
Abstract
Objectives
Posttraumatic stress disorder (PTSD) and cannabis use disorder (CUD) commonly co-occur. Conditioned associations between psychological trauma cues, distress, cannabis use, and desired relief outcomes may contribute to the comorbidity. These conditioned associations can be studied experimentally by manipulating trauma cue exposure in a cue-reactivity paradigm (CRP) and examining effects on affective and cognitive outcomes in participants with and without PTSD. However, traditional CRPs take place in-lab limiting recruitment/power. We aimed to examine the effects of CRP condition (trauma and neutral) and PTSD group (likely PTSD+ and PTSD−) on affective and craving outcomes using a stand-alone online expressive writing CRP.
Methods
Participants (n = 202; 43.6% male; Mage = 42.94 years, SD = 14.71) with psychological trauma histories and past-month cannabis use completed a measure of PTSD symptoms (PTSD Checklist-5 for DSM-5 [PCL-5]) and were randomized to complete either a trauma or neutral expressive writing task. Then they completed validated measures of affect (Positive and Negative Affect Schedule-Short Form [PANAS-SF]) and cannabis craving (Marijuana Craving Questionnaire-Short Form [MCQ-SF]).
Results
Linear mixed models tested the hypothesized main and interactive effects of CRP condition (trauma and neutral) and PTSD group (likely PTSD+ and PTSD−) on negative and positive affect (PANAS-SF) and cannabis craving dimensions (MCQ-SF). The hypothesized main effects of trauma versus neutral expressive writing were found for negative affect and the expectancy dimension of cannabis craving and of PTSD group for negative affect and all cannabis craving dimensions; no interactions were observed.
Conclusions
Expressive writing appears a useful online CRP. Interventions focused on reducing negative affect and expectancy craving to trauma cues may prevent/treat CUD among cannabis users with PTSD.
Plain Language Summary Title
The Use of an Online Expressive Writing as a Trauma Cue Exposure: Effects on Craving and Emotions
Plain Language Summary
People who have gone through trauma sometimes experience both post-traumatic stress disorder (PTSD) and a tendency to use cannabis excessively (cannabis use disorder or CUD). Researchers believe that there's a connection between traumatic memories, emotional distress, cannabis use, and the relief people feel afterward. These associations can be studied experimentally by using a cue-reactivity paradigm (CRP) to examine effects on craving and affective outcomes in those with and without PTSD. This study included 202 participants who had a history of trauma and reported regular cannabis use. They were randomly assigned to write about a traumatic or neutral personal experience. After, they filled out questionnaires about their PTSD symptoms, emotions (both positive and negative), and cravings for cannabis during the task. We expected that the type of writing task (those assigned to the trauma vs. neutral condition) and PTSD status would be associated with increased cannabis craving, negative emotions, and reduced positive emotions. We found that writing about trauma increased negative feelings and positive expectations about using cannabis for relief, especially for those with PTSD. People with PTSD also seemed to have more ongoing negative feelings and cravings for cannabis. The authors suggest that traditional in-lab experiments might be necessary to fully understand how trauma reminders can influence cravings and emotions in individuals with PTSD-CUD.
Introduction
Posttraumatic stress disorder (PTSD) involves distressing symptoms (e.g., physiological reactivity to and avoidance of trauma reminders) following exposure to a traumatic event. 1 There is a high comorbidity between PTSD and substance use disorder (SUD). 2 PTSD–SUD is clinically significant given its more severe symptoms, poorer treatment response, and higher relapse rates compared to either disorder alone.2–5 This comorbidity extends to cannabis use disorder (CUD)6,7: individuals with CUD are 4 times more likely to have PTSD than those without CUD. 8 Moreover, longitudinal research suggests that continued cannabis use is associated with worse PTSD outcomes. 9 With few randomized controlled trials conducted, 10 some caution against the use of cannabis as a means of addressing PTSD symptoms. 11 Mechanistic studies to understand PTSD-cannabis use/CUD links are vital to identify intervention targets.
One mechanism proposed to underlie comorbid PTSD–CUD is trauma cue-elicited substance craving arising through conditioning. Two-factor learning theory 12 posits stimuli paired with a traumatic experience can become conditioned cues, inducing negative affect (NA) upon future exposure. This conditioned NA may drive substance use for relief, negatively reinforcing the behaviour. Given the frequent pairing of trauma cues/reminders with substance use to cope, trauma cues come to elicit conditioned substance craving. Research shows that substance users with trauma histories exhibit higher NA, lower positive affect (PA), and increased substance craving when exposed to trauma cues compared to neutral cues. 13 These responses are theoretically stronger in individuals with PTSD diagnoses or more severe PTSD symptoms14,15 and research supports this.15–17
In the context of PTSD–SUD research, cue reactivity paradigms (CRPs) can be used in a laboratory setting to experimentally examine the effects of trauma (vs. neutral) cue exposure on substance-relevant responses, such as affective reactions and substance craving. The gold-standard protocol for CRP research in the PTSD–SUD comorbidity field 18 draws from a prominent theory of emotional imagery, 19 using a 2-session protocol. 20 The first session uses a semistructured interview 21 to have participants recall details of their most traumatic experience, which are later distilled into a brief personalized audiovisual cue used as the CRP in the second session. 15 An identical procedure is used for the neutral/control cue.
