
Abstract
Background
Generalized anxiety disorder (GAD) is a prevalent anxiety disorder characterized by uncontrollable worry, trouble sleeping, muscle tension, and irritability. Cognitive behavioural therapy (CBT) is one of the first-line treatments that has demonstrated high efficacy in reducing symptoms of anxiety. Electronically delivered CBT (e-CBT) has been a promising adaptation of in-person treatment, showing comparable efficacy with increased accessibility and scalability. Finding further scalable interventions that can offer benefits to patients requiring less intensive interventions can allow for better resource allocation. Some studies have indicated that weekly check-ins can also lead to improvements in GAD symptoms. However, there is a lack of research exploring the potential benefits of online check-ins for patients with GAD.
Objective
This study aims to investigate the effects of weekly online asynchronous check-ins on patients diagnosed with GAD and compare it with a group receiving e-CBT.
Methods
Participants (n e-CBT = 45; n check-in = 51) with GAD were randomized into either an e-CBT or a mental health check-in program for 12 weeks. Participants in the e-CBT program completed pre-designed modules and homework assignments through a secure online delivery platform where they received personalized feedback from a trained care provider. Participants in the mental health check-in condition had weekly asynchronous messaging communication with a care provider where they were asked structured questions with a different weekly theme to encourage conversation.
Results
Both treatments demonstrated statistically significant reductions in GAD—7-item questionnaire (GAD-7) scores over time, but when comparing the groups there was no significant difference between the treatments. The number of participants who dropped out and baseline scores on all questionnaires were comparable for both groups.
Conclusions
The findings support the effectiveness of e-CBT and mental health check-ins for the treatment of GAD.
Plain Language Summary Title
Comparing the Effectiveness of Electronically Delivered Therapy (e-CBT) to Weekly Online Mental Health Check-ins for Generalized Anxiety Disorder—A Randomized Controlled Trial
Plain Language Summary
Generalized anxiety disorder (GAD) is a prevalent psychiatric condition that leads to symptoms like uncontrollable worry, trouble sleeping, muscle tension, and irritability. Cognitive behavioural therapy (CBT) is a common psychotherapy used for GAD since it has been shown to reduce symptoms. However, traditional CBT that is in person can have barriers such as being inaccessible and costly, and therefore electronically delivered CBT (e-CBT) is a viable alternative since previous studies have shown its efficacy in reducing symptoms and being similar compared to face-to-face CBT. Previous studies have also shown reductions in GAD symptomology through the use of checking in on people and their mental health. Therefore, this study aimed to compare e-CBT to a check-in condition and had a total of 45 individuals in e-CBT and 51 participants in the check-in condition. Participants in the e-CBT condition completed 12 weeks of predesigned e-CBT modules, homework and received personalized feedback from a care provider. In contrast, individuals in the check-in condition completed 12 weeks of unstructured asynchronous messaging with a care provider. Results from the study showed that both the e-CBT and check-in condition demonstrated statistically significant improvements in GAD-7 across time, but when comparing the groups there was no significant difference. The results show the efficacy of e-CBT and checking in on people's mental health to reduce GAD and future research should examine the 2 conditions combined.
This visual abstract was created by Michael Wong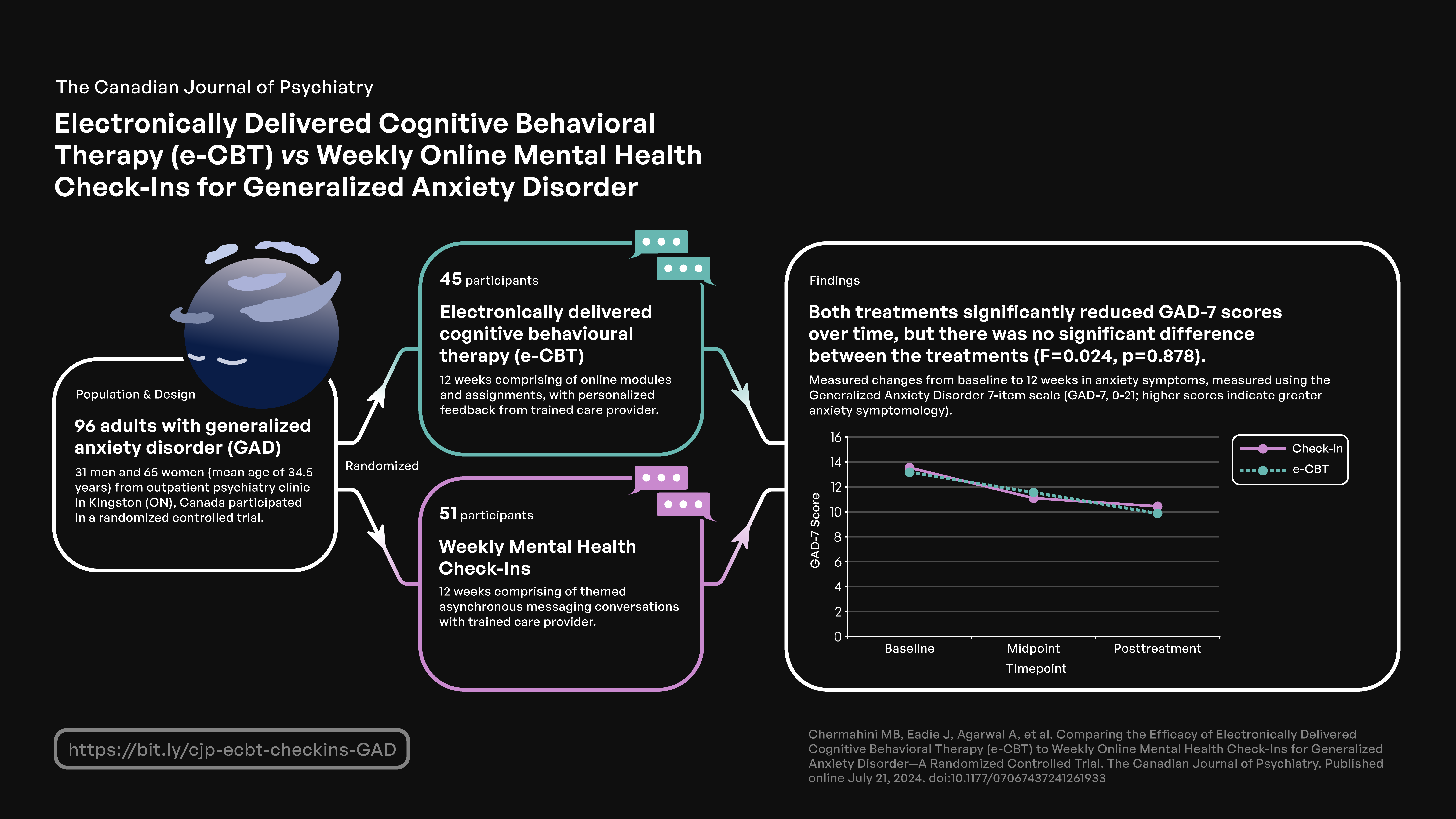
Introduction
Over 450 million people live with generalized anxiety disorder (GAD), characterized by symptoms including uncontrollable worry most days, trouble sleeping, muscle tension, poor concentration, and irritability.1–4 Individuals with GAD can experience challenges in aspects of life including, social relationships, work, and school. 5 Furthermore, GAD has a high comorbidity with depression, alcohol use disorder, and other anxiety disorders, making finding effective treatment options essential to reduce the prevalence of the other disorders.6,7
Cognitive behavioural therapy (CBT) is one of the first-line interventions for GAD, demonstrating high efficacy in symptom reduction compared to treatment as usual, waitlist controls, and other forms of psychotherapy at 6-month follow-ups. 8 CBT targets thought patterns and behavior, allowing one to become more aware of their maladaptive thoughts which can aid in behavior change. 9 CBT can effectively reduce symptoms of worry with comparable efficacy to pharmaceutical interventions. 10 However, traditional face-to-face CBT poses accessibility barriers including long waitlists to see practitioners, high costs, and the stigma that can surround seeking in-person help.11–14
