
Abstract
Background:
There is continuing debate as to the latent structure underpinning posttraumatic stress disorder symptomatology. The transdiagnostic vulnerability factors of negative affect, anxiety sensitivity (and subcomponents) and intolerance of uncertainty have previously demonstrated the ability to explain symptom clusters in a range of anxiety and depressive disorders, and may give further understanding of PTSD symptomatology.
Method:
Within an Australian Defence Force veteran population, structural equation modeling is utilized to assess whether a hierarchical Original Model containing negative affect as the general cognitive factor, anxiety sensitivity and intolerance of uncertainty as mid-level factors, can explain variability among posttraumatic stress disorder symptom clusters as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. A further hierarchical Anxiety Sensitivity Extended model consisting of the general cognitive factor of negative affect and the three sub-factors of anxiety sensitivity as mid-level factors was also tested upon PTSD symptom clusters.
Results:
Both the hierarchical Original and Anxiety Sensitivity Extended models fit the data well. Within both models, negative affect consistently showed significant direct effects upon the posttraumatic stress disorder symptom clusters. In the Original Model, anxiety sensitivity served as a significant mediator of negative affect for several symptom clusters, while intolerance of uncertainty was non-significant both as a direct effect and as a mediator of negative affect. In the Anxiety Sensitivity Extended Model, the cognitive concerns sub-factor of anxiety sensitivity served as a significant mediator of negative affect for several symptom clusters, while the social and physical concerns sub-factors did not have significant direct or mediating effects.
Conclusions:
This study demonstrates a transdiagnostic hierarchical model significantly explains the severity of Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition posttraumatic stress disorder symptom constructs within a subclinical population. Negative affect and anxiety sensitivity can each be targeted with specific interventions, suggesting new avenues to augment current gold standard psychotherapeutic interventions.
In addition to regular training, the Australian Defence Force (ADF) has been on continuous overseas operations since 1999. This tempo is widely regarded as contributing to a number of mental health concerns in ADF veterans, including posttraumatic stress disorder (PTSD; Oster et al., 2017). Within the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association, 2013), the symptoms of PTSD are arranged under four distinct symptom clusters of intrusions, avoidance, negative alterations in cognitions and mood and alterations in arousal and reactivity (hyperarousal). However, both these symptom clusters and the individual symptoms of PTSD show a high level of comorbidity and symptom overlap with other anxiety and depressive disorders. This overlap has become an increased focus of researchers over the past decade (Barnes et al., 2018). One strategy to understanding commonalities among psychiatric disorders, including that of PTSD, has been to investigate how symptomatology may relate to established transdiagnostic factors.
The transdiagnostic approach states the differing anxiety and depressive disorders are fundamentally linked by deeper factors, as opposed to being separate ontological constructs (Norton and Paulus, 2017). Three dominant transdiagnostic factors within the literature are negative affect, anxiety sensitivity and intolerance of uncertainty, with each of these demonstrating unique links to PTSD symptomatology. Negative affect predisposes an individual to experience emotions such as depression, anxiety and fear (Watson et al., 1988a) and is associated with increased risk of developing PTSD, as well as greater symptom severity (Brown et al., 2018). Anxiety sensitivity is a cognitive trait causing the individual to fear their anxiety-related symptoms (McNally, 1999) and has also been linked to increased risk of developing (Cobb et al., 2017), and the severity of (Marshall et al., 2010), PTSD symptoms. Finally, intolerance of uncertainty is conceptualized as a trait-like cognitive vulnerability of a negative perception and fear of uncertainty and its ramifications (Dugas and Robichaud, 2012) with demonstrated links to the PTSD symptom clusters of hyperarousal and intrusions (Bardeen et al., 2013; Oglesby et al., 2016).
These three transdiagnostic factors are conceptualized as relating to one another in a hierarchical fashion. As initially proposed by Sexton et al. (2003), negative affect is regarded as the higher order personality factor, with direct though disparate links to the differing anxiety and depressive disorders. In order to account for this relative diversity, anxiety sensitivity (conceptualized as a more immediate fear-based construct) and intolerance of uncertainty (conceptualized as a future-orientated sense of anxiety) are seen as secondary cognitive factors mediating the influence of negative affect. Using simple path analysis with a sample of undergraduate students, Sexton et al. (2003) found support for this model where negative affect directly influenced anxiety sensitivity and intolerance of uncertainty which, in turn, differentially associated with panic, health anxiety, obsessive-compulsive and generalized anxiety symptoms. This model was subsequently replicated using simple path analysis with a sample of outpatients presenting to a hospital-based mood and anxiety disorder clinic (Norton et al., 2005).
Noting the potential for measurement error inherent to regression analyses, as well as to address the inability of such analyses to assess mediated pathways between the variables, Norton and Mehta (2007) utilized structural equation modeling to test this hierarchical model upon anxious and depressive symptoms within a non-clinical community sample. This approach was furthered by Paulus and colleagues (2015) within an independent out-patient anxiety disorder sample, who showed this model could identify commonalities, as well as account for heterogeneity among multiple anxiety and depressive diagnoses. Specifically, in both Norton and Mehta (2007) and Paulus and colleagues (2015), negative affect accounted for a significant amount of variance in all the tested anxiety and depressive disorders. Anxiety sensitivity, but not intolerance of uncertainty, further accounted for unique aspects of fear-based disorders (e.g. panic disorder), while intolerance of uncertainty, but not anxiety sensitivity, was associated with anxious-distress based disorders (e.g. generalized anxiety disorder, obsessive compulsive disorder). However, none of these four studies (Norton and Mehta, 2007; Norton et al., 2005; Paulus et al., 2015; Sexton et al., 2003) examined PTSD or posttraumatic symptoms.
Indeed, while no prior study has employed the full hierarchical model to examine PTSD, two studies have examined the relationship between components of the hierarchical model and PTSD, with each showing a strong relationship between intolerance of uncertainty and specific DSM-5 PTSD symptom clusters (Oglesby et al., 2017; Raines et al., 2019). However, Raines and colleagues only measured intolerance of uncertainty and anxiety sensitivity, and not negative affect. Oglesby and colleagues, although measuring each of the aforementioned transdiagnostic factors, showed a large degree of collinearity between intolerance of uncertainty and the PTSD symptom clusters, which raises questions as to the explanatory effect of intolerance of uncertainty.
Building on those initial studies, Kreminski et al. (2021) recently tested the hierarchical version of the model upon DSM-5 PTSD symptom clusters in a trauma-exposed community sample and found negative affect was the dominant explanatory factor in each of the symptom clusters. Anxiety sensitivity acted as a partial mediator across all symptom clusters, with additional unique direct effects upon the intrusions and hyperarousal constructs (Kreminski et al., 2021). However, contrary to the findings of both Oglesby and colleagues (2017) and Raines and colleagues (2019), intolerance of uncertainty was not a significant predictor of any PTSD symptom cluster, as either a direct effect or a mediator. Thus, although preliminary and requiring replication, it would appear the PTSD symptoms clusters have a stronger link to the immediate-fear based construct of anxiety sensitivity than to the more future-focused construct of intolerance of uncertainty, when examined together within the hierarchical model.
Although multiple studies have shown anxiety sensitivity, overall, relates to PTSD symptom clusters (Cobb et al., 2017; Kreminski et al., 2021; Marshall et al., 2010), its various sub-factors may be differentially related to PTSD symptoms. Anxiety sensitivity includes three individual sub-factors: (1) cognitive concerns (where the individual fears the sensation of cognitive dyscontrol), (2) physical concerns (where the individual fears the physical sensations of their anxiety) and (3) social concerns (where the individual fears social judgment of their anxiety reactions; (McNally, 2002). These sub-factors have shown differing effects upon different emotional disorders, with physical concerns strongly loading onto both panic disorder and agoraphobia (Olatunji and Wolitzky-Taylor, 2009; Zinbarg et al., 2001), social concerns showing stronger links to social anxiety disorder and major depressive disorder (Allan et al., 2014; Olatunji and Wolitzky-Taylor, 2009) and cognitive concerns related to generalized anxiety disorder (Allan et al., 2014; Olthuis et al., 2014). Cognitive concerns have also demonstrated strong links upon both overall PTSD symptom severity (Farris et al., 2016) as well as severity of each of the individual PTSD symptom clusters (Raines et al., 2017b).
In addition to the empirical evidence, there are conceptual links between the cognitive concerns sub-factor and PTSD. A trauma-exposed individual with elevated cognitive concerns of losing control may be more acutely distressed by their cognitive PTSD symptoms (such as intrusive thoughts or exaggerated negative beliefs). This distress, and subsequent avoidant behaviors, may in turn inadvertently amplify these symptoms (Raines et al., 2017b). Of potential clinical utility, cognitive concerns have been shown to mediate the relationship between PTSD symptoms and suicidality (Raines et al., 2017a) and the targeting of this sub-factor has been shown to lead to reductions in PTSD symptomatology (Mitchell et al., 2014). Accordingly, the anxiety sensitivity sub-factor of cognitive concerns is seen to have clear and established links to PTSD symptomatology.
