
Abstract
Objectives
This study identified predictors of prompt (1+ outpatient physician consultations/within 30 days), adequate (3+/90 days) and continuous (5+/365 days) follow-up care from general practitioners (GPs) or psychiatrists among patients with an incident mental disorder (MD) episode.
Methods
Study data were extracted from the Quebec Integrated Chronic Disease Surveillance System (QICDSS), which covers 98% of the population eligible for health-care services under the Quebec (Canada) Health Insurance Plan. This observational epidemiological study investigating the QICDSS from 1 April 1997 to 31 March 2020, is based on a 23-year patient cohort including 12+ years old patients with an incident MD episode (n = 2,670,133). Risk ratios were calculated using Robust Poisson regressions to measure patient sociodemographic and clinical characteristics, and prior service use, which predicted patients being more or less likely to receive prompt, adequate, or continuous follow-up care after their last incident MD episode, controlling for previous MD episodes, co-occurring disorders, and years of entry into the cohort.
Results
A minority of patients, and fewer over time, received physician follow-up care after an incident MD episode. Women; patients aged 18-64; with depressive or bipolar disorders, co-occurring MDs–substance-related disorders (SRDs) or physical illnesses; those receiving previous GP follow-up care, especially in family medicine groups; patients with higher prior continuity of GP care; and previous high users of emergency departments were more likely to receive follow-up care. Patients living outside the Montreal metropolitan area; those without prior MDs; patients with anxiety, attention deficit hyperactivity, personality, schizophrenia and other psychotic disorders, or SRDs were less likely to receive follow-up care.
Conclusion
This study shows that vulnerable patients with complex clinical characteristics and those with better previous GP care were more likely to receive prompt, adequate or continuous follow-up care after an incident MD episode. Overall, physician follow-up care should be greatly improved.
Introduction
Receiving prompt (1+ outpatient consultations/within 30 days), adequate (3+/90 days), or continuous (5+/365 days) follow-up physician care after an incident mental disorder (MD) episode, including substance-related disorders (SRDs), is crucial for optimizing patient recovery 1 and a key trend in system reforms.2,3 Such follow-up care may prevent adverse outcomes such as high emergency department (ED) use, 4 hospitalization,5,6 and death. 7 Even a small amount of follow-up care after hospital discharge, when patients are still vulnerable, promotes better access to biopsychosocial specialized 8 or outpatient care,6,7 continuity of care, 8 health outcomes, 9 and treatment compliance.6,10 Still, few studies have evaluated the quality of follow-up care by the number of outpatient consultations received with general practitioners (GPs) or psychiatrists over a 1-year period or close after a patient MD incident episode. Patients first diagnosed with schizophrenia, 11 and those with incident depressive disorders, suicidal behaviours, 12 and chronic physical illnesses 13 are especially in need of close follow-up care. Better knowledge of individual characteristics and prior service use of patients with incident MD episodes who have or have not received prompt, adequate or continuous follow-up care may suggest interventions to improve such care.
Most previous studies have investigated prompt follow-up care within 30 days of patient hospital discharge5,6,14 or after a first schizophrenia or psychotic disorder episode8,15 or new incident depressive disorder episodes, 16 but few have studied follow-up care by comparing different incident MD episodes and integrating adequate follow-up care within 90 days (acute treatments aimed at reducing severe symptoms)14,17 and continuous follow-up care within 365 days14,18 (based on previous benchmarks, treatments aimed at full patient recovery). 14 Roughly 60% of Canadian patients first diagnosed with schizophrenia between 1999 and 2008, 8 and those with a depressive disorder discharged from hospital in 2005–2006 19 received prompt physician follow-up care. A 2000–2004 US study 10 and a 2003–2005 Canadian study 14 showed that, respectively, 31% and 48% of patients initiating antidepressant treatment or affected by an incident depressive disorder received adequate follow-up care. Another 2007–2008 Canadian study found that 52% of patients with depressive disorders received at least one minimally adequate treatment, and that, as reported in related studies,8,14 having a family physician was a key predictor. 20 Men8,14 and older patients 14 were less likely to receive follow-up care within 30 or 90 days, while those having depressive or anxiety disorders or SRDs were less likely to receive follow-up within 30 days, but more likely within 90 days. 14 Patients having antidepressant prescriptions also were more likely to receive physician follow-up care within 90 days. 10
To our knowledge, no previous study has investigated predictors of 30-, 90- and 365-day follow-up care associated with patient characteristics and prior service use of individuals diagnosed with an incident MD episode, including SRDs. Patients with specific sociodemographic characteristics or types of MDs, and those with co-occurring disorders, and better previous GP care may be more likely to receive follow-up care. Few studies have reported data on service use variables that may influence follow-up care. Most longitudinal studies do not cover several years15,16 or control for previous MD treatment episodes. This study reported incident MD episodes among patients over a 23-year period, controlling for prior MD episodes, co-occurring disorders, and years of follow-up care—better knowledge of follow-up care over years and of predictors may help decision makers to improve patient care. This study aimed to identify predictors of prompt (1+ outpatient GP or psychiatrist consultations/30 days), adequate (3+/90 days) or continuous (5+/365 days) physician follow-up care among patients in their last incident MD episode. We hypothesized that the most vulnerable patients with complex clinical characteristics and better prior GP care are more likely to receive prompt, adequate, or continuous follow-up.
