
Abstract
Objective
Alexithymia is characterized by difficulty identifying and/or describing emotions, reduced imaginal processes, and externally oriented thinking. High levels of alexithymia may increase the challenge of supporting individuals with co-occurring depression and hazardous alcohol use. This secondary analysis sought to investigate whether or not alexithymia moderated the outcomes of an online intervention for depression and alcohol use.
Method
As part of a randomized controlled trial, 988 participants were randomly assigned to receive an intervention dually focused on depression and alcohol use, or an intervention only focused on depression. The pre-specified mediation hypothesis was that changes in drinking at 3 months follow-up would effect the association between the intervention and change in depression at 6 months. This secondary analysis extends the investigation by adding alexithymia as a moderator.
Results
The current analysis demonstrated that including alexithymia as a moderator resulted in a conditional direct effect. Specifically, there was an intervention effect where participants who received the combined depression and alcohol intervention had larger improvements in their depression scores at 6 months, but this was only when their alexithymia score at baseline was also high (60.5 or higher).
Conclusion
These results suggest that treatment planning and intervention effectiveness could be informed and optimized by taking alexithymia severity into consideration. This is especially merited as alexithymia can contribute to the weaker therapeutic alliance, more distress and dysphoria, shorter periods of abstinence, and more severe depression, compounding the complexity of supporting individuals with comorbid conditions. More research is needed to systematically investigate these possible modifying effects.
Plain Language Title
Does difficulty identifying/describing emotions or externally-oriented thinking influence the effectiveness of an intervention among people with both depression and hazardous alcohol use?
Plain Language Summary
In a recent study we recruited participants who were concerned with both their alcohol use and low mood. We provided two different online interventions. Half of the participants received an intervention designed for both concerns and half received an intervention that addressed only depression. We hypothesized that receiving the combined intervention for both concerns would result in greater benefits, however, our results indicated no apparent difference. This analysis uses the same data, but investigated the influences of alexithymia on the effectiveness of the interventions. Alexithymia is defined as having difficulty identifying/describing emotions and/or thinking more about external events than internal feelings. It commonly co-occurs with depression and with hazardous alcohol use and can increase the challenge of supporting individuals with these co-occurring concerns. The results of this analysis showed support for our original hypothesis that participants who received the intervention that addressed both their mood and alcohol concerns had lower depression scores 6-months later, but only among individuals who also had alexithymia scores above 60.5. Taking alexithymia severity into consideration during treatment planning may help optimize the effectiveness of interventions. These results show merit for future research to consider alexithymia as a variable that could potentially impact outcomes among individuals with co-occurring depression and hazardous alcohol use.
Introduction
Depression and hazardous alcohol use are significant contributors to preventable disease burden1,2 and often co-occur,3,4 yet supporting individuals with comorbid concerns can be challenging due to shared symptoms, denial of substance use harms, and/or concerns related to legal consequences. 4 Nonetheless, the importance of identifying these co-occurring concerns is clear given their association with greater symptom severity, more negative health consequences, an increased risk of complications, and an increased risk of relapse.3–7
While there are well-established, evidence-based treatments to effectively address depression and hazardous alcohol use independently, 3 it is less clear which model is optimal for co-occurring conditions.3,4 One consideration is whether treatments should be single- or dual-focused. Single-focused approaches commonly assume that addressing either condition will result in positive improvements in the other. 3 In contrast, dual-focused approaches assume that addressing both conditions will result in greater improvements. 3 Dual-focused approaches may: (a) address one concern and then the other (i.e., sequential); (b) address both concerns independently, but at the same time (i.e., parallel); or (c) address both concerns simultaneously with equal weight given to each condition and their interactions (i.e., integrated).3,8 Most international guidelines recommend an integrated approach.3,4
Although there is some evidence that empirically supports the integrated model for depression and alcohol use, research proving it is the optimal approach remains in its early stages. Whether delivered in-person or through an online program, relatively few reviews have compared outcomes and these have reported mixed results.3,4 Focusing on interventions administered over the Internet, one systematic review and meta-analysis of 6 studies evaluating the efficacy of different digital interventions reported positive effects with reductions in depressive symptoms at 3 months and in alcohol use at 6-month follow-ups, respectively, compared to control conditions. This analysis was limited by some small sample sizes, high risk of bias, and clinical heterogeneity of population characteristics and interventions. 9 Conversely, other systematic reviews have reported limited or no evidence of superiority between models.3,7 These reviews note, however, that methodological and sample differences make comparisons between studies difficult.7,10
Our recent randomized controlled trial (RCT) of an online intervention for individuals experiencing depression and hazardous alcohol use demonstrated no apparent benefit to providing a dual-focused program over a single-focused version that addressed depression alone. 11 Of specific interest to this paper, we also found no evidence supporting the pre-specified mediation hypothesis that compared to the single-focused intervention, the dual approach would result in greater changes in alcohol use at 3 months follow-up, which would have an indirect effect and result in greater change in depression at 6 months. 11 This null result led to the current secondary analysis investigating the potential moderating effect of alexithymia.