The previous study by Kreminski et al. (2021) examined the total anxiety sensitivity construct, but not the sub-factors. It is therefore possible the potential effects of cognitive concerns may have been suppressed by the other two anxiety sensitivity sub-factors. If true, the variance in PTSD symptoms clusters accounted for by negative affect may have been overestimated and/or the variance accounted for by the cognitive concerns sub-factor of anxiety sensitivity may have been underestimated. Furthermore, as Kreminski et al. (2021) was conducted within a general population, its findings, and the potential clinical implications identified, may not generalize to populations with repeated or severe trauma exposure. In contrast, ADF veterans, compared to the general Australian population, experience an approximately threefold risk of high or very-high psychological distress, with an estimated 12-month prevalence of PTSD of 17.7% (Van Hooff et al., 2018). Furthermore, with 80% of ADF veterans diagnosed with PTSD experiencing co-morbidity with at least one other affective disorder, there is an identified need within this population to research potential factors underpinning this distress (Van Hooff et al., 2018).
The aims of the current study were twofold. The first aim was to replicate and extend the findings with the original hierarchical model (Original Model; Kreminski et al., 2021) to a sub-clinical population typically experiencing multiple trauma exposures, and therefore at higher risk of developing PTSD (i.e. veterans of the ADF). The second aim, based on the findings of Kreminski et al. (2021), was to assess the fit of a modified hierarchical model consisting of negative affect as the higher-order factor and only the anxiety sensitivity sub-factors as secondary factors upon DSM-5 PTSD symptom clusters within this population (Anxiety Sensitivity Extended Model). This study had three hypotheses: (1) within the Original Model, negative affect will show direct effects upon all the DSM-5 PTSD symptom clusters, anxiety sensitivity will show direct effects on only the intrusions and hyperarousal symptom clusters, while intolerance of uncertainty will show no direct effects on any of the PTSD symptom clusters; (2) within the Original Model, anxiety sensitivity but not intolerance of uncertainty will partially mediate the effects of negative affect upon all PTSD symptom clusters; and (3) within the Anxiety Sensitivity Extended Model, cognitive concerns will predict more variance in each of the four DSM-5 PTSD symptom clusters than the sub-factors of physical or social concerns; however, negative affect will continue to explain a greater amount of variance overall in the symptom clusters.
Method
Participants
Participants were 209 veterans of the ADF (82.8% male, 15.3% female, 0.96% non-binary, 0.96% unknown; for further demographic information see Table 1) recruited online through social media posts. The inclusion criteria were the participant being over the age of 18, a veteran of the ADF, residing in Australia, and self-reporting a prior exposure to a traumatic event, as defined by DSM-5 criterion A, of actual or threatened death, injury or sexual assault (American Psychiatric Association, 2013). There were no additional, specific, exclusion criteria.
Demographic Information.
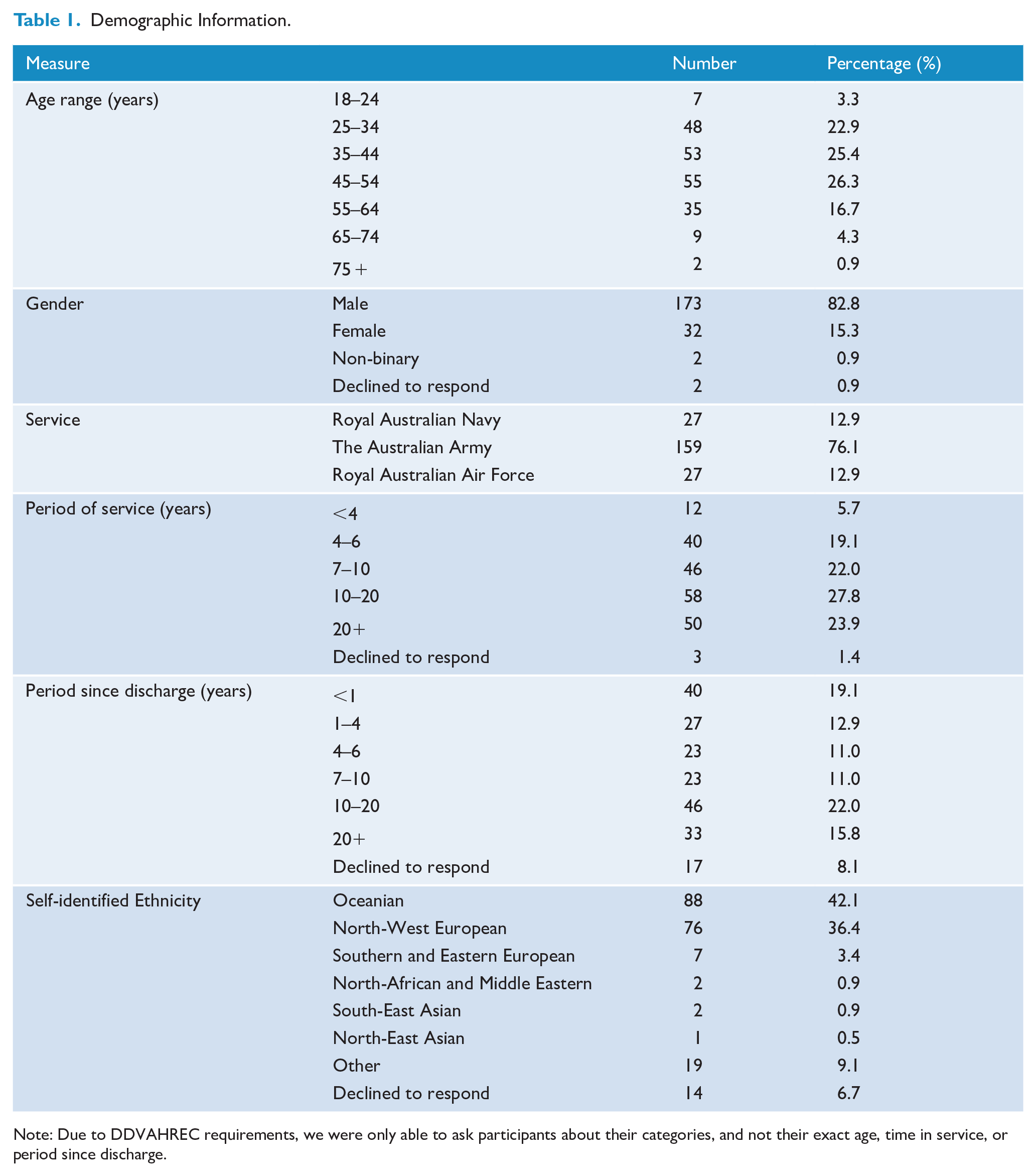
Note: Due to DDVAHREC requirements, we were only able to ask participants about their categories, and not their exact age, time in service, or period since discharge.
Procedures
This study was performed in line with the principles of the declaration of Helsinki, with both the Departments of Defense and Veterans’ Affairs Human Research Ethics Committee (DDVAHREC; Protocol 207-20) and the Monash University Human Research Ethics Committee (MUHREC; Protocol 27639) approving all procedures for this study. Written informed consent was obtained from all individual participants included in the study. Participants were recruited online through social media and, per DDVAHREC requirements, were not provided with financial remuneration or any other form of incentive. Participants were provided with a web-link and invited to participate in an online Qualtrics-based survey at their own convenience. The survey was introduced as research on the effects deeper state-based traits could have upon traumatic symptoms. Participants were initially asked if they were a veteran of the ADF and whether or not they had been exposed to a traumatic event as per DSM-5 criterion A. Participants then completed each questionnaire, as well as measures of conscientious responding (Marjanovic et al., 2014).
Measures
The Life Events Checklist for DSM-5 (LEC-5; Weathers et al., 2013a)
This measure screens for potentially traumatic events across the respondent’s lifetime. There are 16 different events assessed (e.g. ‘fire or explosion’) which have been shown to potentially result in PTSD, as well as the option of adding an unlisted event. Participants indicate which event(s) they have encountered and how they encountered it (e.g. ‘part of my job’). In order to meet DSM-5 Criterion A and be eligible for the study, participants had to indicate exposure (they witnessed it/ happened to them/ part of their job/ they learned about it happening to a close other/) to one or more of the 16 specific events.
