
Abstract
Objective:
This study examined baseline risk and protective predictors and interim correlates of the persistence/recurrence, remission, and onset of posttraumatic stress disorder (PTSD) in a 16-year prospective, nationally representative sample of Canadian Forces members and veterans.
Methods:
The 2018 Canadian Armed Forces Members and Veterans Mental Health Follow-up Survey is a prospective study of 2,941 regular force service members and veterans who participated in the 2002 Canadian Community Health Survey on Mental Health and Wellbeing: Canadian Forces Supplement (n = 5,155; ages 15 to 64 years; response rate 68%). PTSD diagnoses in 2002 and 2018 were used to create 4 groups: (1) no lifetime, (2) remitted, (3) new onset, and (4) persistent/recurrent PTSD. Multinomial regressions were conducted to identify predictors of PTSD courses.
Results:
Female sex, being a junior noncommissioned member (vs. officer), and land (vs. air) operations in 2002 were associated with all PTSD courses relative to no lifetime PTSD (relative risk ratio [RRR] range: 1.28 to 3.65). After adjusting for sociodemographic variables, baseline predictors of all PTSD courses included lifetime mental disorder, history of mental health care utilization, all trauma type categories (deployment-associated, sexual, “other”), and the number of lifetime traumatic events (RRR range: 1.14 to 8.95). New (“since 2002”) traumas, transitioning to veteran status, and alcohol dependence were mostly associated with the new onset and persistent/recurrent PTSD courses (RRR range: 1.79 to 4.31), while mental health care utilization and greater avoidance coping were associated with all PTSD courses (RRR range: 1.10 to 17.87). Protective factors for several PTSD courses at one or both time points included social support, social network size, and problem-focused coping (RRR range: 0.71 to 0.98).
Conclusions:
This is the first population-based survey to examine the longitudinal course of PTSD in Canadian Forces members. Prevention and intervention programs focused on bolstering social support and active coping strategies as possible protective factors/correlates may help mitigate the development and persistence of PTSD.
Posttraumatic stress disorder (PTSD) is a prevalent mental disorder that may occur following trauma exposure and is even more prevalent among certain occupational groups who are at higher risk for experiencing trauma. In the Canadian Armed Forces (CAF), the prevalence of PTSD appears to be increasing, with past-year PTSD nearly doubling from 2.8% in 2002 to 5.3% in 2013. 1 The mental and physical health conditions that often co-occur with PTSD have been well documented, 1,2 as have the deleterious effects of this disorder on personal, social, and work functioning. 3,4 Although previous research has examined the development and persistence of PTSD in military samples, population-based, prospective studies remain limited.
Studies examining the longitudinal course of PTSD symptoms in military populations have demonstrated that a considerable minority (i.e., 10% to 13%) continues to experience clinically significant symptoms long after baseline assessment. 5 –7 Notably, some studies have found a persistent course of PTSD symptoms to be even more prevalent than this range. 8 In a representative U.S. sample of Vietnam War veterans, 10.8% of men and 8.7% of women had current subthreshold or threshold PTSD diagnoses 40 years or more following the war. 9 Some studies have demonstrated that symptoms can worsen over time or that onset may be delayed, 6,7,10 –12 and others have reported that PTSD symptoms may decrease or remit over time. 6,7 However, the vast majority of individuals—typically between 80% and 90%—remain resistant/resilient to the effects of trauma exposure. 6,11
Several studies have prospectively examined predictors of PTSD in military samples, with findings converging on a number of common risk factors—female sex, 13,14 combat exposure and deployment-related experiences, 5,7,15,16 previous or current mental health difficulties, 7,15 substance misuse or a substance use disorder, 7 a greater overall trauma load, 15 and a history of childhood adversity. 7,10 Lower social support and community integration have also been linked to symptomatic PTSD trajectories. 16,17 Finally, religiosity and spirituality have been found to be associated with lower odds of probable PTSD in some cross-sectional studies, 18 and adaptive and maladaptive coping strategies (e.g., positive emotion-focused coping and self-blame coping) have also been found to be protective or risk correlates for PTSD, respectively. 19
While extant prospective studies of PTSD in military service members and veterans have helped inform understanding of the courses and risk factors for PTSD, they have notable limitations. First, most studies have been conducted in nonrepresentative samples and with self-report measures assessing PTSD symptoms rather than diagnostic interviews. Second, most studies have employed briefer follow-up periods, with little opportunity of understanding PTSD symptoms persisting past a decade. Third, no studies have examined the course of PTSD in CAF members specifically, using a nationally representative sample.
