
Abstract
Objective
This 5-year longitudinal study evaluated patients with an onset of mental disorder (MD) following index emergency department (ED) visits, in terms of (1) patient profiles based on 12-month outpatient follow-up care received, (2) sociodemographic and clinical correlates, and (3) adverse health outcomes for the subsequent 2 years.
Methods
Data from administrative databases were collected for 2541 patients with an onset of MD, following discharge from Quebec ED. Latent class analysis was performed to identify patient profiles based on the adequacy of follow-up care after ED discharge. Bivariate analyses examined associations between class membership and sociodemographic and clinical correlates, high ED use (3 + visits/yearly), hospitalizations, and suicidal behaviors.
Results
Five classes of patients were identified. Class 1, the smallest, labeled “patient psychiatrist only,” included mainly young patients with serious MD. Classes 2 and 3, roughly 20%, were labeled “high use of patient general practitioner (GP) and psychiatrist” and “low use of patient GP and psychiatrist,” respectively. Both included patients with complex MD, but Class 2 had more women and older patients with chronic physical illnesses. The 2 largest classes were labeled “no usual patient service provider” (Class 5) and “patient GP only” (Class 4). Class 5 included more younger men with substance-related disorders, while Class 4 had the older patients living in rural areas, many with common MD and chronic physical illnesses. Class 3 patients had the poorest outcomes, followed by Classes 1 and 2, while Classes 4 and 5 had the best outcomes.
Conclusions
Results revealed that nearly 40% of patients experiencing an onset of MD received little or no outpatient care following ED discharge. Higher severity or complexity of MD and, to a lesser extent, no or low GP follow-up may explain these adverse outcomes. More adequate, continuous care, including collaborative care, is needed for these vulnerable, high-needs patients.
Introduction
Ensuring the delivery of adequate follow-up care for patients with mental disorders (MD) is a major public health issue. 1 Early intervention after an onset or acute MD-related episode is highly recommended, contributing to treatment efficacy, patient recovery, and reduced costs.2–4 Patients discharged from emergency departments (ED) are particularly vulnerable and require close follow-up. Early intervention, adequate intensity, and continuity of outpatient care have been found to decrease ED use, hospitalizations,5,6 and suicidal behaviors. 7 For newly diagnosed patients with MD, receiving physician care at least once within 30 days following ED discharge or hospitalization, or twice within the 90-day acute phase of MD8,9 are also indicators of adequate follow-up care.
However, most patients with MD do not use mental health (MH) services, while those who do so experience considerable variation in the services received.3,4 Few studies have investigated profiles of patients based on the nature and extent of follow-up care received. Studies that have developed patient profiles focused mainly on service use, including types and frequency of outpatient services, 10 ED use or hospitalization,11,12 types of care, 13 and fluctuations in services provided to patients with MD over time.14,15 One study distinguished 3 classes of patients according to low, moderate, or high use of MH services, 16 while 2 other studies identified classes related to intensity and diversity of care for MH reasons.17,18 Moreover, few studies have linked profiles of patients based on follow-up care with sociodemographic and clinical characteristics. Younger age,12,19 single civil status, 20 and diagnoses of common MD or substance-related disorder (SRD)11,21 were associated with lower continuity and less adequate care, compared with older age, serious MD, and having social support. Older patients with more serious MD and co-occurring health or social problems made more use of ED and experienced more suicidal behaviors and hospitalizations than other patients.3,4,22
To our knowledge, no studies have investigated patient profiles based on follow-up care for an onset of MD with various indicators of adequate care. A better understanding of these profiles, and associated sociodemographic and clinical characteristics and outcomes, may promote services answering patient needs. Patients experiencing an onset of MD may receive variable adequacy and continuity of care during recovery. Further investigation is required for the period following ED discharge, as these patients, due to overall vulnerability, may face serious challenges in accessing MH care. Based on a cohort of 2541 patients who experienced an onset of MD and were discharged from Quebec (Canada) ED, this study identified: (1) patient profiles according to outpatient follow-up care over a 12-month period; (2) sociodemographic and clinical correlates, and (3) adverse patient outcomes for the subsequent 2 years.
Methods
Study Population and Design
The study included 12 000 patients from the ED of 6 university or psychiatric hospitals located in urban areas of Quebec, and is based on a 5-year investigation (April 1, 2012 to March 31, 2017) using provincial medical administrative databases (Régie de l’assurance maladie du Québec, RAMQ). To enter the cohort, patients had to be eligible for the RAMQ, be aged 12 + , and diagnosed with an onset of MD (including SRD) at their first ED visit in 2014 to 2015 (index year) including a two-year previous clearance period of being without MD. Patients were excluded if they were hospitalized for more than 30 days following the index ED visit, or for one-third or more of the follow-up care periods (30, 90, or 365 days) subsequent to index ED visit, as these would prevent to measure adequately outpatient follow-up care.
Data Sources
The medical administrative database developed for the study included RAMQ, integrating billing systems for most physician services except for 6% of services occurring outside the public system, 23 and other databases providing information on patient sociodemographic characteristics (FIPA), service use (BDCU), hospitalization (MED-ECHO), and psychosocial interventions received in community healthcare centers (I-CLSC). Diagnostic codes from these databases were framed by the International Classification of Diseases Ninth and Tenth Revisions (Appendix 1). Figure 1 identifies the databases linked to each study variable. Databases were linked using a unique patient identifier. The Quebec Commission of Access to Information and the ethics committee of an MH organization approved the study protocol.