To address these barriers, electronically delivered CBT (e-CBT) is a promising solution and has been shown to improve symptoms of anxiety, depression, and sleep quality.15–19 e-CBT is also effective in treating GAD for a multitude of populations including older adults and postsecondary students.20–22 Moreso, e-CBT can provide comparable efficacy to its in-person counterpart. 23 Given the widespread nature of electronic devices, e-CBT presents a unique opportunity to expand access to provide effective care. In a systematic review, smartphone app-based e-CBT significantly reduced anxiety symptoms but treatment effects were not as great compared to in-person CBT.17,24 Furthermore, e-CBT has been found to reduce social and recreational risk avoidance in people with GAD. 25 However, one study showed that e-CBT was ineffective as a preventive method for reducing anxiety symptoms, but was still effective in improving secondary outcomes such as anxiety sensitivity. 26 Additionally, e-CBT is more cost-effective than in-person and hybrid models. 27 Therefore, finding a balance between cost-effectiveness and high-efficacy treatments is essential for proper resource allocation.
Checking in on people's mental health is a low-resource-intensive way to provide care and support, which can have positive effects on mental health. 28 However, checking in on an individual's mental health with specific weekly topics through messaging has minimal research evidence supporting its efficacy. A study from New Zealand found that text messages directed at participants with depression and anxiety were a good alternative to face-to-face therapy, improving symptoms while also offering accessibility benefits and reducing fear of face-to-face interactions. 29 Furthermore, text messaging services have become a popular way for therapists to communicate with their clients since they are accessible and convenient for different populations. 30 However, text messaging check-in limitations include the inability to teach thoroughly constructed CBT. Therefore, using a more structured digital platform for mental health check-ins could address this limitation.31,32 More research on the effectiveness of online structured check-ins is needed.
Objectives
This study investigated the efficacy of e-CBT compared to asynchronous online mental health check-ins for treating GAD. Based on evidence supporting the effectiveness of e-CBT, it was hypothesized that asynchronous online check-ins through weekly prompts would be effective at improving generalized anxiety disorder—7-item questionnaire (GAD-7) symptoms, but e-CBT would be superior.
Methods
Design
In this randomized trial, participants were randomly assigned through a randomization code in Excel, to either a 12-week e-CBT program or a mental health check-in program that used asynchronous online check-ins. After completing the check-in program, participants were given the option to voluntarily engage in the e-CBT program. Similarly, those who finished the e-CBT program could choose to participate in the check-in program. However, if participants decided to engage in the alternate afterwards, their data from the second program was not used for analysis. This study was registered through the ClinicalTrials.gov system (NCT04754438).
Sample Size and Recruitment
Participants (total: n = 96; e-CBT: n = 45; check-in: n = 51) were recruited in Kingston, Ontario, Canada from outpatient psychiatry clinics at Kingston Health Sciences Centre, referrals from primary care physicians, specialists, clinicians, and self-referrals. Data from prior research that used this e-CBT program demonstrated that a sample of 50 participants in each group was sufficient for an effect size of 0.5, an α of .05, and a power of 0.8. 33 Although 120 participants were recruited, only 96 started either the e-CBT or check-in condition.
Eligibility
Inclusion criteria included being 18 years and older, a GAD diagnosis confirmed through a video call with a psychiatrist using the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, 34 competence to consent to participate, consistent and reliable internet, and the ability to communicate and read English. Exclusion criteria included active psychosis, acute mania, suicidal/homicidal ideation, and severe alcohol/substance use disorder. Participants were also excluded if they received another psychotherapy program or received CBT in the past year to avoid confounding factors. Informed consent included disclosing the potential harms of the study and informing clients of their right to stop at any time. Once informed consent was obtained from all eligible participants, they were included in the study and randomly assigned to treatment groups by the lab manager.