To address these limitations, we sought to examine the nature and determinants of PTSD courses in a prospective, 16-year population-based study of regular force CAF members and veterans from 2002 to 2018. We hypothesized that female sex, deployment experiences, traumatic exposures, and other mental disorders would be associated with PTSD courses relative to no PTSD 14,20 –22 and that persistent PTSD would be associated with more mental health comorbidity, trauma exposure, and lower social support and problem-focused coping than the remitting course. 23 –25
Methods
Sample
The 2018 Canadian Armed Forces Members and Veterans Mental Health Follow-up Survey (CAFVMHS) is a nationally representative follow-up study of regular force service members and veterans who participated in the 2002 Canadian Community Health Survey on Mental Health and Wellbeing: Canadian Forces Supplement (CCHS-CF). The CCHS-CF included n = 5,155 regular force personnel aged 15 to 64 years, and n = 2,941 (response rate: 68%) of these respondents participated in the 2018 follow-up survey. Overall, participants were similar to nonparticipants; predictors of attrition included younger age and serving in land operations. 26 Additional details about the survey methodology can be found elsewhere. 27 –29
Assessments
Sociodemographic and military variables
The following variables were assessed at baseline: sex (male, female), race/ethnicity (white, non-white), age (continuous), marital status (married/common-law, separated/widowed/divorced, single/never married), household income (
Deployment status
In 2002, respondents were asked whether they had ever been on deployments of 3 months or more. In 2018, they were asked whether they had been on any deployments since 2002.
Trauma exposure
As part of the World Health Organization Composite International Diagnostic Interview (WHO-CIDI) PTSD module, respondents were asked about lifetime exposure to 28 potentially traumatic events in 2002 (e.g., involvement in combat and peacekeeping operations, sexual assault, accident, or some other unexpected event). 30,31 Bivariate regression analyses were conducted between each traumatic event and lifetime deployment status, and events that were positively associated with deployment formed a summary “deployment-associated traumatic events” variable. Remaining events were collapsed into “any sexual trauma” and “other” trauma categories. New exposures to these events since 2002 were reassessed in 2018, and the same 3 summary categories were examined as interim correlates. Number of traumatic event variables in 2002 (lifetime) and in 2018 (since 2002) were also examined.
Childhood adversities
In 2002, respondents were asked about some possible adversities as a child or teenager, including a hospital stay of 2+ weeks, parental divorce/separation, parental unemployment, problematic parental alcohol or drug use, apprehension by child protection services, being badly beaten by parents/guardians, and witnessing domestic violence. Respondents were also asked about lifetime sexual trauma with 2 items, with age-of-onset of these traumas was also assessed and used to determine sexual trauma occurring before the age of 18 years. Consistent with previous work, 32 responses to these items were used to create 2 variables—“any childhood adversity” (yes/no) and “number of childhood adversities” (possible range 0 to 9).
PTSD and other mental disorders
The WHO-CIDI is a structured diagnostic interview that was used by trained lay interviewers to assess mental disorders according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria. The validity and reliability of this instrument have been well established. 33,34 The WHO-CIDI assessed lifetime PTSD in 2002 and PTSD “since 2002” in 2018. Diagnoses in 2002 and 2018 were used to create the following 4-level variable: (1) no lifetime PTSD diagnosis in 2002 and no PTSD diagnosis “since last interview” (no lifetime PTSD); (2) lifetime diagnosis in 2002 but no diagnosis since 2002 (remitted); (3) no lifetime diagnosis in 2002, but since 2002 diagnosis (new onset); (4) lifetime diagnosis in 2002 and since 2002 diagnosis (persistent/recurrent). Participants with an unknown or missing PTSD diagnostic status at either time point were excluded from this variable.
Other lifetime mental disorders assessed in 2002 included major depressive episodes, panic disorder, social phobia, and generalized anxiety disorder, which were combined to create an “any non-PTSD mental disorder” variable. Alcohol dependence “since last interview,” assessed in 2018, was also included in this study.
Mental health services utilization
Mental health services used in 2002 (lifetime time frame) and since 2002 were assessed by asking respondents whether they had contact with the following professionals about their emotions, mental health, or substance use: Psychiatrist, psychologist, family doctor, other medical doctor, nurse/nurse practitioner/physician’s assistant/medic, social worker/counsellor/psychotherapist, religious/spiritual advisor, or other. Responses were summed to create dichotomous (yes/no) variables for any lifetime mental health care utilization in 2002 and utilization since 2002.
Social support and social network size
Social support was assessed with the Medical Outcomes Study Social Support Survey in 2002 and 2018. 35 This measure consists of 19 items, each rated on a 0 to 4 Likert scale (None to All of the Time), assessing active social interaction, tangible, affection, and emotion or information-based types of social support. Item responses were summed to create a continuous variable (range 0 to 76) at both time points, with higher scores indicating higher levels of support. Social network size was assessed by asking respondents about their number of close friends and relatives.