As avoidance of trauma reminders is a symptom of PTSD, 1 CRP research is fraught with high attrition between the interview and CRP session. 18 Our recent work suggests that the semistructured interview alone, requiring only a single lab visit, can serve as a valid CRP in eliciting relevant cannabis craving and NA responses. 14 A remaining issue is obtaining in-lab sample sizes large enough to detect theorized, smaller magnitude, interactions. 22 Online data collection can achieve a broader reach for recruitment, thereby permitting the necessary larger samples.
In this study, we used an online expressive writing task (trauma vs. neutral) based on Pennebaker's 23 work as a novel stand-alone CRP, allowing single-session administration and increased sample size. Previous studies have only used brief expressive writing in combination with audio CRPs to study co-occurring PTSD–SUD,16,24 but this necessitates lab-based administration. Our study is the first to use expressive writing alone as a CRP in eliciting theorized conditioned affective and craving responses to trauma cues that are potentially mechanistically involved in PTSD–CUD comorbidity. 13 We hypothesized those randomized to a trauma-expressive writing task would display greater reactivity across cannabis craving dimensions (H1), greater NA (H2), and lesser PA (H3), relative to those assigned to a neutral writing task. We also hypothesized that participants with likely PTSD a would display greater reactivity across cannabis craving dimensions (H4), greater NA (H5), and lesser PA (H6), relative to those without PTSD. Finally, we hypothesized cue condition × PTSD interactions for cannabis craving (H7), NA (H8), and PA (H9), with writing task effects stronger for those with (vs. without) likely PTSD.
Method
Participants
Participants were recruited via Qualtrics Panels, an online survey company which uses researcher-specified recruitment criteria. We advertised for cannabis users with a past traumatic experience(s). Eligibility criteria were: residing in Canada; 19 b –65 years old; lifetime exposure to ≥1 DSM-5 1 PTSD Criterion A potentially traumatic event(s) 25 ; and past month cannabis use (≥1 g). N = 6917 potential participants responded to our survey. N = 5973 of these did not meet one or more eligibility criteria; 520 did not follow the writing task instructions (e.g., 1 word written repeatedly; wrote about a stressful event that was not a Criterion A trauma); 98 were from duplicate internet protocol address; 77 did not respond appropriately to cannabis regimen measures to be used in another study; and 47 failed an attention check (e.g., “Select ‘4’ for this item”). After this stringent quality assurance check, there was a final sample of 202 participants (43.6% male; Mage = 42.94 years, SD = 14.71). Participants were compensated by Qualtrics at a rate based on factors such as survey length, panellist profile, and target acquisition difficulty.
Tasks and Measures
Demographics. Participants reported demographic information (i.e., sex and age).
Trauma Exposure. The Life Events Checklist (LEC) 25 assessed lifetime trauma c (DSM-5 PTSD criterion A). 1 If respondents had >1 lifetime trauma exposure, they were instructed to answer all further trauma-related questions/tasks with respect to their most traumatic event. d
PTSD. The 20-item PTSD Checklist for DSM-5 (PCL-5) 26 was used to categorize participants into 2 groups. Participants self-reported how bothered (0 = not at all to 4 = extremely) they were by each PTSD symptom (e.g., repeated and disturbing memories of the event) over the past month. The PCL-5 has good psychometric properties 27 ; in our sample, α = 0.95. Those scoring ≥38 were placed in the likely PTSD group, 28 and the rest in the no PTSD group. e , f
Cannabis Use. The Cannabis Timeline Followback (C-TLFB), 29 a method with excellent interrater reliability, 30 assessed past-month cannabis use to confirm study eligibility. Participants indicated on a past-month calendar the days they had used cannabis, and the amount used (in grams) on each day. Conversion rates were provided for concentrates and edibles (i.e., 1 g concentrate = 4 g flower; 1000 mg edible = 1 g flower). 31
CUD Symptom Severity. The 8-item CUD Identification Test-Revised (CUDIT-R) 32 measured CUD symptom severity. Participants indicated on a 0–4 scale (never to daily or almost daily) how often in the past 6 months they experienced various cannabis-related problems. Scores were summed. The CUDIT-R has good psychometric properties 32 ; internal consistency was adequate in our sample, α = 0.75.
Distress. The 9-item Patient Health Questionnaire (PHQ-9) 33 and 7-item Generalized Anxiety Disorder Scale 34 are validated33,34 measures of depressive and general anxiety symptom frequency, respectively. Items are rated on 0–3 scales (not at all to nearly every day). We used these measures to create a “distress” composite (i.e., the validated PHQ-Anxiety and Depression Scale [ADS]) 35 to use as a covariate in supplementary analyses to determine the specificity of findings to PTSD given the high co-occurrence of PTSD with depression and anxiety.36,37 The reliability of the PHQ-ADS in our sample was excellent (α = 0.95).
Expressive Writing. Participants were randomized to 1 of 2 expressive writing tasks 23 : trauma-related (i.e., worst lifetime trauma) or neutral (i.e., morning routine). First, the writing task instructed participants to describe what happened and to detail the bodily sensations, thoughts, and feelings that occurred during the event. 21 After reading these instructions, participants wrote for 2 min minimum with the instructions remaining for reference throughout the task. Participants were encouraged to take their time, and only allowed to proceed to the second screen after at least 2 min; there they were instructed to continue visualizing the event 16 just described for another 2 min. Task programming ensured these minima.