Interventions
e-CBT: Participants in the e-CBT arm were offered 12 weekly previously validated modules that focused on developing constructive and balanced coping strategies, behaviour modification, cognitive restructuring, relaxation strategies, and symptom management, which have all been shown to help reduce GAD.16,19,35 As seen in Table 1, the e-CBT modules also helped connect one's thoughts to emotions, physiological reactions, situations, and behaviours to become better engaged in day-to-day activities and learn to deal with negative situations or thoughts more productively. The weekly set of modules consisted of ∼30 slides that were delivered through the Online Psychotherapy Tool (OPTT), a secure, cloud-based, digital mental health platform (www.optt.health). Once participants finished their weekly module, they completed homework and submitted it to their care provider for personalized feedback. For each session of e-CBT, it takes ∼30 to 45 min to read the information and complete the homework, depending on the amount of effort that the client puts into their work. Each session was considered completed when the client finished and submitted their homework questions.
Twelve-Week e-CBT Program Content and the Check-in Program Question Prompts.
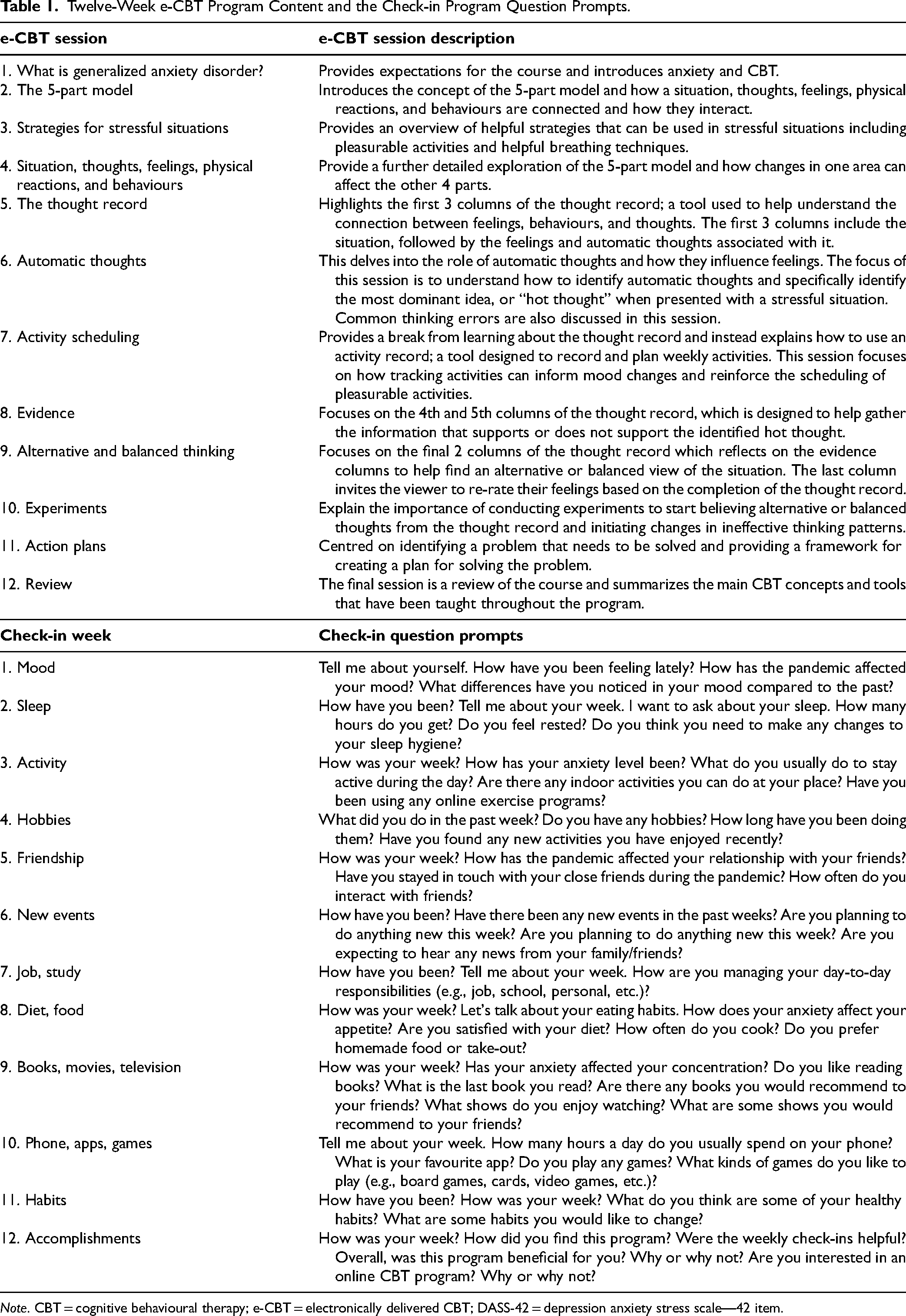
Note. CBT = cognitive behavioural therapy; e-CBT = electronically delivered CBT; DASS-42 = depression anxiety stress scale—42 item.
Check-In: Participants in the check-in arm had weekly check-ins with their care provider for 12 weeks through the asynchronous messaging system on OPTT. Care providers wrote to the participants weekly using structured pre-designed templates with questions (Table 1) and participants would communicate back to them. These questions were structured to encourage responses and therefore required the use of probing and critical thinking to help the clients better connect their feelings and experiences to the specific questions. Asking probing questions is a common therapy technique and has been shown to help individuals provide more details about the situation, feelings, and needs. 36 Although care providers checked in on the participants and provided support, no psychotherapy strategies were taught. Therefore, it would take clients a few minutes to complete the check-in condition each week, but would depend on how much detail they wanted to use in order to answer the question. Each week, the check-in condition was considered completed when a client responded to the prompts that they were sent.