Coping
In 2002 and 2018, respondents were asked about their frequency of use of several coping strategies with items derived from the Coping Inventory to Problems Experienced (COPE) Scale, the Ways of Coping Questionnaire, and the Coping Strategy Indicator. 28 Examples included trying to solve the problem, feeling better by drinking alcohol, and relaxing by doing something enjoyable. Items were rated on a 4-point Likert scale from “often” to “never.” A previous factor analysis of these items suggested a three-factor solution: Active coping (4 items), avoidance coping (5 items), and self-medication (2 items). 36 These coping types were examined separately as continuous variables at both time points.
Religiosity and spirituality
In 2002, frequency of past-year religious service attendance was assessed on a 5-point Likert scale from “never” to “at least once per week.” Responses were dichotomized into less than once per month versus once per month or more.
Work stress
Work stress in 2002 and in 2018 was assessed with a 12-item measure based on items from the Job Content Questionnaire. 37 Items assessed 6 dimensions of work stress (i.e., decision authority/control, job insecurity, psychological demand, physical exertion, social support from colleagues/supervisors, and skill discretion/demand) on a 5-point Likert scale from “strongly agree” to “strongly disagree.” Items were summed to create a total work stress score. Analyses examining work stress in 2018 as a potential correlate of PTSD courses were restricted to those individuals who were in active duty or were employed at the time of the interview.
Statistical Analyses
Analyses were conducted using STATA/MP (Version 16). 38 Weights calculated by Statistics Canada were applied to all inferential analyses to ensure representativeness of all Canadian Forces members in 2002. Bootstrapping was used as a standard error estimation technique to account for the survey’s complex sampling design. Weighted cross-tabulations were used to examine the prevalence of each variable among the 4 PTSD courses. A series of multinomial regressions adjusted for sociodemographic variables were conducted to examine the associations between each potential baseline predictor, interim correlate, and persistent/recurrent, remitted, and new onset PTSD courses relative to no lifetime PTSD. To understand factors associated with persistence relative to recovery from PTSD, the remitting and persistent/recurrent PTSD courses in the multinomial models were also compared.
Results
The response rate of the CAFVMHS was 68%. As previously reported, 27 78.6% of the sample had no lifetime PTSD, 14.5% had new-onset PTSD, 4.1% had remitted PTSD, and 2.7% had persistent/recurrent PTSD. Table 1 displays the prevalence of sociodemographic and military demographic variables at baseline for each of the 4 PTSD courses, as well as the results of unadjusted, multinomial regression analyses examining associations between each of these variables and PTSD courses. Relative to individuals with no lifetime PTSD, all PTSD courses were positively associated with being female, being a junior noncommissioned member (vs. officer), and serving on land (vs. air). Older age was negatively associated with the new onset course; and having a household income of CAD$49,999 or less (vs. CAD$50,000 or more), being widowed/separated/divorced (vs. married/cohabiting), a senior noncommissioned officer (vs. officer), and serving in a sea (vs. air) environment were positively associated with select courses. Relative to the remitting PTSD course, individuals in the persistent/recurrent PTSD course were more likely to be female.
Sociodemographic Predictors of Remission, New Onset, and Persistence/Recurrence of PTSD.