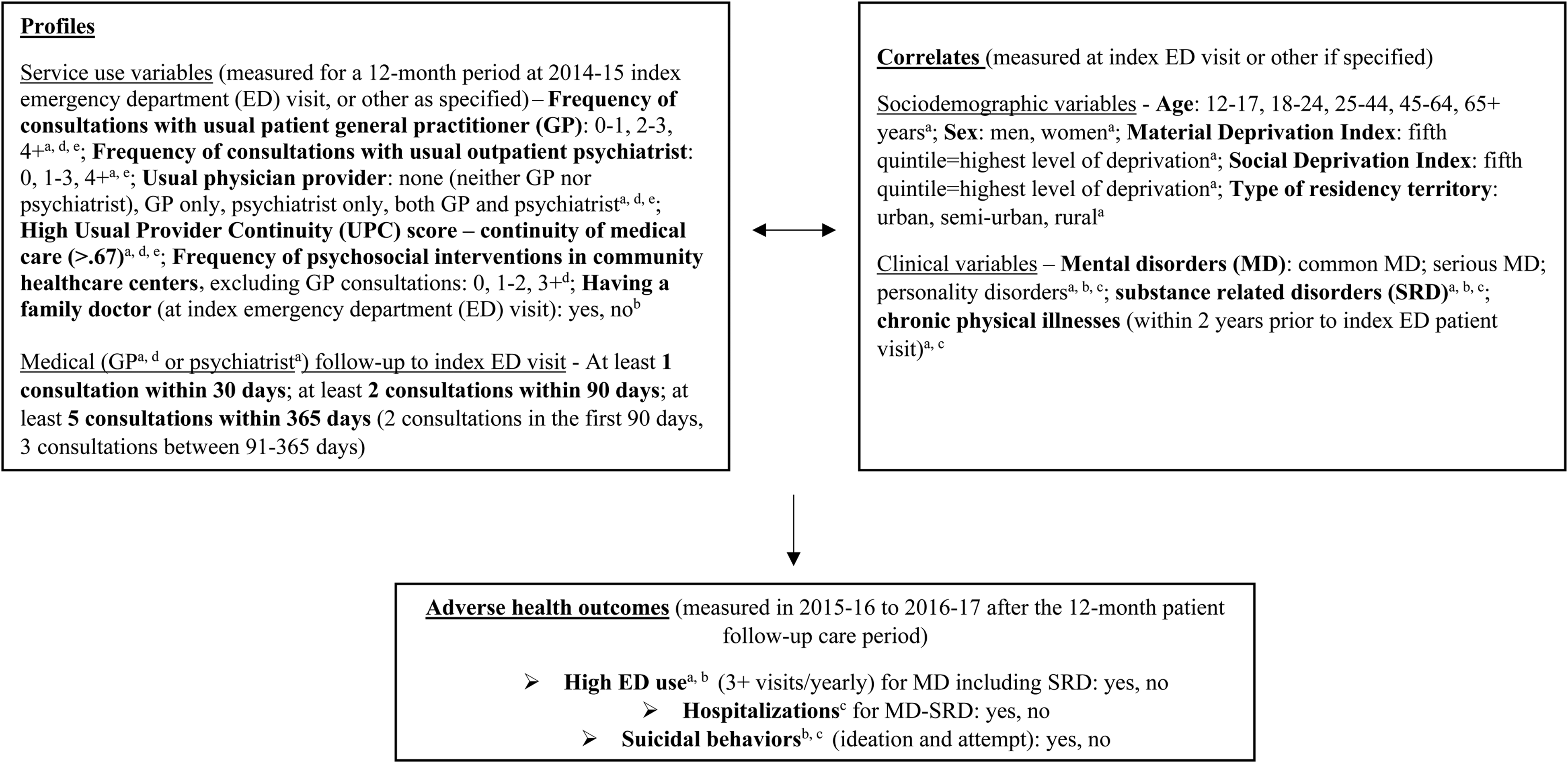
Conceptual framework of profiles, correlates, and outcomes among patients experiencing an onset of mental disorder based on outpatient care received following index emergency department visits.