Craving. The reliable and valid 12-item Marijuana Craving Questionnaire-Short Form (MCQ-SF) 38 assessed 4 3-item cannabis craving dimensions: compulsivity (inability to control cannabis use; α = 0.76), emotionality (cannabis use in anticipation of relief from negative mood; α = 0.84), expectancy (anticipation of positive outcomes from cannabis use; α = 0.77), and purposefulness (intention to use cannabis; α = 0.89).
Affect. The psychometrically sound 39 20-item Positive and Negative Affect Schedule-Short Form (PANAS-SF) 40 assessed state PA (α = 0.86) and NA (α = 0.91). Participants indicated how much (1 = very slightly or not at all to 5 = extremely) they were feeling each of 10 positive (e.g., active and inspired) and 10 negative (e.g., distressed and nervous) affective states. Items for each type of affect were summed.
Procedure
Potential participants first provided informed consent and responded to questionnaires assessing eligibility (demographics; C-TLFB 29 and LEC 25 ). For eligible respondents, the survey began with the PCL-5, 26 CUDIT-R, 32 and baseline MCQ-SF 38 and PANAS-SF. 40 Next, participants were randomized to complete the assigned expressive writing task CRP (trauma [n = 96] and neutral [n = 106]). Prior to data cleaning, randomization was 1:1 across the 2 writing conditions; randomization was not stratified on any variables. Participants again completed the MCQ-SF 38 and the PANAS-SF, 40 this time for how they were feeling during the writing task.
Analyses
For our main analyses, we ran linear mixed models (Rv.4.2.1; lme4 package) with cue condition, PTSD group, and their interaction g predicting each cannabis craving dimension, NA, and PA. To determine which variables should be covaried in sensitivity analyses, we ran 2 × 2 linear mixed models with cue condition, PTSD group, and their interaction predicting theoretically relevant covariates (age, PHQ-ADS, CUDIT-R, writing task word count, and baseline craving and affect). h A 4 × 2 (group × sex) chi-square tested group differences in sex distribution. Sensitivity analyses involved rerunning our primary models with necessary covariates (each in a separate analysis).
Results
Sample Characteristics: Table 1 presents sample demographic and clinical characteristics by cue condition and PTSD group. The mean PCL-5 score was 31.51 (SD = 18.71) with 36% (n = 73) scoring ≥38 indicating likely PTSD. 28 The mean CUDIT-R 32 score of 11.37 (SD = 6.25; range = 0–32) was above the cutoff for hazardous use (≥8) and just below the cutoff for likely CUD (≥12). 32 In the past month, the average total grams of cannabis used by our sample was 37.33 (SD = 90.90) and the mean number of cannabis-using days was 14.03 (SD = 10.40).
Descriptive and Clinical Characteristics.
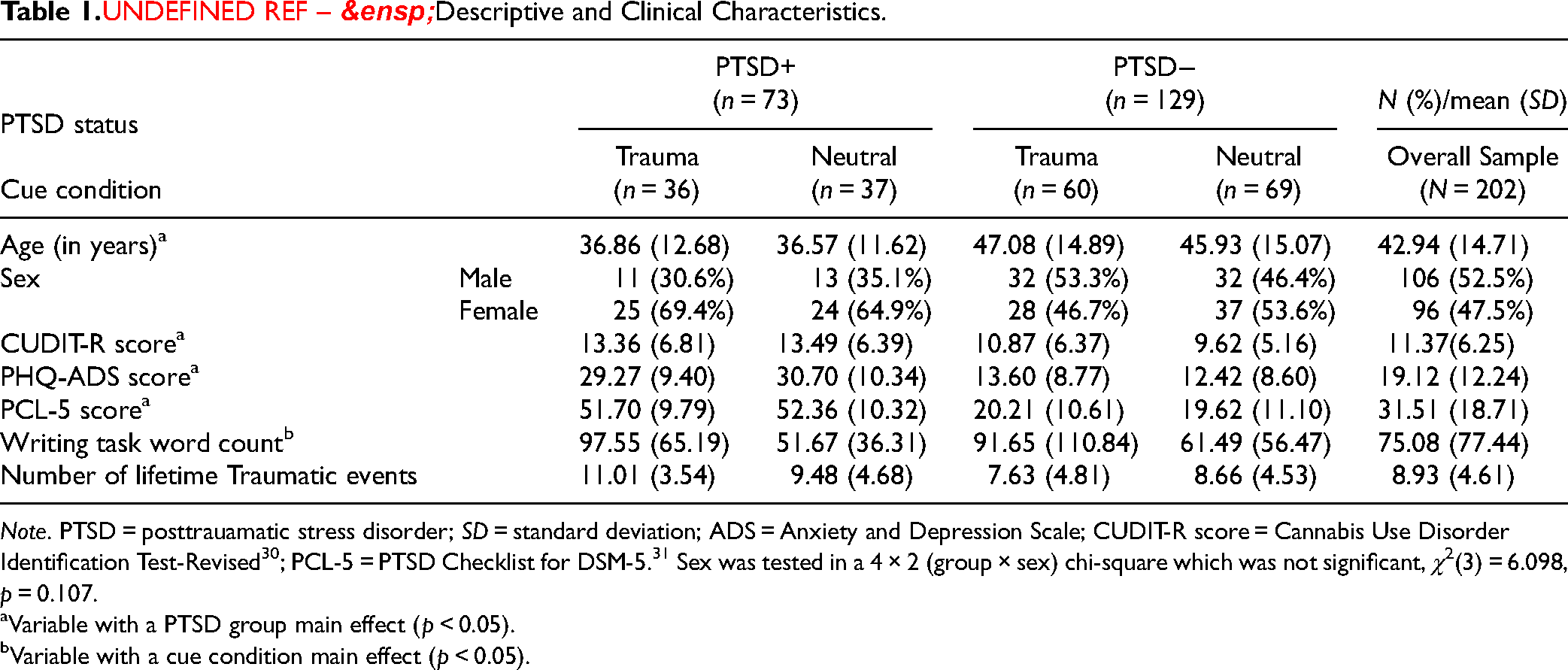
Note. PTSD = posttrauamatic stress disorder; SD = standard deviation; ADS = Anxiety and Depression Scale; CUDIT-R score = Cannabis Use Disorder Identification Test-Revised 30 ; PCL-5 = PTSD Checklist for DSM-5. 31 Sex was tested in a 4 × 2 (group × sex) chi-square which was not significant, χ2(3) = 6.098, p = 0.107.
