
Abstract
Objectives
Military sexual trauma (MST) is a prevalent issue among actively serving members and Veterans, and is associated with adverse health outcomes including mental disorders. This study sought to identify correlates and protective factors for the development of mental disorders among Canadian MST survivors.
Methods
We analyzed data from participants of the longitudinal 2018 Canadian Armed Forces Members and Veterans Mental Health Follow-up Survey (CAFVMHS) who experienced MST (rounded n = 455; 9.6%). A semi-structured diagnostic interview assessed MST and mental disorders in accordance with DSM-IV criteria. Multivariable logistic regressions examined associations between sample characteristics (2002 and 2018) and psychosocial factors (at baseline [i.e., 2002] and 2018) and any mental disorder since 2002. Analyses were run among the full subsample of MST survivors and additionally stratified by sex, when possible.
Results
Among MST survivors, 66.5% had a mental disorder since 2002. Among the total sample, those who were officers (odds ratio [OR] = 0.58) or on active duty (OR = 0.52) had reduced odds of any mental disorder since 2002. In addition, less frequent use of avoidance coping in 2002 and 2018 (adjusted odds ratio [AOR]: 0.86, 0.64), more frequent use of active coping in 2018 (AOR = 0.64), less frequent use of self-medication coping in 2018 (AOR = 0.79), greater perceived social support in 2018 (AOR = 0.94), and reduced work stress across various domains in 2018 (AOR: 0.67–0.87) were associated with reduced odds of any mental disorder since 2002. Some variability emerged according to sex (e.g., types of work stress or coping emerging as protective).
Conclusions
Results highlight certain sample characteristics and psychosocial factors that illustrated a protective relationship with mental disorders among MST survivors. Findings may inform targeted intervention strategies that could help mitigate adverse mental health impacts of MST.
Plain Language Summary
Sexual trauma in the military is an important issue and negatively impacts the mental health of actively-serving members and veterans. Using data that represents the Canadian Armed Forces from 2002, and follow-up data from 2018, we examined factors that may help improve mental health in those who have experienced military sexual trauma. Nearly two-thirds of survivors of military sexual trauma had a mental health condition since 2002. Factors identified that may help improve mental health in military sexual trauma survivors included: less use of avoidance and self-medication coping, more use of active coping, increased social support, and reduced work stress. These results may help guide important treatment targets to improve mental health for survivors of military sexual trauma.
Introduction
Military sexual trauma (MST) is a pervasive issue for active military personnel and Veterans. The definition of MST commonly includes sexual assault and sexual harassment that occurs while serving in the military, with some variability across studies. 1 Meta-analyses and reviews estimate that between 15% and 45% of active members and Veterans report experiencing MST, with heterogeneity throughout the literature.2,3 Estimates of MST are consistently elevated among females compared to males.2–8 Other identified risk factors for MST include younger age, lower military rank, being single, and lower income.2,6–9
In addition to establishing prevalence estimates and identifying risk factors for MST, another focus within the MST literature is outcomes or correlates of MST. Mental disorders are most commonly examined, with consistent evidence revealing survivors of MST have increased odds of a range of disorders, such as posttraumatic stress disorder (PTSD), depression, anxiety disorders, and substance use disorders.1,2,5,7,10,11 Other health-related correlates of MST include suicidality and self-harm, physical conditions or somatic symptoms, sexual dysfunction, and disability.1,2,4,10,11 Some studies have identified that relationships between MST and health outcomes may vary according to sex or gender.1,7,10 For example, PTSD symptoms in MST survivors may be more severe for males compared to females 1 and there may be gender differences in the prevalence of mental disorders among MST survivors (e.g., PTSD and eating disorders are more common among women, bipolar is more common among men). 10 Other research has found greater mental health impacts of MST among males compared to females (e.g., greater number of adverse mental health outcomes). 7 Additional research is warranted to examine these differences further.
It is clear that MST is prevalent and associated with adverse health outcomes. More research is needed to develop targeted interventions to mitigate the adverse impacts of MST. For example, understanding protective factors against adverse outcomes of MST can help inform intervention and health promotion targets. Similarly, survivors with limited protective factors may benefit from early and/or targeted intervention. One recent study examined the impact of social support and spirituality on the relationship between recent sexual trauma (within the past 3 years) and PTSD, depression, somatic symptoms, and insomnia among a population-based sample of U.S. service members and Veterans. These factors were not protective against PTSD and depression among those who experienced recent sexual trauma (including sexual assault and harassment). 11 This study was limited by the narrow scope of protective factors and mental disorders examined, the restrictive definition of recent sexual trauma, and the use of self-report questionnaires to assess mental health outcomes. To the best of our knowledge, no other population-based studies exist on this specific topic. More research is needed to comprehensively examine possible protective factors for adverse mental health outcomes among survivors of MST. In addition, the majority of research in this area has focused on U.S. samples, with minimal studies utilizing Canadian data.6,8 More research is warranted to understand MST and its correlates within Canadian samples. Using Canadian population-based data, collected across a 16-year period, this study aimed to identify protective factors for mental disorders (assessed via diagnostic interview) among survivors of MST.