Alexithymia is characterized by difficulty identifying and/or describing emotions, distinguishing between bodily sensations related to emotional arousal, reduced imaginal processes, and an externally oriented thinking style 12 (i.e., a preference for thinking about external details rather than feelings, fantasies, or other internal aspects of life). 13 Alexithymia has been theorized to interfere with emotional regulation 14 (i.e., the ability to influence the type, timing, and expression of emotions),15,16 and lead to the use of less adaptive coping strategies.14,16,17 Alexithymia has been implicated in the development, maintenance, and recovery from both hazardous alcohol use14,17,18 and depression.10,18–20 Furthermore, among other factors, alexithymia has been theorized to play a role in the heterogeneity of depression and alcohol use disorder by contributing to different affective functioning between individuals.10,15,16
There are several reasons to be interested in the potential influence of alexithymia. With respect to substance use, higher levels of alexithymia tend to correlate with: more distress and dysphoria, attendance at fewer treatment sessions, weaker therapeutic alliances, and generally worse treatment outcomes.14,21 For alcohol use in particular, alexithymia has been associated with increased obsessive thoughts and compulsive urges to drink, 21 and predicts shorter periods of abstinence.19,22 Likewise, higher levels of alexithymia are correlated with more severe depression10,16 and psychiatric symptoms 10 and are thought to influence therapy outcomes 23 and interfere with recovery.10,19
The current secondary analysis was designed to be hypothesis generating, but was guided by the research question: Does alexithymia moderate the direct and indirect associations proposed in the original mediation model? Specifically, this investigation was interested in determining if the dual-focused intervention (MoodGYM + Check Your Drinking [CYD]) was associated with greater decreases in depression scores among participants with higher alexithymia scores compared to participants who received the single-focused intervention (MoodGYM) This hypothesis is based on the strong associations documented in the literature between alexithymia and both depression and alcohol use. The conceptual model of the relationships predicted in the original hypothesis is displayed in Figure 1 and shows the proposed addition of alexithymia as a moderator (dashed arrows).