Methods
Study Background and Data Sources
The Canadian universal health insurance covers 99% of the population. 21 Data for this study were extracted from the Quebec Integrated Chronic Disease Surveillance System (QICDSS), 22 which covers 98% of the population eligible for health-care services under the Quebec Health Insurance Plan (RAMQ). This included billing documents from physicians working on a fee-for-service basis, 22 which accounts for 80% of total physician remuneration in the public system—only 6% of physician billing occurred outside the public system in 2016--2017. 23 The QICDSS includes the health insurance registry, patient sociodemographic characteristics, the Physician Claims database (diagnoses, consultations, and physician seniority), and the Hospital Inpatient and Day Surgery database (hospitalizations). 22 Diagnostic codes from the Physician Claims and Hospital Inpatient databases were framed by the International Classification of Diseases, Ninth or Tenth Revisions (Appendix 1). The study protocol was approved by a research ethics committee.
Study Design and Sample
This observational epidemiological study investigated a 23-year patient cohort based on data from the QICDSS (1 April 1997 to 31 March 2020). Patients had to be 12+ years old and diagnosed with incident MD episodes, including SRDs. Based on previous research,8,24 incident case required 2 MD diagnoses in the Physician Claims database, or only 1 principal MD diagnosis in the Hospital Inpatient database—except for SRDs, for which only 1 diagnosis was required in databases, as SRDs are underdiagnosed. 25 Any physician could diagnose an MD, with the first MD being reported after a 3-year period without MD, but while considering co-occurring disorders within the same fiscal year. For patients with several incident MD episodes over the 23-year investigation, only the last episode was included, controlling for the number of previous MD episodes and the year of entry into the cohort's final regression model. The cohort included 2,670,133 patients diagnosed with incident MD episodes. Deceased patients and those hospitalized for more than one-third of the 30-, 90- or 365-day follow-up periods were excluded (as outpatient follow-up care was hindered), as well as patients whose data were not available for the entire follow-up period. Medical follow-up care was measured from 1 April 2000 to 31 March 2020—taking into account the 3-year clearance required for case definition of an incident MD episode (1997–2000), which is consistent with the notion of recovery for MDs–SRDs. 26 For patients diagnosed during hospitalization, follow-up care started at discharge. Reporting of the study followed the Strobe guideline for epidemiological studies. 27
Study Variables
The 3 dependent variables were follow-care within a prompt (30-day), adequate (90-day) or continuous (365-day) period, measured after the patient's last incident MD episode. Only outpatient follow-up care provided by GPs or psychiatrists in hospital settings or medical clinics was measured. Prompt follow-up care entailed at least 1 outpatient physician consultation within 30 days; adequate follow-up care, at least 3 within 90 days 17 ; and continuous follow-up care, at least 5 within 365 days. 18 The analytical framework (Figure 1) identified sociodemographic, clinical, and service use independent variables linked to specific databases, with measurement timeframes.
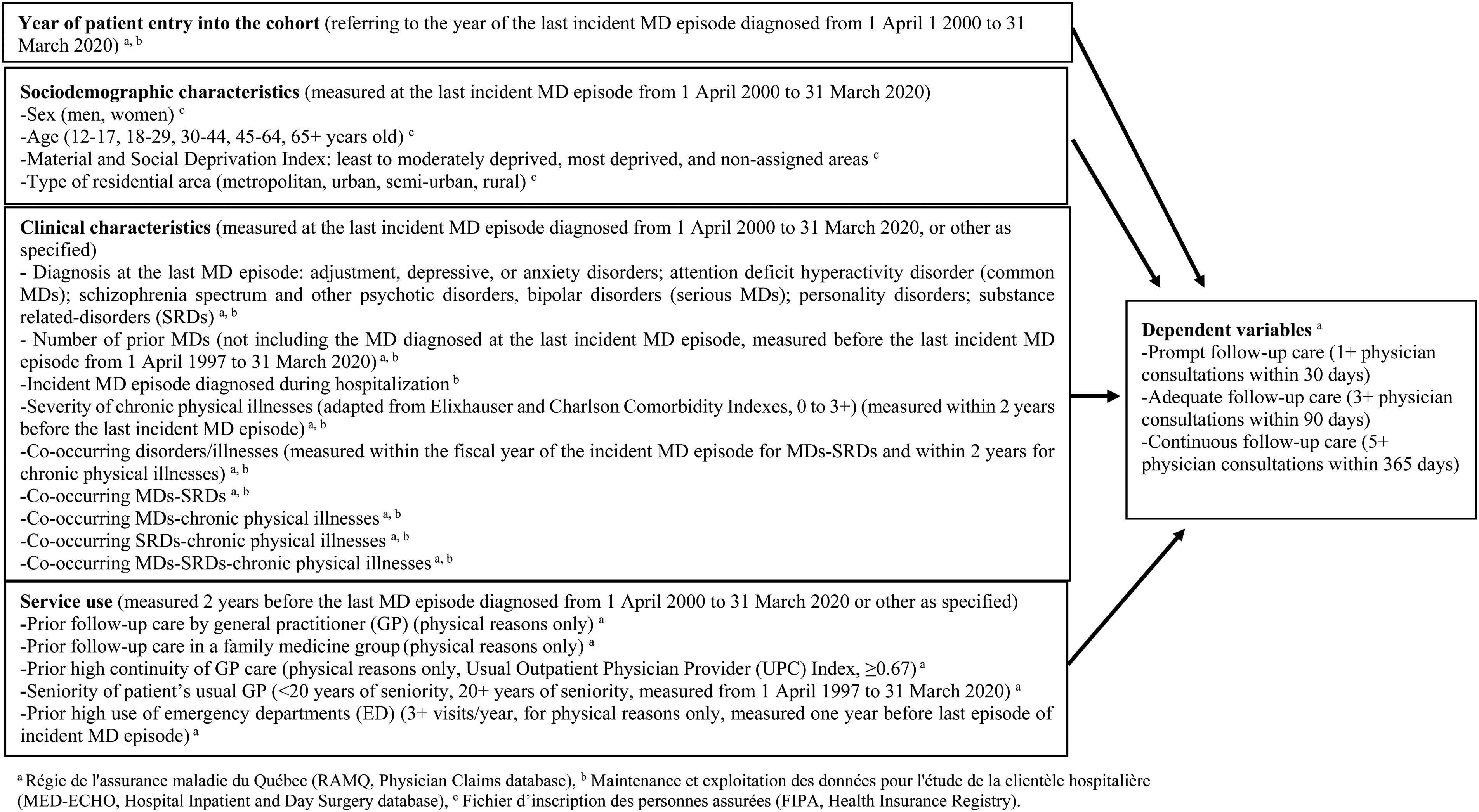
Conceptual framework: predictors of prompt, adequate, and continuous follow-up care among patients affected by an incident mental disorder (MD) episode diagnosed from 1 April 2000 to 31 March, 2020.