Care Providers
The care providers in this study were research assistants who were medical doctors, with certifications in psychotherapy and also had training (mandatory CBT workshops) from the principal investigator (PI), who is an expert in the delivery of psychotherapy and online psychotherapy. They received training in e-CBT and learned how to provide feedback before interacting with participants. Their training included examining feedback scripts with practice participants and completing feedback that was reviewed by the PI. The PI or the other senior psychotherapist on the team (expert on online CBT) reviewed all weekly feedback before being submitted to participants. Care providers were given templates to write their feedback and personalized it based on participants’ homework submissions. The goal was to increase scalability similar to previous work showing that feedback tools can decrease the duration of writing feedback per participant, without sacrificing the quality of care. 35
Outcomes and Analysis
Participants completed reliable and clinically validated questionnaires at baseline, midpoint (week 6), and posttreatment (week 12). Participants completed the GAD-7, quality of life enjoyment and satisfaction questionnaire—short form (Q-LES-Q-SF), depression anxiety stress scale—42 item (DASS-42), and a demographic questionnaire.37–40 The GAD-7 was the primary outcome measure in order to examine changes in anxiety symptomatology. Secondary outcomes included Q-LES-Q-SF which assesses changes in quality of life and the DASS-42 which examines changes in depression, anxiety, and stress which are reported as such throughout.37–40
Before analysis, data were examined for missing, nonsensical, and outlying variables. Missing data were not imputed and was analysed on a per-protocol basis. The statistical significance level was 0.05, except in cases where a Bonferroni correction was used. Demographic information of program completers and dropouts was compared, and any possible differences were identified using independent samples t-tests. The primary analysis was intention-to-treat (ITT) conducted to determine the effect of treatment type on primary and secondary outcomes for all participants. A linear mixed-effects model was the main analysis used, with random effects as patient identification and fixed effects as treatment, time, and their interaction. This analysis involved all participants, including those who did not complete all sessions. Additionally, a 2 × 3 (treatment group × time) repeated measures analysis of variance (ANOVA) was performed on the primary and secondary outcomes. This analysis investigated changes in outcomes among individuals who completed all sessions of the treatments. The analyses were all done through IBM SPSS Statistics for Mac, Version 24 (IBM Corp., Armonk, NY, USA).
Results
Participants
Recruitment occurred from May 2021 to August 2023 with a satisfactory sample size (Figure 1). Participants who began the interventions were included in the analysis and nonstarters were excluded, yielding 45 participants for e-CBT and a sample of 51 in the check-in condition. Across the e-CBT and check-in group, participants were an average of 34.5 (standard error (SE) = 1.36) years old, predominantly female (n = 65; 67.71%), and completed an average of 9.25 sessions (SE = 0.54). More specifically, participants in the e-CBT group completed an average of 8.68 (SE = 1.88) sessions compared to the check-in group who completed 9.85 (SE = 0.53) on average. In total 24 (53.33%) participants completed e-CBT and 28 (54.90%) completed check-in.
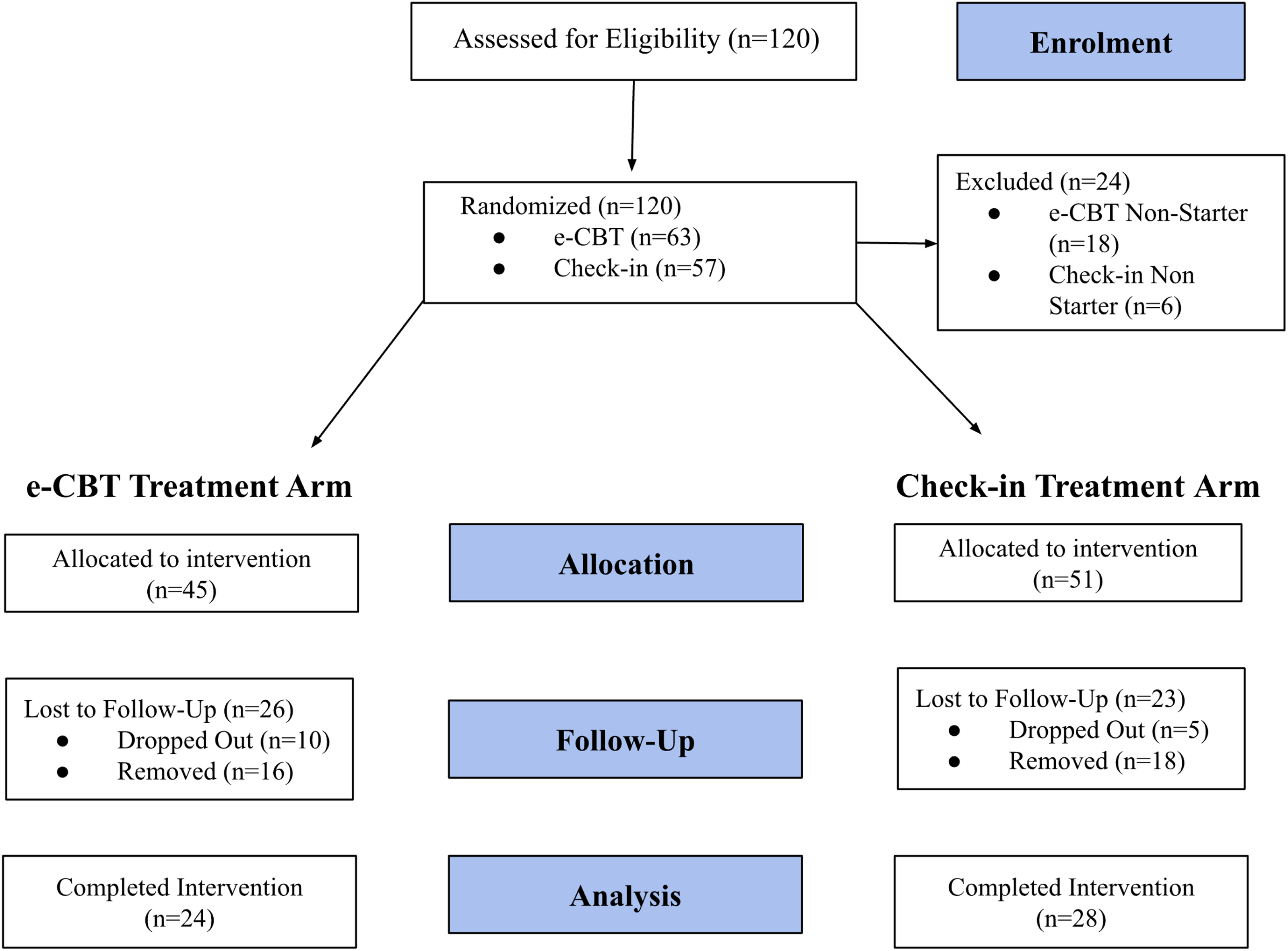
Participant recruitment and enrolment flowchart.