Variables
Based on the MH service use literature,10–22 variables used to construct profiles of patients based on outpatient follow-up care included: having a family doctor; frequency of consultations with a usual patient general practitioner (GP) or outpatient psychiatrist; usual physician provider (GP or psychiatrist only, both GP and psychiatrist, or neither); high continuity of medical care; number of psychosocial interventions in community healthcare centers, measured from the index ED visit for a 12-month period; at least one medical consultation (GP or psychiatrist) within 30 days, 2 medical consultations within 90 days, or 5 medical consultations within 365 days following index ED visit (2 consultations in the first 90 days, and 3 between 91 and 365 days) (Figure 1). Usual patient GP, a proxy for a family doctor, was defined as having a minimum of 2 consultations with the same GP or with at least 2 GP working in the same family medicine group. 24 At least 60% of Quebec GP worked in family medicine groups collaborating with nurses and social workers, striving to ensure continuity of care and extended medical coverage. 25 Regarding usual psychiatrists, patients with only one consultation had to have made at least 2 consultations with their GP, defined as collaborative care. 26 Continuity of care was measured with the Usual Provider Continuity Index, which describes the proportion of consultations to usual GP and psychiatrist of total GP and psychiatrist consultations. 27 A score of > 0.67 indicates high care continuity. 28 Interventions in community healthcare centers, excluding GP consultations, mainly involved psychosocial services provided by multidisciplinary MH teams. The 30-day benchmark for receiving at least one follow-up medical appointment is a strong indicator for adequate access to care following the onset of MD. 9 Having at least 2 follow-up medical visits after the onset of MD (ie, 3 visits in total including index ED visit) is another key indicator of adequate care in the acute MD phase. 8 The indicator of at least 5 consultations within 12 months, excluding the index ED visit, is generally viewed as adequate “long-term” care following an onset of MD. 29
Sociodemographic and clinical correlates were measured at index ED visit. Sociodemographic variables included: age group, sex, material, and social deprivation, and type of residential area (eg, urban). Based on the 2011 Canadian census, the Material Deprivation Index 30 was derived from the ratio of population employment, average income, and number of individuals without a high school diploma; while Social Deprivation Index 30 measured proportions of individuals living alone, without a spouse and single-parent families. Both indices were classified in quintiles but regrouped into 3 categories representing low,1,2 moderate, 3 and high deprivation (4-5 or not assigned). The not assigned groups included patients without an address, for example, homeless individuals. Clinical correlates included: MD, SRD, and chronic physical illnesses as follows: for MD, common MD (anxiety, depressive, adjustment, and attention deficit/hyperactivity disorders), serious MD (bipolar disorders, schizophrenia spectrum and other psychotic disorders), and personality disorders; for SRD, alcohol- and drug-related disorders (use, induced, intoxication, withdrawal). The list of chronic physical illnesses was adapted from the Elixhauser Comorbidity Index. 31
Adverse health outcomes measured for an additional 24-month period (2015-2016 to 2016-2017) after the 12-month follow-up period included high ED use and hospitalizations for MD–SRD, and suicidal behaviors (ideation, attempt). High ED use, defined as 3 + ED visits/year, is based on previous Quebec research32,33 and reflects standard estimates.34,35 These 3 outcomes are among the strongest indicators of adverse health outcomes.7,36
Data Analysis
The Chi-square test was used for comparisons between the study cohort and excluded patients on sociodemographic and service use variables. Latent class analysis (LCA) was performed to identify profiles of patients in follow-up care after ED discharge.37,38 LCA is a model-based technique that identifies population heterogeneity by analyzing individual patterns of behavior for common types or “classes.” 39 LCA considers categorical variables to assess model fit using likelihood statistics, which capture uncertainty in the classification. 40 A series of latent class models were produced, evaluating from 1 to 6 classes. Four indices, the Akaike Information Criteria, 41 Bayesian Information Criteria, 42 consistent AIC, 43 and entropy value 44 were used to calculate the best-fit model. Bivariate analysis (chi-squared test) was used to examine associations between class memberships, that is, sociodemographic and clinical correlates and outcomes. Missing data (˂1%) on the LCA and latent status indicators are permitted in these procedures. All analyses were performed using Stata 15, and SAS 9.4 for the LCA. 39
Results
Sample Characteristics
Of the 12 000-patient cohorts, 2819 were diagnosed with an onset of MD (including SRD). Of these patients, 278 were excluded, including 93 hospitalized for more than 30 days after their index ED visit, and 185 hospitalized for one-third or more of the follow-up care periods after index ED visit. The final study sample consisted of 2541 patients. Comparison analyses between the study cohort and excluded patients showed that the latter differed significantly only in terms of (older) age and ratings on the Social Deprivation Index (more at level 3); yet they differed quite significantly on service use, justifying the exclusion from the study of patients whose length of hospital stay was too prolonged to appropriately measure outpatient care (Appendix 2).
Of the 2541 patients (Table 1), 37.8% were 25 to 44 years old and 52.0% male; 45.1% and 62.5% of patients scored 4 to 5 or were not assigned on Material and Social Deprivation Indices; 76.6% lived in urban territories. Diagnoses included common MD (54%), serious MD (16.7%), personality disorders (12.8%), SRD (22.9%), and chronic physical illnesses (23.1%), while 45.7% of patients reported not having a family doctor, and 38.9% no usual physician provider. GPs were the usual provider for 33.1%. Regarding follow-up care, 49.2% and 72.0% did not consult their respective usual GP and psychiatrists. Some 55.2% had high scores on continuity of care, and 30.3% scored high on psychosocial interventions in community healthcare centers; 30% of patients received at least 1 medical consultation within 30 days, 33.1% 2 visits within 90 days, and 20.0% had 5 consultations within 365 days of index ED visit. Regarding adverse patient outcomes, 13.3% reported high ED use, 12.9% hospitalizations, and 14.1% suicidal behaviors.
Patient Characteristics (n = 2541).