Methods
Data
We analyzed data from the Canadian Armed Forces Members and Veterans Mental Health Follow-up Survey (CAFVMHS), 12 conducted by Statistics Canada. The sample was comprised of Regular Forces personnel from the 2002 Canadian Community Health Survey–Canadian Forces Supplement (CCHS-CFS) who also completed the 2018 CAFVMHS, 16 years later. The CCHS-CFS was administered to a population-based sample of Canadian Armed Forces members ages 15–64 years. CCHS-CFS participants who were Reserve Force members or completed the 2016 Life After Service Survey or the CAF Transition and Well-Being Survey were ineligible to participate. Other exclusion criteria were loss of contact and death since 2002. Of the 4,299 CCHS-CFS respondents who were contacted to participate in the 2018 CAFVMHS, 2,941 consented and were re-interviewed, yielding a response rate of 68.4%. Additional details of the CCHS-CFS and CAFVMHS methodologies have been published elsewhere.12–15
Measures
Military sexual trauma
Within the World Health Organization Composite International Diagnostic Interview (WHO-CIDI), 16 two items from the PTSD module, within the traumatic events section, assessed lifetime exposure to sexual trauma in 2002 and 2018: (1) sexual assault: “anyone forcing you or attempting to force you into any unwanted sexual activity by threatening you, holding you down, or hurting you in some way” and (2) unwanted sexual touching: “anyone ever touched you against your will in any sexual way … touching or grabbing, to kissing or fondling.” In 2018, those who reported having either of these experiences in their lifetime were asked whether the sexual trauma: (1) took place while deployed as part of a Canadian Forces operation, (2) occurred in the Canadian Forces workplace, or (3) was perpetrated by a member of the Canadian Forces or a civilian employee within the Department of National Defence at the time of occurrence. In line with prior research, participants responding “yes” to any of these items were categorized as having experienced MST. 6 Of note, this definition does not include sexual harassment.
Mental disorders
The WHO-CIDI 16 assessed mental disorders, including major depressive episode (MDE), generalized anxiety disorder (GAD), social phobia (SP), panic disorder (PD), and PTSD through Computer Assisted Personal Interviews administered by Statistics Canada. The WHO-CIDI is a valid and reliable 17 standardized diagnostic interview in accordance with DSM-IV criteria. Lifetime mental disorders with an onset “since 2002” (following the 2002 CCHS-CF) were assessed in 2018. We collapsed those meeting criteria for MDE, GAD, SP, PD, and PTSD since 2002 to derive a single “any mental disorder since 2002” variable. We selected the “since 2002” timeframe as opposed to lifetime to increase the likelihood of assessing mental disorders with onset closer to or after experiencing MST.
Coping style
In 2002 and 2018, items from the Coping Inventory to Problems Experienced (COPE) Scale, the Ways of Coping Questionnaire, and the Coping Strategy Indicator assessed participants’ frequency of use of coping strategies. 18 A factor analysis from prior research identified three coping subtypes: active coping (four items; e.g., problem-solving), avoidance coping (five items; e.g., wishing the situation would go away), and self-medication (two items; e.g., drinking alcohol). 19 Items were rated with a 4-point scale ranging from “often” to “never.” Coping subscales were re-scored with a higher score indicating more frequent use of adaptive styles of coping (active coping) or less frequent use of maladaptive styles of coping (avoidance, self-medication).
Social support
In 2002 and 2018, the Medical Outcomes Study (MOS) Social Support Survey 20 assessed perceived social support. This scale was comprised of 19 items, rated on a 4-point scale ranging from “none” to “all of the time,” to assess the frequency of availability of various forms of social support (e.g., someone to confide in). Items were summed to create a total scale at each time point (2002, 2018), where higher scores indicate higher levels of social support.
Work stress
In 2002 and 2018, an abbreviated version of the Job Content Questionnaire 21 assessed perceived work stress. This measure was comprised of 12 items (e.g., your job was very hectic), rated on a 5-point scale ranging from “strongly agree” to “strongly disagree.” Items were summed to form six continuously scored subscales: skill discretion/demand (level of skill required, flexibility to decide which skills to employ), decision authority/control (autonomy), psychological demand (mental workload), job insecurity (fear of and likelihood), physical exertion (physical workload), social support (from supervisor/coworkers). Subscales were re-scored to reflect higher scores indicating lower levels of work stress. In 2018, participants who had released from military service were administered this scale if they reported that they were currently working.
Sociodemographic and military characteristics
Participants self-reported their age (assessed continuously), sex (male, female), race (White, person of colour), marital status (married/common-law, not married), household income (≤$49,999, ≥$50,000), education (secondary school graduate or less, some post-secondary education or higher), rank (junior/senior non-commissioned member, officer), environment (land, air, sea), lifetime deployment history (no, yes), and member status (active duty, Veteran). The categorizations of these variables were chosen in accordance with prior research. 6 We included the 2002 assessment of these variables, with the exceptions of member status, which was only assessed in 2018 and sex, which due to Statistics Canada vetting policy, the 2002 version could not be released.