Positive and Negative Affect Scale (PANAS; Watson et al., 1988b)
This self-report test uses 20 items to measure both negative and positive affect. A 5-point Likert-type scale is used to score the items ranging from 0 (very slightly or not at all) to 4 (extremely) on how regularly they felt a particular way over the past few weeks; sample items include ‘guilty’ and ‘excited’. Higher scores indicate greater levels for each subscale construct. Good internal consistency has been reported previously for both the negative (α = .84-.87) and positive (α = .86-.90) affect subscales (Watson et al., 1988b). Within the current study, negative affect was measured using the negative affect subscale, with these 10 items demonstrating excellent internal consistency (α = .92).
The Anxiety Sensitivity Index—Version 3 (ASI-3; Taylor et al., 2007)
This test utilizes 18 items to measure the 3 factors of anxiety sensitivity; physical, social and cognitive concerns. Items are rated a 5-point Likert-type scale from 0 (very little) to 4 (very much); sample item ‘I worry that other people will notice my anxiety’. Each factor’s score calculated (range: 0–24) with higher scores indicating higher levels of anxiety sensitivity, before being summed to generate a total score (range: 0–72). This measure’s subscales have been shown to have good internal consistency and construct validity (α = 0.73–0.91; Taylor et al., 2007). Within the current study, the subscales utilized to measure the sub-factors of anxiety sensitivity: social concerns (α = 0.81), cognitive concerns (α = 0.93) and physical concerns (α = 0.87), demonstrated either good or excellent internal consistency.
Intolerance of Uncertainty Scale 12-Item (IUS-12; Carleton et al., 2007)
This self-report test utilizes 12-items to measures the 2 factors of intolerance of uncertainty: inhibitory and prospective anxiety. A Likert-type scale is used to score the items ranging from 0 (not at all characteristic of me) to 4 (entirely characteristic of me); sample item ‘I can’t stand being taken by surprise’. Each sub-factor’s scale score is calculated (range: 0–30) with higher scores indicating higher levels of intolerance of uncertainty, and then summed to generate a total score (range: 0–60). This scale demonstrated both excellent internal consistency (α = 0.91) as well as comparing to the original 27-item scale (r = 0.96; Carleton et al., 2007). Within this study, the two subscales utilized as indicators of the intolerance of uncertainty construct, inhibitory anxiety (α = 0.91) and prospective anxiety (α = 0.83), showed excellent and good internal consistency respectively.
Posttraumatic Checklist for DSM-5 (PCL-5; Blevins et al., 2015)
This measure utilizes 20-items to measure each of the PTSD symptoms for the DSM-5 conceptualization of the disorder. Participants utilize a 5-point Likert-type scale to indicate over the past month how often they were bothered by various trauma symptoms ranging from 0 (not at all) to 4 (extremely); sample item ‘Repeated, disturbing dreams of the stressful experience?’ with higher scores indicative of higher trauma symptoms. The PCL-5 has demonstrated excellent internal consistency (α = 0.94), good test–retest reliability (r = 0.82) and convergent validity (rs = 0.74–0.85; Blevins et al., 2015). Within the current study, the DSM-5 symptom clusters of intrusion (α = 0.92), avoidance (α = 0.89), negative alterations in cognition and mood (α = 0.90), and hyperarousal (α = 0.85) showed either good or excellent internal consistency. Although not a formal diagnostic scale, a provisional diagnosis can be made if a participant scores 33 or higher on the PCL-5 (Weathers et al., 2013b), with 125 participants (61%) in the current sample meeting this criterion.
Data Analyses
All assumptions for structural equation modeling were initially tested utilizing Statistical Package for the Social Sciences (SPSS) version 23. Of the eligible participants, 287 initiated the survey with 71 withdrawing from the survey before completion for unknown reasons (for further information on withdrawal rates, please see Table 2). Of the remaining 216 participants, a further 7 were identified as engaging in non-conscientious responding (Marjanovic et al., 2014), and their data were excluded. The utilization of electronic data collection and required responses meant there were no data missing from the remaining 209 participants in the dataset. Structural equation modeling model fit was tested with MPlus (Muthen and Muthen, 2012). The first Original Model, based upon Kreminski et al. (2021), Norton and Mehta (2007), and Paulus et al. (2015) was hierarchical, including negative affect as a higher order factor and anxiety sensitivity and intolerance of uncertainty as mid-level factors (see Figure 1). The second, Anxiety Sensitivity Extended Model was also hierarchical, including negative affect as the higher order factor and the anxiety sensitivity sub-factors of cognitive, physical and social concerns as mid-level factors (see Figure 2).
Per-measure Timing of Participant Study Withdrawal.
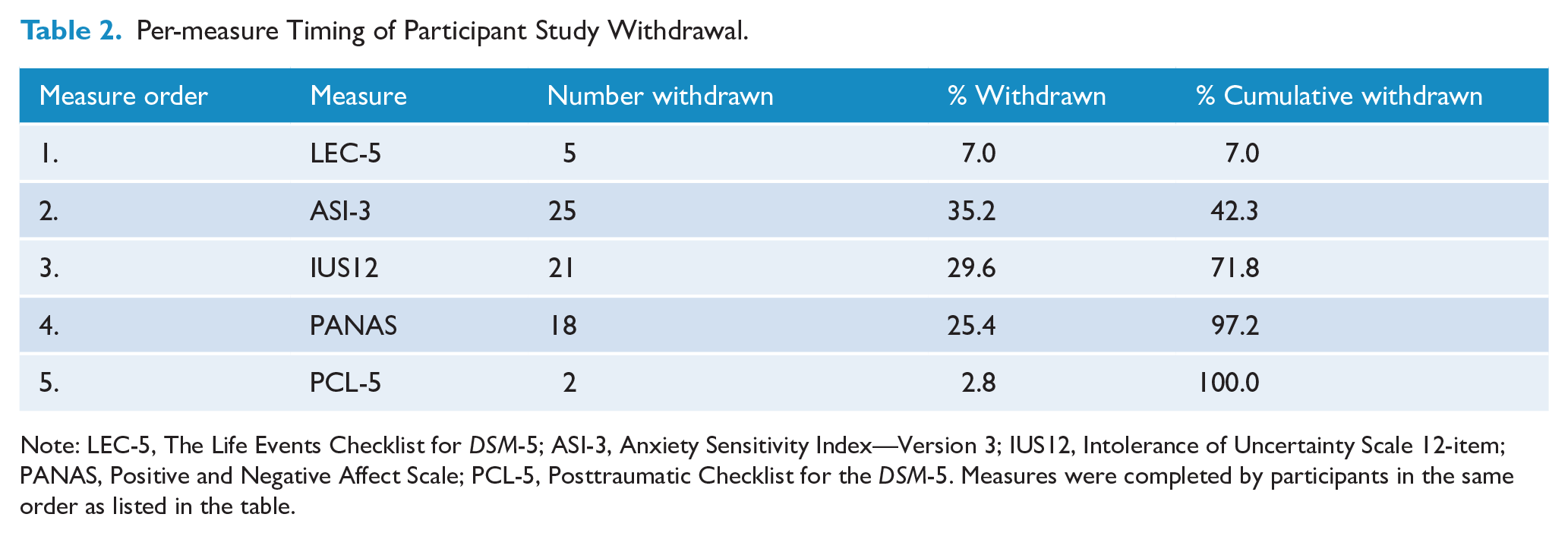
Note: LEC-5, The Life Events Checklist for DSM-5; ASI-3, Anxiety Sensitivity Index—Version 3; IUS12, Intolerance of Uncertainty Scale 12-item; PANAS, Positive and Negative Affect Scale; PCL-5, Posttraumatic Checklist for the DSM-5. Measures were completed by participants in the same order as listed in the table.