Sociodemographic characteristics measured within the last incident MD episode included sex, age, material and social deprivation, and type of residential area (e.g., urban). Material and social deprivation indexes based on the smallest geographic areas delineated in recent versions of the Canadian census were merged into 3 groups: least or moderately deprived, most deprived, and nonassigned areas (e.g., nursing homes where index assignment was not feasible, missing address, and homeless). The Material Deprivation Index measured the ratio of population employment, average income, and the number of individuals without a high school diploma, while the Social Deprivation Index included individuals living alone, single-parent families, and individuals without a spouse.
Clinical characteristics included: last incident MD episode; whether MDs were diagnosed during hospitalization; number of MDs prior to the last episode; co-occurring MDs or SRDs within the fiscal year of the last incident MD episode; and chronic physical illnesses within 2 years. MDs included depressive, anxiety, or adjustment disorders; attention deficit hyperactivity disorder (common MDs); schizophrenia spectrum and other psychotic disorders, bipolar disorders (serious MDs); personality disorders; SRDs (alcohol or drug use, induced disorders, intoxication, or withdrawal). MD diagnosed during hospitalization was a proxy for patient illness severity needing more intensive follow-up care. 5 Chronic physical illnesses (e.g., diabetes) were assigned a 0–3 severity score, as adapted from the Elixhauser and Charlson Comorbidity Indexes. 28
Service use variables included prior usual GP follow-up care, especially in family medicine groups, and prior high continuity of GP care measured 2 years before the last incident MD episode. The patient's usual GP seniority (measured from 1 April 1997 to 31 March 2020) and prior high use of EDs (measured 12 months before the last incident MD episode) were also assessed. Prior usual GP consultations and ED use were considered for physical reasons only. To be designated as the patient's usual GP, a proxy for family physician, at least 2 consultations with the same GP or with a GP in the same family medicine group were required. Family medicine groups are clinics with patient registration that include GP working with psychosocial clinicians such as nurses and social workers, who deliver extended medical coverage. 29 Continuity of physician care was measured with the Usual Provider Continuity Index, 30 with scores ≥0.67 indicating high continuity of care. 31 This index describes the proportion of consultations with the usual GP (the most frequently used GP) out of all GPs consulted in outpatient care, including walk-in clinics. The 20-year benchmark for GP seniority was based on a 50% distribution of GP seniority in the database. High ED use referred to a minimum of 3+ ED visits per year.32,33 Studies report that high ED users are often patients without adequate follow-up care, 34 and that ED care is one of the costliest options. 35
Data Analysis
Descriptive analyses followed by multivariate regressions were produced to test associations between each independent variable and the 3 dependent variables—prompt (1+ outpatient physician consultations within 30 days), adequate (3+/90 days), or continuous (5+/365 days) follow-up care after the last incident MD episode. Independent variables without collinearity and with an alpha value of p < 0.01 were entered in the multivariate models. Risk ratios were calculated using robust Poisson regressions 36 to measure patient characteristics and their previous service use associated with the risk of receiving prompt, adequate, or continuous follow-up care. Risk ratios were calculated with a 99% confidence interval. All analyses were performed using SAS Enterprise Guide version 7.15.
Results
Of the 2,670,133 patients who got prompt follow-up care, 38,206 (1%) died, 51,717 (2%) were hospitalized for more than one-third of the follow-up period, and 504 (0.02%) were excluded because patient data were not available. For patients who got adequate follow-up care, the numbers were 56,265 (2%), 35,001 (1%), and 1,433 (0.05%), respectively. Respective numbers for continuous follow-up care were 110,533 (4%), 8,534 (0.3%), and 8,309. After these exclusions, the final cohorts for prompt, adequate, or continuous follow-up care included 2,579,706, 2,577,434, and 2,542,757 patients, respectively (Appendix 2). From 1 April 2000 to 31 March 2020, the cohort increased by 4% to 7% each year. During this period, the percentage of patients receiving prompt follow-up care decreased from 45% to 33%, adequate follow-up care from 44% to 33%, and continuous follow-up care from 58% to 43% (Figure 2). More than 90% of follow-up care was provided by GPs.
