Scale introductory language was modified to assess in-the-moment experiences (“If I drank RIGHT NOW…”). Responses were averaged to calculate positive (within-level α = .95, from tetrachoric correlations) and negative (within-level α = .94, from tetrachoric correlations) subscales, with at least four items required for scale computation at each momentary assessment.
Drinking motives
Participants reported their reasons for drinking during each momentary assessment using an abbreviated version of the Drinking Motives Questionnaire. 12 Two items from each subscale with the highest factor loadings in the original measure development work 12 were selected to reduce response burden, encompassing coping (e.g., “To forget about your problems”), enhancement (e.g., “Because you like the feeling”), social (e.g., “Because it improves parties and celebrations”), and conformity (e.g., “To be liked”) motives. Scale introductory language was modified to assess in-the-moment experiences (“Right now, how motivated are you to drink for the following reasons?”), and participants responded using a scale ranging from 1 (not at all) to 4 (very much). Responses were averaged to calculate subscales (within-level αs = .85, .88, .91, and .87, respectively).
Data Analytic Strategy
Multilevel regression in Mplus 32 was used to examine whether drinking motives and/or PTSD-alcohol expectancies (Level 1) moderated within-person associations between PTSD symptoms (Level 1) and alcohol outcomes (Level 1). Regarding missing data, retention for daily survey completion from the enrollment session to the end of the momentary survey period was excellent (94%). Participants lost to attrition tended to complete most of the monitoring period (M = 11 / 14 days), and there were no significant differences in baseline demographics (i.e., sex, gender, Hispanic ethnicity, race, public income assistance) between participants who completed versus withdrew from participation. There were missing data on PTSD symptoms (5%), alcohol craving and consumption (6%), and drinking motives (7%), as well as missing data on PTSD-alcohol expectancies by design. Study analyses utilized maximum likelihood estimation with robust standard errors to accommodate missing data and non-normality. 32
Random intercept only models (“null” models) first estimated within- and between-person variability in alcohol outcomes. Intraclass correlation coefficients (ICCs) were computed to characterize proportion of variability accounted for by clustering. Additional random effects (e.g., slopes) were added to the model iteratively and retained based on nested likelihood ratio tests as well as comparisons of the Akaike information criterion and Bayesian information criterion. Random slopes were supported for main effects of PTSD symptoms and drinking motives on alcohol craving, but not remaining main and interaction effects. Models for alcohol craving controlled for several Level 1 (i.e., weekend status [Thursday–Saturday versus Sunday–Wednesday]; time of day [6:00AM–12:00PM, “morning;” 12:00PM–6:00PM, “afternoon;” 6:00PM–6:00AM, “evening”]; measurement reactivity [days since beginning EMA]; survey type [scheduled, random, self-initiated]) and Level 2 (i.e., sex, typical weekly drinking quantity) covariates; survey type was not significantly related to alcohol urge or consumption. For alcohol consumption, data were arranged to test cross-lagged effects. These models controlled for the same Level 1 and 2 predictors as well as alcohol consumption reported during the previous momentary assessment. Level 1 predictors were centered within persons, and Level 2 predictors were centered around the overall mean. Cross-product terms tested moderation by PTSD-alcohol expectancies and/or drinking motives, and significant interactions were probed through simple slopes at values below (−1 SD), at, and above (+1 SD) the mean (quantpsy.org).
Results
Sample Characteristics
Participants endorsed, on average, almost nine potentially traumatic events in their lifetime at enrollment (M = 8.98; SD = 4.63), with the most common index traumatic events comprising sudden unexpected death of someone close (32%), sexual assault (19%), and physical assault (13%). Participants’ average CAPS-5 total symptom severity score was 28.56, generally comparable across male (M = 27.42; SD = 8.69) and female (M = 29.17; SD = 10.36) participants. Participants reported consuming, on average, 23 drinks per week at enrollment, higher for male (M = 32.95; SD = 31.24) than female (M = 18.83; SD = 7.33) participants.