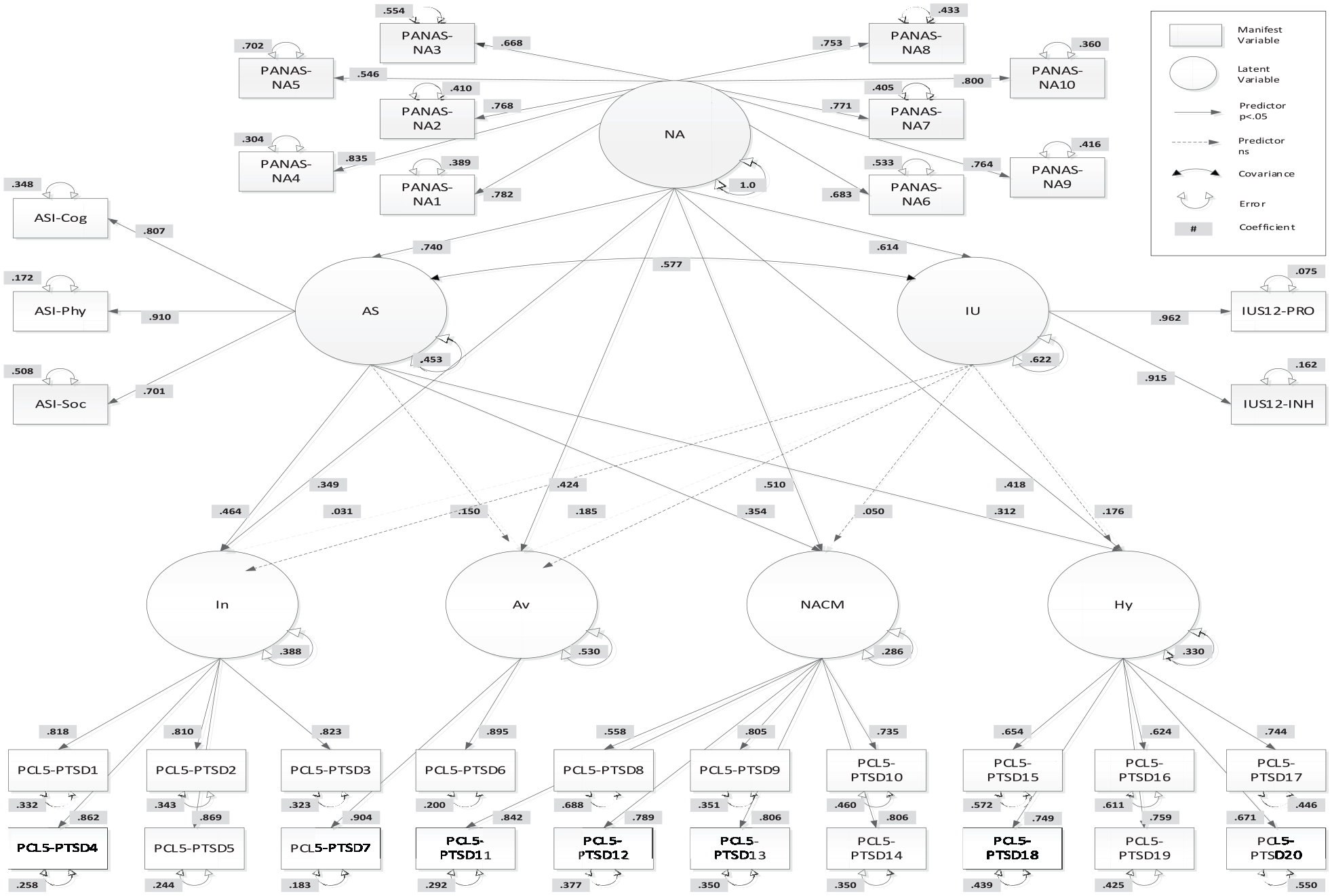
Hierarchical Original Model.
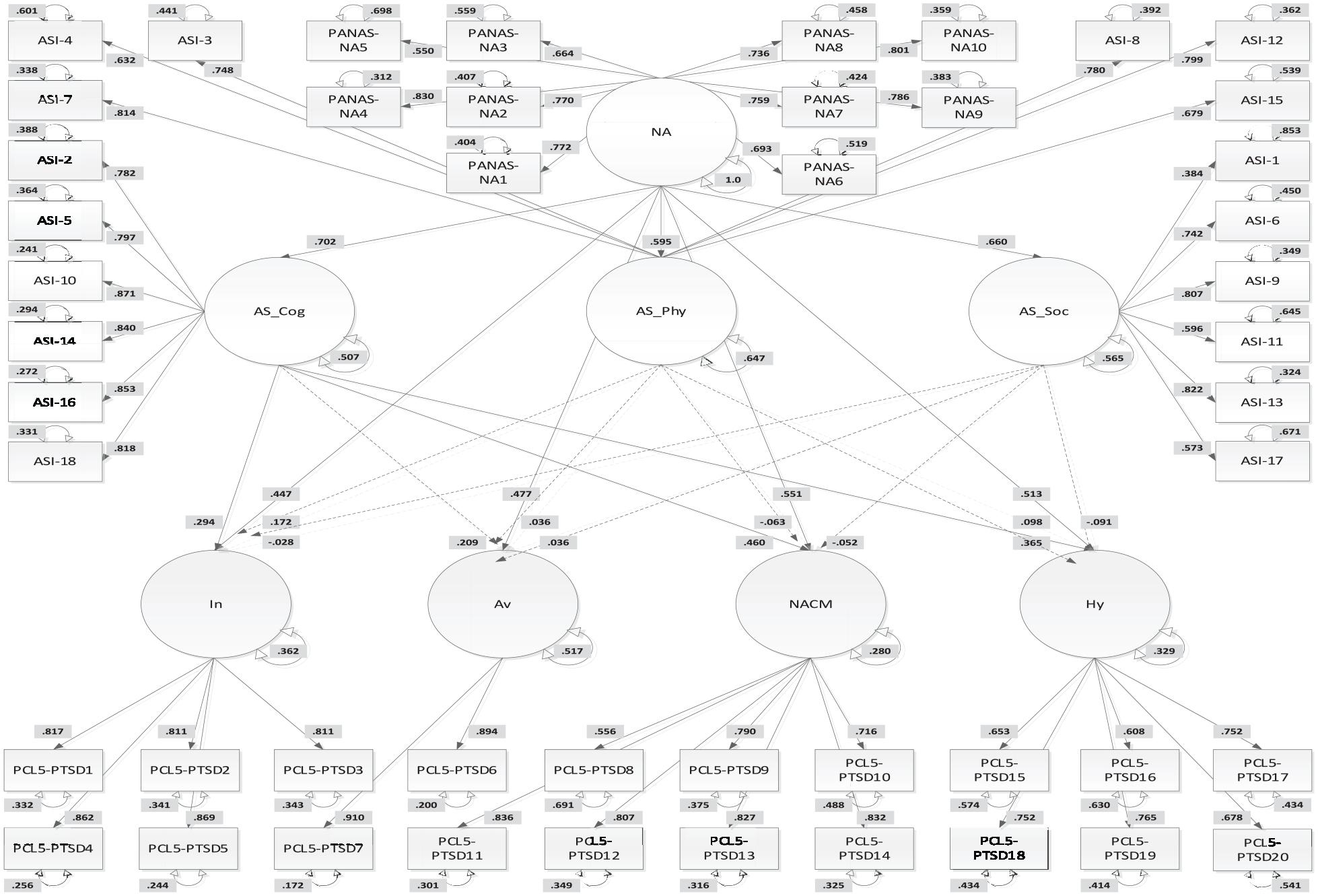
Hierarchical Anxiety Sensitivity Extended Model.
The direct and indirect effects of negative affect, anxiety sensitivity and intolerance of uncertainty in the first model, and negative affect and the anxiety sensitivity sub-factors of cognitive, physical and social concerns in the second model, were estimated for the latent constructs of PTSD symptom clusters (Evermann and Tate, 2016). This was done utilizing the DSM-5 conceptualization of PTSD with the four factors of intrusion, avoidance, negative alterations in cognition and mood, and hyperarousal (American Psychiatric Association, 2013). The dependent latent variables of the PTSD symptom constructs were allowed to correlate in both models.
Standardized root mean square residual (SRMR) values < .08 have been previously proposed as measures of good fit (Hu and Bentler, 1999). Ideally, root mean square error of approximation (RMSEA) should be between .02 and .07 (Browne and Cudeck, 1992). The accepted rule-of-thumb for comparative fit index (CFI) should be > .90 (Marsh and Hau, 1996).
Results
Descriptive statistics for each of the observed indicators in both models are provided in Table 3. The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Univariate Summaries of Observed Indicators.