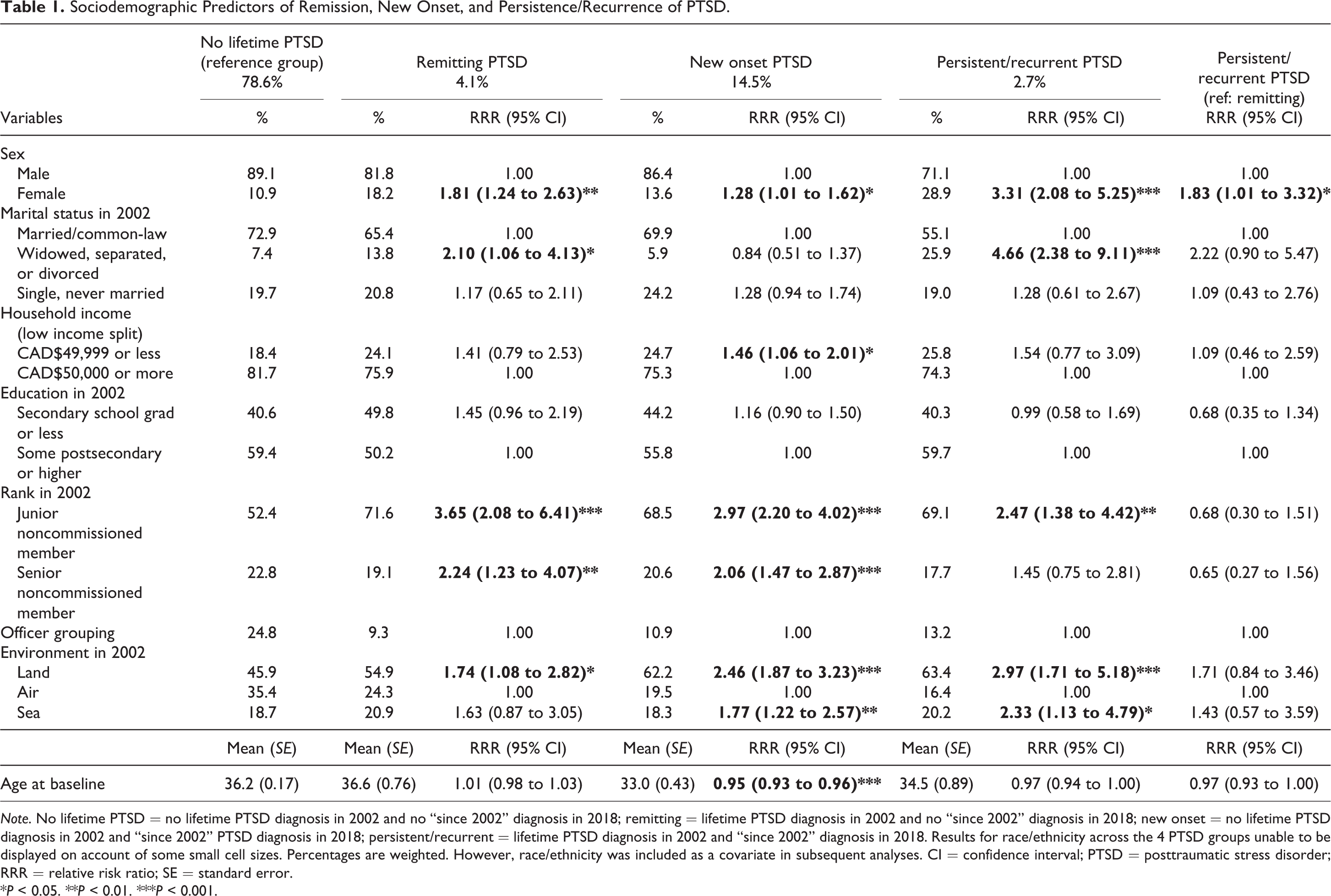
Note. No lifetime PTSD = no lifetime PTSD diagnosis in 2002 and no “since 2002” diagnosis in 2018; remitting = lifetime PTSD diagnosis in 2002 and no “since 2002” diagnosis in 2018; new onset = no lifetime PTSD diagnosis in 2002 and “since 2002” PTSD diagnosis in 2018; persistent/recurrent = lifetime PTSD diagnosis in 2002 and “since 2002” diagnosis in 2018. Results for race/ethnicity across the 4 PTSD groups unable to be displayed on account of some small cell sizes. Percentages are weighted. However, race/ethnicity was included as a covariate in subsequent analyses. CI = confidence interval; PTSD = posttraumatic stress disorder; RRR = relative risk ratio; SE = standard error.
*P < 0.05. **P < 0.01. ***P < 0.001.
Table 2 shows the prevalence and associations of trauma-related, mental health, and psychosocial variables at baseline across each of the 4 PTSD courses, adjusting for all variables in Table 1. A lifetime mental disorder other than PTSD, any deployment-associated traumatic experience, sexual or “other” traumatic experience, greater number of lifetime traumas, and a history of mental health care services utilization were associated with all PTSD courses relative to no lifetime PTSD. History of deployment, exposure to childhood adversity and number of childhood adversities, religious service attendance once a month or more, greater work stress, and a higher frequency of avoidance and self-medication coping were also positively associated with some PTSD courses. Level of perceived social support and higher social network size were negatively associated with select PTSD courses. Finally, endorsing lifetime deployment as well as any deployment-associated traumatic experience (and specifically, engagement in peacekeeping operations and a life-threatening accident), a higher number of traumatic events, and more frequent avoidance coping were positively associated with the persistent/recurrent relative to the remitting PTSD course.
Baseline Predictors of PTSD Course, Adjusted for Table 1 Demographics.