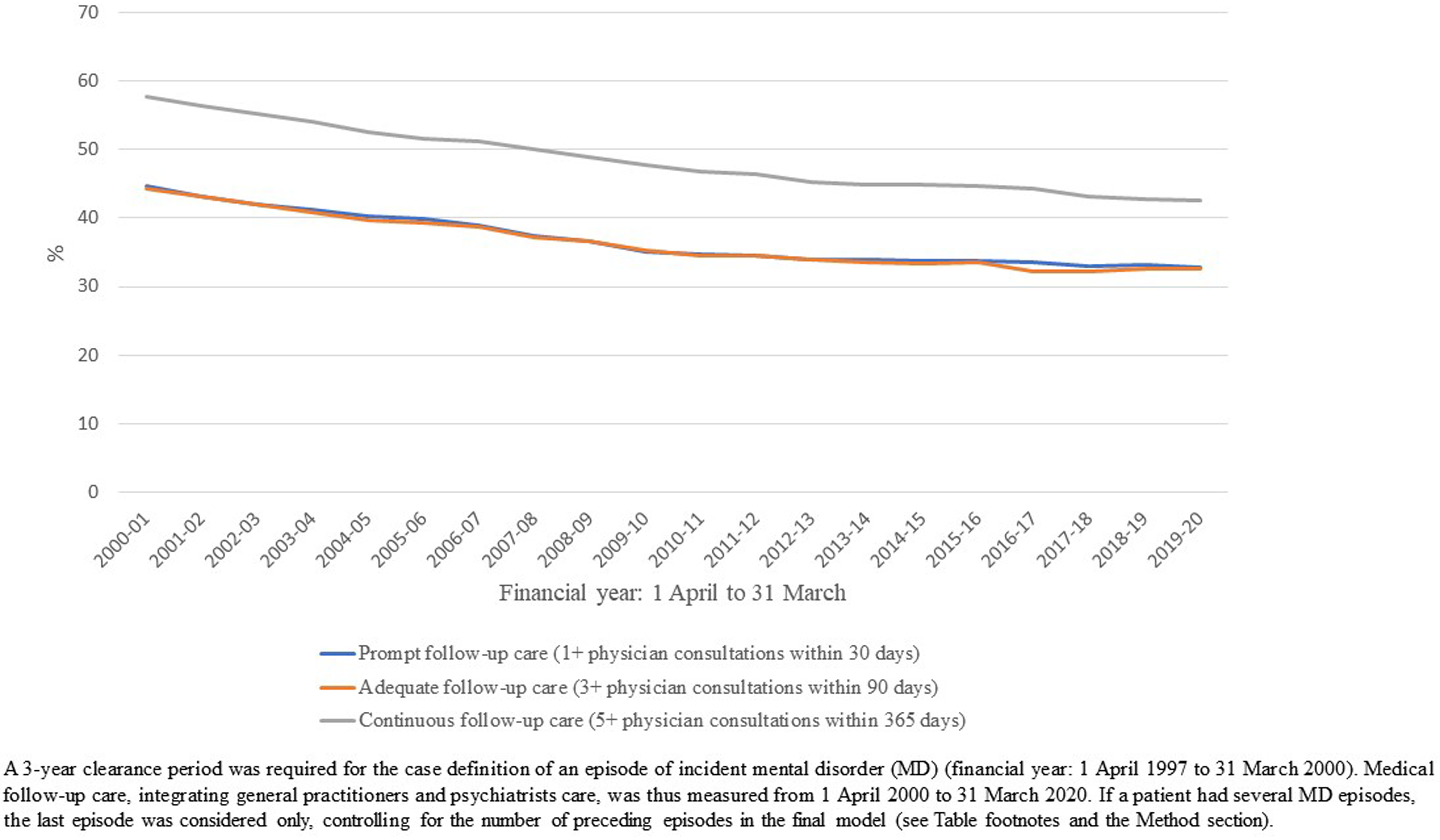
Percentage of patients receiving medical follow-up care per year (N = 2,670,133).
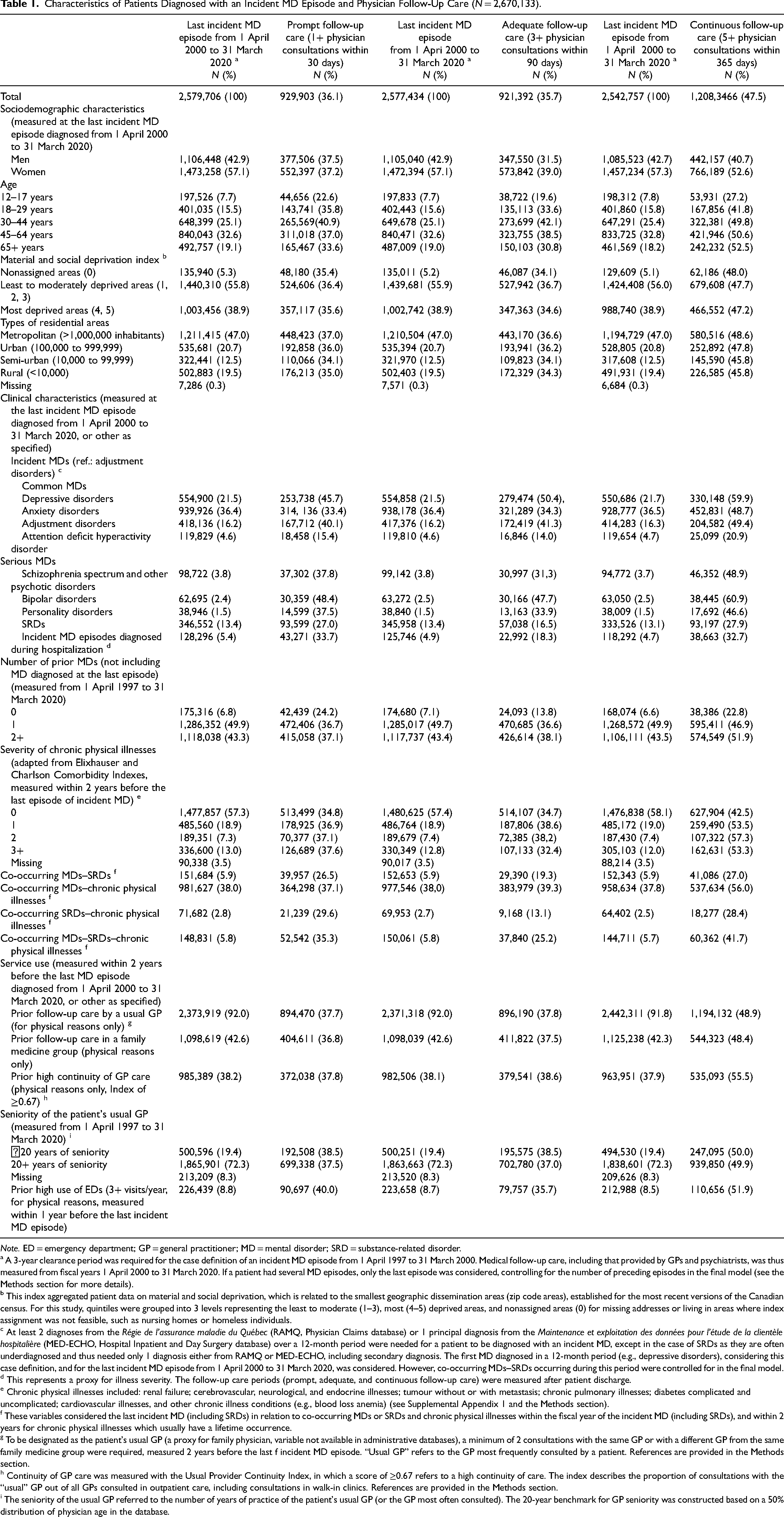
Of these patients, 57% were women, and 33% were aged 45 to 64 years; 56% lived in the least to moderate deprived areas and 47% in the Montreal metropolitan area (Table 1). Most patients (79%) had common MDs, 6% serious MDs, 2% personality disorders, and 13% SRDs. For 5% of them, MDs were diagnosed during hospitalization, and 93% had at least one prior MD. Nearly half (43%) had chronic physical illnesses, 13% with high severity (3+), and 6% had co-occurring MDs–SRDs or MDs–SRDs–chronic physical illnesses. Within the 2 years prior to their last incident MD episode, 92% received follow-up care from their usual GP, 43% in family medicine groups, and 38% received high continuity of GP care. Most patients (72%) had a usual GP with over 20 years of seniority. In the year prior to their last incident MD episode, 9% were high ED users.
Characteristics of Patients Diagnosed with an Incident MD Episode and Physician Follow-Up Care (N = 2,670,133).
Note. ED = emergency department; GP = general practitioner; MD = mental disorder; SRD = substance-related disorder.
a A 3-year clearance period was required for the case definition of an incident MD episode from 1 April 1997 to 31 March 2000. Medical follow-up care, including that provided by GPs and psychiatrists, was thus measured from fiscal years 1 April 2000 to 31 March 2020. If a patient had several MD episodes, only the last episode was considered, controlling for the number of preceding episodes in the final model (see the Methods section for more details).
b This index aggregated patient data on material and social deprivation, which is related to the smallest geographic dissemination areas (zip code areas), established for the most recent versions of the Canadian census. For this study, quintiles were grouped into 3 levels representing the least to moderate (1–3), most (4–5) deprived areas, and nonassigned areas (0) for missing addresses or living in areas where index assignment was not feasible, such as nursing homes or homeless individuals.