Participants reported frequent PTSD symptoms across the 14-day EMA phase, endorsing at least one symptom during 93% of momentary assessments. Participants reported drinking alcohol considerably less frequently (35% of momentary assessments), consuming an average of three standard drinks (M = 3.07; SD = 1.77) during drinking occasions. Participants tended to perceive more positive (M = 0.50; SD = 0.38) than negative (M = 0.35; SD = 0.35) effects of alcohol on PTSD symptoms, and participants were slightly more likely to endorse enhancement (M = 2.57; SD = 1.01) or coping (M = 2.52; SD = 1.05) than social (M = 2.32; SD = 1.07) or conformity (M = 2.14; SD = 1.04) drinking motivations.
Alcohol Craving
There was a strong clustering effect for alcohol craving (ICC = 0.57). Regarding the model with PTSD-alcohol expectancies, there were no significant interactions of PTSD symptoms with either positive (b = –0.02[–0.11,0.07], p = .67) or negative (b = –0.40[–0.09,0.01], p = .14) PTSD-alcohol expectancies on alcohol craving. Greater positive (b = 1.41[0.27,2.56], p = .02) but not negative (b = –0.57[–1.49,0.35], p = .23) expectancies related to greater alcohol craving, regardless of PTSD symptoms. Greater PTSD symptoms also related to greater alcohol craving (b = 0.09[0.06,0.12], p < .001). Greater typical weekly drinking quantity (b = 0.05[0.02,0.08], p < .001) and later survey time (b = 0.54[0.26,0.82], p < .001) related to stronger alcohol craving; no additional covariates reached statistical significance. Regarding the model with drinking motives, there was a significant interaction between PTSD symptoms and coping motives on alcohol craving (b = 0.03[0.01,0.05], p = .001). Simple slopes revealed that greater PTSD symptoms related more strongly to momentary alcohol craving at high (b = 0.07, p < .001) and moderate (b = 0.06, p < .001) relative to low (b = 0.04, p = .02) levels of coping motives (Figure 1). There were no significant interactions of PTSD symptoms with social, enhancement, or conformity motives on alcohol craving (bs = –0.02 to 0.01, ps = .05 to .91). Greater typical weekly drinking quantity (b = 0.04[0.003,0.08], p = .04) and later survey time (b = 0.34[0.16,0.51], p < .001) related to stronger alcohol craving; no additional covariates reached statistical significance.
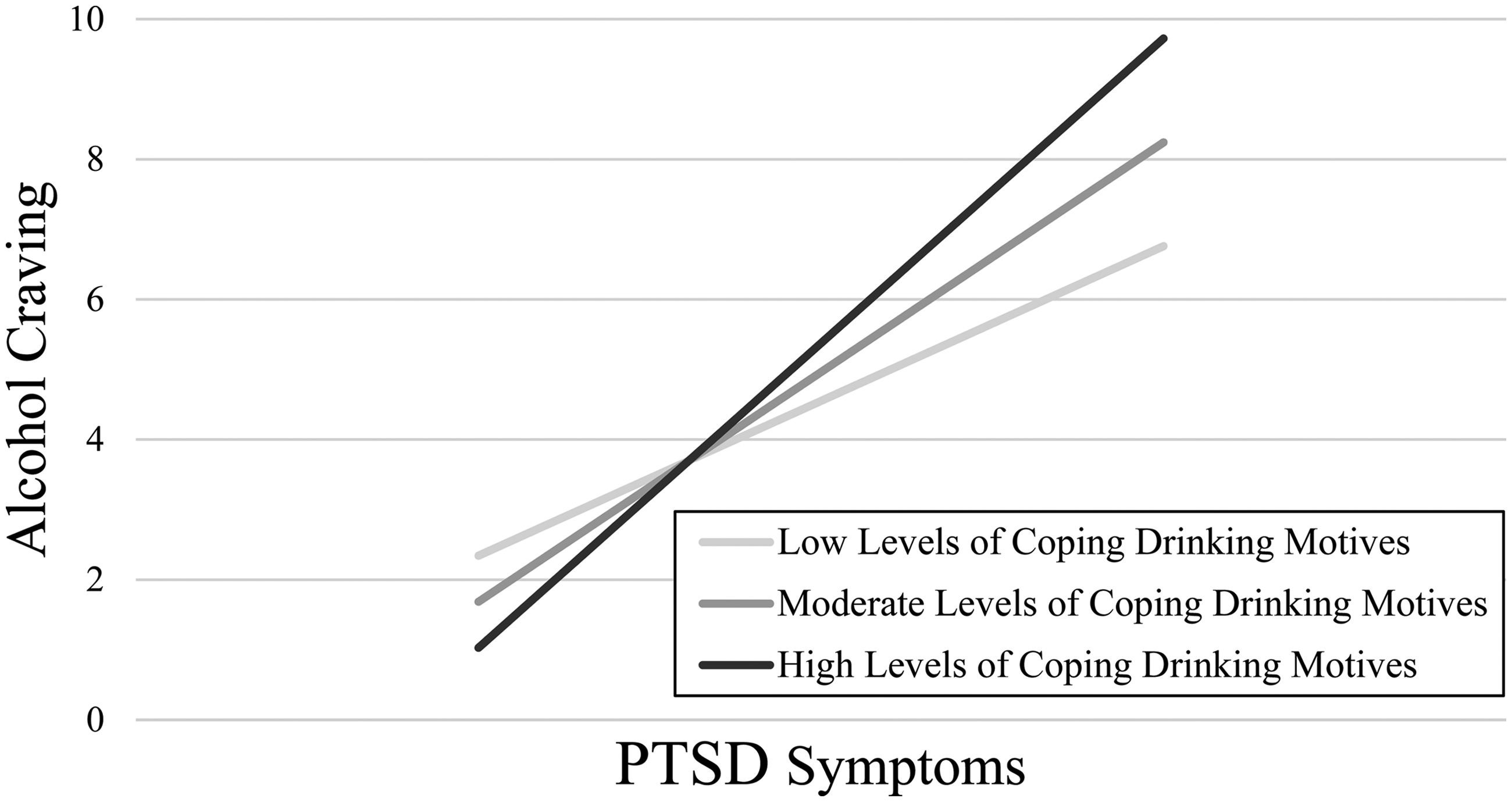
Interaction of PTSD symptoms with coping drinking motives on momentary alcohol craving.
Alcohol Consumption