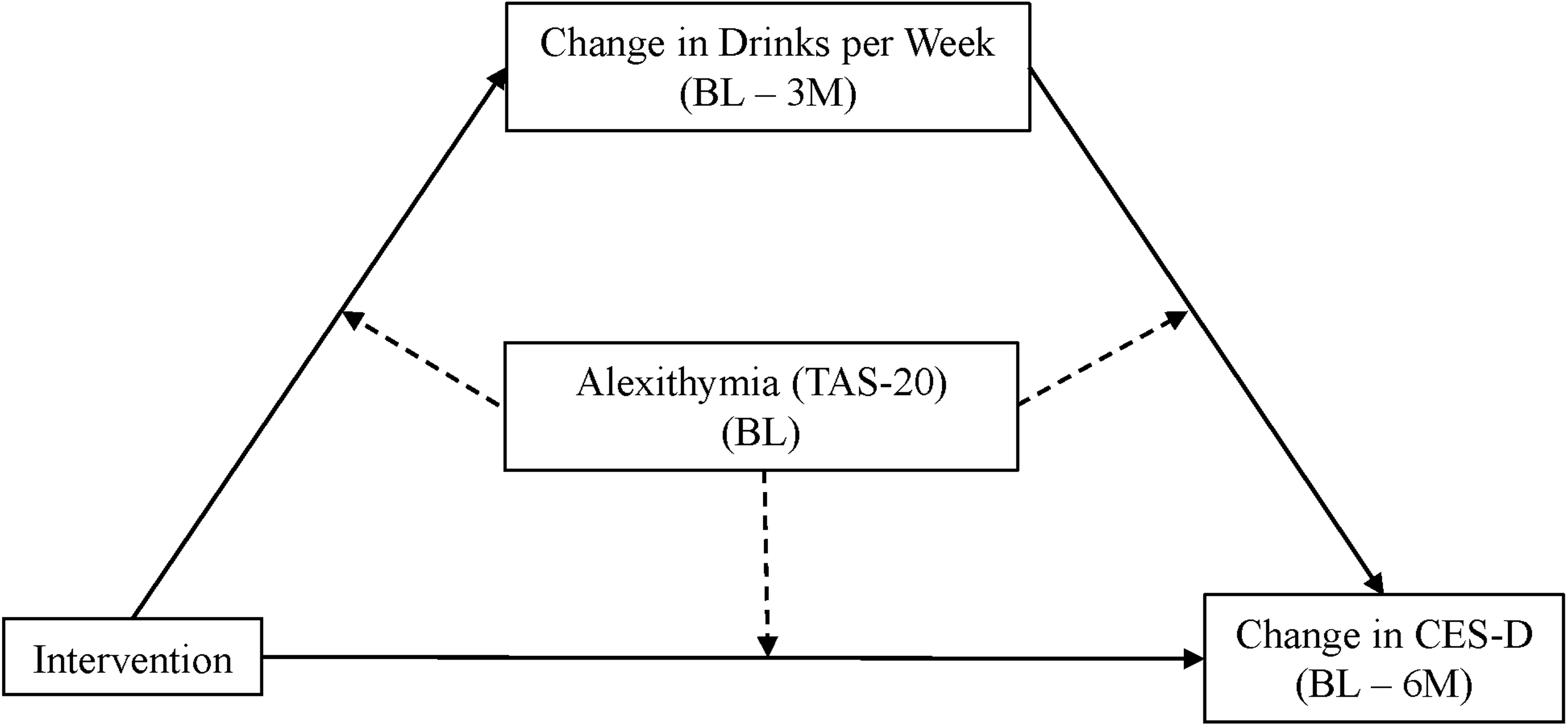
Conceptual model.
Methods
Randomized Controlled Trial
Adults (18 years or older) with self-reported persistent low mood (Patient Health Questionnaire-9 (PHQ-9) 24 >9) and hazardous alcohol use (Alcohol Use Disorders Identification Test (AUDIT) 25 >7) were recruited between April 2018 and July 2020 from across Canada using online advertisements. Half of the 988 participants were randomized to receive MoodGYM, an established, online intervention for mood disorders (MoodGYM – only) 26 while the other half were provided with MoodGYM combined with CYD, a brief, personalized feedback report outlining the participant's current alcohol use and severity of hazardous drinking (MoodGYM + CYD). 27 Follow-up interviews were conducted 3 and 6 months following the baseline interview and completion rates were high at 84.9% and 86.4%, respectively.
The RCT protocol was approved by the Centre for Addiction and Mental Health's research ethics board (approval no. 064/2017) and informed consent to participate was obtained electronically from all participants prior to beginning the baseline interview.
Alexithymia
During the baseline interview, participants completed the Toronto Alexithymia Scale-20 (TAS-20). The TAS-20 has demonstrated good internal consistency, strong support for convergent and concurrent validity, modest discriminant validity and good-to-excellent reliability.12,13,21,28,29 The TAS-20 consists of 20 items rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). 12 Responses are combined to create a total score with higher totals indicating greater degrees of alexithymia (range 20–100). 12 The TAS-20 can also be divided into 3 subscales: Difficulty Identifying Feelings (range 7–35), Difficulty Describing Feelings (range 5–25), and Externally Oriented Thinking (range 8–40).10,12,21 This 3-factor structure has been replicated in both clinical and nonclinical samples. 13 In the current sample, the total TAS-20 scale had a Cronbach's α-coefficient = 0.84 and omega (ω) = 0.83. This is similar to internal consistency scores published elsewhere in the literature.13,29
Analysis Plan
Independent t-tests were used to determine if there were any significant differences in total alexithymia scores among different demographic groups. Pearson correlations were conducted to examine any bivariate correlations between alexithymia and clinical measures of depression and alcohol use.