c At least 2 diagnoses from the Régie de l'assurance maladie du Québec (RAMQ, Physician Claims database) or 1 principal diagnosis from the Maintenance et exploitation des données pour l'étude de la clientèle hospitalière (MED-ECHO, Hospital Inpatient and Day Surgery database) over a 12-month period were needed for a patient to be diagnosed with an incident MD, except in the case of SRDs as they are often underdiagnosed and thus needed only 1 diagnosis either from RAMQ or MED-ECHO, including secondary diagnosis. The first MD diagnosed in a 12-month period (e.g., depressive disorders), considering this case definition, and for the last incident MD episode from 1 April 2000 to 31 March 2020, was considered. However, co-occurring MDs–SRDs occurring during this period were controlled for in the final model.
d This represents a proxy for illness severity. The follow-up care periods (prompt, adequate, and continuous follow-up care) were measured after patient discharge.
e Chronic physical illnesses included: renal failure; cerebrovascular, neurological, and endocrine illnesses; tumour without or with metastasis; chronic pulmonary illnesses; diabetes complicated and uncomplicated; cardiovascular illnesses, and other chronic illness conditions (e.g., blood loss anemia) (see Supplemental Appendix 1 and the Methods section).
f These variables considered the last incident MD (including SRDs) in relation to co-occurring MDs or SRDs and chronic physical illnesses within the fiscal year of the incident MD (including SRDs), and within 2 years for chronic physical illnesses which usually have a lifetime occurrence.
g To be designated as the patient's usual GP (a proxy for family physician, variable not available in administrative databases), a minimum of 2 consultations with the same GP or with a different GP from the same family medicine group were required, measured 2 years before the last f incident MD episode. “Usual GP” refers to the GP most frequently consulted by a patient. References are provided in the Methods section.
h Continuity of GP care was measured with the Usual Provider Continuity Index, in which a score of ≥0.67 refers to a high continuity of care. The index describes the proportion of consultations with the “usual” GP out of all GPs consulted in outpatient care, including consultations in walk-in clinics. References are provided in the Methods section.
i The seniority of the usual GP referred to the number of years of practice of the patient's usual GP (or the GP most often consulted). The 20-year benchmark for GP seniority was constructed based on a 50% distribution of physician age in the database.