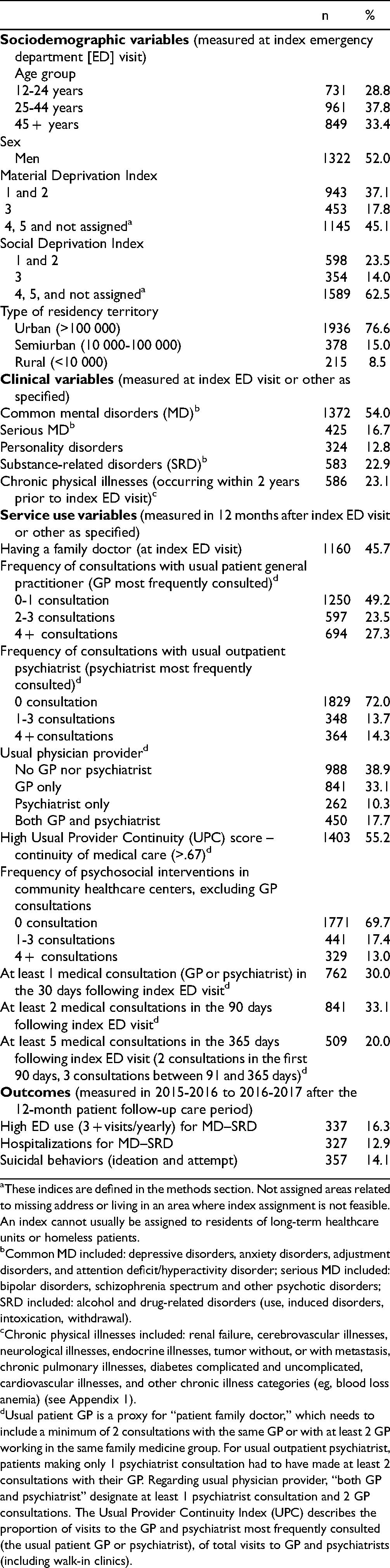
These indices are defined in the methods section. Not assigned areas related to missing address or living in an area where index assignment is not feasible. An index cannot usually be assigned to residents of long-term healthcare units or homeless patients.
Common MD included: depressive disorders, anxiety disorders, adjustment disorders, and attention deficit/hyperactivity disorder; serious MD included: bipolar disorders, schizophrenia spectrum and other psychotic disorders; SRD included: alcohol and drug-related disorders (use, induced disorders, intoxication, withdrawal).
Chronic physical illnesses included: renal failure, cerebrovascular illnesses, neurological illnesses, endocrine illnesses, tumor without, or with metastasis, chronic pulmonary illnesses, diabetes complicated and uncomplicated, cardiovascular illnesses, and other chronic illness categories (eg, blood loss anemia) (see Appendix 1).
Usual patient GP is a proxy for “patient family doctor,” which needs to include a minimum of 2 consultations with the same GP or with at least 2 GP working in the same family medicine group. For usual outpatient psychiatrist, patients making only 1 psychiatrist consultation had to have made at least 2 consultations with their GP. Regarding usual physician provider, “both GP and psychiatrist” designate at least 1 psychiatrist consultation and 2 GP consultations. The Usual Provider Continuity Index (UPC) describes the proportion of visits to the GP and psychiatrist most frequently consulted (the usual patient GP or psychiatrist), of total visits to GP and psychiatrists (including walk-in clinics).
Latent Class Analysis (LCA)
The LCA determined a five-class solution (BIC: 4 class = 3897.0, 5 class = 3148.5, 6 class = 3193.3; CAIC: 4 class = 3964.0, 5 class = 3232.5, 6 class = 294.3). The entropy value for the five-class solution was 0.989, with values greater than 0.8 indicating good separation and limited class overlap. Class 1 (Table 2), labeled “patient psychiatrist only,” was the smallest of the 5 classes (n = 165, 6.5%). All Class 1 patients received follow-up from their psychiatrist and the frequency of consultations was highest, with 75.8% making 4 + consultations. Yet these patients had no usual GP follow-up and was the second highest class reporting no family doctor (41.2%). Continuity of care was also high for Class 1 (87.7%). Thirty-day medical follow-up was adequate for 69.1% of patients, 90-day follow-up adequate for 100%, while 365-day follow-up was adequate for 47.9%.
Characteristics of the Five-Class Model Based on Follow-up Care Variables.
