
Abstract
Objective
Cannabis is commonly used by Canadian emerging adults (ages 18–25 years), many of whom attend post-secondary institutions. Frequent cannabis use is linked with psychotic-like experiences (PLEs); however, the exact nature of this association remains unclear. Anxiety symptoms may mediate this association, as they are prevalent in emerging adults and have been independently linked with both cannabis use and PLEs. Past work found that anxiety mediated the association between cannabis use frequency and attenuated positive psychotic symptoms (further along the psychosis continuum than PLEs), however this research had yet to be validated in the Canadian population, and trait rather than state anxiety (frequency of anxiety symptoms) was studied. Thus, our primary objective was to examine if anxiety symptoms mediated the association between cannabis use frequency and PLEs in Canadian emerging adult undergraduates. Despite known sex differences in cannabis use, expression of anxiety, and PLEs, past work did not evaluate the potential impact of biological sex on the anxiety-mediated model, and thus is the secondary objective of the present study.
Methods
1,266 first-/second-year emerging adult undergraduates from five Canadian universities provided cross-sectional, self-report survey data in fall 2021 semester. Validated measures of cannabis use frequency, anxiety, and PLEs were administered.
Results
Path analyses supported mediation from cannabis use to PLEs through anxiety (b = 0.07, P < 0.001, 95% bootstrap CI [0.03, 0.10]). No direct effect was found (P = 0.457), suggesting that the cannabis-to-PLEs association was mediated by anxiety. Mediation did not depend on biological sex (i.e., bootstrapped 95% CIs crossed zero).
Conclusions
Anxiety symptoms mediated the association between cannabis use and PLEs in emerging adults regardless of their biological sex. Assuming replication in prospective research, results highlight anxiety as an important intervention target in frequent cannabis-using emerging adults, to potentially prevent development/worsening of PLEs, and in turn psychotic illness.
Many Canadian emerging adults (aged 18–25) use cannabis. In 2021, ∼49% of those aged 20–24 years reported cannabis use; 1 26% of male and 24% of female emerging adult cannabis users reported daily/almost daily use. 1 Of Canadian emerging adults attending post-secondary institutions pre-COVID-19 pandemic, 48% reported past-year cannabis use; 9% of all male and 6% of all female students reported past month daily/almost daily use. 2
Research shows an association between cannabis use and psychosis, with higher rates of use observed in patients with, versus without, psychosis. 3 This association is dose-dependent, with higher frequency and THC potency of cannabis use significantly increasing the risk for psychosis.3–5 Daily cannabis users are > three times more likely to develop a primary psychotic disorder compared to never users, increasing to nearly five-times the risk with higher potency cannabis. 5 Cannabis risk mitigation strategies may benefit from examining processes earlier in psychotic illness development, specifically psychotic-like experiences (PLEs).
PLEs are defined as non-persistent changes in thoughts, perceptions, and behaviors that do not impede overall functioning (e.g., perceptual abnormalities, magical thinking), thus not qualifying as primary psychotic disorder symptoms.6,7 According to the psychosis continuum hypothesis, 7 the same factors that increase risk for psychotic disorders (e.g., frequent cannabis use) underlie the entire spectrum, thus also contributing to the prevalence of PLEs in the general population.6,8,9 Individuals with PLEs are at risk of developing psychotic disorders.10,11 As first episodes of psychosis tend to present in emerging adulthood, 12 examining links between cannabis use and symptoms earlier along the psychosis continuum is important given the high prevalence of cannabis use in this cohort. Thus, it is important to expand our limited understanding of the link between cannabis use and the development of PLEs, including underlying mechanisms.
Anxiety is common in Canadian emerging adults: approximately 23% of those aged 18–24 reported moderate-to-severe anxiety, 13 which typically increases in the first year of post-secondary education. 14 Frequent cannabis use is a risk factor for maintaining/worsening anxiety symptoms in adolescents and emerging adults. Early onset users, those using weekly or more, and those with greater lifetime cannabis exposure were all more likely to report elevated anxiety symptoms at later assessments compared to less frequent users.14–17 Anxiety is also a risk factor for PLEs: emerging adults with anxiety disorders are approximately five times more likely to score in the highest (versus lowest) quartile of PLE scores compared to non-anxious peers.10,18 Given these established links, anxiety appears an important potential mediating variable in clarifying the cannabis use-to-PLEs association in emerging adults.