Analytic Strategy
Analyses were restricted to the subsample of participants who experienced MST (rounded n = 455; 9.6% of total sample). Crosstabulations and descriptive statistics assessed sample characteristics and candidate protective factors (2002 variables) and correlates (2018 variables) in those with and without any mental disorder since 2002. Next, unadjusted logistic regressions examined associations between sample characteristics and any mental disorder since 2002. Finally, bivariate and multivariate logistic regressions examined associations between individual candidate protective factors and correlates and any mental disorder since 2002. We included an unadjusted model and a model adjusting for sex, age, income, marital status, and member status. Covariates were chosen based on prior research with the CAFVMHS showing relationships between these variables and mental disorders and MST 6 (see Refs.19,22–24 for research identifying correlates/protective factors of mental disorders among active members and veterans, regardless of MST exposure), and results of the current study's unadjusted model examining relationships between sociodemographic characteristics and any mental disorder since 2002, among those who experienced MST. Analyses were run among the full subsample of those who experienced MST, and when cell sizes permitted, were re-run stratified by sex (sex was removed as a covariate). Analyses were conducted using STATA (version 16). To enable representativeness of the 2002 CAF population, sampling weights developed by Statistics Canada were applied to all analyses, and bootstrapping accounted for the complex sampling design. In line with Statistics Canada's policies, unweighted ns were rounded to base 5, and cells with n < 5 could not be released.
Results
Sample Characteristics
As reported elsewhere, 6 9.6% of the 2018 CAFVMHS sample (rounded n = 455) indicated experiencing MST in their lifetime. The prevalence of MST was 44.6% among females and 4.8% among males. 6 See Table 1 for sample characteristics. The prevalence of any mental disorder since 2002 among those who experienced MST was 66.5%. The prevalence of any mental disorder since 2002 according to sample characteristics, among the full MST sample and stratified by sex, is reported in Table 2.
Sample Characteristics of Survivors of Military Sexual Trauma (n = 455).
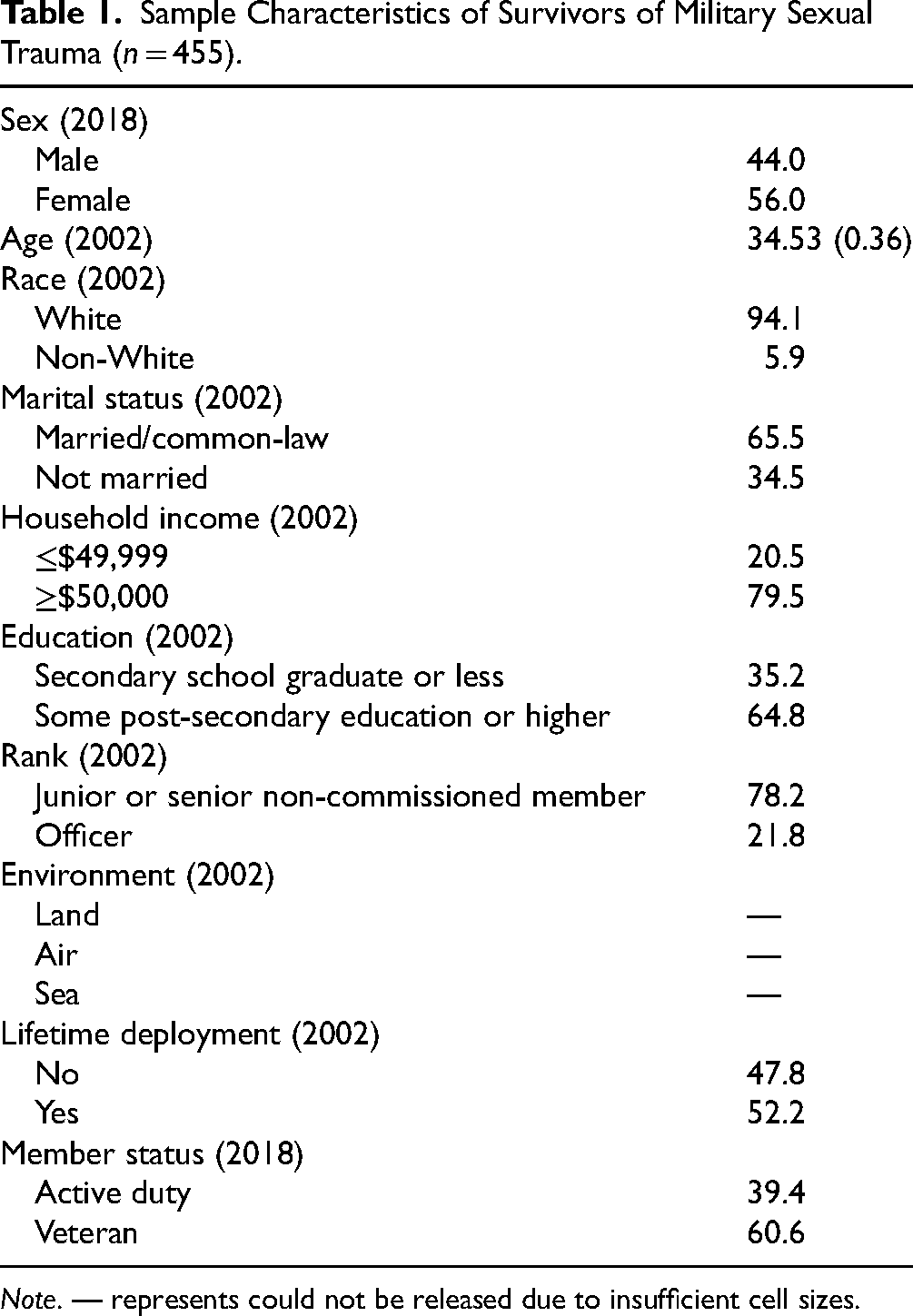
Note. — represents could not be released due to insufficient cell sizes.