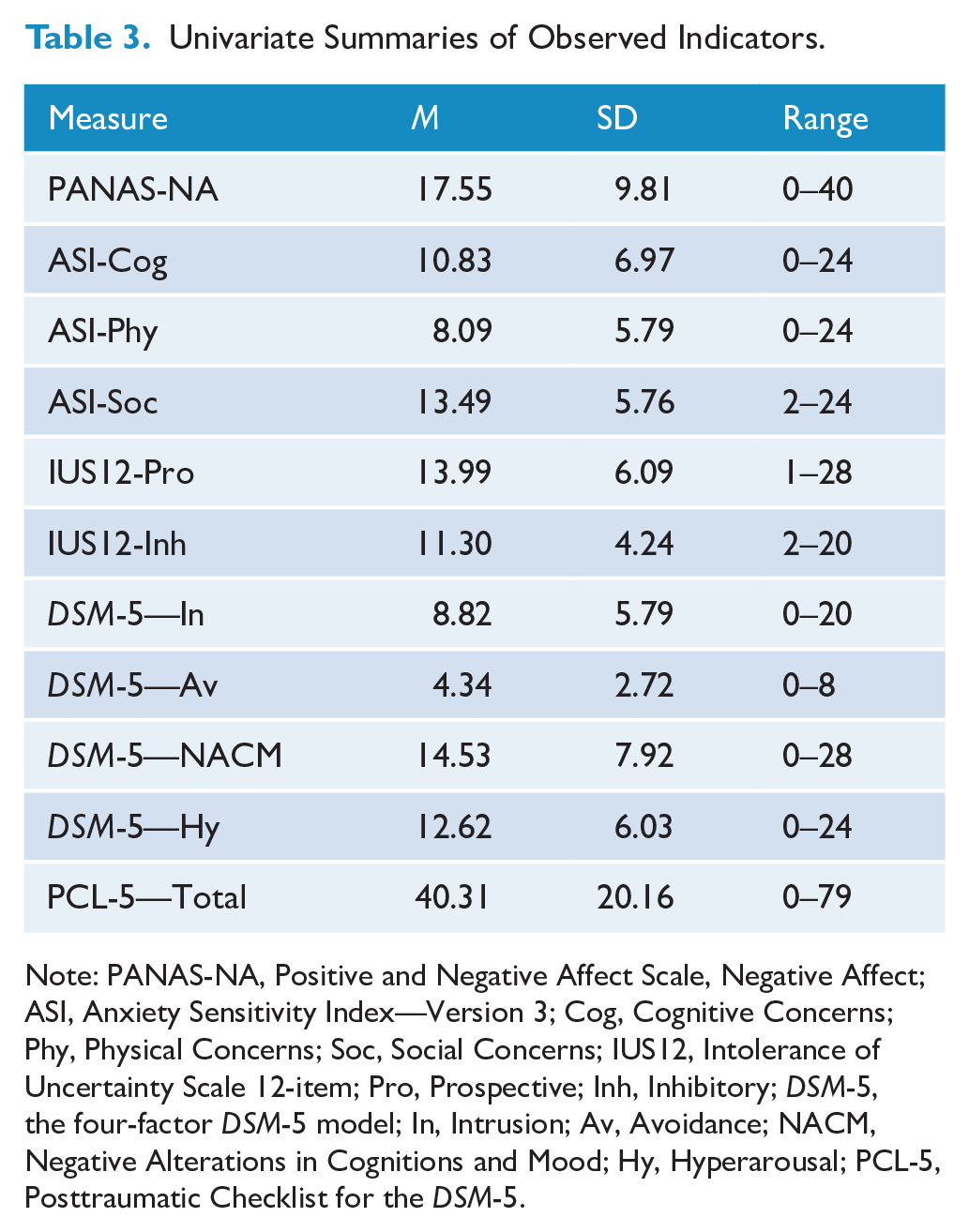
Note: PANAS-NA, Positive and Negative Affect Scale, Negative Affect; ASI, Anxiety Sensitivity Index—Version 3; Cog, Cognitive Concerns; Phy, Physical Concerns; Soc, Social Concerns; IUS12, Intolerance of Uncertainty Scale 12-item; Pro, Prospective; Inh, Inhibitory; DSM-5, the four-factor DSM-5 model; In, Intrusion; Av, Avoidance; NACM, Negative Alterations in Cognitions and Mood; Hy, Hyperarousal; PCL-5, Posttraumatic Checklist for the DSM-5.
Original Model
The sample covariances of the Original Model were well replicated and had adequate fit (SRMR = .06, RMSEA = .09, CFI = .86). As shown in Figure 1, each observed indicator was highly associated with the respective latent variable. Although not shown, the latent variables of the PTSD symptom clusters were significantly related to one another (rs = 0.37–0.75, p < 0.001). After accounting for the influence of negative affect, anxiety sensitivity and intolerance of uncertainty were significantly related to each other in the model (r = 0.58, p < 0.001).
Table 4 shows the direct effects of each factor within the Original Model, as well as the associations among the predictive factors within the model. Table 5 shows the results for the mediation analyses of negative affect. Negative affect showed strong associations with both anxiety sensitivity (R2 = 54.8%) and intolerance of uncertainty (R2 = 37.7%). Negative affect also showed direct associations with all latent symptom constructs. Percentage of variance explained (R2) for the latent constructs ranged from .38 to .71 with all ps < 0.001.
Standardized Direct Regression Coefficients for the Original Model.
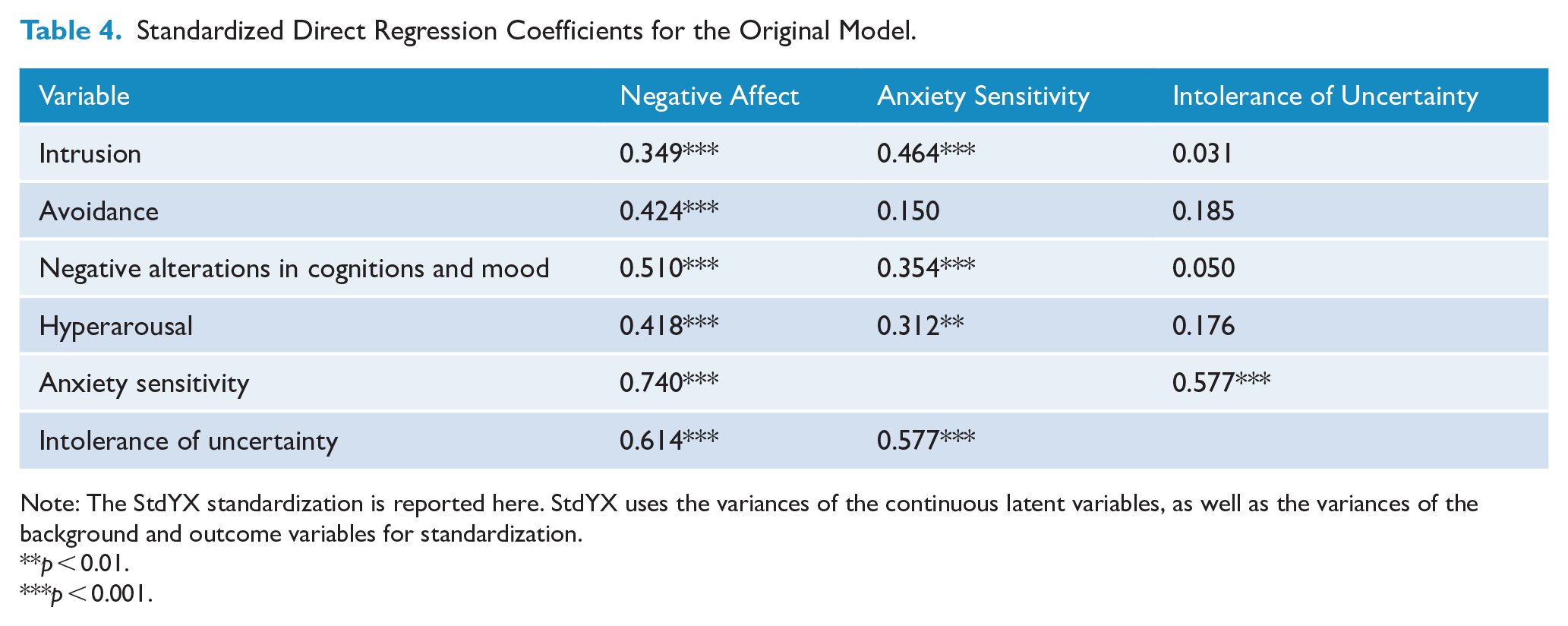
Note: The StdYX standardization is reported here. StdYX uses the variances of the continuous latent variables, as well as the variances of the background and outcome variables for standardization.
p < 0.01.
p < 0.001.
Direct, Indirect and Total Effects of Negative Affect for the Original Model.