Reeves and colleagues demonstrated that the link between cannabis use frequency and attenuated positive psychotic symptoms (APPS) was mediated by trait anxiety in an American sample aged 17–35 years. 19 Their results require replication and extension for four reasons. First, their data were collected in 2013 from a US sample in a state where recreational cannabis use remains illegal, 20 potentially limiting generalizability to the current Canadian undergraduate context. In Canada, recreational cannabis use was legalized in 2018, 1 increasing accessibility/normalization of cannabis, and potentially increasing participants’ willingness to report actual cannabis use levels.21,22 Second, Reeves et al. 19 measured trait anxiety (a stable personality trait) 23 which is less conceptually relevant as a mediator of the cannabis use-to-PLEs association than anxiety symptom frequency. Their results warrant replication using a validated measure of anxiety symptoms, which would more accurately assess if higher frequency cannabis use is a risk factor for increased frequency of anxiety symptoms,14–17 which, in turn, increases the risk for PLEs.10,18 Third, Reeves et al. specified their outcome as APPS19,24 which are further along on the psychosis continuum 7 (i.e., closer to psychotic disorder) than PLEs. Keeping earlier risk mitigation for psychotic disorders in mind, it is important to examine if anxiety-mediation can be demonstrated earlier along the psychosis spectrum.6–9