Variable with a PTSD group main effect (p < 0.05).
Variable with a cue condition main effect (p < 0.05).
Craving. Partially consistent with H1, expectancy craving was higher in the trauma (M = 4.67, SD = 1.80) than neutral (M = 4.30, SD = 1.79) cue condition (t[198] = 2.13, 95% CI, 0.05 to 1.24, p = 0.035). However, the cue condition failed to predict the other 3 craving dimensions (Table 2). Consistent with H4, the expectancy (t[198] = 4.47, 95% CI, 0.87 to 2.24, p < 0.001), emotionality (t[198] = 4.31, 95% CI, 0.87 to 2.34, p < 0.001), compulsivity (t[198] = 4.19, 95% CI, 0.78 to 2.16, p < 0.001), and purposefulness craving dimensions (t[198] = 2.81, 95% CI, 0.34 to 1.96, p < 0.001), were higher in the likely PTSD versus no PTSD group (Figure 1 and Table 2). Contrary to H7, there were no cue condition × PTSD group interactions for any craving dimension (Table 2).
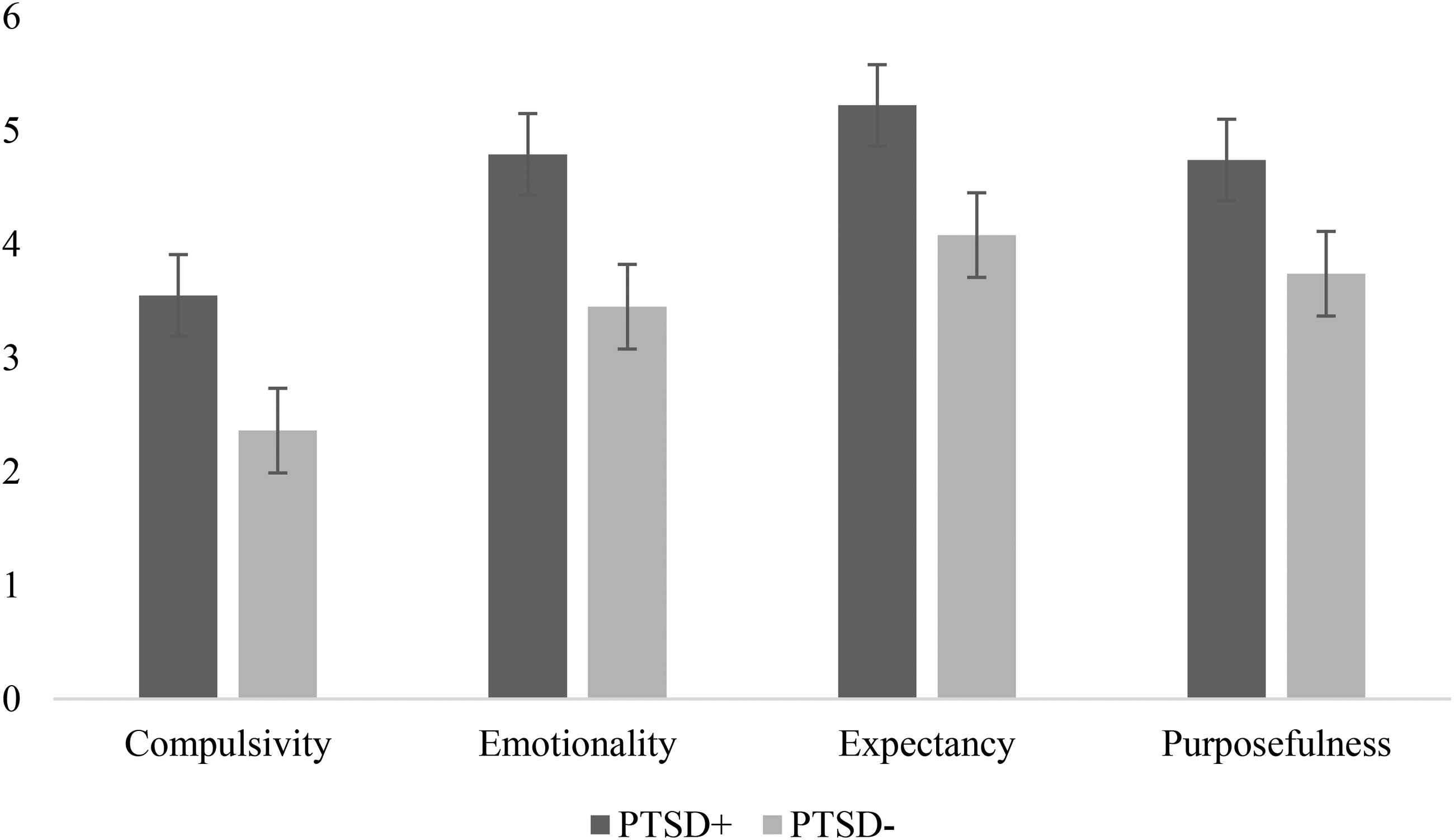
Mean cannabis craving subscale scores by posttraumatic stress disorder (PTSD) group.