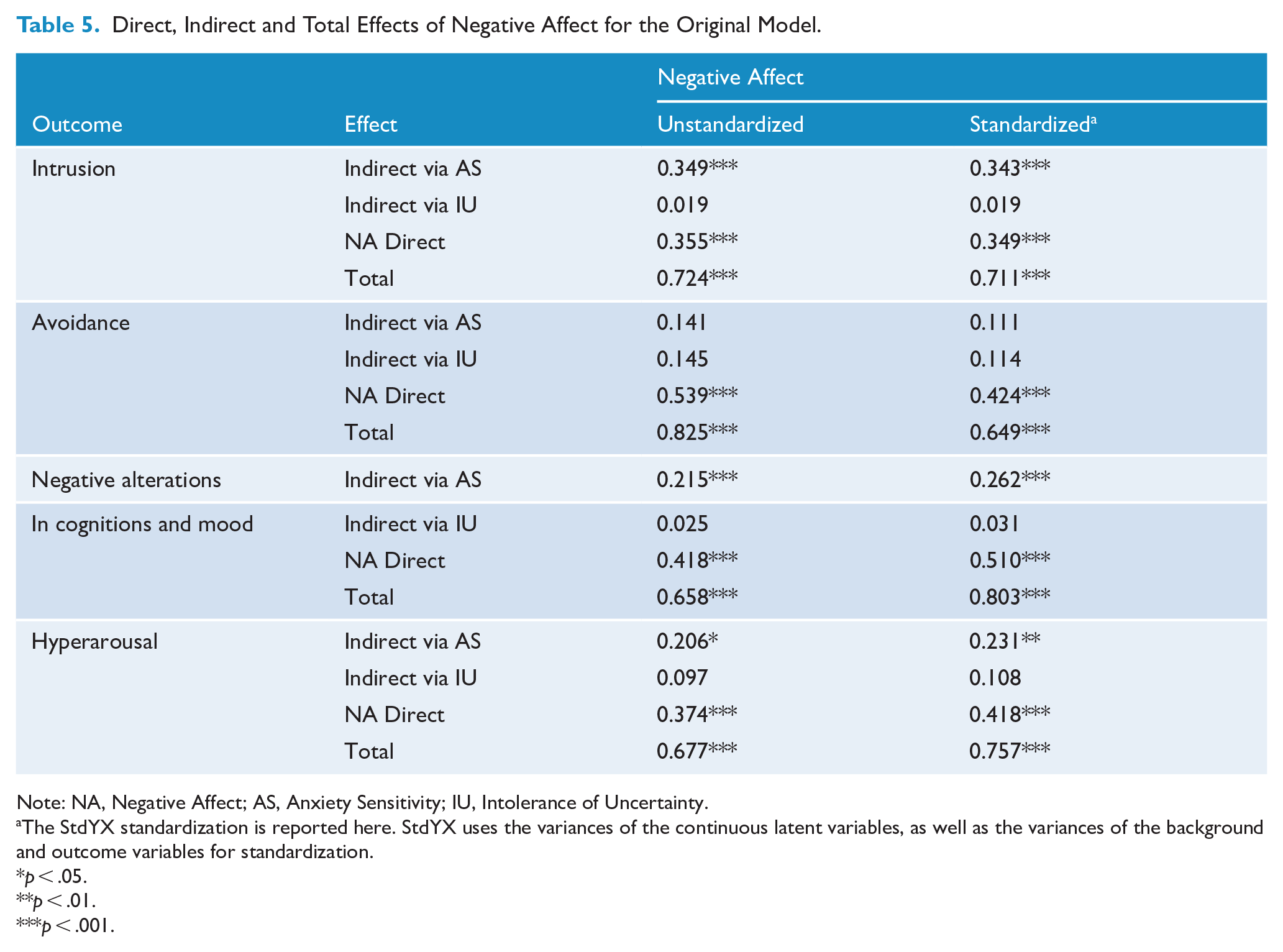
Note: NA, Negative Affect; AS, Anxiety Sensitivity; IU, Intolerance of Uncertainty.
The StdYX standardization is reported here. StdYX uses the variances of the continuous latent variables, as well as the variances of the background and outcome variables for standardization.
p < .05.
p < .01.
p < .001.
Intrusion
The model explained 61.2% of the variability in intrusion. Negative affect had a moderate direct effect on intrusion (β = .35), which accounted for 12.2% of the variance. Anxiety sensitivity had non-significant direct effect on intrusion (β = .12), contributing 1.5% of the variance. Its role as a mediator was much more substantial however, contributing an additional 11.8% via mediation of negative affect (β = .34). Intolerance of uncertainty was non-significant both as a direct effect (β = .01) and via mediation of negative affect (β = .02), contributing only 0.01% and .4% of the variance respectively.
Avoidance
The model explained 47.0% of the variability in avoidance. Negative affect had a direct effect on avoidance (β = .42) contributing 17.9% of the variance. Anxiety sensitivity was non-significant both as a direct effect (β = .04) and via mediation of negative affect (β = .11) where it contributed 0.2% and 1.2% of the variance respectively. Again, intolerance of uncertainty was non-significant both as a direct effect (β = .07) and via mediation of negative affect (β = .11), contributing 0.5% and 1.2% of the variance respectively.
Negative alterations in cognitions and mood
The model explained 71.4% of the variance in this construct. Negative affect had a significant direct effect (β = .51) contributing 26.0% of the variance. Anxiety sensitivity had a non-significant direct effect (β = .09), contributing 0.9% of the variance, however via mediation of negative affect (β = .28), it contributed a significant 7.8% of the variance. Intolerance of uncertainty remained non-significant both as a direct effect (β = .02) and via mediation of negative affect (β = .03), contributing 0.04% and .09% of the variance, respectively.
Hyperarousal
The model explained 67.0% of the variance in hyperarousal. Negative affect had a direct effect on hyperarousal (β = .42), contributing 17.5% of the variance. Anxiety sensitivity had non-significant direct effect (β = .08), contributing 0.7% of the variance; however, via mediation of negative affect (β = .23) it contributed a significant 5.3% of the variance. Intolerance of uncertainty remained non-significant as a direct effect (β= .07) contributing 0.5% of the variance, and via mediation of negative affect (β = .12) where it contributed an additional 1.2% of the variance.
Anxiety Sensitivity Extended Model
The sample covariances of the Anxiety Sensitivity Extended Model were well replicated and had adequate fit (SRMR = .06, RMSEA = .07, CFI = .85). As shown in Figure 2, each observed indicator was highly associated with the respective latent variable. Although not shown, the latent variables of the PTSD symptom clusters were significantly related to one another (rs = 0.41–0.73, p < 0.001). Likewise, although not shown and accounting for the influence of negative affect, the cognitive and physical (r = 0.67, p < 0.001), cognitive and social (r = 0.54, p < 0.001), and physical and social (r = 0.56, p < 0.001) concerns sub-factors of anxiety sensitivity were all significantly related to each other.
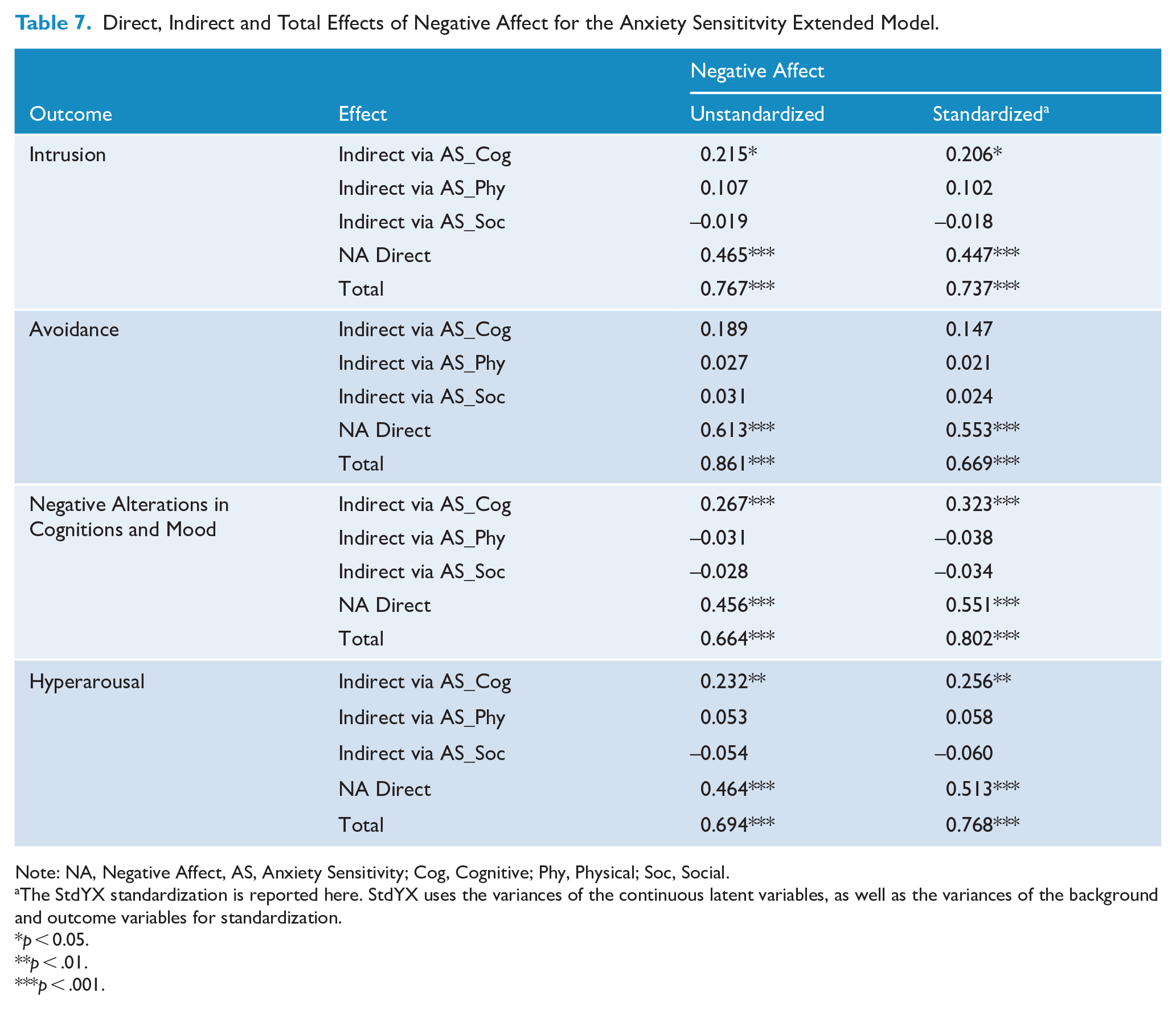
Table 6 shows the direct effects of each factor within the Anxiety Sensitivity Extended Model, as well as the associations among the predictive factors within the model. Table 7 shows the results for the mediation analyses of negative affect. Negative affect showed strong associations with the cognitive (R2 = 49.3%), physical (R2 = 35.4%) and social (R2 = 43.6%) concerns of anxiety sensitivity. Negative affect also showed direct associations with all latent PTSD symptom constructs in this model. Percentage of variance explained (R2) for the latent constructs ranged from .35 to .72 with all ps < 0.001.
