
Abstract
Objective:
The associations between adverse childhood experiences (ACEs) and psychopathology have been well-established in the general population. Research on ACEs in the homeless population has been limited. This study examined whether ACE exposure is associated with specific mental health outcomes among a national sample of homeless adults with mental illness and whether this association varies according to ACE dimension and gender.
Methods:
This cross-sectional study utilized data from a national sample of 2,235 homeless adults with mental illness in Canada to evaluate their sociodemographic characteristics, exposure to ACEs, and mental health outcomes. Exploratory and confirmatory factor analyses were conducted to identify and confirm ACE dimensions (maltreatment, sexual abuse, neglect, divorce, and household dysfunction) from individual ACE items. Multivariable logistic regression was used to examine the associations between total ACE score and ACE dimensions with mental illness diagnoses and psychopathology severity.
Results:
The mean total ACE score among all study participants was 4.44 (standard deviation [SD]: 2.99). Total ACE score was positively associated with several mental illness diagnoses and psychopathology severity. Unique associations were found between specific ACE dimensions and poor mental health outcomes. The prevalence of almost all ACEs was significantly higher among women. Yet, associations between several ACE dimensions and poor mental health outcomes existed uniquely among men.
Conclusions:
There are unique and gender-specific associations between specific ACE dimensions and mental health outcomes among homeless adults. Better understanding of the mechanisms underlying these associations is needed to inform screening, prevention, and treatment efforts, particularly given the very high prevalence of ACEs among this vulnerable and marginalized population.
Introduction
Adverse childhood experiences (ACEs) have been consistently linked with a wide range of poor social, economic, and health-related outcomes over the lifecourse. 1 –3 The pioneering Centers for Disease Control (CDC)-Kaiser ACE study revealed that adults exposed to ACEs were much more likely to have poor physical and mental health in later life. 4 Strong associations have also been reported between ACEs and such poor mental health outcomes as anxiety disorders, mood disorders, and suicidality. 5 –7
The majority of ACE studies have focused primarily on adults with stable housing and private health insurance. 8 Therefore, their findings cannot be generalized to vulnerable populations such as homeless adults, who are disproportionately exposed to childhood adversities. 9 In particular, homeless individuals incur a double burden from early adversities; in addition to the well-established associations of ACEs with poor health outcomes, 9 ACE exposure increases the risk of homelessness through fragmented familial ties, decreased social support, and limitations in education/employment opportunities. 10,11 The distinct associations between specific early adversities and mental health outcomes in homeless adults have rarely been examined. Studying ACEs in this context is important for developing tailored prevention programs and trauma-informed and trauma-specific services for this population.
Past ACE studies have mainly employed 2 broad approaches: (1) the cumulative approach and (2) the selective approach. The former approach sums the number of ACEs into an overall score, elucidating a dose–response relationship between total ACE score and poor later-life outcomes. 8,12 For example, adults exposed to 1, 4, and 7 or more ACEs are 1.7, 3.9, and 17.0 times more likely to have attempted suicide than those exposed to no ACEs. 5 However, the shortcoming of a cumulative approach is that it effectively equates disparate experiences. It is unlikely that individual ACEs such as childhood sexual abuse and parental divorce influence the same outcomes through the same mechanisms. 13 The selective approach focuses on a specific ACE but does not account for other contemporaneous adverse experiences. For example, childhood sexual abuse is associated with lifetime diagnoses of depressive disorders, post-traumatic stress disorder (PTSD), and suicide attempts. 14 However, the same outcomes are also associated with childhood physical abuse, emotional abuse, and neglect. 15 The shortcoming of a selective approach is that ACEs are highly intercorrelated, giving rise to omitted-variable biases. 16
There has also been limited research exploring the role of gender in early adversities and mental health outcomes among homeless individuals. Disparities in psychopathology have been well-established across sex and gender groups; women more often develop mood and anxiety disorders and men more often develop substance-related and externalizing disorders. 17 However, gender as a social construct will be the focus here instead of biological sex. Social realities faced by different gender groups such as gender roles and gender-based violence determine both exposure to and impact of early adversities. 18 –20 The experiences of early adversities and homelessness have also been shown to be distinct across gender groups in small qualitative studies, but they have rarely been studied in quantitative research with large samples. 21,22 Further gendered analysis of ACEs is crucial for informing practice and policy to better address the unique needs of homeless men, women, and individuals of other gender identities.
This study examines the relationship between dimensions of early adversities and mental health outcomes among individuals experiencing homelessness using a gendered lens. First, we investigate the differential associations of distinct ACE dimensions with several mental health outcomes. Second, we investigate whether these associations are different for self-identified men and women.