Linear Mixed Models’ Omnibus Results for Craving Responses.
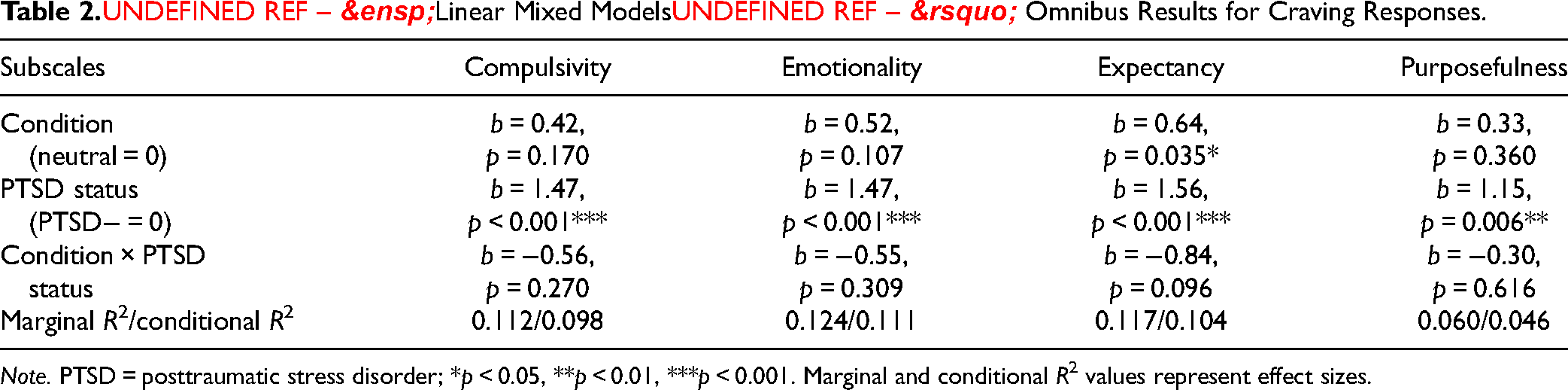
Note. PTSD = posttraumatic stress disorder; *p < 0.05, **p < 0.01, ***p < 0.001. Marginal and conditional R2 values represent effect sizes.
Affect. Consistent with H2 and H5, NA was greater in the trauma versus neutral cue condition (t[198] = 2.05, 95% CI, 0.11 to 5.73, p = 0.042) and among those with versus without likely PTSD (t[198] = 7.97, 95% CI, 9.86 to 16.34, p < 0.001), but contrary to H8, no cue condition × PTSD group interaction emerged (Figure 2 and Table 3). Contrary to H3, H6, and H9, PA did not differ between the trauma and neutral cue conditions, or between those with and without likely PTSD, and no interaction emerged (Figure 2 and Table 3).