Prevalence of Any Mental Disorder Since 2002 According to Sample Characteristics Among Survivors of Military Sexual Trauma (n = 455; 9.6% of Sample).
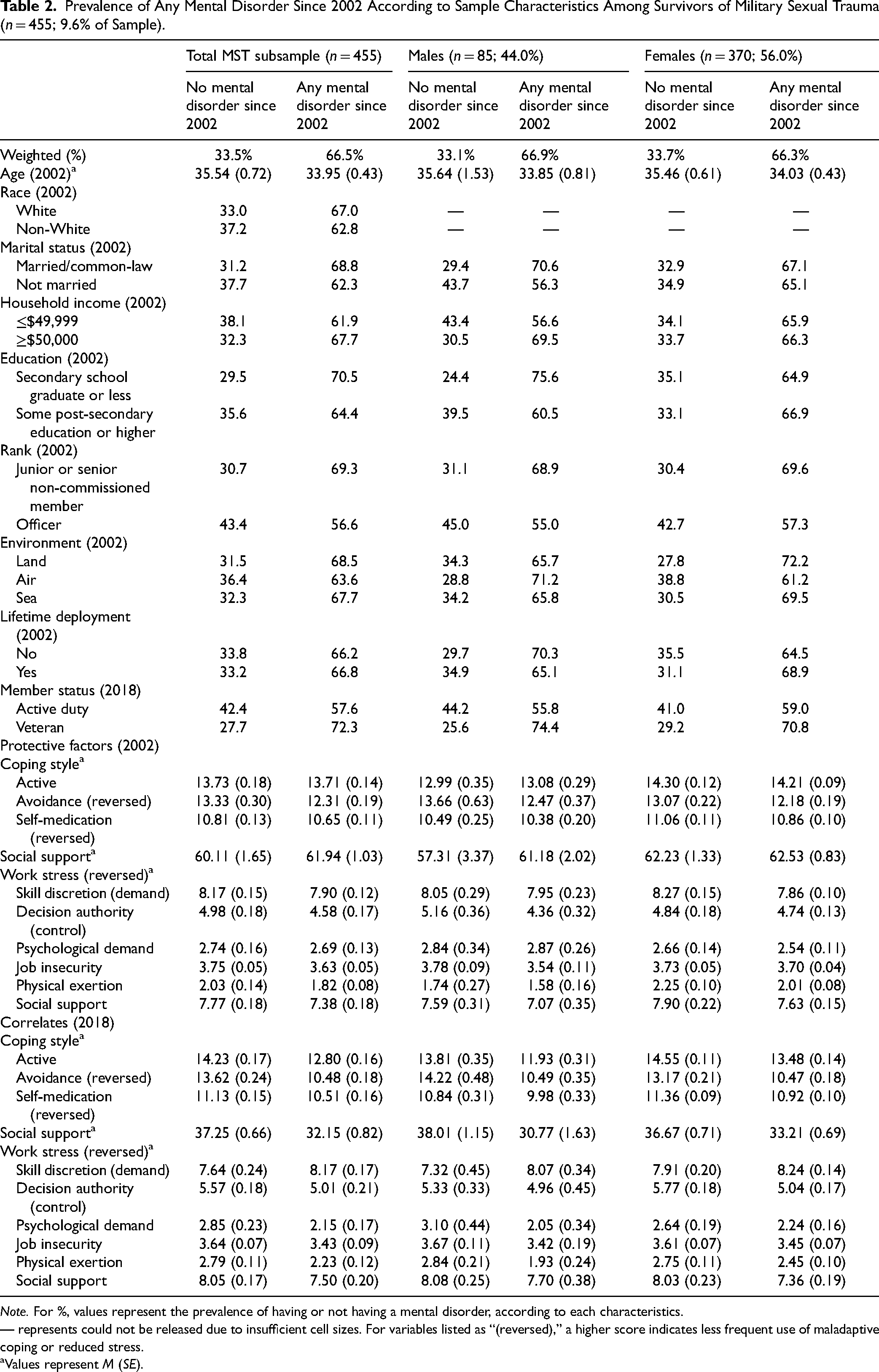
Note. For %, values represent the prevalence of having or not having a mental disorder, according to each characteristics.
— represents could not be released due to insufficient cell sizes. For variables listed as “(reversed),” a higher score indicates less frequent use of maladaptive coping or reduced stress.
Values represent M (SE).
As shown in Table 3, among those who experienced MST, officer rank (odds ratio [OR] = 0.58, 95% confidence interval [CI] [0.36–0.94], p < .05; reference = non-commissioned member) and being on active duty (OR = 0.52, 95% CI [0.31–0.87], p < .05; reference = Veteran) were associated with reduced odds of any mental disorder since 2002. Among females, older age (OR = 0.97, 95% CI [0.95–1.00], p < .05), officer rank (OR = 0.59, 95% CI [0.40–0.86], p < .01), working in an air environment (OR = 0.61, 95% CI [0.38–0.98], p < .01; reference = land), and being on active duty (OR = 0.60, 95% CI [0.39–0.92], p < .05) were associated with reduced odds of any mental disorder since 2002. No significant associations emerged among males. Sex-stratified results for race and marital status could not be released due to insufficient cell sizes.
Associations Between Sample Characteristics and Mental Disorders Among Survivors of Military Sexual Trauma (n = 455).