A mediation analysis was conducted and reported previously 11 as part of the pre-specified study hypotheses (see Figure 1, solid lines). Briefly, the analysis tested whether participants who received the intervention (i.e., MH + CYD) reported larger changes in depression scores between baseline interviews and 6-month follow-up (outcome) compared to the control group (i.e., MH only). It also examined whether the intervention was associated with a greater reduction in the number of drinks consumed per week at a 3-month follow-up (mediator) and whether this reduction in drinking was associated with larger changes in depression scores when controlling for which intervention was received. Finally, the analysis assessed whether reductions in the number of drinks at 3 months strengthened the association between the intervention and depression outcome (i.e., mediation). Of the associations tested only the relationship between changes in drinking and depression was significant. That is, independent of the intervention received, participants who reported consuming fewer drinks at 3 months were more likely to report lower depression scores at 6 months (P < 0.001).
This analysis builds on the previously reported mediation by adding alexithymia as a moderating variable. This will determine if alexithymia modifies the associations described above (i.e., moderation). Hayes’ PROCESS macro version 3.3 for SPSS (model 59) 30 was used to test the moderated mediation model. Missing values were managed using listwise deletion. 30 Associations with p-values <0.1 were further probed and plotted according to the Johnson–Neyman technique31,32 to identify any regions of significance. 30 The values of these regions will indicate where the conditional effect of alexithymia transitioned to being statistically significant. 30 Bias-corrected, 95% boot-strapped confidence intervals (CIs) were calculated with 5,000 iterations. Results were considered significant if the range did not include zero. 33 Similarly, p-values of 0.05 or less were considered significant in evaluating the analyses.
Results
Characteristics at Baseline
A total of 988 participants were enrolled and were randomly assigned to receive either the single- or dual-focused intervention. Sample characteristics are reported in more detail in the primary outcome paper. Briefly, 73.5% of participants were female and the average age was 36.2 years (SD = 13.5). The average AUDIT Consumption subscale score reported at baseline was 6.4 (SD = 2.5) with an average of 15.8 drinks (SD = 14.7) consumed in a typical week. The average depression score, as measured by the Center for Epidemiological Studies Depression Scale (CES-D) was 35.3 (SD = 8.29). The original analysis found no statistically significant demographic differences across intervention groups. 11 The average alexithymia score in the sample was 56.9 (SD = 11.9). A series of independent measure t-tests were conducted to test for significant differences between sample demographic characteristics and alexithymia at baseline. Of these comparisons, there was a significant difference between the intervention groups at baseline with participants receiving the MoodGYM-only intervention reporting higher alexithymia scores at baseline compared to those randomized to receive the MoodGYM + CYD intervention (p = 0.014). Likewise, participants with no post-secondary education reported higher alexithymia scores compared to those with post-secondary schooling.
Small to medium Pearson correlations were found between alexithymia and clinical characteristics of the sample as measured at baseline (Table 1). Depression (CES-D), 34 Generalized Anxiety Disorder-7 (GAD-7), 35 PHQ-9 24 scores, as well as, alcohol-related consequences, 36 the number of drinking motives reported, and the total number of intervention modules completed were positively correlated with alexithymia (i.e., scores increased with higher levels of alexithymia, P < 0.05). Conversely, lower quality of life scores (EUROHIS) 37 and lower age were associated with higher levels of alexithymia (P < 0.05). While the correlations were significant, all were relatively small, however, each correlation was in the expected direction, based on the literature.
Sample Characteristics and Descriptive Analysis of the Full Sample and Alexithymia at Baseline (n = 988).