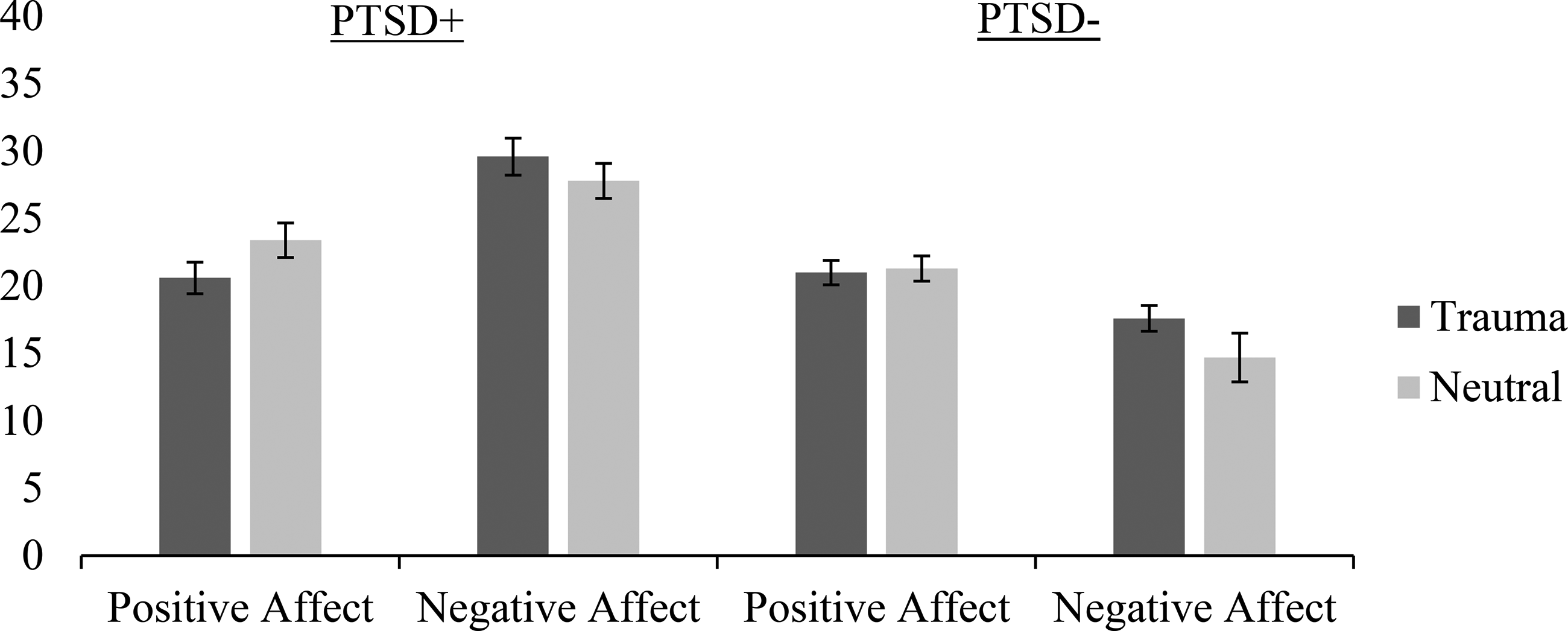
Mean negative and positive affect scores by posttraumatic stress disorder (PTSD) status.
Linear Mixed Models’ Omnibus Results for Affective Responses.
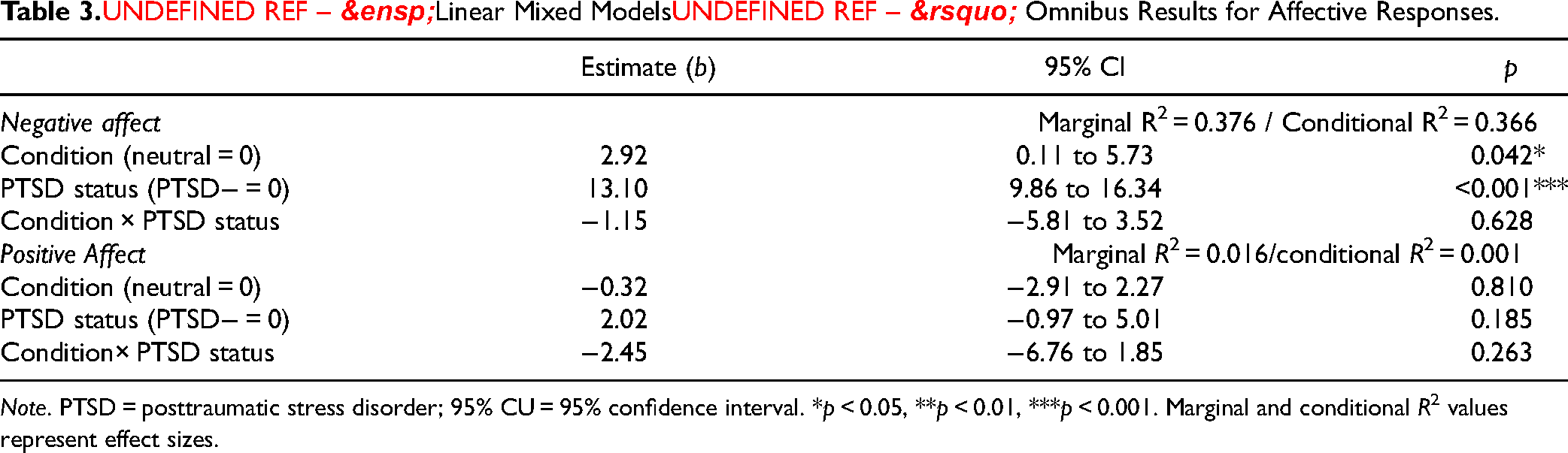
Note. PTSD = posttraumatic stress disorder; 95% CU = 95% confidence interval. *p < 0.05, **p < 0.01, ***p < 0.001. Marginal and conditional R2 values represent effect sizes.
Analyses of Potential Covariates: Our analyses of potential covariates revealed a statistically significant effect of PTSD group on age (t[198] = −9.36, 95% CI, −15.00 to 3.72, p < 0.001), CUDIT-R (t[198] = 10.59, 95% CI, 8.40 to 12.78, p = 0.002), PHQ-ADS (t[198] = 18.28, 95% CI, 14.61 to 21.95, p < 0.001), baseline NA (t[198] = 12.27, 95% CI, 8.93 to 15.62, p < 0.001), and baseline emotionality (t[198] = 1.29, 95% CI, 0.60 to 1.98, p < 0.001), expectancy (t[198] = 1.23, 95% CI, 0.57 to 1.88, p ≤ 0.001), and compulsivity craving (t[198] = 1.24, 95% CI, 0.60 to 1.88, p ≤ 0.001), a significant effect of cue condition on writing task word count (t[198] = 30.16, 95% CI, 3.77 to 56.55, p = 0.025), and a significant interaction between PTSD and cue condition on the number of lifetime traumas (t[198] = 2.57, 95% CI, −0.02 to 5.17, p = 0.05). These covariates were controlled in a series of sensitivity analyses to test whether the effects in the primary analyses persisted.