Lastly, Reeves et al. 19 did not evaluate the potential moderating impact of sex on the anxiety mediation model. Males use cannabis more frequently and in higher quantities, are more likely to have a cannabis use disorder, and are at higher risk for primary psychotic disorders than females.16,25,26 Comparatively, females are at greater risk for developing anxiety disorders than males.14,27 Moreover, female versus male daily cannabis users have greater than five times the risk of developing anxiety.16,27 Anxiety mediation of the cannabis use-PLEs link suggested by Reeves et al. 19 may also differ by sex.
Considering these gaps, we aimed to replicate previous mediational findings 19 in a sample of Canadian emerging adult undergraduates. We also attempted to extend Reeves et al.'s 19 model by specifying anxiety symptoms as the mediator and PLEs as the outcome, and by testing potential sex moderation. We hypothesized that (H1) more frequent cannabis use would be indirectly associated with greater PLEs through greater anxiety symptoms (Figure 1a). We hypothesized that sex would moderate this mediational model, with (H2) the cannabis-to-anxiety symptoms path (i.e., the a-path in the indirect effect) proving statistically stronger for females and (H3) the direct path from cannabis use frequency to PLEs proving stronger for males (Figure 2a).
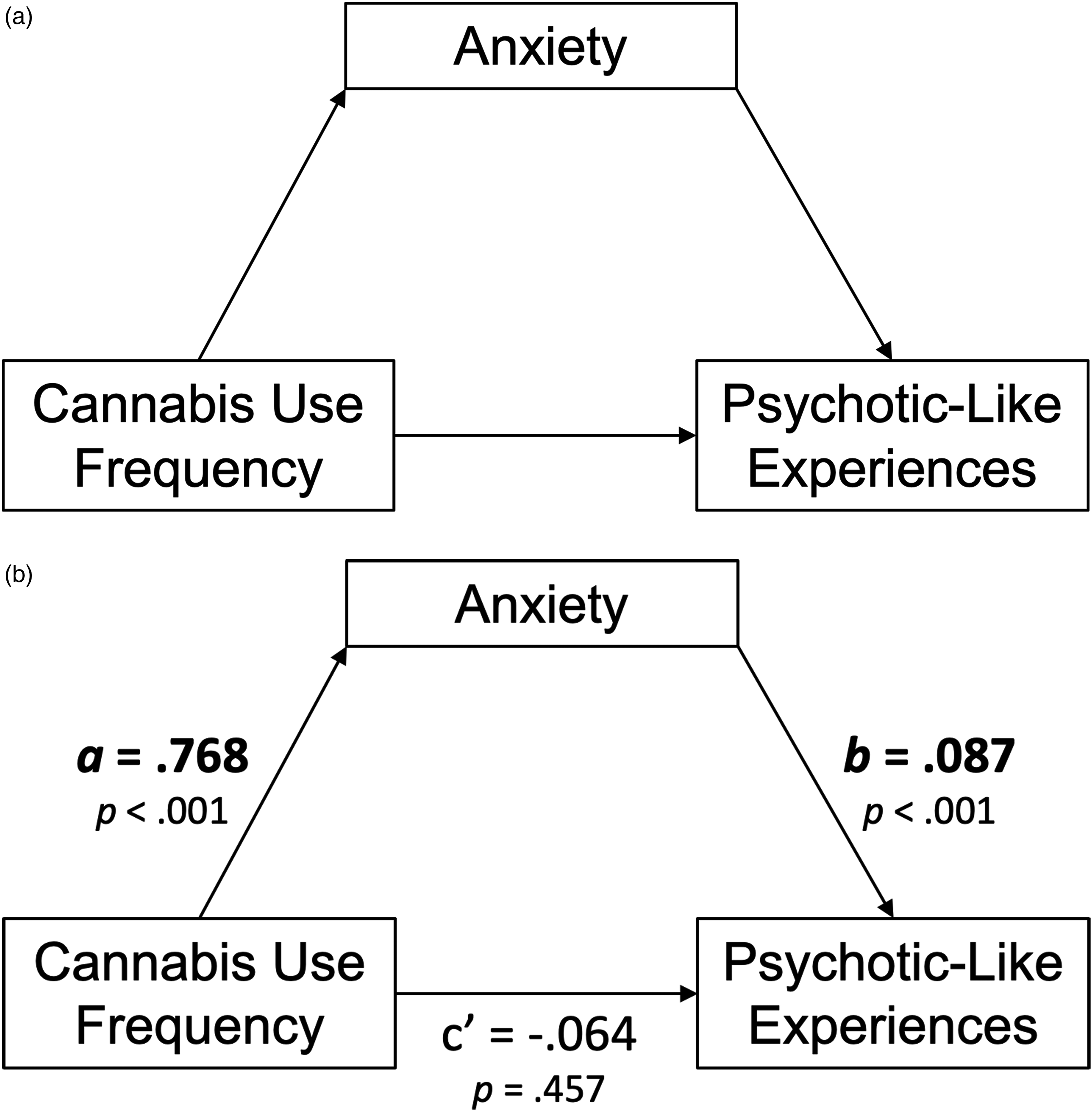
(a) Conceptual model of the simple mediation model. (b) N = 1,251. Path diagram of the simple mediation model.
