
Abstract

To the Editor,
Postprocedural urinary retention is a distressing complication. It has been our observation that some patients undergoing electroconvulsive therapy (ECT) under general mask anesthesia develop postprocedural urinary retention. This is an unexpected postprocedural complication considering the brevity of the ECT procedure and limited use of anesthetic agents. Contemporary literature does not provide information on the rate or risks for urinary retention after ECT. Our institution has an active ECT practice which provides an opportunity to investigate post-ECT urinary retention with the aims of calculating its incidence and assessing for potential association with clinical variables. Specifically, we hypothesize that post-ECT urinary retention is associated with periprocedural administration of anticholinergic agents, which are administered to treat postictal bradyarrhythmias or sialorrhea. 1
This study included consecutive adult patients who underwent ECT under general mask anesthesia at our institution, from May 5, 2018, to February 24, 2023, and provided prior written authorization for review of their medical records. Patients on hemodialysis and those with indwelling catheters or undergoing regular intermittent urinary catheterization were excluded.
Anesthetic management consisted of general mask anesthesia typically induced with etomidate and muscle relaxation with succinylcholine. Anticholinergic agents (glycopyrrolate, atropine) were administered to treat postictal bradydysrhythmias or sialorrhea. Post-procedurally, patients returned to an inpatient psychiatric ward or return home following recovery. Patients unable to void following ECT were evaluated by a specialized bladder catheterization team which placed a urinary catheter if urinary retention was diagnosed.
Electronic medical records were abstracted for demographics, home use of anticholinergic medications (tricyclic antidepressants, phenothiazines, diphenhydramine, and other psychiatric medications with anticholinergic burden [footnote Table 1]), cardiovascular disease, central nervous system diseases [e.g., dementia, stroke], diabetes mellitus, anesthetic induction agent (etomidate vs other) and periprocedural anticholinergic medication administration. All patients who had documentation of bladder catheter placement or urology consultation within 24 h of ECT underwent manual chart review to confirm a diagnosis.
Post-ECT urinary retention was the primary outcome of interest. It was defined as the inability to void post-ECT, requiring new urinary catheterization. Urinary retention was analyzed using Generalized Estimating Equations with a logit link (analogous to logistic regression) and robust “sandwich” covariance estimates to account for individuals undergoing multiple ECT treatments. Both univariable and multivariable analyses were performed. The results of the multivariable analysis are summarized by presenting odds ratios with 95% confidence intervals. The analyses were conducted by using SAS software, v9.4 (SAS Institute Inc).
We identified 776 patients who underwent a total of 10,834 ECT treatments. Seven patients underwent 90 treatments that did not meet inclusion criteria (2 on hemodialysis, 2 had indwelling catheters, and 3 regularly underwent intermittent catheterization). This left 769 patients who underwent 10,744 ECT treatments, with a median of 8 [interquartile range 6–12] ECT treatments per patient (treatment range 1–251). Thirty-four patients had 80 cases of post-ECT urinary retention, yielding an incidence of 7.4 (95% CI 4.8 to 11.5) urinary retention cases per 1,000 ECT treatments. Table 1 summarizes the clinical characteristics of patients who developed post-ECT urinary retention compared to those who did not. Only older age (odds ratio = 1.63 per 10 years [95% confidence interval 1.33, 2.00], P < 0.001) was associated with increased risk for urinary retention. There were 390 (3.7%) ECT cases where anticholinergic agents (387 glycopyrrolate, 6 atropine) were periprocedurally administered, and this was associated with increased risk for post-ECT urinary retention (odds ratio 6.22 [95% confidence interval 2.38, 16.29], P < 0.001).
Recently, several reports have found that the risk for urinary retention following general anesthesia varies greatly based on agents used to reverse nondepolarizing neuromuscular blockade. Decreased risk is reported with the use of sugammadex (which has no anticholinergic properties) compared to traditional reversal with neostigmine which requires obligatory use of an anticholinergic agent to prevent severe bradycardia or asystole. While the reported incidence of urinary retention following procedures performed under general anesthesia ranges between 5% and 70%, 2 the incidence of post-ECT urinary retention in the current study of ECT patients was less than 1%. This can be expected as ECT is a very short procedure with minimal exposure to anesthetic agents. However, we found an increased risk for post-ECT urinary retention in patients administered anticholinergic agents during ECT. Anticholinergic agents decrease bladder detrusor muscle tone, impeding micturition, 3 and their administration has been associated with increased risk for postoperative urinary retention. 4
In conclusion, even though urinary retention was less frequent following ECT than other procedures performed under general anesthesia, its risk increases with advancing age and administration of anticholinergic medications during the procedure. Anesthesia providers should inform the psychiatric team when these medications are used so they can alert care providers (inpatient psychiatric nurses and family members) to be vigilant for signs and symptoms of urinary retention, especially considering ECT patients may have postictal cognitive changes.
Clinical Characteristics of Patients Undergoing Electroconvulsive Therapy Who Developed Urinary Retention.