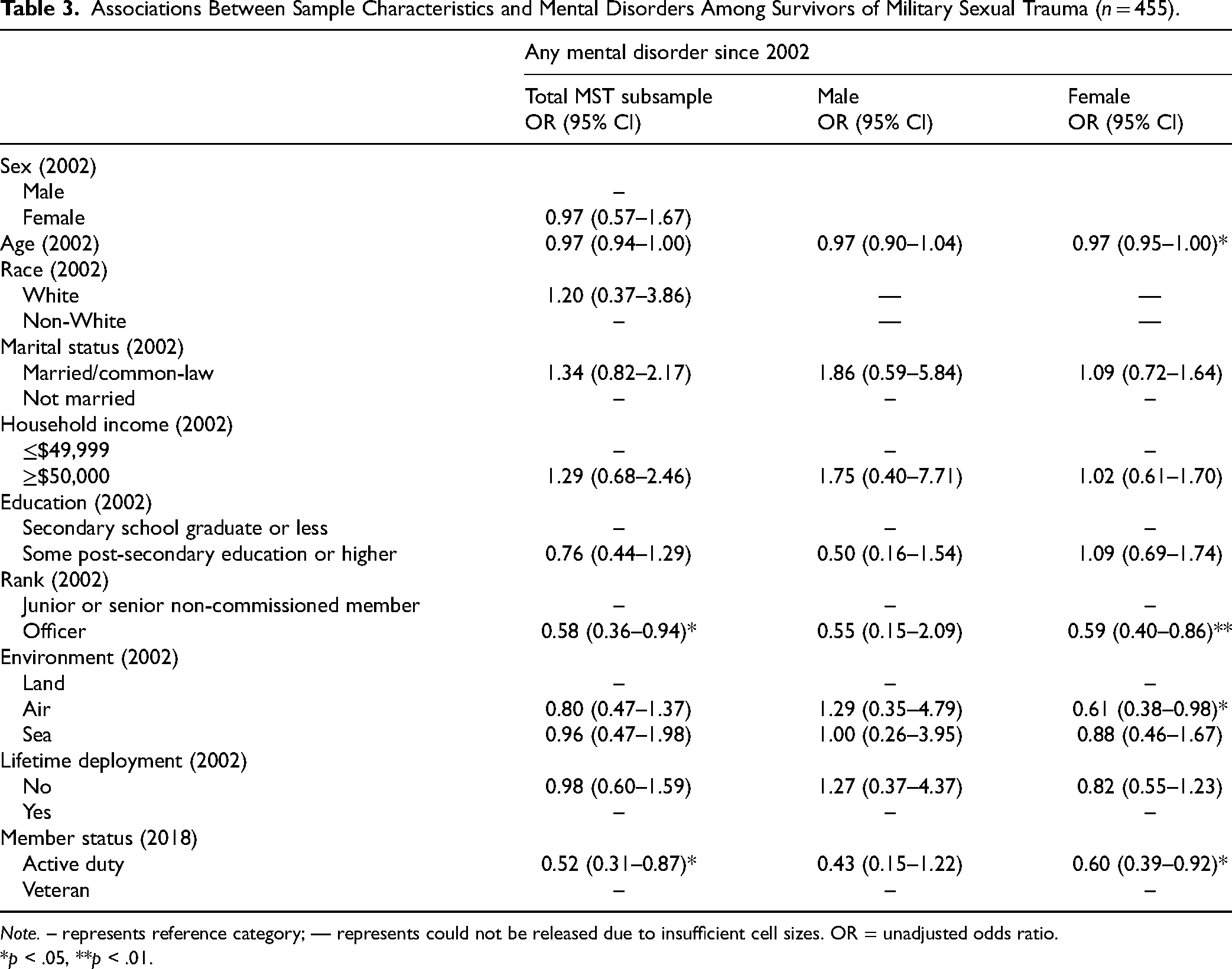
Note. – represents reference category; — represents could not be released due to insufficient cell sizes. OR = unadjusted odds ratio.
*p < .05, **p < .01.
Correlates of Mental Disorders
Associations between candidate protective factors (2002) and correlates (2018) and any mental disorder since 2002 are shown in Table 4. Within the adjusted model, less frequent use of avoidance coping was the only variable assessed in 2002 associated with reduced odds of any mental disorder since 2002 among the MST sample and females (adjusted odds ratio [AOR] = 0.86, 0.89, p < .01).
Associations Between Possible Protective Factors and Correlates and Mental Disorders Among Survivors of Military Sexual Trauma (n = 455).