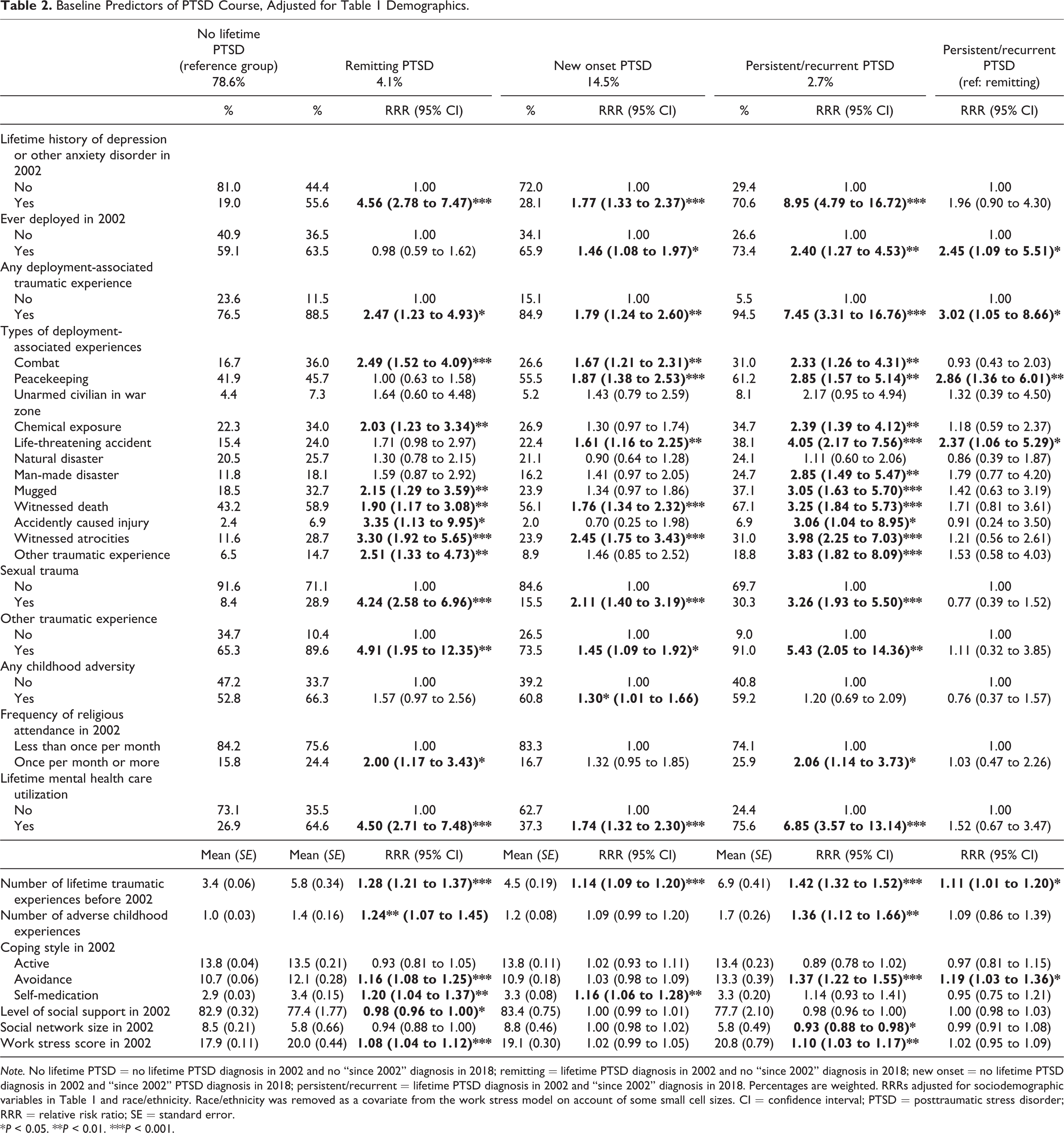
Note. No lifetime PTSD = no lifetime PTSD diagnosis in 2002 and no “since 2002” diagnosis in 2018; remitting = lifetime PTSD diagnosis in 2002 and no “since 2002” diagnosis in 2018; new onset = no lifetime PTSD diagnosis in 2002 and “since 2002” PTSD diagnosis in 2018; persistent/recurrent = lifetime PTSD diagnosis in 2002 and “since 2002” diagnosis in 2018. Percentages are weighted. RRRs adjusted for sociodemographic variables in Table 1 and race/ethnicity. Race/ethnicity was removed as a covariate from the work stress model on account of some small cell sizes. CI = confidence interval; PTSD = posttraumatic stress disorder; RRR = relative risk ratio; SE = standard error.
*P < 0.05. **P < 0.01. ***P < 0.001.