There was a moderate clustering effect for alcohol consumption (ICC = 0.33). Regarding the model with PTSD-alcohol expectancies, there were no significant main or interaction effects of PTSD symptoms and PTSD-alcohol expectancies on subsequent alcohol consumption (bs = –0.66 to 0.36, ps = .09 to .91). Greater drinking at the preceding timepoint (b = 0.29[0.15,0.44], p < .001) related to greater alcohol consumption; no additional covariates reached statistical significance. Regarding the model with drinking motives, there were no significant interaction effects of any motives on subsequent alcohol consumption (b = –0.01 to 0.00, p = .62 to .86). Greater social motives predicted greater subsequent alcohol consumption (b = 0.18[0.02,0.34], p = .03), but other motives or PTSD symptoms did not (bs = –0.07 to 0.06, ps = .57 to .97). Greater drinking at the preceding timepoint (b = 0.11[0.03,0.20], p = .01), later survey time (b = 0.28[0.12,0.45], p = .001), and earlier survey day (b = –0.03[–0.05, −0.01], p = .01) related to greater alcohol consumption; no additional covariates reached statistical significance.
Discussion
The present study sought to identify momentary alcohol cognitions that may increase alcohol craving and/or consumption in response to PTSD symptoms occurring in daily life. Findings identified in-the-moment PTSD-related drinking risk conferred by coping drinking motives. Specifically, frequent drinkers craved alcohol more amid PTSD symptoms when experiencing relatively higher coping motivations. Nevertheless, neither coping motives nor additional cognitions conferred risk for subsequent alcohol consumption. Findings begin to characterize the processes operating in real-time that contribute to PTSD-related alcohol craving, while also suggesting potential protective factors operating in these moments that might restrict consumption despite strong craving.
Coping drinking motives increased in-the-moment risk for PTSD-related alcohol craving. Findings support negative reinforcement models of stress- and trauma-related drinking (i.e., tension reduction, self-mediation, distress coping)33–37 and converge with prior research supporting moderating roles for coping motives in proximal PTSD-related drinking processes. 18 Notably, the present findings are the first, to our knowledge, to demonstrate support for such processes in-the-moment drinkers experience PTSD symptoms amid their daily lives. Clinical efforts for comorbid PTSD/AUD could be delivered when drinkers endorse elevated coping motives in an effort to reduce alcohol craving. Traditional interventions for comorbid PTSD and alcohol or substance use disorder often challenge alcohol-promoting cognitions 38 such as coping motives, and such intervention content could be adapted for incorporation into in-the-moment supports.