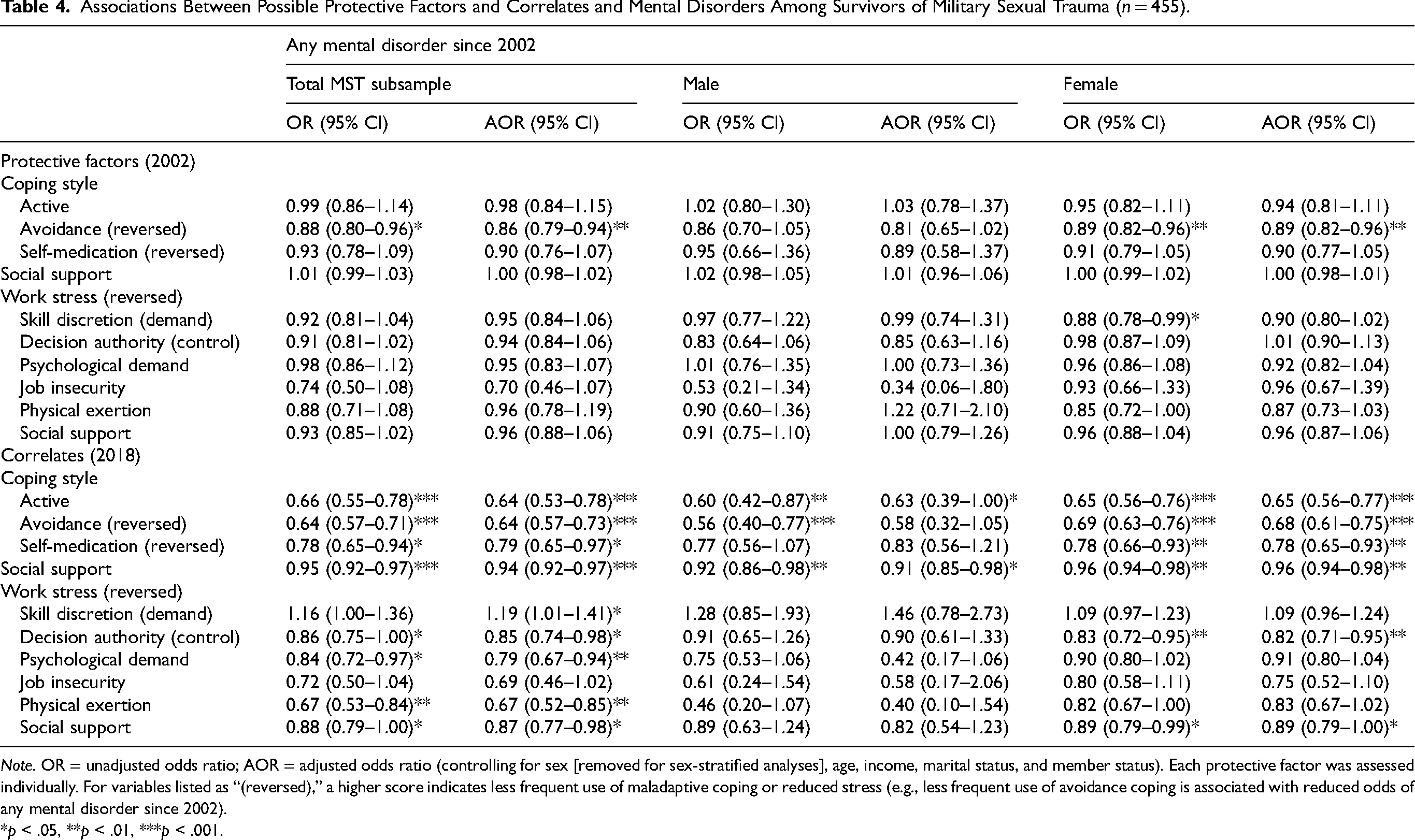
Note. OR = unadjusted odds ratio; AOR = adjusted odds ratio (controlling for sex [removed for sex-stratified analyses], age, income, marital status, and member status). Each protective factor was assessed individually. For variables listed as “(reversed),” a higher score indicates less frequent use of maladaptive coping or reduced stress (e.g., less frequent use of avoidance coping is associated with reduced odds of any mental disorder since 2002).
*p < .05, **p < .01, ***p < .001.
In 2018, more frequent use of active coping (AOR = 0.63–0.65, p < .05) and greater social support (AOR = 0.91–0.96, p < .05) were associated with reduced odds of any mental disorder since 2002. Also in 2018, within the full sample and the female subsample, less frequent use of avoidance (AOR = 0.64, 0.68, p < .001) and self-medication coping (AOR = 0.79, 0.78, p < .05), less decision authority-related work stress (AOR = 0.85, 0.82, p < .05), and less social support-related work stress (AOR = 0.87, 0.89, p < .05) were associated with reduced odds of any mental disorder since 2002. Within the full sample only, less psychological demand and physical exertion-related work stress in 2018 were associated with reduced odds of any mental disorder since 2002 (AOR = 0.79, 0.67, p < .01).
Less skill discretion-related work stress in 2018 was associated with increased odds of any mental disorder since 2002 among the full sample (AOR = 1.19, 95% CI [1.01–1.41], p < .05).
Comparison with Non-MST Subsample
Post-hoc sensitivity analyses descriptively examined trends among participants who did not experience MST. The prevalence of any mental disorder since 2002 was lower compared to the MST subsample (42.2% vs. 66.5%). Similarly to the MST subsample, those with no mental disorder since 2002 were older and the prevalence of any mental disorder was lower for those of higher rank and on active duty. Unlike the MST subsample, the prevalence of any mental disorder was lower among those who were White, married, and had higher income. Consistent across groups, those without a mental disorder since 2002 used less avoidance coping (2002 & 2018) and self-medication coping (2018), used more active coping (2018), and reported increased social support (2018) and less support-related work stress (2018). Unlike the MST subsample, those without a mental disorder reported increased social support in 2002 compared to those with a mental disorder. There were also larger mean discrepancies across variables (for any mental disorder vs. no mental disorder) for the MST subsample compared to the non-MST subsample. For an in-depth comparison of sample characteristics between participants with and without MST, see Mota et al. 6
Discussion
This study comprehensively examined protective factors and correlates of mental disorders among a population-based sample of CAF MST survivors. Strengths include the use of a diagnostic interview to assess mental disorders, examination of sex differences, the use of longitudinal data, the population-based sample, and the inclusion of various protective factors. The prevalence of MST in the current sample was 9.6% (females: 44.6%, males: 4.8%), which varies from prior research (see Mota et al. 6 for discussion). Results identified sample characteristics (e.g., active duty) and psychosocial factors (e.g., coping styles, support) that may be protective against mental disorders among those who have experienced MST, with some variability across sexes (see Table 5). Results may contribute to intervention strategies to mitigate adverse mental health impacts of MST.