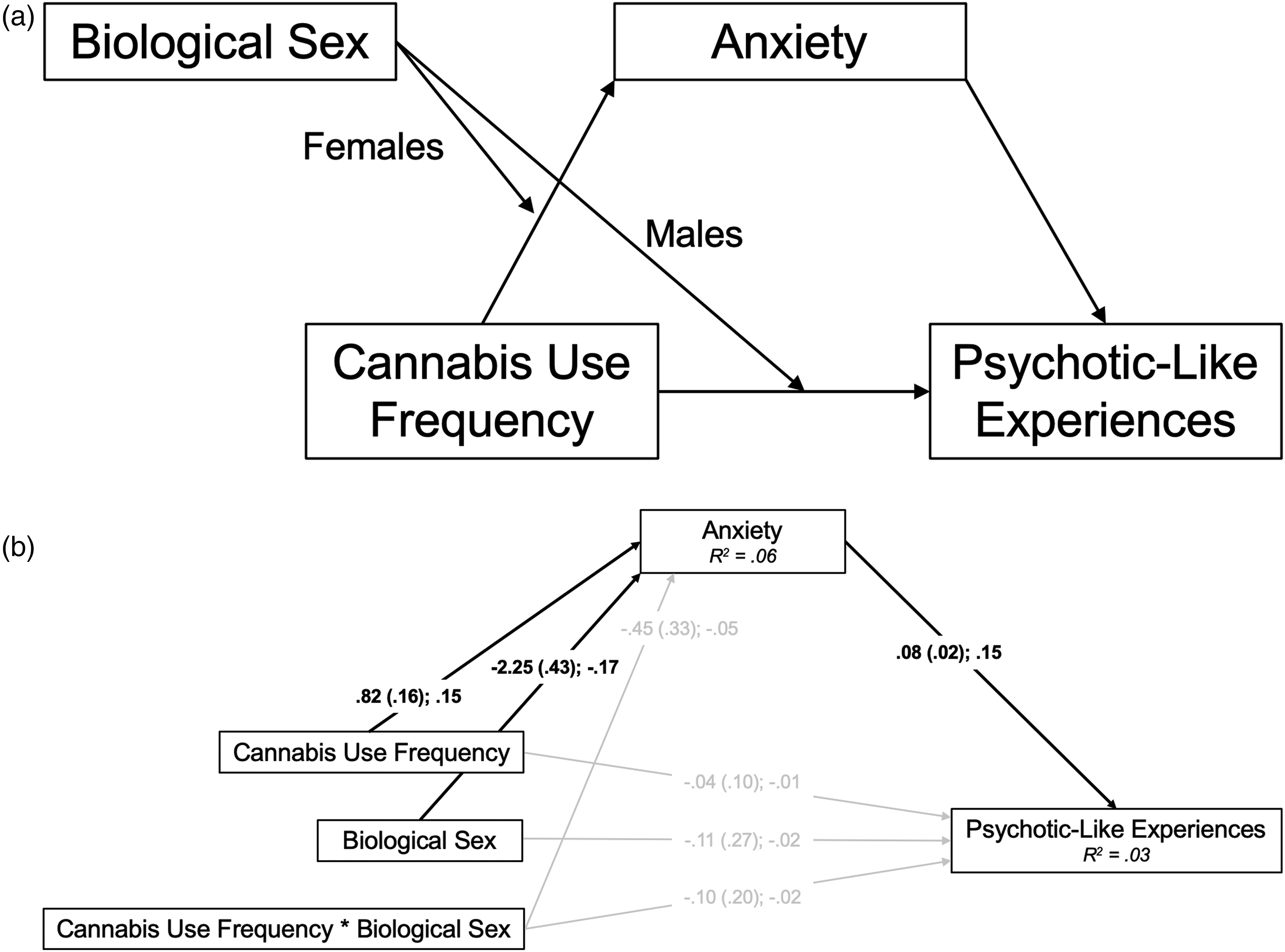
(a) Conceptual model of the conditional process (moderated mediation) model. (b) N = 1,248. Path diagram of the conditional process (moderated mediation) model; females = 0, males = 1. Path estimates presented as unstandardized coefficient (standard error); standardized coefficient. Bold denotes specified paths that were statistically significant (P < 0.05). R2 values represent the proportion of variance in the dependent variable that can be explained by the independent variables, significant at P < 0.001. MLR estimation was used to account for skewness.
Materials & Methods
Participants and Procedures
Hypotheses were tested using cross-sectional, self-report survey data collected in fall 2021 from first-/second-year emerging adult undergraduates aged 18–25 years. Students were recruited from five Canadian universities to participate in the UniVenture substance misuse prevention project 1 . All sites received research ethics board approval to conduct the survey. Recruitment occurred via online undergraduate research participation pools, campus-/faculty-wide electronic communications, social media/website advertisements (e.g., Facebook, Instagram), and/or on-campus posters/information booths. Participants gave written, electronic informed consent before completing online surveys. Participants received partial credit for an eligible psychology course or a gift card as compensation for their participation.