Sensitivity Analyses: All PTSD group effects remained when controlling PTSD group differences in the identified covariates except: compulsivity craving when controlling baseline levels; expectancy, emotionality, and purposefulness craving when controlling PHQ-ADS; and purposefulness craving when controlling CUDIT-R. Both cue condition effects remained when controlling cue condition differences in writing task word count and number of lifetime traumatic experiences (Supplemental Tables S2–S4).
Discussion
The primary aims of our study were to eliminate the attrition common to 2-session trauma CRP studies and recruit a sufficiently large sample to allow detection of both main and interactive cue condition and PTSD group effects on outcomes relevant to understanding PTSD–CUD comorbidity. Our online trauma cue exposure—an expressive writing task—significantly increased the expectancy of cannabis craving and NA relative to the neutral writing task. Likely PTSD was a significant predictor of all craving dimensions and NA. No interactions emerged for any outcome, though for NA and expectancy craving, the greatest reactivity was observed in those with likely PTSD who completed the trauma-expressive writing task.
Partially consistent with expectations (H1), writing about a personal traumatic (vs. neutral) event did enhance expectancy craving. Theory suggests trauma cue exposure might enhance state expectancies regarding the perceived relieving effects of cannabis. 41 While the MCQ-SF expectancy scale lacks relief-reward differentiation, 42 2 of its 3 items conceptually tap cannabis relief expectancies (i.e., decreased nervousness and sleeping better); this suggests the expectancy of relief from cannabis following trauma cue exposure may drive the increased cannabis craving tapped on this scale. Importantly, other CRP studies15,43 have shown the effects of trauma CRPs eliciting cannabis craving across all 4 dimensions of the MCQ-SF. This difference may be due to the nature of our trauma CRP, an online writing task, whereas prior CRP studies15,43 used an in-person CRP. Perhaps the potential to stop writing, 16 combined with the lack of experimenter presence, reduced the efficacy of our CRP in eliciting some cannabis craving dimensions (e.g., feeling more in control might reduce compulsivity craving).
As expected (H4), likely (vs. no) PTSD significantly predicted heightened cannabis craving across MCQ-SF subscales. This is partially consistent with prior findings of the main effects of PTSD symptom severity on the compulsivity, purposefulness, and emotionality (but not expectancy) dimensions of cannabis craving. 15 Perhaps our use of a categorical predictor (i.e., likely PTSD vs. no PTSD) was more sensitive to PTSD effects on expectancy craving than the continuous PTSD symptom severity measure used previously, 15 given the results of latent class analyses that emphasize categorical variations rather than continuous gradients in PTSD symptoms within trauma-exposed samples.44–46
As expected (H2) and consistent with prior work,18,43 NA was greater following the trauma than neutral expressive writing CRP. This finding replicates our prior research showing trauma CRPs to be predictors of increased NA compared to neutral cues or baseline.13,14 Further, likely PTSD predicted greater post-cue NA overall, a result consistent with H5 and with prior findings. 15 Contrary to H3 and H6, neither cue condition nor PTSD predicted lesser PA. This pattern of results, along with the greatest effect sizes in our study being detected for NA (Table 3), provides evidence that trauma CRPs are primarily NA inductions,14,16 and is consistent with reports that greater PTSD symptoms predict greater NA but not lesser PA to trauma cue exposure. 15
Interestingly, NA and expectancy craving were influenced by both the expressive writing condition and PTSD group. Although no interactions were detected, individuals with likely PTSD in the trauma condition showed the highest levels of NA and expectancy craving postwriting, indicating activation of NA and relief craving by trauma cue exposure, as possible mechanisms of PTSD–CUD comorbidity. Indeed, this finding supports Baker et al.'s 47 theoretical framework, suggesting the act of writing about a personal trauma may heighten not only distress but also substance cravings among users as substance use is anticipated to relieve the distress provoked by trauma memories.
Several potential limitations should be considered when interpreting our results. First, while our data were stringently vetted for quality, the online method precluded determining whether participants precisely followed expressive writing instructions. Specifically, while we asked participants to write for a minimum of 2 min and prevented them from moving on until this minimum had elapsed, many responses were short. Verbal descriptions from in-lab interviews may offer more vivid imagery than written ones without an experimenter present, possibly explaining the lack of interactions on all outcomes. In fact, some prior research using the traditional CRP in the 2-session protocol showed positive interactions between cue condition and PTSD in predicting cue-elicited craving for cocaine and cannabis.15,43 Perhaps those with PTSD were more avoidant during the trauma writing task (e.g., stopping writing when feeling anxious), working against the hypothesized interactions.