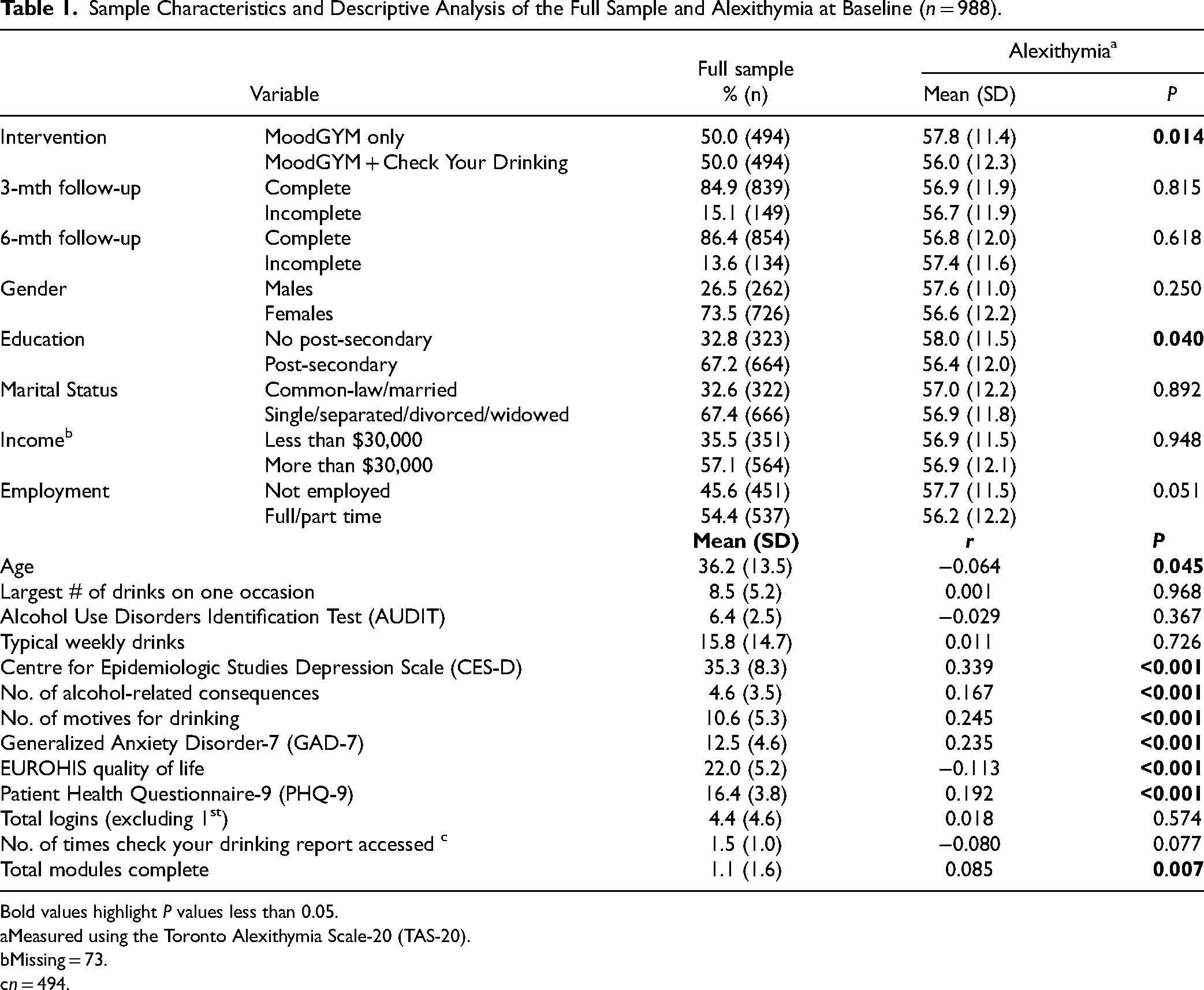
Bold values highlight P values less than 0.05.
Measured using the Toronto Alexithymia Scale-20 (TAS-20).
Missing = 73.
n = 494.
Moderated Mediation
The results of the conditional process model are presented in Table 2. There was a statistically significant direct effect of the intervention, conditional on alexithymia. Participants who received MoodGYM + CYD showed more changes in their depression, when a change in drinks per week was kept constant and when they also scored higher in alexithymia (Coeff. = 0.19, P = 0.004).