Measures
Statistical Analysis
R version 4.2 42 and SPSS Statistics version 28 43 were used to clean the data/obtain descriptive statistics. Two path models tested our hypotheses: in the simple mediation model, cannabis use frequency was specified as a predictor of PLEs (outcome) through anxiety (mediator); in the conditional process model, sex was examined as a moderator of the indirect (through anxiety) and direct pathways from cannabis use to PLEs. Here, cannabis use, sex, and the cannabis use by sex interaction term were specified as predictors of anxiety and of PLEs. Bias-corrected bootstrapped 95% confidence intervals (CI) were used to determine the presence and magnitude of indirect effects. Mplus version 8.7 44 was used to conduct the path analyses with FIML for missing data, and a maximum likelihood estimator robust to non-normal distributions (MLR), accounting for skewness. We considered both models supported if the relevant 95% CIs did not include zero. 45
Results
Demographic Variables
Cross-site data were merged, scored, and cleaned: 1,875 participants were excluded, having withdrawn from participation (n = 1,218, i.e., closed browser prior to completion), ineligibility (n = 504, e.g., not 18–25 years), and unreliable responding (n = 153, e.g., inconsistent responses to similar items), resulting in a final sample of 1,266 participants (see Table 1 for demographics).
Descriptive Statistics–Demographic Variables.
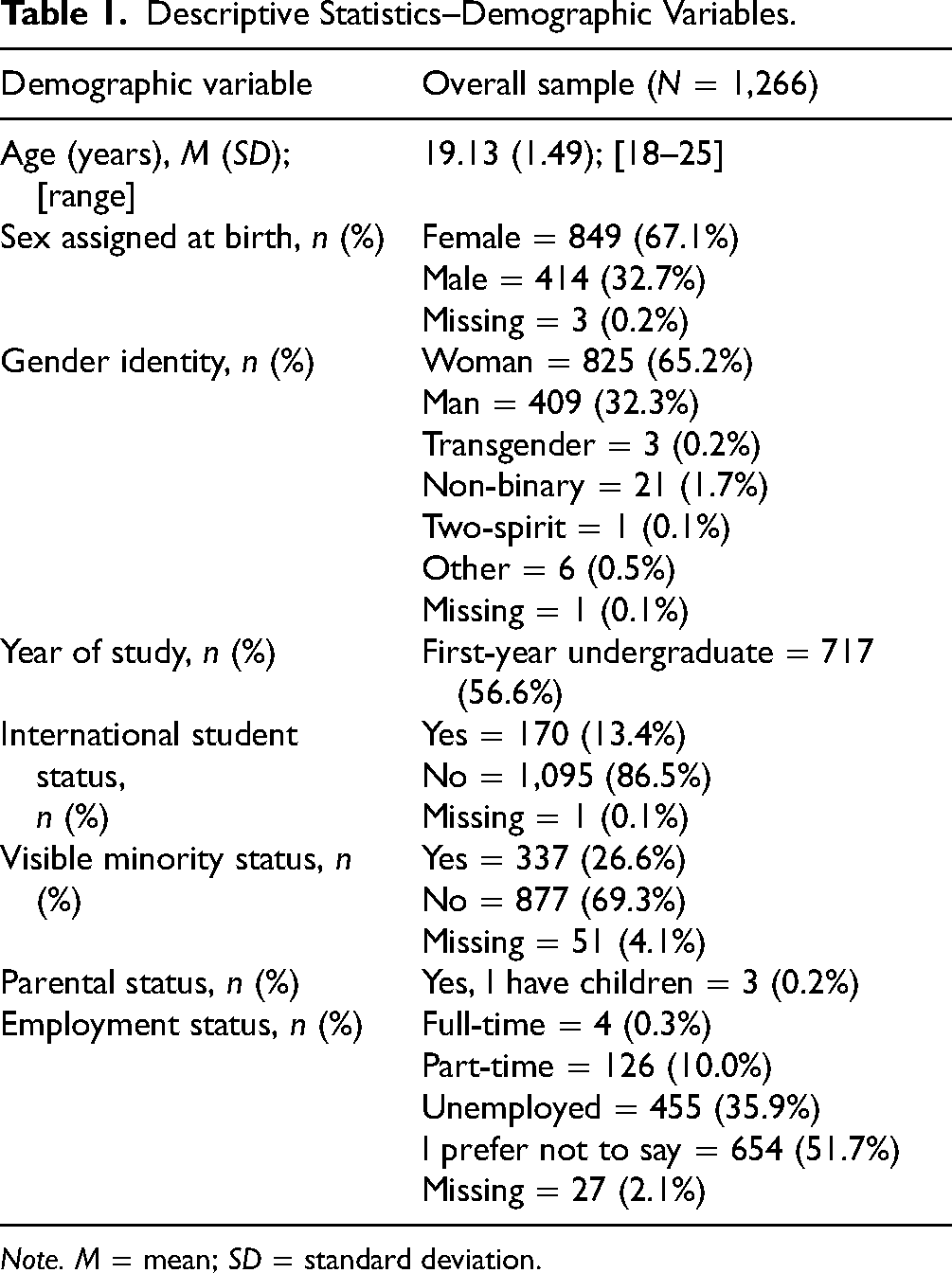
Note. M = mean; SD = standard deviation.