Treatment Comparison: ITT Analysis
There was no difference in GAD-7 scores at baseline between the groups (e-CBT = 13.18, SE = 0.66; check-in = 13.55; SE = 0.59; p = 0.68). Q-LES-Q-SF scores were also similar (e-CBT = 40.38, SE = 1.48; check-in = 38.53; SE = 1.11; p = 0.32), and there was no significant difference in baseline depression (e-CBT = 18.80, SE = 1.82; check-in = 18.40, SE = 1.44; p = 0.89), anxiety (e-CBT = 16.50, SE = 1.35; check-in = 14.82, SE = 1.16; p = 0.35), or stress (e-CBT = 23.22, SE = 1.27; check-in = 21.80, SE = 1.11; p = 0.40) scores.
To compare the effect of treatment types on primary and secondary outcomes, an unstructured mixed-effect model was conducted (arm and time point as fixed factors), including participants who did not complete all treatment sessions (ITT analysis).
The GAD-7 scores for both e-CBT and check-in treatment groups significantly changed over time (F = 13.92, p < 0.001). The GAD-7 mean score (observed mean) for the e-CBT group decreased from 13.18 (baseline) to 11.56 (midpoint) to 9.875 (posttreatment), while the check-in scores decreased from 13.55 (baseline) to 11.1 (midpoint) to 10.44 (posttreatment). There was no significant difference between the treatment groups for GAD-7 scores (F = 0.024, p = 0.878). Moreover, the effect size representing the interaction of treatment and time was not significant (F = 1.368, p = 0.262; Table 2 and Figure 2a).
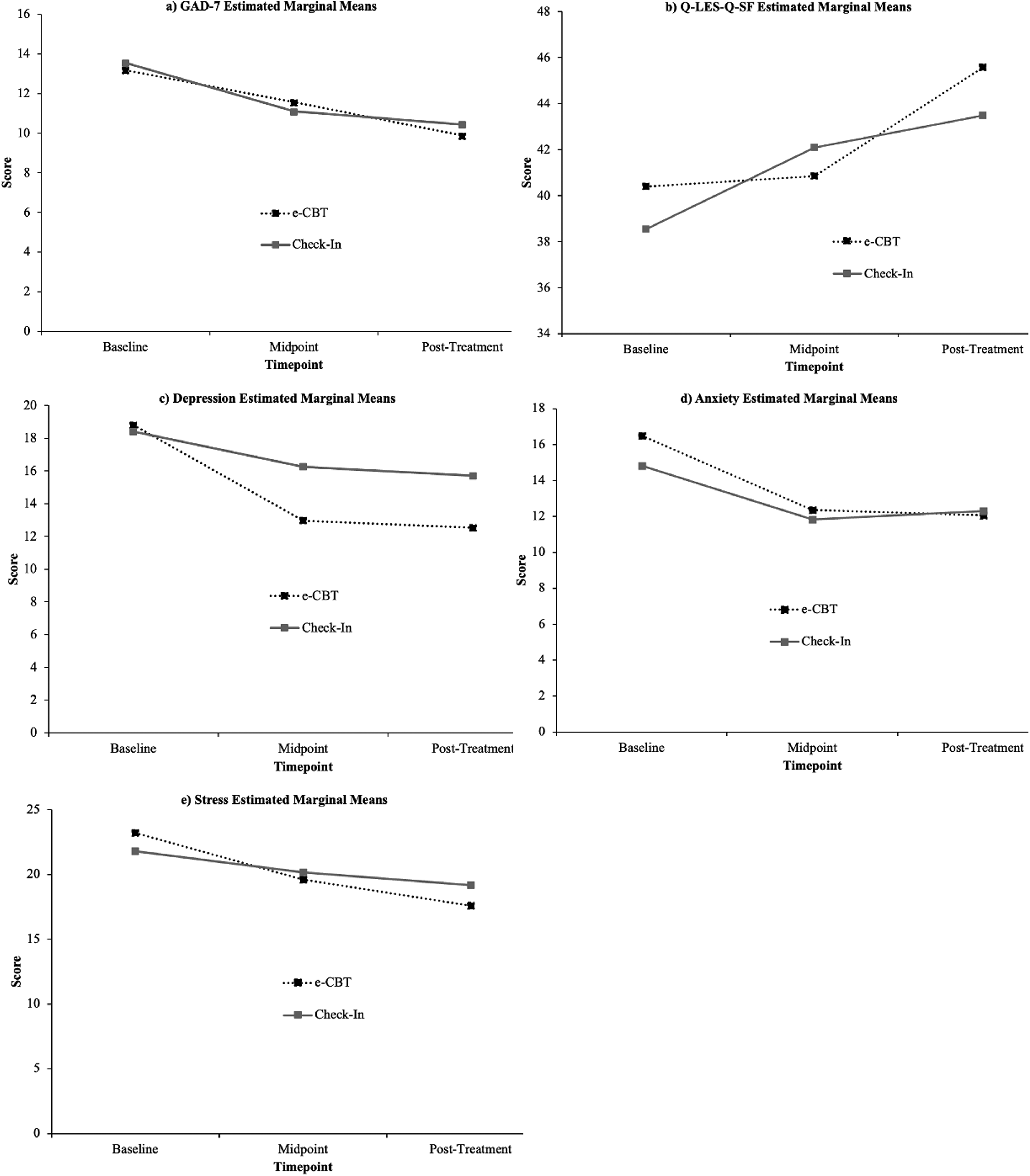
(a) GAD-7 scores at 3 points of treatment, initial (week 0), mid (week 6), and final (week 12), for e-CBT and check-in. (b) Q-LES-Q-SF scores at 3 points of treatment, initial (week 0), mid (week 6), and final (week 12), for e-CBT and check-in. (c) Depression (DASS-42) scores at 3 points of treatment, initial (week 0), mid (week 6), and final (week 12) in e-CBT and check-in. (d) Anxiety (DASS-42) scores at 3 points of treatment, initial (week 0), mid (week 6), and final (week 12), for e-CBT and check-in. (e) Stress (DASS-42) scores at 3 points of treatment, initial (week 0), mid (week 6), and final (week 12), in e-CBT and the check-in condition.