Change in Depression From Baseline to 6 Months (CES-D) Mediated by Change in Alcohol Consumption from Baseline to 3 Months (No. of Drinks per Week) Moderated by Alexithymia Scores Measured at Baseline (n = 795).
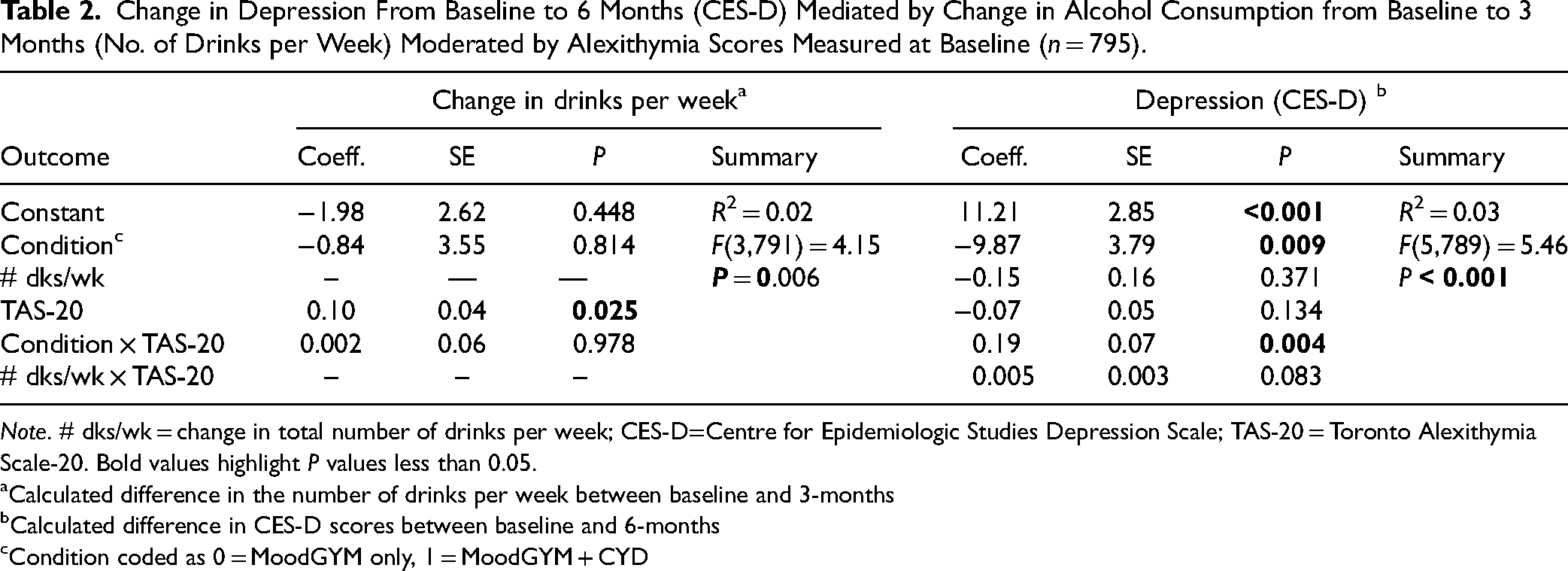
Note. # dks/wk = change in total number of drinks per week; CES-D=Centre for Epidemiologic Studies Depression Scale; TAS-20 = Toronto Alexithymia Scale-20. Bold values highlight P values less than 0.05.
Calculated difference in the number of drinks per week between baseline and 3-months
Calculated difference in CES-D scores between baseline and 6-months
Condition coded as 0 = MoodGYM only, 1 = MoodGYM + CYD
The Johnston–Neyman technique was used to probe any interaction with a p-value <0.1. This revealed that the direct effect was significant when alexithymia scores were below 35.6 (4.7% of the sample, 37 participants) or above 60.5 (41.0% or 326 participants). Figure 2 shows the critical region where these critical alexithymia scores alter the association between the intervention received and depression scores so that MoodGYM + CYD is associated with lower depression scores at 6 months follow-up compared to the MoodGYM-only intervention.