Summary of Emergent Protective Factors and Correlates for Any Mental Disorder Since 2002 Among Survivors of Military Sexual Trauma (n = 455).
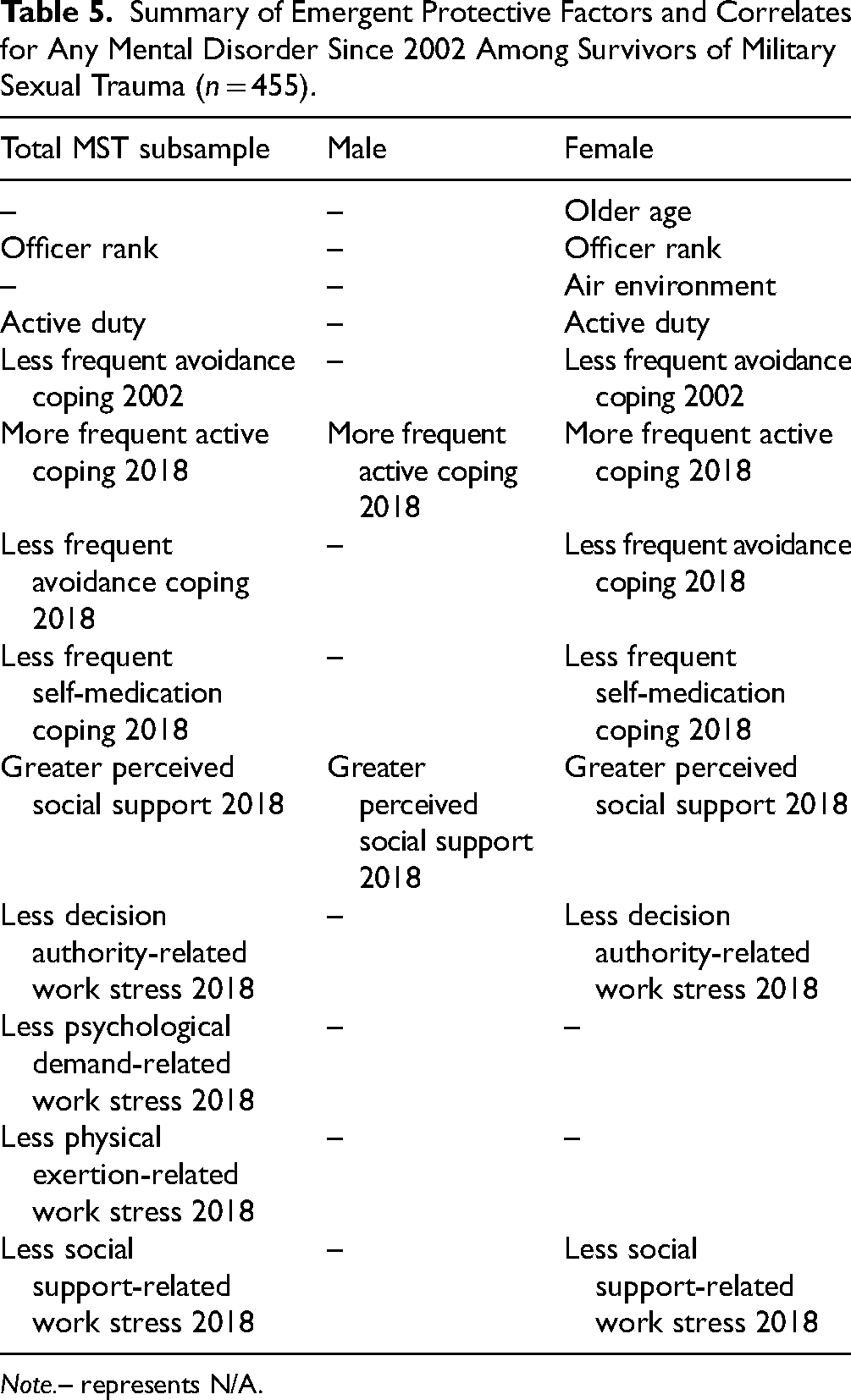
Note.– represents N/A.