Table 3 shows associations of interim variables across each of the 4 PTSD courses after adjusting for Table 1 variables. Relative to no lifetime PTSD, mental health care utilization since 2002 and a higher frequency of avoidance coping in 2018 were positively associated with all PTSD courses, while more problem-focused coping was negatively associated with all PTSD courses. Fewer years of service were associated with the persistent/recurrent PTSD course, while transitioning to veteran status, new (since 2002) deployment-associated trauma exposure, sexual and “other” trauma exposures, number of traumatic events since 2002, alcohol dependence since 2002, and greater work stress were associated with the new onset and/or persistent/recurrent PTSD courses, but not with the remitting course. Deployment since 2002 was positively associated with the new onset PTSD course but negatively associated with the persistent/recurrent course. Higher levels of perceived social support were negatively associated with the new onset and persistent/recurrent PTSD courses. Compared to the remitting PTSD course, the persistent/recurrent course was characterized by a higher likelihood of mental health care utilization, a higher likelihood of new exposures to all trauma types, a higher number of new traumas, more avoidance coping, and less problem-focused coping.
Interim Correlates of PTSD Course, Adjusted for Table 1 Demographics.
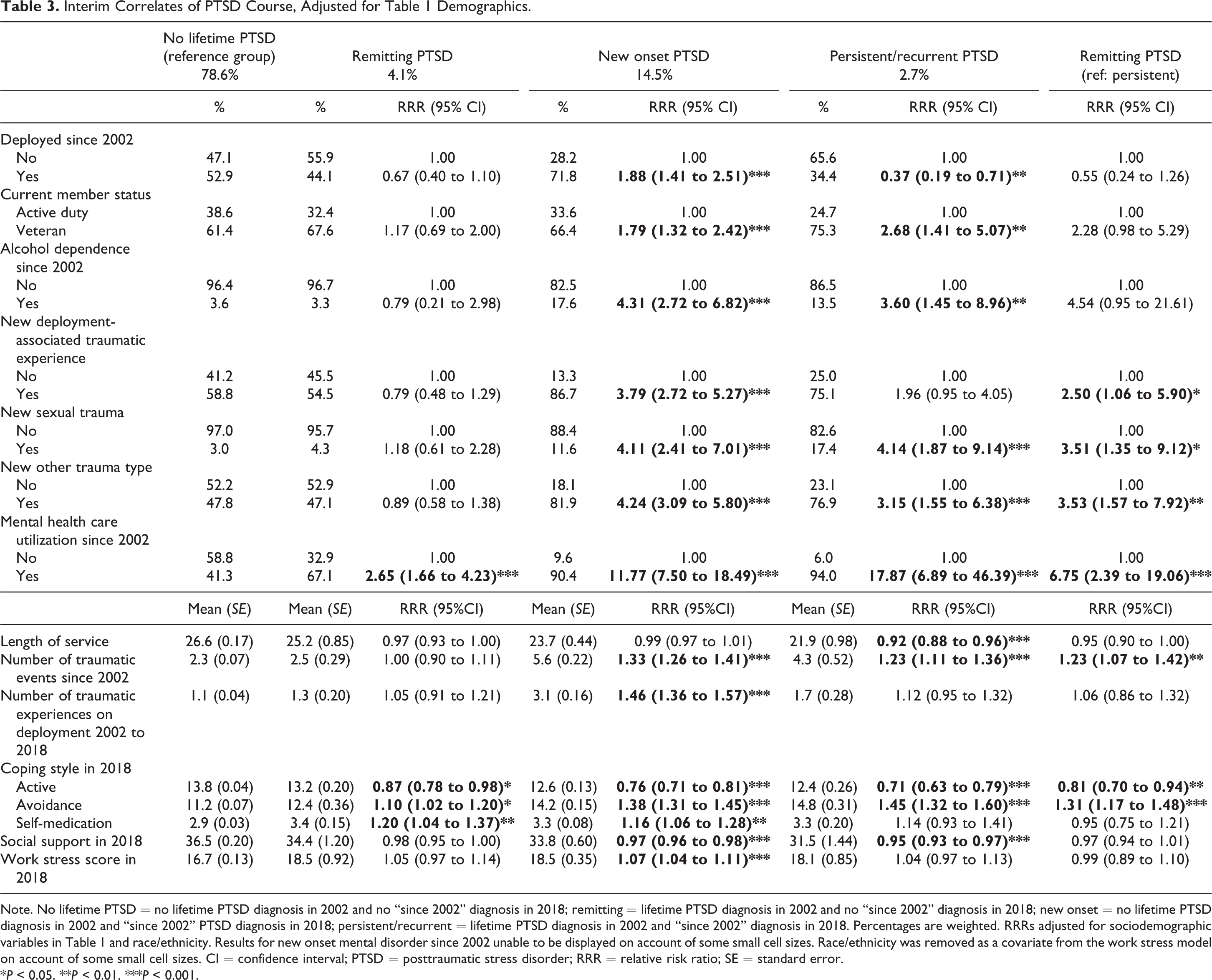
Note. No lifetime PTSD = no lifetime PTSD diagnosis in 2002 and no “since 2002” diagnosis in 2018; remitting = lifetime PTSD diagnosis in 2002 and no “since 2002” diagnosis in 2018; new onset = no lifetime PTSD diagnosis in 2002 and “since 2002” PTSD diagnosis in 2018; persistent/recurrent = lifetime PTSD diagnosis in 2002 and “since 2002” diagnosis in 2018. Percentages are weighted. RRRs adjusted for sociodemographic variables in Table 1 and race/ethnicity. Results for new onset mental disorder since 2002 unable to be displayed on account of some small cell sizes. Race/ethnicity was removed as a covariate from the work stress model on account of some small cell sizes. CI = confidence interval; PTSD = posttraumatic stress disorder; RRR = relative risk ratio; SE = standard error.