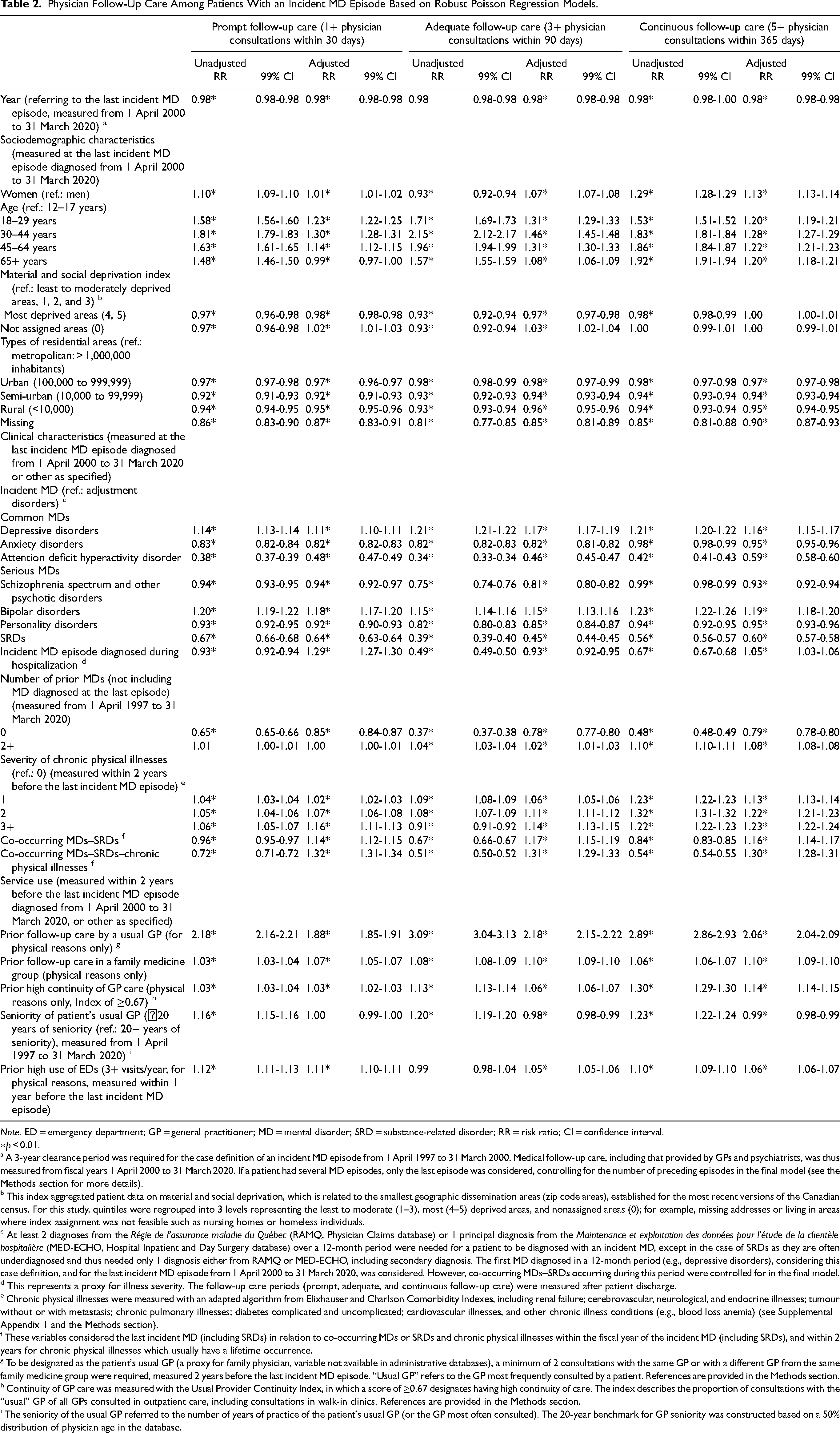
Patients more recently diagnosed with a last incident MD episode were less likely to receive follow-up care (Table 2). Compared with men and patients 12 to 17 years old, women and older patients were more likely to receive follow-up care—except patients aged 65+ who were less likely to receive prompt follow-up care. Patients living in the Montreal metropolitan area were more likely to receive follow-up care. Compared with patients residing in the least to moderately deprived areas, those in the most deprived areas were less likely to receive prompt or adequate follow-up care, while patients living in nonassigned areas were more likely to receive such follow-up care. Compared to patients with adjustment disorders, patients with depressive or bipolar disorders had a higher probability of receiving follow-up care, as did those with co-occurring MDs–SRDs, MDs–SRDs–chronic physical illnesses or chronic physical illnesses. Patients diagnosed with incident MD episodes during hospitalization were more likely to receive prompt and continuous follow-up care than those in outpatient care settings, but less likely to receive adequate follow-up care. Compared to patients with adjustment disorders and those with prior MD episodes, patients with anxiety, attention deficit hyperactivity, schizophrenia spectrum and other psychotic disorders, personality disorders or SRDs, or without prior MD were also less likely to receive follow-up care. Patients who received prior GP physical follow-up care, especially in family medicine groups, and who had high continuity of GP care, and patients with high previous ED use were more likely to receive follow-up care than those without these conditions. And finally, compared to patients whose usual GP had more seniority, those treated by a usual GP with <20 years of seniority were less likely to receive adequate or continuous follow-up care.