Observed Means, SEs, and Linear Mixed Model Analysis of Primary and Secondary Outcomes as a Function 2 × 3 Design (Treatment Group × Time).
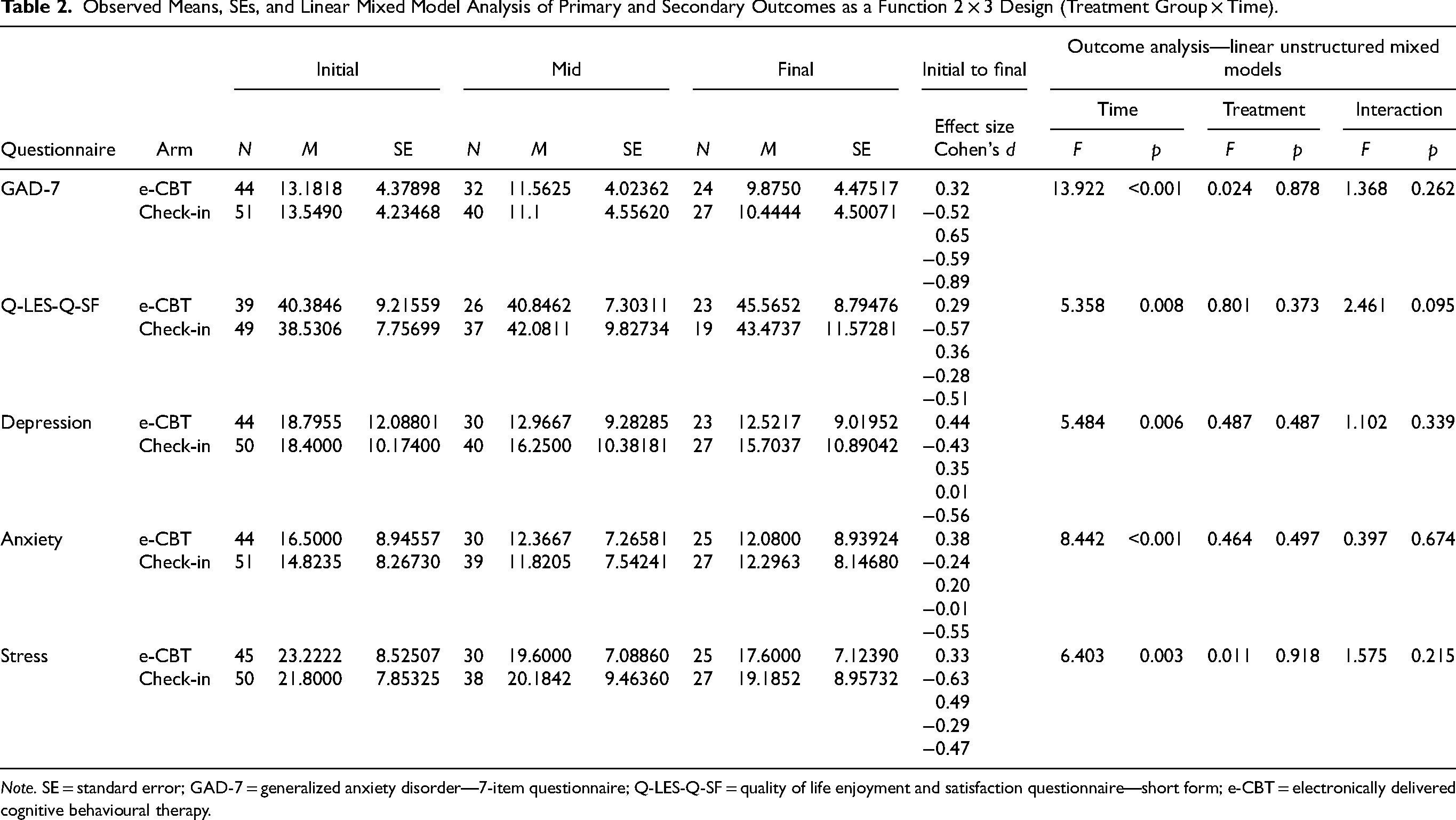
Note. SE = standard error; GAD-7 = generalized anxiety disorder—7-item questionnaire; Q-LES-Q-SF = quality of life enjoyment and satisfaction questionnaire—short form; e-CBT = electronically delivered cognitive behavioural therapy.