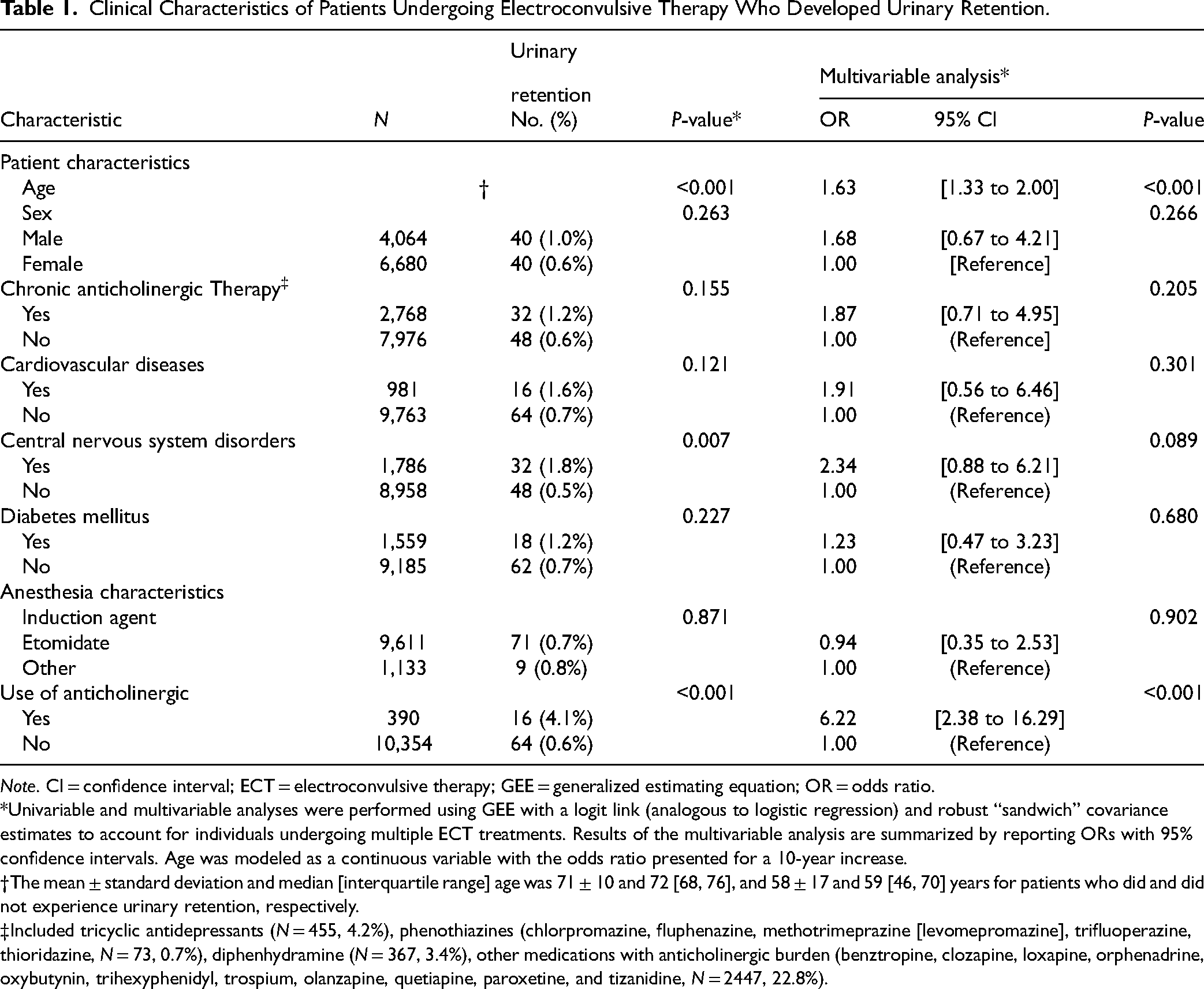
Note. CI = confidence interval; ECT = electroconvulsive therapy; GEE = generalized estimating equation; OR = odds ratio.
*Univariable and multivariable analyses were performed using GEE with a logit link (analogous to logistic regression) and robust “sandwich” covariance estimates to account for individuals undergoing multiple ECT treatments. Results of the multivariable analysis are summarized by reporting ORs with 95% confidence intervals. Age was modeled as a continuous variable with the odds ratio presented for a 10-year increase.
†The mean ± standard deviation and median [interquartile range] age was 71 ± 10 and 72 [68, 76], and 58 ± 17 and 59 [46, 70] years for patients who did and did not experience urinary retention, respectively.
‡Included tricyclic antidepressants (N = 455, 4.2%), phenothiazines (chlorpromazine, fluphenazine, methotrimeprazine [levomepromazine], trifluoperazine, thioridazine, N = 73, 0.7%), diphenhydramine (N = 367, 3.4%), other medications with anticholinergic burden (benztropine, clozapine, loxapine, orphenadrine, oxybutynin, trihexyphenidyl, trospium, olanzapine, quetiapine, paroxetine, and tizanidine, N = 2447, 22.8%).
Footnotes
Acknowledgements
We are grateful to Ms. Kimberly Hamilton (Anesthesia Clinical Research Unit Data Specialist) for her help with data extraction.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TNW received consulting fees from Medtronic and Merck. These are unrelated to this study. All other authors have no potential conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.