To maintain participant focus without the necessity of a laboratory setting, in future, participants might be asked to report on the quality of their visualization experience, including the option to indicate if they did not attempt to visualize the event. This additional step could screen out participants who did not fully engage with the task. While consistent with some prior research, 16 the 2 min minimum was substantially shorter than the 20 min writing sessions recommended by Pennebaker. 23 Future research should establish the optimal length of trauma-expressive writing in eliciting various forms of cue reactivity. A further limitation is that participants’ prior experience with prolonged exposure-based therapies was not measured or controlled. Finally, the PTSD group was established via a single-score cutoff on a self-report questionnaire rather than a clinical interview (the latter was not practical in a larger N, online study), which may have led to miscategorization.
Supplementary analyses suggested PTSD group effects on some outcomes may have been secondary to pre-existing baseline differences in the case of compulsivity craving; PTSD group differences in general distress in the cases of expectancy, emotionality, and purposefulness craving; and PTSD group differences in CUD symptoms in the case of purposefulness craving. Thus, studies of PTSD group effects on cue-induced craving should assess and control for these potentially important confounds. Finally, we only focused on a controlled cognitive process (i.e., craving). 15 Automatic cognitive processes (i.e., requiring less awareness, assessed indirectly through reaction time or association tasks) 48 may also be relevant to understanding PTSD–CUD comorbidity16,20 and should be probed using the stand-alone expressive writing CRP in future.
Our findings have several clinical implications. NA and expectancy craving were highest in participants with likely PTSD who wrote about trauma, suggesting these affective and cognitive outcomes elicited by trauma cue exposure should be specific targets of intervention for treating/preventing comorbid CUD in cannabis users with PTSD. It would be informative to test whether exposure-based intervention for PTSD–CUD not only reduces NA to trauma cue exposure but also trauma cue-elicited cannabis relief expectancies or whether specific interventions to target these expectancies need to be added, such as via expectancy challenge techniques. 49 Indeed, existing safe and efficacious integrated therapies for concurrent PTSD–SUD (including CUD), such as the COPE treatment, 50 address both disorders concurrently and target underlying mechanisms that contribute to their maintenance and exacerbation. 50 Such integrated treatments involve verbal recounting of the trauma with one's provider rather than written expressions of trauma as the exposure component. Given lower attendance, but higher efficacy, was seen for cannabis users receiving in-person exposure-based (vs. non-exposure-based) treatment for comorbid PTSD–SUD in a recent meta-analysis, 51 remote exposure-based interventions may be helpful for increasing treatment attendance in this population.
Future trials could aim to validate the use of remote expressive writing about one's trauma as the exposure component in such integrated treatments for comorbid PTSD–SUD, 52 given our findings that the expressive writing CRP successfully elicited the NA necessary for corrective emotional processing. 53 Indeed, extending work showing expressive writing about trauma to be an effective exposure therapy for PTSD,49,50 a randomized controlled trial of 149 women with an SUD assigned to either a 4-session trauma or neutral expressive writing intervention showed those randomized to the trauma condition reported decreased PTSD symptoms at follow-up. 54 Moreover, the anxiety elicited by the trauma writing task habituated by the 4th session. 54 These results suggest promise for expressive writing as a form of exposure therapy for comorbid PTSD–SUD, but results require extension to substance-relevant outcomes. 55 Overall, it is important to conduct feasible, adequately powered CRP research, as this work can inform refinements to integrated trauma exposure-based treatments for comorbid PTSD–SUD. 56
Supplemental Material
sj-docx-1-cpa-10.1177_07067437241255104 - Supplemental material for Effects of Trauma Cue Exposure and Posttraumatic Stress Disorder (PTSD) on Affect and Cannabis Craving in Cannabis Users With Trauma Histories: Use of Expressive Writing as an Online Cue-Reactivity Paradigm: Effets de l'exposition aux signaux traumatiques et du SSPT sur l'affect et le besoin de cannabis chez les consommateurs de cannabis ayant des antécédents de traumatismes : utilisation de l'écriture expressive comme paradigme de réactivité en ligne
Supplemental material, sj-docx-1-cpa-10.1177_07067437241255104 for Effects of Trauma Cue Exposure and Posttraumatic Stress Disorder (PTSD) on Affect and Cannabis Craving in Cannabis Users With Trauma Histories: Use of Expressive Writing as an Online Cue-Reactivity Paradigm: Effets de l'exposition aux signaux traumatiques et du SSPT sur l'affect et le besoin de cannabis chez les consommateurs de cannabis ayant des antécédents de traumatismes : utilisation de l'écriture expressive comme paradigme de réactivité en ligne by Sarah DeGrace, Sean P. Barrett, Igor Yakovenko, Philip G. Tibbo, Pablo Romero-Sanchiz, R. Nicholas Carleton, Thomas Snooks, Abraham Rudnick and Sherry H. Stewart in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Nova Scotia Health Authority Research Fund, Dalhousie Medical Research Foundation, Chronic Pain Centre of Excellence for Canadian Veterans, Tier 1 Canada Research Chair in Addictions and Mental Health, L’Oréal-UNESCO & France–Canada Research Fund, Dalhousie University, Commission de la santé mentale du Canada, (grant number MacQuarrie Neuroscience Research Graduate Students, Capacity Building Initiative, Women in Science Scholarship, Dr Paul Janssen Chair in Psychotic Disorders, Cannabis and Mental Health Catalyst Grant).
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.