The Q-LES-Q-SF mean score (observed mean) significantly improved from 40.38 to 40.85 to 45.56 (baseline, midpoint, and posttreatment) in the e-CBT group and from 38.53 to 42.08 to 43.47 in the check-in group (F = 5.358, p = 0.008). There was no significant difference between the treatment groups for the Q-LES-Q-SF score (F = 0.801, p = 0.373). The effect size for the interaction between treatment and time effects was also not significant (F = 2.461, p = 0.095; Table 2 and Figure 2b).
The scores for the depression section of the DASS-42 showed significant changes over time for both the e-CBT and check-in treatment groups (F = 5.484, p = 0.006). The mean score (observed score) from the depression section of the DASS-42, for the e-CBT group decreased from 18.80 (baseline) to 13.00 (midpoint) to 12.52 (posttreatment), while the check-in scores decreased from 18.40 (baseline) to 16.25 (midpoint) to 15.70 (posttreatment). There was no significant difference between the treatment groups for depression (DASS-42) scores (F = 0.487, p = 0.487). Moreover, the effect size representing the interaction of treatment and time effects was not significant (F = 1.102, p = 0.339; Table 2 and Figure 2c).
The anxiety (DASS-42) scores for both e-CBT and check-in treatment groups significantly decreased over time (F = 8.442, p < 0.001). The anxiety (DASS-42) mean score (observed mean) for the e-CBT group decreased from 16.50 (baseline) to 12.40 (midpoint) to 12.10 (posttreatment), while the check-in scores changed from 14.82 (baseline) to 11.82 (midpoint) to 12.30 (posttreatment). There was no significant difference between the treatment groups for anxiety (DASS-42) scores (F = 0.464, p = 0.497). Moreover, the effect size representing the interaction of treatment and time effects was not significant (F = 0.397, p = 0.674; Table 2 and Figure 2d).
The stress (DASS-42) scores for both e-CBT and check-in treatment groups significantly decreased over time (F = 6.403, p = 0.003). The stress (DASS-42) mean score (observed mean) for the e-CBT group decreased from 23.22 (baseline) to 19.60 (midpoint) to 17.60 (posttreatment), while the check-in scores decreased from 21.80 (baseline) to 20.18 (midpoint) to 19.18. There was no significant difference between the treatment groups for stress (DASS-42) scores (F = 0.011, p = 0.918). Moreover, the effect size representing the interaction of treatment and time effects was not significant (F = 1.575, p = 0.215; Table 2 and Figure 2e).
Treatment Comparison-Completer Sample
A repeated measures ANOVA was performed on the primary and secondary outcomes to analyse changes in scores among treatment completers. The analysis showed no significant difference between e-CBT and check-in scores for GAD-7 (F = 0.070, p = 0.793), depression (F = 1.289, p = 0.262), Q-LES-Q-SF (F = 0.328, p = 0.571), anxiety (F = 0.038, p = 0.847) and stress (F = 0.012, p = 0.912). Additionally, a significant change in scores over time was observed for all outcomes GAD-7 (F = 16.41, p < 0.001), anxiety (F = 4.120, p = 0.048), stress (F = 5.806, p = 0.020), and Q-LES-Q-SF (F = 9.734, p = 0.004), except depression (F = 4.120, p = 0.212). The interaction term for the effect of time and treatment type was not significant for any of the outcomes including GAD-7 (F = 0.259, p = 0.613), depression (F = 0.408, p = 0.526), anxiety (F = 0.437, p = 0.512), stress (F = 2.577, p = 0.115), and Q-LES-Q-SF (F = 0.790, p = 0.380; Table 3).
Observed Means, SEs, and Repeated Measures ANOVA of Primary and Secondary Outcomes as a Function of 2 × 3 Design (Treatment Group × Time).
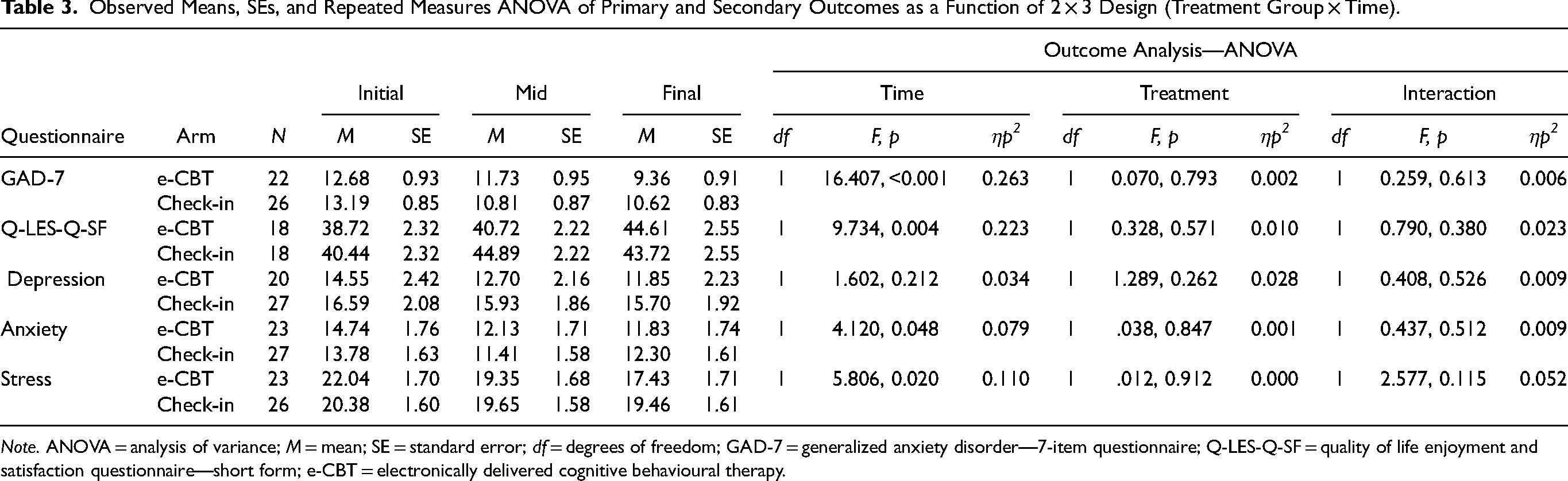
Note. ANOVA = analysis of variance; M = mean; SE = standard error; df = degrees of freedom; GAD-7 = generalized anxiety disorder—7-item questionnaire; Q-LES-Q-SF = quality of life enjoyment and satisfaction questionnaire—short form; e-CBT = electronically delivered cognitive behavioural therapy.