Standardized Direct Regression Coefficients for the Anxiety Sensitivity Extended Model.
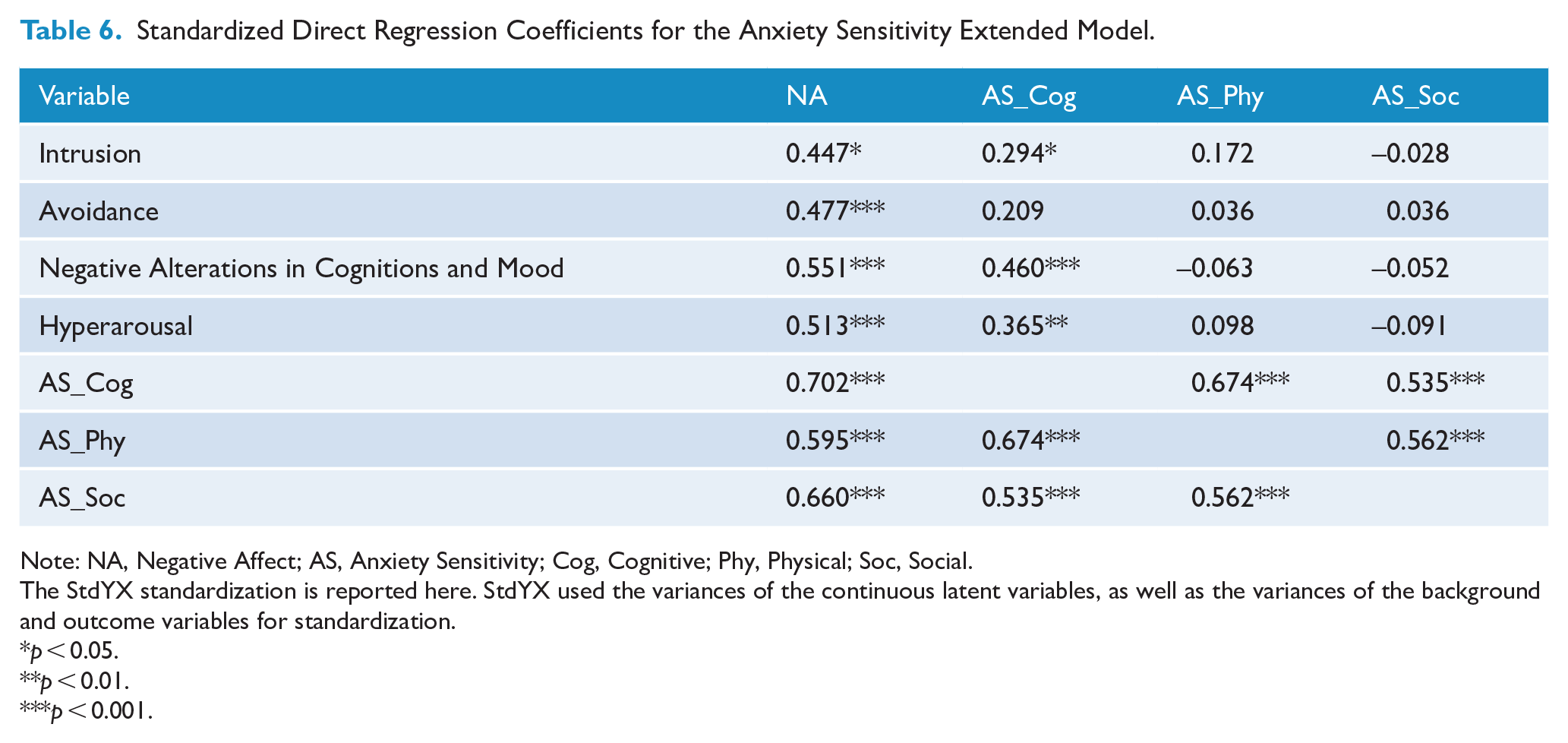
Note: NA, Negative Affect; AS, Anxiety Sensitivity; Cog, Cognitive; Phy, Physical; Soc, Social.
The StdYX standardization is reported here. StdYX used the variances of the continuous latent variables, as well as the variances of the background and outcome variables for standardization.
p < 0.05.
p < 0.01.
p < 0.001.
Direct, Indirect and Total Effects of Negative Affect for the Anxiety Sensititvity Extended Model.
Note: NA, Negative Affect, AS, Anxiety Sensitivity; Cog, Cognitive; Phy, Physical; Soc, Social.
The StdYX standardization is reported here. StdYX uses the variances of the continuous latent variables, as well as the variances of the background and outcome variables for standardization.
p < 0.05.
p < .01.
p < .001.
Intrusion
The model explained 63.8% of the variability in intrusion. Negative affect had a direct effect on intrusion (β = .45), which accounted for 19.9% of the variance. Cognitive concerns had a non-significant direct effect on intrusion (β = .08), contributing. In all, 8% of the variance. Its role as a mediator was significant though, contributing an additional 4.2% via mediation of negative affect (β = .21). Physical concerns was non-significant as either a direct effect (β = .07) or via mediation of negative affect (β = .27), contributing 0.5% and 1.0% of the variance, respectively. Likewise, social concerns was non-significant as either a direct effect (β = -.01) or via mediation of negative affect (β = -.018), contributing 0.01% and 0.03% of the variance respectively.
Avoidance
The model explained 48.3% of the variability in avoidance. Negative affect had a direct effect on avoidance (β = .47) contributing 22.8% of the variance. Cognitive concerns had a non-significant direct effect on avoidance (β = .06), contributing .04% of the variance. Likewise, its role as a mediator was non-significant, contributing an additional 2.2% via mediation of negative affect (β = -.15). Again, physical concerns was non-significant either as a direct effect (β = .02) or via mediation of negative affect (β = .02), contributing 0.02% and 0.04% of the variance respectively. Likewise, social concerns was also non-significant either as a direct effect (β = .01) or via mediation of negative affect (β = .02), contributing 0.01% and 0.06% of the variance respectively
Negative alterations in cognitions and mood
The model explained 72.0% of the variance in this construct. Negative affect had a significant direct effect (β = .55) contributing 30.4% of the variance. Cognitive concerns had a non-significant direct effect (β = .14), contributing 1.9% of the variance. Its role as a mediator was significant though, contributing an additional 10.4% via mediation of negative affect (β = .32). Physical concerns was non-significant either as a direct effect (β = -.03) or via mediation of negative affect (β = -.034), contributing 0.08% and 0.1% of the variance respectively. Likewise, social concerns was non-significant either as a direct effect (β = -.02) or via mediation of negative affect (β = -.03), contributing 0.03% and 0.1% of the variance respectively.
Hyperarousal
The model explained 67.1% of the variance in hyperarousal. Negative affect had a direct effect on hyperarousal (β = .51), contributing 26.3% of the variance. Cognitive concerns had a non-significant direct effect (β = .04), contributing 1.2% of the variance. Its role as a mediator was significant though, contributing an additional 6.6% via mediation of negative affect (β = .26). Physical concerns had a non-significant direct effect (β = .04) contributing just 0.2% of the variance. In its role of mediating negative affect (β = .06), it was also non-significant, contributing 0.3% of the variance. Likewise, social concerns was non-significant either as a direct effect (β = -.03) or via mediation of negative affect (β = -.06), contributing just 0.09% and 0.4% of the variance respectively.