Clinical Variables
Table 2 provides the means and bivariate correlations of the clinically relevant variables under study and possible confounding variables. We found statistically significant positive correlations between cannabis use frequency and anxiety, and between anxiety and PLEs, the two paths constituting the hypothesized indirect effect.
Descriptive Statistics and Bivariate Correlations—Clinical Variables.
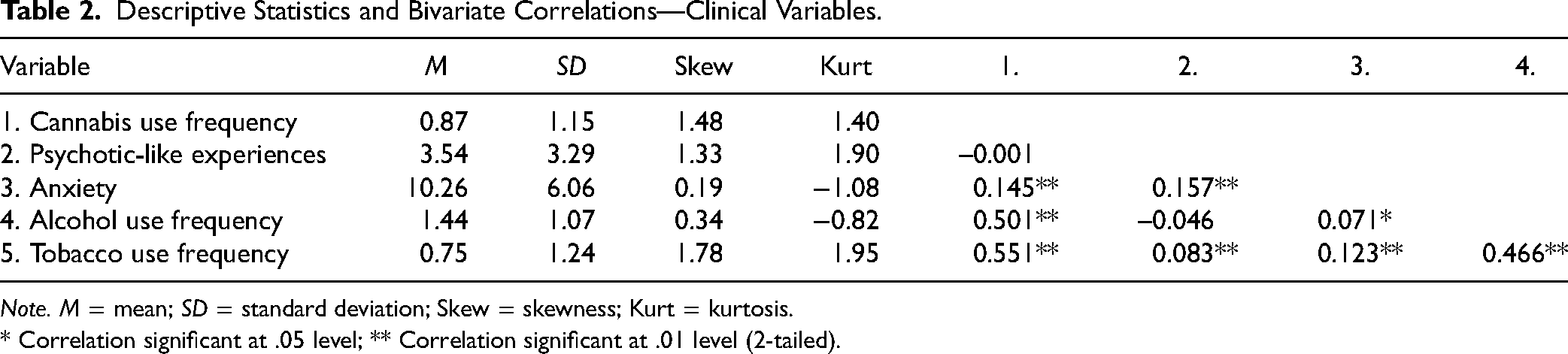
Note. M = mean; SD = standard deviation; Skew = skewness; Kurt = kurtosis.
* Correlation significant at .05 level; ** Correlation significant at .01 level (2-tailed).
Simple Mediation Model
This model tested H1 that more frequent cannabis use would be associated with greater PLEs through greater anxiety symptoms. Both a- and b-paths constituting the indirect (mediated) effect were statistically significant at P < 0.001, as was the associated indirect effect (b = 0.07, P < 0.001, 95% CI [0.03, 0.10]); thus, we found support for H1. After accounting for the indirect effect, there was no evidence of a remaining direct effect of cannabis use frequency on PLEs (c’ = −0.06, P = 0.457), suggesting anxiety symptoms fully mediate the cannabis-to-PLEs association in emerging adult undergraduates (see Figure 1b for full path diagram). The direction, magnitude, and significance of effects remained when controlling for study site and co-morbid alcohol and tobacco use.