*P < 0.05. **P < 0.01. ***P < 0.001.
Discussion
This is the first known study to prospectively examine courses of PTSD over a 16-year period in a nationally representative Canadian military sample. New-onset PTSD was the most prevalent symptomatic course (14.5%), followed by remitting (4.1%) and persistent/recurrent (2.7%) courses. Although not directly comparable, the proportion of remitting cases is most similar to previous research, while estimates of new-onset and persistent courses appear more variable across studies, 7,12,23,39 possibly due to differences related to time since trauma occurrence or demographic and military characteristics. Consistent with previous research 14 and compared to no lifetime PTSD, all PTSD courses were positively associated with being female, a junior noncommissioned member (relative to an officer), and in land operations (relative to air). Other characteristics were also associated with some PTSD courses. While the underlying mechanisms driving the higher burden of PTSD among women continue to be investigated, hormonal effects and sex differences in the encoding and consolidation of fear memories have been proposed. 40 –42 Regarding operational environment, it is possible that the higher likelihood of PTSD among individuals in land operations may be indicative of greater combat exposure. That lower ranks were associated with a greater likelihood of membership in PTSD courses may also imply higher exposure to military trauma or the role of training and perceived preparedness in mitigating against trauma-related symptoms. 23 Becoming a veteran between 2002 and 2018 was also positively associated with the new-onset and persistent/recurrent PTSD courses relative to no lifetime PTSD. Although myriad research has documented the high rates of PTSD and other mental health conditions among veterans, 43 –45 to our knowledge, this is the first population-based survey to capture the impact of transitioning to life after service. These findings highlight the need for availability of both formal and informal supports during this key period of change.
Lifetime mental disorder, any lifetime mental health service use, number of lifetime traumatic events, and history of deployment-associated trauma exposure, and sexual and “other” trauma exposure at baseline were found to be associated with all PTSD courses. Childhood adversity, lifetime deployments, and higher levels of work stress were also associated with some PTSD courses. Not surprisingly, new trauma exposures since 2002 were mostly associated with the new-onset and persistent/recurrent PTSD courses, but not with the remitting course. Although greater trauma load has consistently been associated with PTSD symptom courses in military samples, 17,46,47 the current study indicates that deployment-associated traumatic events are not necessarily the most notable traumas in contributing to PTSD development and persistence. These findings underscore the importance of timely assessment and treatment of symptoms in relation to a broad range of traumas. In line with previous literature, 14,17 the current findings demonstrate the role of psychiatric comorbidity in the development and persistence of PTSD, highlighting the possible need for early intervention and transdiagnostic approaches to the treatment of mental disorders.
Relative to no lifetime PTSD, adjusted models also showed positive associations between a higher frequency of avoidance and self-medication coping at baseline and select PTSD courses, while more frequent religious service attendance at baseline was also surprisingly positively associated with the remitting and persistent/recurrent courses. Self-medication coping in 2018 was not associated with any PTSD course; however, avoidance coping in 2018 was significantly and positively associated with all PTSD courses. This is among the first population-based studies to demonstrate that military service members living with PTSD may have a propensity toward avoidance coping (e.g., isolating from others, self-blame) and self-medicating stress with substances. Findings also support prior research suggesting a longitudinal association between avoidance coping and PTSD symptom severity in military and veteran samples. 48,49 On the other hand, temporality remains difficult to discern even in this longitudinal study, since it is possible that individuals experienced trauma-related symptoms before the baseline assessment. Future research is needed to evaluate these directional relationships.