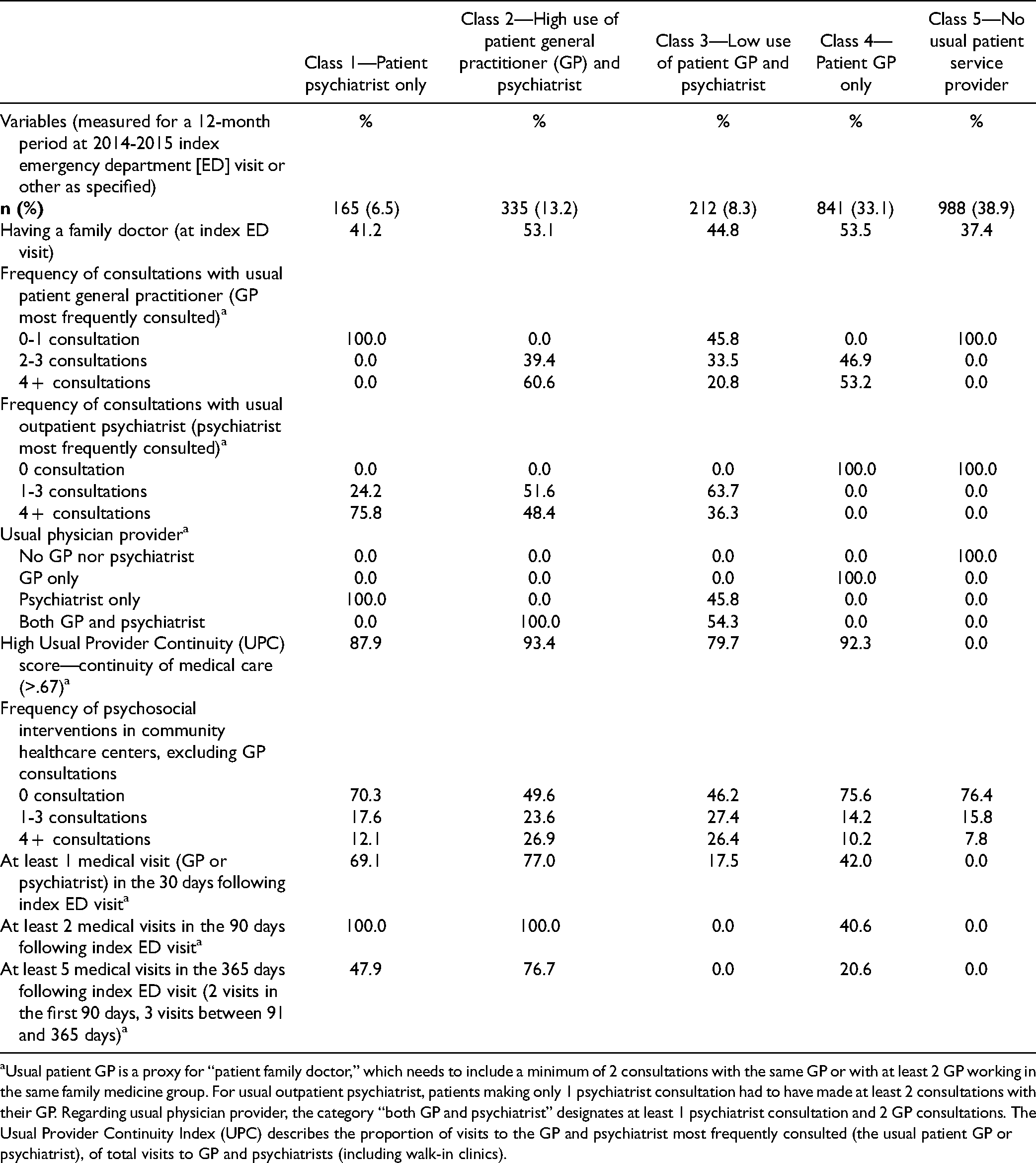
Usual patient GP is a proxy for “patient family doctor,” which needs to include a minimum of 2 consultations with the same GP or with at least 2 GP working in the same family medicine group. For usual outpatient psychiatrist, patients making only 1 psychiatrist consultation had to have made at least 2 consultations with their GP. Regarding usual physician provider, the category “both GP and psychiatrist” designates at least 1 psychiatrist consultation and 2 GP consultations. The Usual Provider Continuity Index (UPC) describes the proportion of visits to the GP and psychiatrist most frequently consulted (the usual patient GP or psychiatrist), of total visits to GP and psychiatrists (including walk-in clinics).
In Class 2 (n = 335, 13.2%), labeled “high use of patient GP and psychiatrist,” all patients were followed by both providers. Their frequency of consultations with usual GP (60.6% with 4 + consultations) was the highest, and the frequency of psychiatrist consultations (48.4% with 4 + consultations) was second highest. Over half (53.1%) had a family doctor. Class 2 also included the highest percentages of patients with high continuity of care (93.4%), high frequency of psychosocial interventions in community healthcare centers (26.9% with 4 + consultations), and high medical follow-up: 77.0% within 30 days, 100% within 90 days, and 76.7% within 365 days.
Class 3, labeled “low use of patient GP and psychiatrist,” was the second smallest class (n = 212, 8.3%), with 54.3% of patients followed by both usual GP and psychiatrist and 45.8% by a psychiatrist only. Of 44.8% who reported having a family doctor, 54.3% made at least 2 consultations. All patients received at least one psychiatrist consultation, with 63.7% receiving up to 3. Class 3 had the second lowest percentage of patients with high continuity of care (79.7%). Like Class 2, 26.4% of Class 3 patients received 4 + psychosocial interventions in community healthcare centers. However, their results for medical follow-up were second lowest, with 17.5% of patients receiving medical follow-up within 30-days and none with adequate follow-up within 90 or 365 days.
Class 4, labeled “patient GP only,” was the second largest class (n = 841, 33.1%), with all patients consulting the usual GP only, and the highest number having a family doctor (53.5%). Class 4 included the second highest percentage of patients registering 4 + consultations with usual GP (53.2%) and high continuity of care (92.3%), but the second lowest percentage with 4 + psychosocial interventions in community healthcare centers (10.2%). In terms of medical follow-up, 42.0% of Class 4 patients were followed within 30 days of index ED visit 40.6% within 90 days, and 20.6% within 365 days.