Physician Follow-Up Care Among Patients With an Incident MD Episode Based on Robust Poisson Regression Models.
Note. ED = emergency department; GP = general practitioner; MD = mental disorder; SRD = substance-related disorder; RR = risk ratio; CI = confidence interval.
∗p < 0.01.
a A 3-year clearance period was required for the case definition of an incident MD episode from 1 April 1997 to 31 March 2000. Medical follow-up care, including that provided by GPs and psychiatrists, was thus measured from fiscal years 1 April 2000 to 31 March 2020. If a patient had several MD episodes, only the last episode was considered, controlling for the number of preceding episodes in the final model (see the Methods section for more details).
b This index aggregated patient data on material and social deprivation, which is related to the smallest geographic dissemination areas (zip code areas), established for the most recent versions of the Canadian census. For this study, quintiles were regrouped into 3 levels representing the least to moderate (1–3), most (4–5) deprived areas, and nonassigned areas (0); for example, missing addresses or living in areas where index assignment was not feasible such as nursing homes or homeless individuals.
c At least 2 diagnoses from the Régie de l'assurance maladie du Québec (RAMQ, Physician Claims database) or 1 principal diagnosis from the Maintenance et exploitation des données pour l'étude de la clientèle hospitalière (MED-ECHO, Hospital Inpatient and Day Surgery database) over a 12-month period were needed for a patient to be diagnosed with an incident MD, except in the case of SRDs as they are often underdiagnosed and thus needed only 1 diagnosis either from RAMQ or MED-ECHO, including secondary diagnosis. The first MD diagnosed in a 12-month period (e.g., depressive disorders), considering this case definition, and for the last incident MD episode from 1 April 2000 to 31 March 2020, was considered. However, co-occurring MDs–SRDs occurring during this period were controlled for in the final model.
d This represents a proxy for illness severity. The follow-up care periods (prompt, adequate, and continuous follow-up care) were measured after patient discharge.
e Chronic physical illnesses were measured with an adapted algorithm from Elixhauser and Charlson Comorbidity Indexes, including renal failure; cerebrovascular, neurological, and endocrine illnesses; tumour without or with metastasis; chronic pulmonary illnesses; diabetes complicated and uncomplicated; cardiovascular illnesses, and other chronic illness conditions (e.g., blood loss anemia) (see Supplemental Appendix 1 and the Methods section).
f These variables considered the last incident MD (including SRDs) in relation to co-occurring MDs or SRDs and chronic physical illnesses within the fiscal year of the incident MD (including SRDs), and within 2 years for chronic physical illnesses which usually have a lifetime occurrence.
g To be designated as the patient's usual GP (a proxy for family physician, variable not available in administrative databases), a minimum of 2 consultations with the same GP or with a different GP from the same family medicine group were required, measured 2 years before the last incident MD episode. “Usual GP” refers to the GP most frequently consulted by a patient. References are provided in the Methods section.
h Continuity of GP care was measured with the Usual Provider Continuity Index, in which a score of ≥0.67 designates having high continuity of care. The index describes the proportion of consultations with the “usual” GP of all GPs consulted in outpatient care, including consultations in walk-in clinics. References are provided in the Methods section.
i The seniority of the usual GP referred to the number of years of practice of the patient's usual GP (or the GP most often consulted). The 20-year benchmark for GP seniority was constructed based on a 50% distribution of physician age in the database.
Discussion
To our knowledge, this study was the first to investigate predictors of prompt, adequate and continuous follow-up care among patients with incident MD episodes. In this study, MDs were reported in roughly one-third of the Quebec population, a number similar to recent prevalence rates for lifetime MDs in Canadian and international estimates.37,38 The number of patients diagnosed with an incident MD episode nearly doubled between 2000 and 2020, going from 3.5% to 6.7%—better MD detection, 38 treatment, 39 and improved mental health literacy 40 could explain these findings. Yet only one-third of patients in this study had received prompt or adequate follow-up care, and less than half had gotten continuous follow-up care. These results show that the Quebec mental health system needs reform, especially when it comes to improving access to prompt and adequate follow-up care within 1 to 3 months of an incident MD episode. More than 20% of Quebecers have no family doctor, 41 and access to a psychiatrist may take months. 42 Previous mental health reforms have focused on improving continuity of care,2,43 which may explain the better results seen on this indicator. From 2000 to 2020, the quality of follow-up care has decreased by roughly 13% despite efforts to optimize the efficacy of the mental health-care system. 2 Similar results were reported in a study of overall physician care. 44 Decreased quality of follow-up care may relate to increased MDs, 39 greater demand for care, 45 or malfunctioning organizational systems. 46 However, current trends recommend optimizing interdisciplinary care both in the Chronic Care 47 and Collaborative Care 48 models, increasing the number of nurse practitioners, 49 and providing more psychosocial care. 50 The inability to account for the other clinicians who work closely with physicians may have contributed to the low rate of follow-up care reported in this study.