Discussion
This study aimed to investigate how a hierarchical Original Model comprising negative affect, anxiety sensitivity and intolerance of uncertainty, and a hierarchical Anxiety Sensitivity Extended Model comprising negative affect and the three sub-factors of anxiety sensitivity fit upon DSM-5 PTSD symptom clusters within a sub-clinical ADF veteran population. Both the hierarchical Original and Anxiety Sensitivity Extended models converged onto the PTSD symptom clusters, with partial support provided to each of the three hypotheses. Negative affect showed large direct effects upon the PTSD symptom clusters in both models. Greater negative affect was associated with greater symptom severity. Negative affect showed the strongest relationships to hyperarousal and negative alterations in cognitions and mood in both models. This is in line with previous research by Kreminski et al. (2021) and Byllesby et al. (2016), who also showed stronger loadings of negative affect upon these symptom clusters. This effect can be explained by these symptoms being more closely aligned to common distress, which negative affect contends to measure, as compared to a purely traumatic response (Byllesby et al., 2016).
Unlike Oglesby et al. (2017) or Raines et al. (2019), but replicating the results of Kreminski et al. (2021), intolerance of uncertainty showed no relationship to any of the PTSD symptom clusters. The analytical approach by both Kreminski and colleagues and the current study, specifying a theoretically driven relationship between the transdiagnostic factors, may explain this lack of effect by intolerance of uncertainty. Specifically, the deeper personality-like trait of negative affect appears to have accounted for the variance otherwise explained by the secondary cognitive and future-focused trait of intolerance of uncertainty in models lacking negative affect.
Within the Original Model, the effects of negative affect upon the PTSD symptom clusters, with the exception of avoidance, was consistently partially mediated by anxiety sensitivity. This is largely in line with previous research (Cobb et al., 2017; Kreminski et al., 2021; Marshall et al., 2010). The consistent lack of direct effects by anxiety sensitivity upon any of the PTSD symptom clusters was unexpected; however, it is noted that the direct effects for anxiety sensitivity upon the PTSD symptom clusters of intrusion and avoidance in Kreminski et al. (2021) were also quite small at 1.7% and 1.4%, respectively. Regardless, the general replication of the results of Kreminski and colleagues within a sub-clinical population, provides support to the addition of PTSD to the original Norton and Mehta (2007) and Paulus et al. (2015) model.
Within the Anxiety Sensitivity Extended Model, only the cognitive concerns sub-factor of anxiety sensitivity showed any effect in the model, with both physical concerns and social concerns remaining entirely non-significant as either mediators or direct effects. Cognitive concerns, again with the exception of the avoidance construct, consistently partially mediated the effects of negative affect upon the PTSD symptom clusters, though it remained non-significant as a direct effect. The effects of cognitive concerns are largely in line with previous research (Farris et al., 2016; Raines et al., 2017b), and are supportive of Raines and colleagues theory that individuals who are troubled by their cognitive symptoms would experience heightened distress (e.g. the sensation of losing control or going crazy) when experiencing PTSD symptoms, which may affect the individuals’ emotional and behavioral response to their trauma. This may end up developing into a positive feedback loop, with cognitive concerns and PTSD symptoms both increasing over time.
An individual who is temperamentally averse to experience either the physical, social or cognitive symptoms of anxiety would be expected to avoid any cue which could trigger these anxious symptoms (Cobb et al., 2017; Raines et al., 2017b). However, here we did not find any effect of anxiety sensitivity or the cognitive concerns sub-factor upon the avoidance symptom cluster. Notably, similar results were seen in Kreminski et al. (2021), as well as previous research in both military and general populations (Lebeaut et al., 2021; Raines et al., 2017b) suggesting the results of this current study are not idiosyncratic to ADF veterans. The reason for this lack of empirical association between anxiety sensitivity and avoidance symptoms is unclear. A potential explanation for these findings may be found in the wider transdiagnostic literature, where a parallel finding has been shown between anxiety sensitivity and the avoidance behavior of alcohol abuse (DeMartini and Carey, 2011). Here, although anxiety sensitivity has a strong positive association with alcohol abuse, this relationship is usually partially or even fully mediated by other elements (e.g. drinking motives). If such a mediation also occurs between anxiety sensitivity and PTSD-related avoidance, the direct effect may not be significant, even in the absence of the mediators in the model. Future research may wish to test potential mediating variables to better understand the relationship between anxiety sensitivity/ cognitive concerns and the DSM-5 PTSD avoidance symptom cluster.
The current data suggest interventions focused upon reducing an individual’s anxiety sensitivity (especially cognitive concerns) and negative affect may benefit PTSD symptomatology. Although existing PTSD interventions have been shown to reduce individuals’ levels of anxiety sensitivity (Gutner et al., 2013), identified issues with these interventions (e.g. high drop-out rates) suggest the need for other treatment modalities to be utilized in the treatment of PTSD (Sciarrino et al., 2020). The cognitive anxiety sensitivity treatment protocol is efficacious in the reduction of anxiety sensitivity cognitive concerns sub-factor and in anxiety sensitivity as a whole (Schmidt et al., 2014). Furthermore, this intervention has been shown to directly reduce PTSD symptoms, and this effect is specifically mediated through declines in the cognitive concerns sub-factor (Mitchell et al., 2014). For the treatment of negative affect, the transdiagnostic group cognitive behavioral therapy protocol (Norton, 2012) has also shown potential in the reduction of symptom severity in a veteran sample with diagnoses of PTSD, anxiety disorders, and/or obsessive-compulsive disorder (Espejo et al., 2016). Noting ADF veterans high comorbidity, there is an identified need to develop treatment programs that specifically address this comorbidity, as opposed to focusing on any one mental health disorder in isolation (Van Hooff et al., 2018). So as to test the potential clinical implications of the current paper, namely the apparent dominance of negative affect upon PTSD symptoms, future studies may wish to directly compare the efficacy of these two transdiagnostic interventions upon PTSD symptoms within ADF veterans.
This study had some limitations worth noting. Although there is a strong relationship between PTSD, alcohol and substance abuse (Vujanovic et al., 2018), data on these or other potential covariates (e.g. depression) was not collected within the current study. The participants overwhelmingly identified as male (82.8%) which may impact generalizability of the findings to other genders. Furthermore, although 61% of participants scored above the suggested clinical cut-off for a provisional PTSD diagnosis, we were unable to determine if the results hold in that subset of individuals, as the models were not stable with the reduced sample size. By having participants required to respond to each question within the survey, this may have led higher withdrawal rates. Finally, although structural equation modeling can identify directionality between variables (Muthen and Muthen, 2012), it is debatable whether this statistical technique is sufficient to infer causality. To rectify these identified limitations, future studies should (1) seek to investigate the effect of established covariates upon either models, (2) aim for a more representative gender balance, (3) utilize formal assessment tools to ensure all participants meet formal criteria for a PTSD diagnosis, (4) allow participants to skip questions they may feel uncomfortable answering, and (5) as seen in Cobb et al. (2017), potentially investigate the causal effects of the identified transdiagnostic factors upon the development of PTSD symptoms.
In conclusion, this study found the transdiagnostic factors of negative affect and anxiety sensitivity explain a significant amount of variability in all DSM-5 PTSD symptoms cluster, largely replicating the results of Kreminski et al. (2021) within a ADF veteran population. Extending the findings even further, the analyses show the cognitive concerns subcomponent is the driving factor underlying the effect of anxiety sensitivity. The predominance of negative affect and the mediating role of anxiety sensitivity within both models is similar to results found for other anxiety and depressive disorders. Overall, these results suggest interventions targeting those transdiagnostic factors may be useful additions to the cognitive-behavioral interventions currently available for PTSD.
Footnotes
Author Note
This material is the result of work supported with resources and the use of facilities at Monash University, Clayton, Victoria, Australia. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of Monash University.
Author’s contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Michael Kreminski. The first draft of the manuscript was written by Michael Kreminski and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Partial funding support was received from Monash University.
Ethics approval
This study was performed in line with the principles of the declaration of Helsinki, with both the Departments of Defense and Veterans’ Affairs Human Research Ethics Committee (DDVAHREC; Protocol 207-20) and the Monash University Human Research Ethics Committee (MUHREC; Protocol 27639) approving all procedures for this study).
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publication
Not applicable.
Availability of data and material
The datasets generated during and analyzed during the current study are available from the corresponding author upon reasonable request.
Code availability
Not applicable.