Class 5, labeled “no usual patient service provider,” was the largest (n = 988, 38.9%), including patients without a usual GP or psychiatrist and the fewest having a family doctor (37.4%). None had high continuity of care. Class 5 ranked lowest in terms of percentages receiving 4 + psychosocial interventions in community healthcare centers (7.8%). No Class 5 patient received medical follow-up at any time point post-ED discharge.
Patient Sociodemographic and Clinical Correlates and Adverse Health Outcomes
Overall, patients were younger in Classes 1, 3, and 5, while those in Classes 2 and 4 were older. Classes 1 and 5 included more men (60.4%, 53.9%) than Class 2 (40.3%) (Table 3). Scores on the Material and Social Deprivation Indices did not differ significantly by class. Compared to Classes 4 and 5, Class 3 had the lowest percentage of patients living in rural territories (9.5% and 8.9% vs 3.3%). Class 4 included the highest percentage of patients with common MD (61.4%) and Class 1 the lowest (47.3%, 15.2%). Class 1 comprised more serious MD (38.8%), compared to Classes 4 and 5 (10.6%, 13.9%) with the lowest rates. Class 4 had the fewest patients with personality disorders (9.9%), versus Class 1 (15.2%). Most SRD cases occurred in Class 5 (30.8%), while Classes 1, 2, and 3 had fewer (9.7%-11.3%). Classes 4 and 2 included more patients with chronic physical illnesses (30.6%, 29.0%) relative to Classes 1 and 5 with the fewest (15.2%, 16.4%). Concerning patient outcomes (Table 4), ED use was higher in Classes 3, 1, and 2 (26.4%, 20.0%, 19,1%), compared with Classes 4 and 5 (9.6%, 10.4%). Hospitalization rates were similar: higher in Classes 3, 1, and 2 (27.8%, 22.4%, 19,1%), compared with Classes 4 and 5 (8.7%, 9.5%). More suicidal behaviors were reported in Classes 3, 2, and 1 (25.5%, 20.0%, 17.6%), than in Classes 5 and 4 (10.5%, 12.3%).
Patient Sociodemographic and Clinical Correlates by Class.
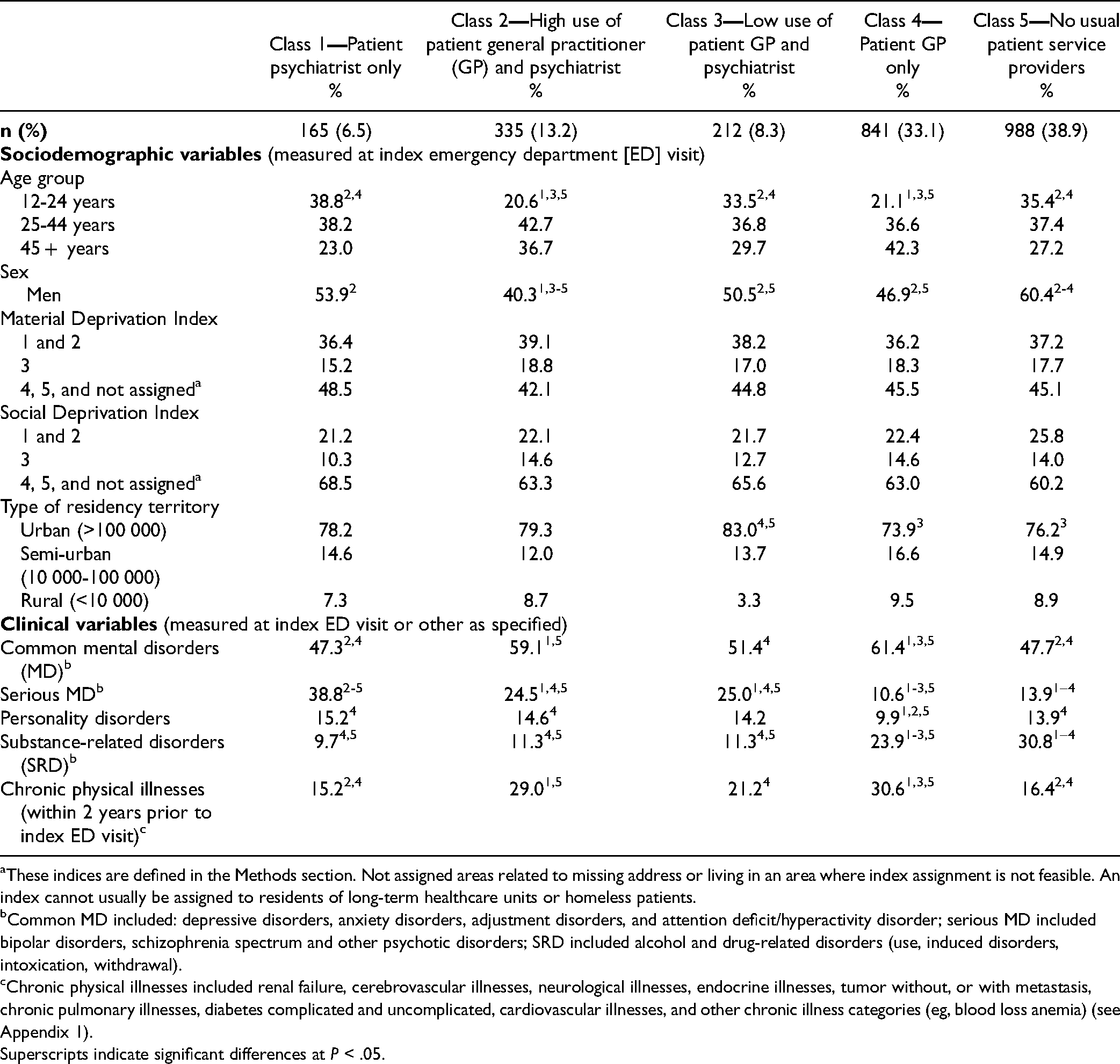
These indices are defined in the Methods section. Not assigned areas related to missing address or living in an area where index assignment is not feasible. An index cannot usually be assigned to residents of long-term healthcare units or homeless patients.