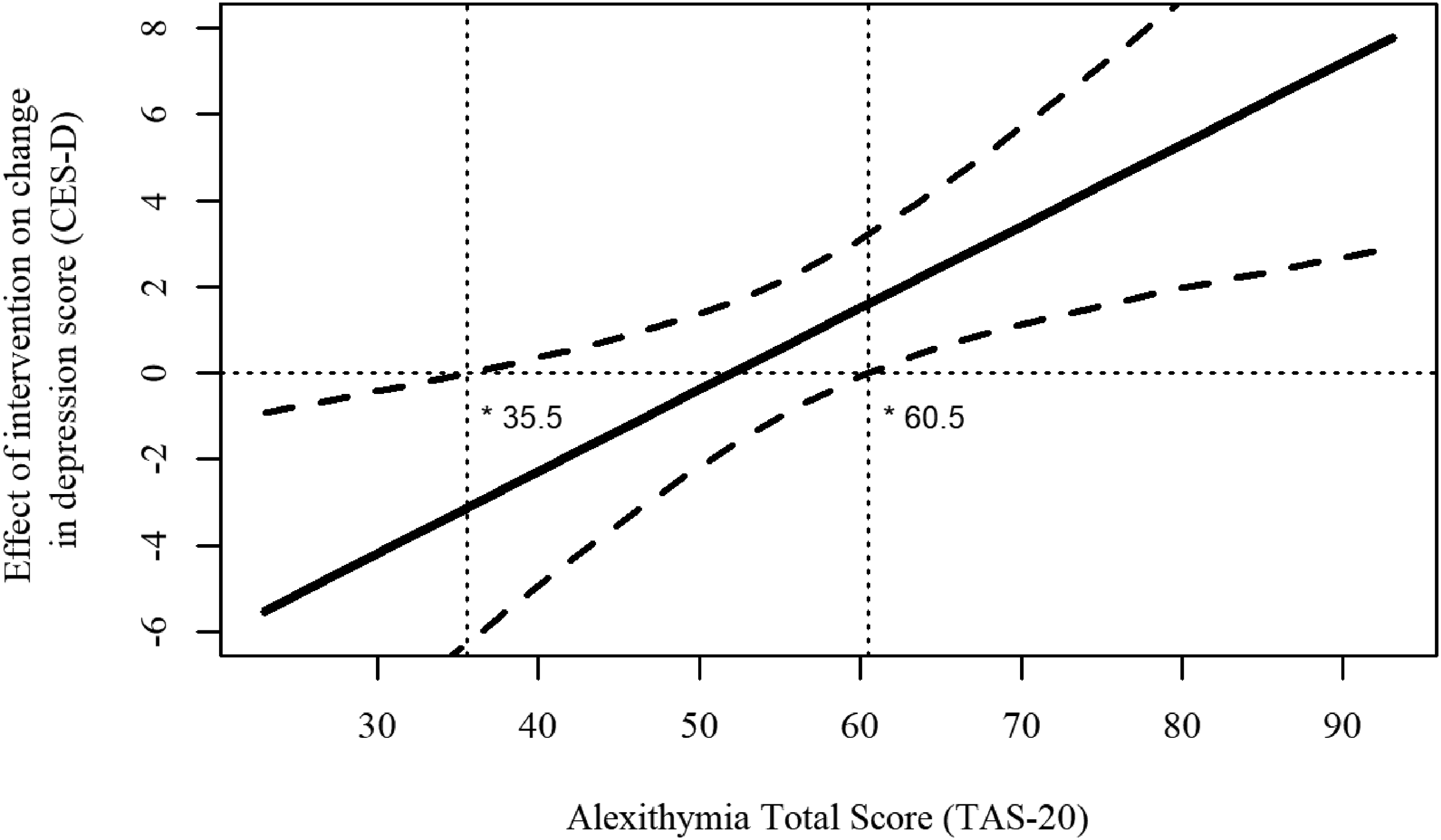
Johnson–Neyman diagrams of model results of the moderator effect of alexithymia on the effect of the intervention on change in depression scores.