Social support and social network size at baseline were negatively associated with the remitted and persistent/recurrent PTSD courses, respectively, relative to no lifetime PTSD, and perceived social support in 2018 was negatively associated with the new onset and persistent/recurrent courses. Frequency of problem-focused coping in 2002 was not associated with any PTSD course; however, a higher frequency of problem-focused coping in 2018 was negatively associated with all symptom courses. A growing number of longitudinal studies in military and veteran samples have documented the potential mitigating role of social support for PTSD, 16,17,50 and problem-focused coping has also been shown to be inversely associated with PTSD symptoms. 50,51 The effectiveness of existing peer support initiatives for CAF members and veterans, such as the Operational Stress Injury Social Support network, should be scientifically evaluated. With regard to problem-focused coping, although its use does not appear to be effective as a preventative strategy for PTSD, initiatives targeting the use of positive coping skills for members and veterans may serve an important role in buffering against or combating ongoing symptoms. Further, given associations between PTSD and impairments in social functioning, 52 the integration of interpersonal effectiveness skills training into trauma-focused psychotherapies may serve to improve social support and protect against longer-term symptoms of PTSD.
In order to understand predictors and correlates of persistent PTSD, we conducted an additional comparison of the persistent/recurrent compared to the remitting PTSD course. Relatively few baseline predictors were identified, among them, a higher likelihood of being female, endorsement of lifetime deployments and exposure to any deployment-associated trauma, a higher number of lifetime traumatic experiences overall, and more frequent avoidance coping. However, more interim variables distinguished between these courses, including a higher likelihood of mental health care utilization since 2002, new trauma exposures and a higher number of new traumatic events, a higher frequency of avoidance coping, and a lower frequency of problem-focused coping. Although reducing avoidance is an important target of cognitive-behavioral interventions for PTSD, 53,54 the current findings suggest that an even earlier focus on the deleterious impact of avoiding difficult emotions and situations may be warranted. The inclusion of more problem-focused approaches to reduce avoidance, as well as the role of distress tolerance skills in managing trauma-related emotional reactions, should be explored as part of possible recovery from PTSD. 55,56
The notable strengths of this study include its national representativeness, long-term, 16-year prospective follow-up period, diagnoses assessed using structured, diagnostic interviews, and assessment of a broad array of both risk and protective factors. However, the current study had a number of limitations. First, some constructs may have been affected by recall bias when the time frame of assessment was lifetime or since 2002. Further, with the 16-year gap between the 2 time points, it was not possible to examine fluctuations in PTSD diagnosis over time from baseline to follow-up or to assess the temporal impact of PTSD on new life events. Future studies should aim to include multiple time points in order to examine PTSD symptom trajectories, that is, more dynamic patterns of resistance/resilience, chronicity, remission, and onset of PTSD over several years. 12,15 Second, although we examined a range of potential predictors and correlates of PTSD course, there were a number of constructs that were not assessed, including peritraumatic dissociation, personality factors, and psychological inflexibility. 57 –59 Third, given that baseline symptoms were assessed using DSM-IV criteria, we used these rather than Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria in 2018. Fourth, although few predictors of attrition were identified in the CAFVMHS, courses and predictors of PTSD may have been impacted by the lower response rate of the second survey time point. Finally, although mental disorders were assessed using a computer-assisted, fully structured diagnostic interview, potential predictors and correlates were assessed via self-report.
Despite these limitations, this study was the first to examine predictors and correlates of PTSD courses in a nationally representative sample of CAF members and veterans over a 16-year period. Results suggest that interventions focused on minimizing trauma exposure, supporting members through their transition to veteran status, increasing social support and problem-focused coping, and decreasing avoidance coping could mitigate PTSD symptoms. Future studies are needed to elucidate temporal associations between predictors and PTSD symptom trajectories over time; identify biopsychosocial mechanisms underlying symptomatic PTSD courses; and evaluate the efficacy of prevention and treatment efforts targeting evidence-based risk and protective factors for PTSD.
Footnotes
Authors’ Note
The authors are not permitted to share the data analyzed from the current study, however, those interested can apply for data access via the Canadian Research Data Centers.
Acknowledgments
The coauthors acknowledge the larger group of CAFVMHS investigators for their contributions to data collection and survey design.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Canadian Institutes of Health Research Foundation grant (#333252; PI: Sareen), True Patriot Love; Canadian Institutes of Military Veterans Health Research; University of Manitoba, Rady Faculty of Health Sciences Research Start-up Funds (Mota & El-Gabalawy); Canadian Institute for Military and Veteran Health Research Mark Zamorski Award (Sommer); U.S. Department of Veterans Affairs National Center for Posttraumatic Stress Disorder (Pietrzak).