Momentary interventions for comorbid PTSD/AUD may be best served by focusing on coping motivations relative to additional motivations. Social motives related to greater alcohol use regardless of PTSD symptoms in the present sample, and high levels of enhancement motives previously have conferred drinking risk broadly regardless of daily PTSD symptom severity. 9 It is possible these additional motives instead confer risk more distally over time, such as in response to general social disengagement (i.e., social motives) or persistent negative affect (i.e., enhancement motives).
Coping motives conferred risk for alcohol craving, yet not alcohol consumption. Extant literature does suggest mixed findings on associations of alcohol craving with consumption.30,39,40 Craving may represent an important alcohol risk endophenotype 41 – one potentially less sensitive to contextual limits than alcohol consumption. That is, drinkers may crave alcohol but be restricted from drinking due to limited alcohol access, financial barriers, or alcohol-restrictive social norms (e.g., in the workplace). It is also possible that the frequent yet not necessarily hazardous drinkers comprising the present sample were able to limit their alcohol consumption even in the presence of strong craving. Given craving's centrality and clinical significance to problem drinking,41,42 strong in-the-moment craving may suggest important drinking vulnerability regardless of alcohol consumption. Thus, even if not always resulting in problem drinking, strong craving may signal high-risk moments for brief interventions to help drinkers engage in steps toward self-protection to lower future drinking risks. Research should better characterize events in which drinkers strongly crave alcohol amid PTSD symptoms yet do not drink heavily. Such knowledge could delineate pathways from PTSD symptoms to alcohol consumption, perhaps identifying multiple intervention points involving both risk and protective factors for PTSD-related drinking.
Momentary PTSD-alcohol expectancies did not modulate PTSD-related alcohol craving or consumption. Theoretical frameworks suggest that motivations to drink are more proximal risk factors than alcohol expectancies 10 such that motives may confer greater in-the-moment risk for drinking in response to posttraumatic distress. It is also possible that such findings resulted from greater power to detect associations involving drinking motives than alcohol expectancies in the present study, because alcohol expectancies were assessed less frequently across momentary assessments. Future research should characterize how PTSD-alcohol expectancies co-vary with PTSD-related drinking risk. Such efforts could explore whether momentary interventions might benefit from targeting drinking motives while additional interventions instead benefit from targeting more static, trait-level alcohol expectancies.
Several study limitations should be considered. First, to minimize reporting burden, the present study collected minimal information on social context and cues. Such contextual factors may be important contributors to PTSD-related drinking and useful for intervention targeting/implementation. Second, despite reducing retrospective bias by assessing in-the-moment processes, the present study nevertheless relied on self-report that may have social desirability biases. 43 Third, systematic differences in unmeasured constructs across retained versus withdrawn participants may have contributed to attrition biases. Relatedly, models did not consider participants’ additional substance use or comorbid mental diagnoses. Research could explore whether comorbid substance use or mental health diagnoses lead to individual differences in likelihood of PTSD-related drinking and/or co-use in response to alcohol-promoting cognitions. Finally, the present study focused only on drinking expectancies and motivations given their well-researched support in PTSD-related drinking.7–11 Efforts could explore additional cognitions (e.g., self-efficacy) that also may represent in-the-moment intervention targets.
Findings suggest that in-the-moment coping drinking motives confer risk for PTSD-related alcohol craving. Future research should explore additional factors operating in these moments that may protect against subsequent alcohol consumption as well as any individual differences in these momentary associations as a function of demographics and trauma experiences. Findings represent an initial step to understand possible in-the-moment intervention targets for comorbid PTSD/AUD.
Footnotes
Acknowledgments
We thank the participants for sharing their experiences.
Data Access
Data and/or research tools used in the preparation of this manuscript are available from the National Institute on Alcohol Abuse and Alcoholism Data Archive (NIAAADA). NIAAADA is a collaborative informatics system created by the National Institutes of Health (NIH) to provide a national resource to support the sharing of federally-funded data for accelerating research. Data can be accessed via ![]() . Dataset identifier(s): C4363. This manuscript reflects the views of the authors and may not reflect the opinions or views of the National Institutes of Health.
. Dataset identifier(s): C4363. This manuscript reflects the views of the authors and may not reflect the opinions or views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under award numbers K99 AA029728 and R00 AA029728. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.