Common MD included: depressive disorders, anxiety disorders, adjustment disorders, and attention deficit/hyperactivity disorder; serious MD included bipolar disorders, schizophrenia spectrum and other psychotic disorders; SRD included alcohol and drug-related disorders (use, induced disorders, intoxication, withdrawal).
Chronic physical illnesses included renal failure, cerebrovascular illnesses, neurological illnesses, endocrine illnesses, tumor without, or with metastasis, chronic pulmonary illnesses, diabetes complicated and uncomplicated, cardiovascular illnesses, and other chronic illness categories (eg, blood loss anemia) (see Appendix 1).
Superscripts indicate significant differences at P < .05.
Adverse Patient Health Outcomes per Class.
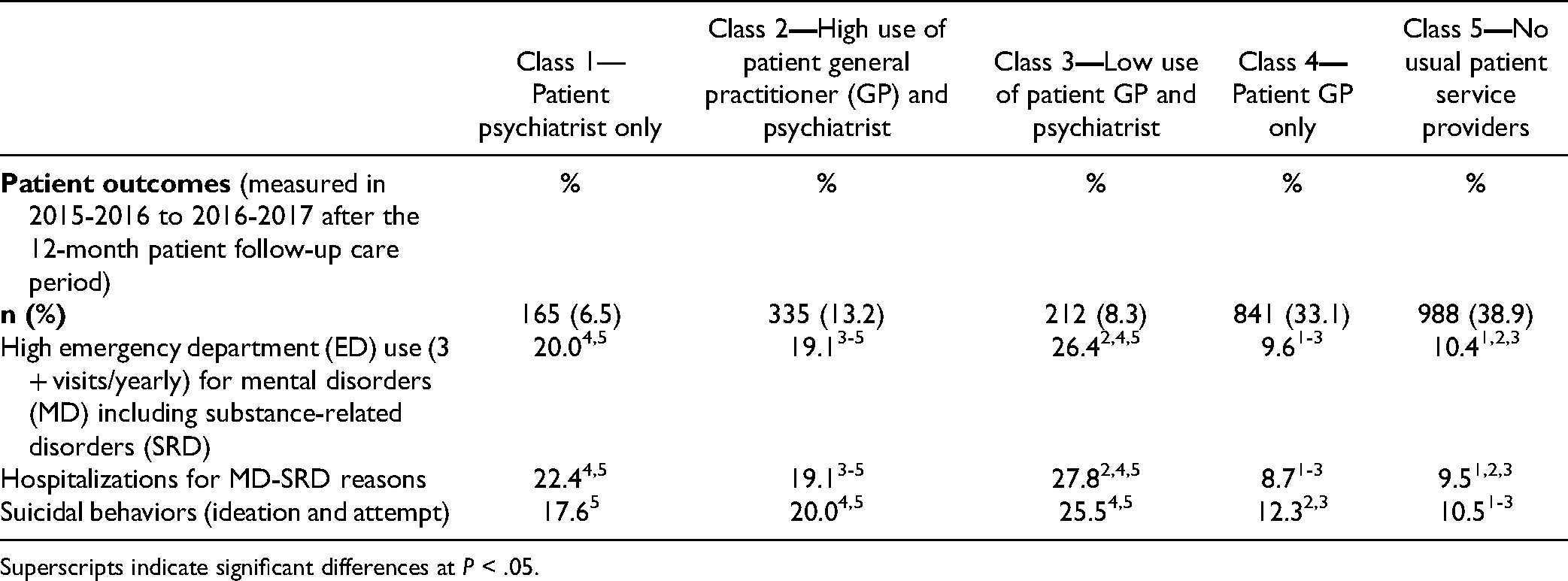
Superscripts indicate significant differences at P < .05.