Conditional Process Model
This model examined sex moderation of the simple mediation model (H2 and H3). The cannabis use frequency by sex interaction term did not predict anxiety symptoms or PLEs; thus, the anxiety mediation model did not depend on sex. Consistent with this lack of sex moderation effects, the 95% CIs crossed zero for both the indirect effect from the interaction term to PLEs through anxiety symptoms (95% CI = −0.093, 0.018], and the direct effect of the interaction term to PLEs [95% CI = −0.493, 0.303]. Inconsistent with H2 and H3, sex did not moderate the direct or indirect effects of cannabis use on PLEs (Figure 2b). 3 4
Discussion
Our primary objective was to examine whether anxiety symptoms mediated the association between cannabis use frequency and PLEs. Results supported anxiety mediation of the link between cannabis use frequency and PLEs, consistent with H1. Our secondary objective was to examine the potential moderating effect of sex on the hypothesized anxiety-mediated model. Contrary to our hypotheses, there was no evidence of sex moderation.
Reeves et al. 19 reported that the cannabis use-APPS association was mediated by trait anxiety in a US sample aged 17–35 years. We successfully replicated this anxiety-mediated model in the Canadian context (where cannabis is currently legal/widely available) 1 , and in a sample focused specifically on the developmentally vulnerable period of emerging adulthood (ages 18–25) 31 when cannabis use is common 1 and psychosis is most likely to onset. 12 Moreover, results supported anxiety mediation despite changing both mediator and outcome variables relative to Reeves and colleagues 19 : mediation was supported when the mediator was current (past-three-month) anxiety symptoms, measured by the GAD-7, 36 rather than trait anxiety. 19 Conceptually, anxiety symptoms are more state-like (variable over time) than trait anxiety (a stable personality trait) 23 and thus, a more relevant mediator in the cannabis use-PLE association. We also successfully extended Reeves et al.'s anxiety mediation model using PLEs as the outcome (versus APPS).19,24 PLEs are less severe/earlier along the psychosis continuum, 7 increasing the relevance of results to early identification and potential prevention of psychosis development in vulnerable emerging adults. This supported mediation model provides further evidence that frequent cannabis use and, in turn, heightened anxiety, are important potential risk factors for PLEs to target in interventions.
We extended Reeves et al. 19 by testing the potential sex-moderation effects on the anxiety-mediation model. Results did not support our sex-moderation hypotheses, suggesting that anxiety mediates the trajectory from frequent cannabis use to PLEs in emerging adults regardless of sex.
Historically, research has supported that males tended to use cannabis more frequently and in higher quantities compared to females.1,2,16,25,26 However, national cannabis surveys show that over time, the gap between sexes in cannabis use has narrowed, with rates of use in females rising to match that of males, a phenomenon known as convergence.47,48 In the present sample, females used cannabis significantly more frequently than males. This might be attributed to the growing social acceptability of cannabis use in young females in Canada. 47 The COVID-19 pandemic may have influenced results: 40% of Canadian emerging adults reported increasing their quantity, and 38% their frequency, of cannabis use during the pandemic. 1 Common reasons for increasing use were increased stress, anxiety, and isolation/loneliness 1 ; these predictors of greater cannabis use17,49 were particularly elevated among Canadian female versus male undergraduates during the pandemic.50,51
While anxiety symptoms were found to be moderately severe overall, females reported significantly more anxiety on the GAD-7 than males. This finding is consistent with literature showing that females are more anxious than males,14,27 and with reports that levels of anxiety have been significantly higher among females throughout the pandemic.50,51 Furthermore, PLEs were prevalent in this sample with students reporting an average of 3.54/18 on the PLEQ,37,38 nearly doubling previous reports (1.64/18 in the past year). 40 ∼37% of the present sample scored four or more on the PLEQ, indicating the presence of PLEs. 40 This rate is elevated compared to the 11.9% of a pre-pandemic sample of emerging adults who scored four or more found previously. 40 As substance use, stress, anxiety, and isolation/loneliness increased during the pandemic, 1 the elevation observed in PLE scores may also be explained by the present sample being taken during the pandemic. Indeed, a recent study compared inpatient psychiatric admissions during the COVID-19 pandemic to an earlier comparator period and found significantly more admissions related to substance use during the pandemic than before (45% vs. 28%). 52 Contrasting literature showing males to be at higher risk for PLEs/primary psychotic disorders compared to females,16,25,26 the number of PLEs reported herein did not vary by sex. Equivalent reports of PLEs by males and females in the present study may be due to females in our sample using cannabis significantly more frequently than the males, given the known links between cannabis use and symptoms along the psychosis continuum.3,6,7,9
Limitations
Firstly, mediation is considered a causal process that unfolds over time, 45 however this study used cross-sectional data limiting causal inference. 53 For example, this study assumed that anxiety symptoms preceded PLEs, however, it is possible that the experience of PLEs causes anxiety symptoms. 10 For this reason, some argue against testing mediation with cross-sectional data. 54 Others suggest that cross-sectional studies are reasonable when evaluating newer mediational models while keeping directional inference limitations in mind.45,53 Our results corroborate those found in a different sample using different measures, 19 supporting this study as a useful early step in increasing our understanding of anxiety's role in the link between cannabis use and psychosis-related outcomes.