There was no significant difference in patient compliance across groups. A chi-square test indicated that the number of patients who completed all 12 sessions was comparable across the 2 groups (e-CBT = 53.33%; check-in = 54.90%; p = 0.459). An independent sample t-test demonstrated that among dropouts, there was no significant difference regarding the number of sessions completed across both treatment groups (p = 0.658). On average, drop-outs completed 6.66 (SE = 0.675) sessions in the e-CBT arm and 7.09 (SE = 0.702) sessions in the check-in arm.
Discussion
This study compared a 12-week e-CBT program to an online mental health check-in program for GAD. All baseline scores were comparable among the e-CBT and check-in conditions. Both the e-CBT and Check-in condition experienced improved symptoms from baseline to the end of treatment and no harm occurred. Results from the linear mixed model demonstrated a statistically significant improvement in primary and secondary outcomes over time. Furthermore, the repeated measures ANOVA showed that both the e-CBT and check-in condition resulted in statistically significant improvements in all outcomes over time except depression, which was not statistically significant.
In line with previous research, the results of this study suggest that e-CBT is an effective treatment for GAD.12–17 Additionally, this study's findings suggest that weekly asynchronous check-ins can also help to reduce symptoms of GAD. This improvement could be due to the therapeutic relationship established through online communication with a healthcare provider. Additionally, these improvements highlight the value of the supportive aspect of therapy in the treatment of GAD. These findings could inform mental health care systems to better allocate resources and improve accessibility of care. For example, patients on the waitlist, or those who need less intense follow-up after their symptoms are more stabilized, could benefit from e-CBT and check-ins.
Research on the effectiveness of check-ins in helping to reduce GAD is limited. Therefore, this study is original since it compares e-CBT with mental health check-ins in treating GAD and provides evidence of the effectiveness of check-ins for patients who require less direct support.
One of the limitations of this study is that the dropout rates were relatively high, potentially introducing bias and impacting our findings. For instance, it is possible that those who completed the study could have had different characteristics compared to those who dropped out and are not an accurate representation of the general patient population. Thus, the improvement in symptomatology may be influenced by other factors not investigated in the study. The dropout rate is comparable to studies that explored the effectiveness of e-CBT. 35 Studies investigating the dropout rate for CBT to treat anxiety disorders and other mental health conditions reported a lower rate, ranging from 16% to 26%.41,42 It is crucial to further investigate the dropout rate of e-CBT and factors that can contribute to patients not completing treatment. Furthermore, previous studies investigating clinically meaningful change in GAD-7 scores have found a change ranging from 4 to 7 points to be clinically significant.43,44 Among the participants, the mean GAD-7 score decreased from the initial session to the final session for the e-CBT group (3.3) and check-in group (3.11; Table 2). Although the observed improvements were statistically significant (Table 2), they may not be clinically meaningful, which future research could investigate. In addition, this study did not have a long-term follow-up evaluation which should also be explored in future research.
In conclusion, this study compared e-CBT and an online mental health check-in program, and they both demonstrated efficacy in improving all of the primary and secondary symptoms across time when looking at the intention to treat analysis. This means that when e-CBT is not available, check-in messaging could be an alternative. Further investigation should be done to understand the effectiveness of these treatments for varying GAD severity, and their impact when used in conjunction, and longer follow-ups should be applied to examine long-term impacts.
Supplemental Material
sj-doc-1-cpa-10.1177_07067437241261933 - Supplemental material for Comparing the Efficacy of Electronically Delivered Cognitive Behavioral Therapy (e-CBT) to Weekly Online Mental Health Check-Ins for Generalized Anxiety Disorder—A Randomized Controlled Trial: Comparaison de l'efficacité de la thérapie cognitivo-comportementale délivrée par voie électronique (e-TCC) aux contrôles hebdomadaires en ligne de santé mentale pour le trouble d'anxiété généralisée - un essai randomisé contrôlé
Supplemental material, sj-doc-1-cpa-10.1177_07067437241261933 for Comparing the Efficacy of Electronically Delivered Cognitive Behavioral Therapy (e-CBT) to Weekly Online Mental Health Check-Ins for Generalized Anxiety Disorder—A Randomized Controlled Trial: Comparaison de l'efficacité de la thérapie cognitivo-comportementale délivrée par voie électronique (e-TCC) aux contrôles hebdomadaires en ligne de santé mentale pour le trouble d'anxiété généralisée - un essai randomisé contrôlé by Melinaz Barati Chermahini, Jazmin Eadie, Anika Agarwal, Callum Stephenson, Niloufar Malakouti, Niloofar Nikjoo, Jasleen Jagayat, Vineeth Jarabana, Amirhossein Shirazi, Anchan Kumar, Tessa Gizzarelli, Gilmar Gutierrez, Ferwa Khan, Charmy Patel, Megan Yang, Mohsen Omrani and Nazanin Alavi in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NA and MO co-founded OPTT and NA, MO, and AS have ownership stakes in OPTT Inc.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.