Discussion
This study was original in identifying profiles of patients in follow-up care for a 12-month period after ED discharge, sociodemographic and clinical correlates, and adverse health outcomes for an additional 2 years. Patients were overall vulnerable, half of them experiencing high material or social deprivation and roughly one-fifth serious conditions. Half of the patients received no follow-up by a GP, while some 40% had no usual physician provider and fewer received psychosocial interventions in community healthcare centers. Medical follow-up was also low, with roughly 20% to 33% receiving adequate care according to 30, 90, or 365-day post-ED visit indicators. Percentages for medical follow-up were similar for the 30-day follow-up period 4 but lower for 90-day 8 compared with results previously reported. However, these studies were not specifically concerned with patients presenting at ED with an onset of MD. Low levels of patient follow-up may be due to difficulties in access to care, particularly GP in the case of Quebec, 8 and among patients with more serious or complex MD and social problems,45,46 GP poor knowledge of MD 47 and some stigmatization behaviors by clinicians. 48 Low deployment of evidence-based treatments, such as insufficient access to collaborative or integrated care with psychiatrists, may also have occurred.49,50
Five classes of outpatient profiles were identified, with Classes 5 and 4 representing nearly 75% of the sample. The findings that Classes 5 and 4, the largest, included no patient with a usual physician provider or patients with only GP follow-up were not surprising, as patients with MD are known for low MH service use 51 and consulting more with GP. 52 Class 5 patients were young and mainly men, many with SRD. Younger men are known to use MH services as a last resort, while SRD often entails non-adherence to treatment, 53 dropouts from services, and reported stigmatization. 54 Class 4 mainly consisted of patients with common MD and the highest incidence of chronic physical illnesses. Many Class 4 patients lived in rural areas, which may explain low follow-up by psychiatrists. Studies also found that GP prefers to treat common MD and co-occurring chronic physical illnesses. 55 Over half of Class 4 patients received intensive GP care, with 40% receiving medical care within 3 months, dropping to about 20% by 12 months post-ED discharge. Moreover, only 10% received intensive psychosocial interventions in community healthcare centers, a poor result considering that stepped care is considered best practice. 56 Regarding adverse outcomes, Classes 4 and 5 patients made the least use of ED and had the fewest hospitalizations and suicidal behaviors, which more likely reflected their less severe clinical profile than inadequate follow-up. Better health outcomes for Class 4 may also be explained by their high rates of GP follow-up and older age.
Classes 2 and 3, roughly 20% of the sample, represented the highest rates of both usual GP and psychiatrist consultations, and also psychosocial interventions in community healthcare centers. Collaborative care is recommended for patients with complex MD. 57 However, Class 3 had the worst results on high ED use and hospitalizations of all classes, significantly higher than Class 2. The fact that Class 3 patients received much less intensive GP follow-up, with poor results on continuity of medical care within 30-, 90-, and 365 days post-ED discharge may explain these outcomes. Compared with Classes 4 and 5, more Class 3 patients lived in urban areas, where patients receive less continuous care from GP working more in walk-in clinics. 58 Class 2 patients included more older women than in Class 3, who in previous studies were said to receive more care from GP than psychiatrists. 59
In Class 1, less than 10% of the sample, patients received intensive follow-up exclusively from psychiatrists, and continuity of care was high. Most were offered adequate medical care within different follow-up periods. However, like Class 3, Class 1 patients had the worst adverse health outcomes in terms of high ED use and hospitalizations, especially compared with Classes 4 and 5. Class 1 patients were younger and with more serious MD than other classes, which seems to account for worse outcomes despite intense psychiatric follow-up. Younger age and more serious MD were associated with both high ED use and hospitalizations in previous studies. 60
Limitations
First, some key data could not be examined, for instance, psychosocial interventions in hospitals, private clinics, or in the voluntary sector, or variables such as patient race/ethnicity, for which there was no information in RAMQ databases. Second, results for patients with an onset of MD discharged from ED, as a unique and highly vulnerable population, may not be compared to results for patients with MD at large. Third, the study also excluded older patients who experienced more lengthy periods of hospitalization, a group that may differ from others in terms of overall profile and adverse health outcomes. Finally, these results may not be generalizable to all healthcare systems, particularly those without universal healthcare coverage.
Conclusion
Findings underline that nearly 40% of patients with an onset of MD, especially those with SRD, received virtually no medical follow-up after discharge from their index ED visit. Roughly half of the patients also relied on their usual GP for care and only 20% received collaborative care. Five classes were identified: the largest groups without a usual physician provider or receiving GP follow-up only; 2 classes including patients with low or high intensity of psychiatrist and GP care, and a single class with psychiatrist care only. Higher severity or complexity of MD and, to a lesser extent, no or low GP follow-up may explain poor outcomes. Results suggest the need for increased GP follow-up in Classes 1, 3, and 5. Assertive community treatment or first-episode psychosis programs may also be promoted for Classes 1 and 3, intensive case management for Class 2, stepped care for Class 4, and outreach services for SRD in Class 5. Considering these results, substantial improvement in MH services is needed, particularly more collaborative and biopsychosocial care and post-ED discharge planning.
Footnotes
Acknowledgments
We gratefully acknowledge the support of the Canadian Institutes of Health Research (CIHR, grant number 8400997). We would also like to thank the Fondation Arbour, the Recherche et intervention sur les substances psychoactives—Québec (RISQ) research team, the Quebec Network on Suicide, Mood Disorders and Related Disorders (RQSHA), and the Fonds de recherche du Québec—Santé (FRQS) for awarding doctoral or publication scholarships to the first author. We thank Judith Sabetti for her editorial assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (grant no. 8400997) and by Quebec Network on Suicide, Mood Disorders and Associated Disorders.