Adding alexithymia as a moderator did not support the hypothesized mediation effect related to decreased alcohol consumption at 3 months follow-up. Alexithymia did not have a conditional effect on the relationship between the intervention condition and change in drinks per week or between change in drinks per week and change in depression (P ≥ 0.05). Likewise, the total indirect effect calculated from these partial associations also demonstrated no conditional effect related to the addition of alexithymia to the mediation (95% CIs included zero).
Discussion
Results supported a moderating role of alexithymia implicating the significant direct effect of the dual-focused intervention (MoodGYM + CYD), such that depression scores showed greater improvements at 6-month follow-up compared to the single-focused intervention (MoodGYM). However, this was only the case when alexithymia scores were either below 35.6 or above 60.5. The lower critical value may not be reliable and should be interpreted with caution as only a small percentage of the sample (5%, 32 participants) scored within the lower significance region (compared to 41%, 323 participants for the upper region). Further research using RCTs will need to verify these findings, however, the conditional effect suggests that investigating possible moderating effects of alexithymia is merited.
The use of the baseline measure of alexithymia in a model involving change over time is a potential limitation that needs discussion. First, the baseline measure corresponds with the randomization of treatment conditions. As higher levels of alexithymia can interfere with treatment adherence, the potential conditional effects caused by baseline scores are of importance.10,19,23 Second, there is still debate in the literature as to whether alexithymia should be treated as a state or trait phenomenon. 38 Investigations have demonstrated the absence of absolute stability (i.e., change over time, before and after treatment) and moderate to high relative stability (i.e., relative differences between subjects remain the same over time) for both the total scores and subscales suggesting both state and trait features. 38 If alexithymia is a stable trait then we would expect little change over the course of the study, however, using only the baseline measure is a potential limitation of the analysis and future research should consider including a measure of alexithymia at follow-up in order to monitor change over time.
This analysis has particularly interesting implications for understanding the effectiveness of interventions. In general, alexithymia can increase the challenge of supporting individuals, however, a better understanding of its moderating effects could help improve outcomes. For instance, a sample of individuals with high alexithymia scores and who used substances demonstrated greater improvements with cognitive behavioural therapy compared to group-based approaches. 21 It has been suggested that cognitive strategies may be easier to learn and practice for individuals with high alexithymia compared to interventions that involve sharing feelings with peers or a therapist.19,21 The proposed robustness of behaviourally based interventions may also help explain our finding of greater change when assigned to the dual-focused intervention which included CYD. CYD provides feedback which compares an individual's alcohol use to age and gender-matched peers. 39 Providing this normative data creates an opportunity for the individual to reflect and correct beliefs about how much alcohol their peers consume. 39 previous findings may help to explain why there was a significant treatment effect when alexithymia was included in this analysis, but not in the original outcomes.
Conclusions
There are relatively few studies involving alexithymia that investigate potential moderating effects or that use nonclinical, general-population samples with co-occurring depression and hazardous alcohol use. More work should consider the role of alexithymia in the future as it has been implicated in contributing to the heterogeneity of both depression and alcohol use disorder.10,15,16 Furthermore, the potential moderating effect on treatment could help guide intervention selection and allow more personalized recommendations.
Footnotes
Acknowledgements
John Cunningham is currently supported by the Nat & Loretta Rothschild Chair in Addictions Treatment & Recovery Studies. Support to CAMH for salary and infrastructure has been provided by the Ministry of Health and Long-Term Care.
Author Contributions
All authors have made an intellectual contribution to this research, participated in the manuscript drafting process, and have read, and approved the final manuscript. This is the authors’ original work. It has not been previously published nor is it under consideration for publication elsewhere.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The RCT (PJT-153 324) was funded by a grant from the Canadian Institutes of Health Research. A Canada Research Chair award to John Cunningham provided additional support. The funders did not have input regarding the design of the study, data collection, analysis, interpretation of data or in writing the manuscript.
Compliance,Ethical Standards,and Ethical Approval
The trial was approved by the Centre for Addiction and Mental Health's research ethics board (approval no. 064/2017). Informed consent to participate in the original RCT was obtained electronically prior to the start of the baseline interview. The research was conducted in accordance with the World Medical Association Declaration of Helsinki.