Findings partially confirmed the first part of our hypothesis, namely that the most vulnerable patients with complex clinical characteristics would be more likely than others to receive prompt, adequate or continuous physician follow-up care after an incident MD episode. Among the most vulnerable patients receiving more follow-up care were those in the nonassigned areas, mostly patients who are living in nursing homes or homeless. These usually are high ED users,51,52 which may explain why they received more prompt or adequate follow-up care. Follow-up care was also higher in the Montreal metropolitan area, which is not surprising considering specialized care and GP walk-in clinics are usually overrepresented in large urban areas 53 and tend to attract more vulnerable patients such as the homeless and individuals with complex health conditions.52,54
Studies also reveal that hospitalized patients are among the most vulnerable, 55 which supports current trends seeking to improve discharge planning and continuous care, 56 and to provide better follow-up care for these patients. Those with co-occurring MDs–SRDs 57 and chronic physical illnesses 55 are also known for highly using services, and their complex conditions justify improving follow-up care. GPs reportedly prefer to treat patients with physical illnesses than those with MDs, 58 and those with common rather than complex MDs. 59 Though depressive disorders are the MD most frequently detected and treated by GPs, 60 patients with bipolar disorders often consult with their GP during depressive episodes. 61 Most of these patients are treatment compliant, 62 which may explain their better rates of follow-up care. Among patients with schizophrenia and other psychotic disorders, or with SRDs, the lower probability of follow-up care may be related to their reluctance to accept these conditions 63 and engage in treatment.8,63 The recent emphasis on detection and treatment of attention deficit hyperactivity disorder could explain why these patients were less likely to receive follow-up care. 64 Not surprisingly, the study found patients with a prior MD received more follow-up care, which suggests they may show a more chronic course of MDs and a greater likelihood of comorbidities.
Younger patients were underserved compared to those aged 18 to 64—the reluctance of patients aged 12 to 17 to seek and receive help 65 partially might explain this result. The situation was even worse for patients over 65 needing prompt follow-up care. Despite Canada having a universal health-care system, patients living in the most deprived areas received less prompt or adequate follow-up care compared to those living in the least to moderately deprived areas. As MDs usually appear prior to adulthood, 16 and given the key importance of early intervention for recovery, measures that impact MD chronicity and improve services for these patients may be prioritized, and in fact are central to most current mental health reforms. 66 More prompt follow-up care may also be implemented for the elderly whose health tends to deteriorate rapidly. 67 Outreach strategies 68 for patients residing in the most deprived areas may also be more effectively promoted. The finding that women have a higher probability of receiving follow-up care than men is easily explained by their higher reported rates of service use. 55
Study findings also confirmed the second part of our hypothesis, namely that patients receiving better prior GP follow-up care would be more likely to receive follow-up care after an incident MD episode. Patients followed by a senior GP in family medicine groups and those receiving a high continuity of GP care were particularly more likely to get follow-up care after an incident MD episode—family medicine groups have regulations that ensure prompt and continuous care, especially for vulnerable populations. A previous study shows that senior GPs play a more active role than their junior counterparts in treating patients with MDs. 58 As for high ED users, those are known to be high outpatient services users 69 as well as a vulnerable clientele with complex health issues, 55 which would explain why they are more likely to receive follow-up care. Overall, these findings align with the view that the Canadian health-care system responds more effectively to the new needs of existing patients than to those of individuals not currently under care, and that facilitating patient access to care could be greatly improved. 70
Limitations
Some variables such as race/ethnicity, suicidal behaviours, and medication compliance that could have impacted follow-up care were not available in the database. The study focused only on follow-up care provided by physicians paid by fee-for-services and did not include follow-up care with psychologists in private practices or other psychosocial clinicians in primary or specialized care, including nursing interventions; this had the effect of underestimating “global” follow-up care. The fact that the first type of MD incident selected had to come after a 3-year clearance period may have influenced study results, even as co-occurring MDs–SRDs were considered. Because patients hospitalized for more than a third of the follow-care period were excluded, more severe cases may have been understudied. Finally, study findings may not be generalizable to other countries, especially those without a public health-care system.
Conclusion
This study showed that more vulnerable patients with complex clinical characteristics, and those with better previous GP care were more likely to receive prompt, adequate or continuous follow-up care for an incident MD episode. However, only a minority of patients in the study had received physician follow-up care, and results showed that the level of care actually decreased over the study period. Prompt and adequate care, in particular, must be improved, as early intervention is key to patient recovery. Men, patients aged 12 to 17, those living in more deprived areas, and patients with anxiety, attention deficit hyperactivity, personality disorders, schizophrenia spectrum and other psychotic disorders, or SRDs, and those without previous MD may especially benefit from improved follow-up care. Better incentives and training for younger physicians may also be promoted, encouraging them to prioritize MD follow-up care.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437231182570 - Supplemental material for Predictors of Physician Follow-Up Care Among Patients Affected by an Incident Mental Disorder Episode in Quebec (Canada)
Supplemental material, sj-docx-1-cpa-10.1177_07067437231182570 for Predictors of Physician Follow-Up Care Among Patients Affected by an Incident Mental Disorder Episode in Quebec (Canada) by Marie-Josée Fleury, Louis Rochette and Lia Gentil, Guy Grenier, Alain Lesage in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437231182570 - Supplemental material for Predictors of Physician Follow-Up Care Among Patients Affected by an Incident Mental Disorder Episode in Quebec (Canada)
Supplemental material, sj-docx-2-cpa-10.1177_07067437231182570 for Predictors of Physician Follow-Up Care Among Patients Affected by an Incident Mental Disorder Episode in Quebec (Canada) by Marie-Josée Fleury, Louis Rochette and Lia Gentil, Guy Grenier, Alain Lesage in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We gratefully acknowledge the finding support of the Canadian Institutes of Health Research (CIHR). We also thank Jacques Tremblay, Victoria Massamba, the Institut national de santé publique du Québec, and the Quebec Network on Suicide, Mood Disorders and Associated Disorders for their support in this study.
Data Availability
In accordance with the applicable ethics regulations for the province of Quebec, the principal investigator is responsible for keeping data confidential.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (CIHR, grant number
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.