Secondly, data were collected via online self-report measures which may be prone to biased responding. Furthermore, the Co-Venture Drug Use Battery 32 is a shortened version of the psychometrically-sound DEP-ADO,33,34 yet the reliability/validity of some specific individual items (e.g., cannabis use frequency) are unavailable. Possible mitigating factors of these limitations include that self-reported substance use has been shown to be acceptably accurate when confidentiality is assured and there are no risks of adverse consequences for responding truthfully (both true for this study). 55 Furthermore, online questionnaires have been shown to reliably capture emerging adults’ self-reported substance use. 22 Future work would benefit from clinician-administered interviews or biological drug testing, for example, to support self-report measures.
This study did not include certain clinically relevant variables such as participants’ family history of substance misuse, psychosis, and trauma. 3 Future studies would benefit from inclusion and control of such variables, to allow a more nuanced interpretation of results.
Lastly, while our sensitivity analyses controlled for site effects and the substances most commonly co-used by cannabis users1,2 and those at clinical high-risk for psychosis 56 other potential confounding variables may have impacted the study. For example, age of onset of cannabis use and other psychiatric comorbidities should be assessed and controlled for in future studies testing anxiety mediation.3,10,16
Conclusion
The high frequency of cannabis use and high prevalence of moderate/severe anxiety and PLEs in this Canadian emerging adult undergraduate sample further supports the need to increase our understanding of the relationship between these variables. Our study moved toward clarifying one potential mechanism (anxiety symptoms) driving the link between cannabis use and PLEs, including assessing for sex moderation. Our results suggest the following possible clinical implications: that reducing anxiety symptoms in frequent cannabis-using emerging adults may help prevent the development/worsening of PLEs, and that anxiety symptoms as an intervention target may be relevant for psychosis risk-reduction among undergraduates regardless of sex.
Footnotes
Acknowledgments
The authors extend their sincere thanks to the UniVenture Consortium which includes researchers and project staff from the five Canadian university data collection sites. In particular, they would like to thank Laura Lambe, Stephanie Cooper, Marion Audet, Nora Fripp, Naama Kronstein, Vanessa Morris, Raquel Nogueira-Arjona, Phillippe Pétrin-Pomerleau, Cassidy Wallis, Katherine Rose, Ramin Rostampour, Annie Wu, and Violet Cieslik.
Data Access
Interested researchers may request access to the deidentified data by contacting the corresponding author (sstewart@dal.ca). Data may be shared with qualified researchers upon reasonable request and pending ethical approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from a Social Sciences and Humanities Research Council (SSHRC) Partnership Grant [Grant#: 895-2019-1021; PI SHS], and a Canadian Institutes of Health Research (CIHR) Canadian Cannabis and Psychosis Research Team Catalyst Grant [Grant#: CA7-170130; co-PIs PJC & PGT]. HCRB's work on the project was supported by the Nova Scotia Research and Innovation Graduate Scholarship, a Maritime SPOR Support Unit Trainee Support Award, and a Scotia Scholar's Masters Award from Research Nova Scotia. PGT is funded through the Dr. Paul Janssen Chair in Psychotic Disorders. PJC is funded through a CIHR Tier 1 Canada Research Chair in Preventative Mental Health and Addiction. FMY is funded through the Mitacs Accelerate Post-Doctoral Fellowship program in collaboration with Injury Free Nova Scotia. SHS is funded through a CIHR Tier 1 Canada Research Chair in Addiction and Mental Health.