Regarding sample characteristics, having a higher rank or being on active duty were associated with reduced odds of any mental disorder in 2002. Among females, in addition to being on active duty, being older in age, higher in rank, and working in an air environment were also associated with reduced odds of any mental disorder. This is largely consistent with broader military and Veteran samples (regardless of MST exposure) showing elevated rates of mental disorders among lower ranks, Veterans, and those who are younger in age.22–25 Findings support the importance of focused mental health screening for MST survivors, particularly among those who are younger, lower rank, and Veterans. Regarding military environment, in our previous work within this sample, we found that females working in an air environment were more likely to report experiencing MST compared to females in a land environment. 6 Though this likely does not fully explain the current study's finding, perhaps the elevated prevalence of MST within this environment supports a sense of shared experience among these females, which could mitigate adverse mental health impacts. Alternatively, there could be important sample characteristics of females working in an air environment (e.g., variable proportions of those on active duty), or differences in military culture (e.g., beliefs about showing emotion) across environments, that may help explain this finding.
Regarding psychosocial factors, less frequent use of avoidance coping strategies (e.g., sleeping more than usual, avoiding being with people) was the only protective factor against any mental disorder since 2002 across time points. Although some forms of avoidance can be helpful in the short term for managing specific types of stressors (e.g., uncontrollable, short-lived), considerable research demonstrates associations between avoidance coping and adverse health outcomes (e.g., poorer mental health, physical symptoms, risky health behaviours, frequent hospitalizations, reduced medical compliance).19,26–28 The other most robust protective factors that emerged were more frequent use of active coping (e.g., problem-solving, talking to others) in 2018 and greater perceived social support in 2018. The significance of these factors in 2018 may suggest an element of temporal relevance. In other words, the mental disorders may have developed long enough after 2002 that the psychosocial correlates assessed in 2002 were less relevant by then. Active coping and social support are also well-established correlates of enhanced mental health,19,26,29,30 rendering these findings unsurprising.
Various elements of work-related stress in 2018 also emerged as protective, although with differences depending on the specific group. In particular, reduced psychological demand and physical exertion-related work stress (i.e., less stress related to mental workload and physical demands) was protective among the total sample only, whereas reduced decision authority (i.e., less stress related to job autonomy) and reduced social support-related work stress (i.e., less interpersonal job stress) were protective among females and the total sample. Prior research has revealed sex differences in elements of work that contribute to greater stress, both in the general population 31 and Canadian military-specific research. 32 These differences may contribute to the emergent results.
Less frequent use of self-medication coping in 2018 among females and the total sample was the only other emergent protective factor. Self-medication is a common form of coping with psychological distress among those with a mental disorder,33,34 and is more commonly used among males compared to females. 33 It is possible that the sex difference in the frequency of self-medication use may be implicated in the current study's finding among females and not males.
Finally, reduced skill discretion-related work stress in 2018 (total sample) was associated with increased odds of any mental disorder since 2002. This dimension of stress refers to the breadth of skills that can be learned and used at work. Although typically lower stress is associated with improved mental health, perhaps “lower stress” for this construct may translate to frustration, boredom, or other negative emotions. Prior research found that elevated skill discretion was associated with reduced emotional exhaustion and intention to leave, and greater well-being and job satisfaction. 35 Perhaps some degree of skill discretion-related stress may be adaptive, though this should be examined explicitly.
Taken together, results may help identify intervention targets for MST survivors. As noted above, MST survivors who are lower rank or Veterans, alongside younger females and females in a land environment, may benefit from closer mental health screening to facilitate early intervention opportunities. For those seeking treatment, targeting the reduction of avoidance and self-medication coping and promoting more active coping styles may support improvements in mental health. Helping clients understand how avoidance and self-medication, despite having some short-term perceived benefits, can also have adverse long-term impacts may be important to facilitate motivation for change. Efforts to enhance social support among MST survivors may also be beneficial, such as through MST support groups or group treatment options. Current gold-standard trauma-focused interventions include prolonged exposure, cognitive processing therapy, and eye movement desensitization and reprocessing. Future research could explore if modifications to these protocols are warranted for MST-specific samples. In addition, it is important that there is awareness of the prevalence of MST at all levels of the CAF and continued efforts toward reducing MST. Finally, helping MST survivors apply more adaptive coping strategies to help manage workplace stress (and/or having leadership assess ways to reduce sources of work stress when possible) may have mental health benefits.
Despite the important findings and implications of this study, it is not without limitations. First, although analyses identified factors associated with mental disorders, the methodology of this study does not permit causal assumptions to be made. In some cases, temporal assumptions also cannot be made (e.g., mental disorder onset may precede a change from active duty to veteran status). Second, although we stratified analyses to better understand sex differences, we were unable to examine gender differences (including examination of LGBTQ+ identifying personnel), as gender identity was not assessed within the survey. Third, due to small cell sizes, certain findings could not be released, in line with Statistics Canada regulations. Fourth, the surveys assessed DSM-IV criteria for mental disorders (to maintain consistency with the 2002 assessment), which is no longer the most contemporary criteria. In particular, there were notable changes to PTSD criteria within DSM-5; results may not reflect the true prevalence of mental disorders since 2002. Finally, although the survey was anonymized, there are various reasons why participants may have chosen not to disclose a history of MST or a mental disorder. Thus, results likely represent underestimates.
The current study established sex-stratified prevalence estimates of having a mental disorder among a population-based sample of MST survivors and identified protective correlates of having a mental disorder within this population. This study extends and compliments a host of quantitative and qualitative research aimed at understanding MST. Future research should evaluate the potential utility of integrating the intervention targets outlined above. In addition, efforts to prevent MST remain a priority to improve health outcomes among this population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a CIMVHR Wounded Warriors of Canada Doctoral Scholarship (J.L.S.).