Methods
Study Population
The At Home/Chez Soi (AH/CS) study was a randomized trial of a Housing First (HF) intervention for homeless adults with mental illness conducted in 5 cities across Canada: Vancouver (British Columbia), Winnipeg (Manitoba), Toronto (Ontario), Montreal (Quebec), and Moncton (New Brunswick). 23 Trial details and related Consolidated Standards of Reporting Trials descriptions have been reported elsewhere. 23 The AH/CS study inclusion criteria were as follows: (1) legal adult status; (2) either absolute homelessness (those who lack a regular, fixed, physical shelter) or precarious housing (those whose primary residence is a single room occupancy, rooming house, or hotel/motel) with experiences of absolute homelessness in the past year; and (3) presence of a serious mental disorder (major depressive disorder, manic or hypomanic episode, mood disorder with psychotic features, panic disorder, PTSD, psychotic disorder) assessed through the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria on the Mini International Neuropsychiatric Interview 6.0 (MINI). 24 The AH/CS study recruited participants through referrals from an extensive network of shelters, drop-in centers, hospitals, outreach programs, mental health services, and community health centers. Information related to housing, health status, community functioning, sociodemographic characteristics, and social service use was collected using validated questionnaires and scales. 23
The present analyses are based upon baseline data collected from 2,235 AH/CS participants between October 2009 and June 2013 and data from the ACE module. Nineteen transgender/transsexual participants were excluded from the analyses, as this small number precludes multivariable analysis. In addition, the effect of ACEs on gender nonconforming individuals is unique and would not be appropriately captured in these analyses. 25,26
Measures
Total ACE score (cumulative ACE measure) and ACE dimensions were considered the main exposures in this study. ACEs were assessed 18 months after the baseline interview using the original ACE module. 4 The ACE module encompasses 10 categories of early adversities: emotional, physical, and sexual abuse; emotional and physical neglect; parental separation/divorce; domestic violence against women; household mental illness; household criminal justice involvement; and household substance abuse. To compute total ACE score, participants received 1 point for a category if they responded “Yes” to one or more questions in a particular category, for a maximum total score of 10. Higher values denote more exposure to ACEs.
The following mental health diagnoses were considered the main outcomes and were identified through the MINI: (1) major depressive disorder, (2) manic or hypomanic episode, (3) PTSD, (4) panic disorder, (5) mood disorder with psychotic features, (6) psychotic disorder, (7) alcohol dependence, (8) substance dependence, (9) alcohol abuse, (10) substance abuse, and (11) suicidality. Response options to the suicidality module include: “no,” “low,” “moderate,” or “high.” To assess co-occurrence of mental disorders, an indicator variable was created to capture having 2 or more mental disorders. The Colorado Symptom Index (CSI) score—measuring severity of self-reported psychiatric symptomatology—was also considered as an outcome. It was measured through a 14-item Likert-type scale with possible scores between 0 and 70, with higher scores indicating greater psychiatric symptomatology. 27 To assess severe psychiatric symptomatology, an indicator variable was created to capture a clinically relevant threshold of 30 points or more. 28 Psychometric properties for all measures are reported elsewhere. 23
Statistical Analysis
The study population was split into 2 random halves for analysis with exploratory factor analysis (EFA) and confirmatory factor analysis (CFA). To identify ACE dimensions, an EFA was performed on tetrachoric correlations of categorical responses to items on the ACE scale. Factor solutions were then obtained using the minimal residual method and Varimax (orthogonal) rotation. The best factorial solution was selected based on common guidelines of model fit, including root mean squared error of approximation (RMSEA), Tucker-Lewis index (TLI), and Bayesian Information Criterion. 29 Supplemental Appendix Table 1 presents the results of the EFA, producing 3 ACE dimensions with high primary factor loadings. Parental separation/divorce and sexual abuse did not load highly on any factor and were considered as separate ACE dimensions. Therefore, 5 ACE dimensions were included in subsequent analyses: maltreatment (emotional and physical abuse), sexual abuse, neglect (emotional and physical neglect), divorce, and household dysfunction (domestic violence, household mental illness, household criminal justice involvement, and household substance abuse). To validate EFA results, CFA was performed by specifying a standardized structural equation model corresponding to the 5 ACE dimensions (Supplemental Appendix Figure 1). Model fit was deemed appropriate based on RMSEA, TLI, and Comparative Fit Index.
Sociodemographic Characteristics, Mental Health Outcomes, and Adverse Childhood Experiences among at Home Study Participants.
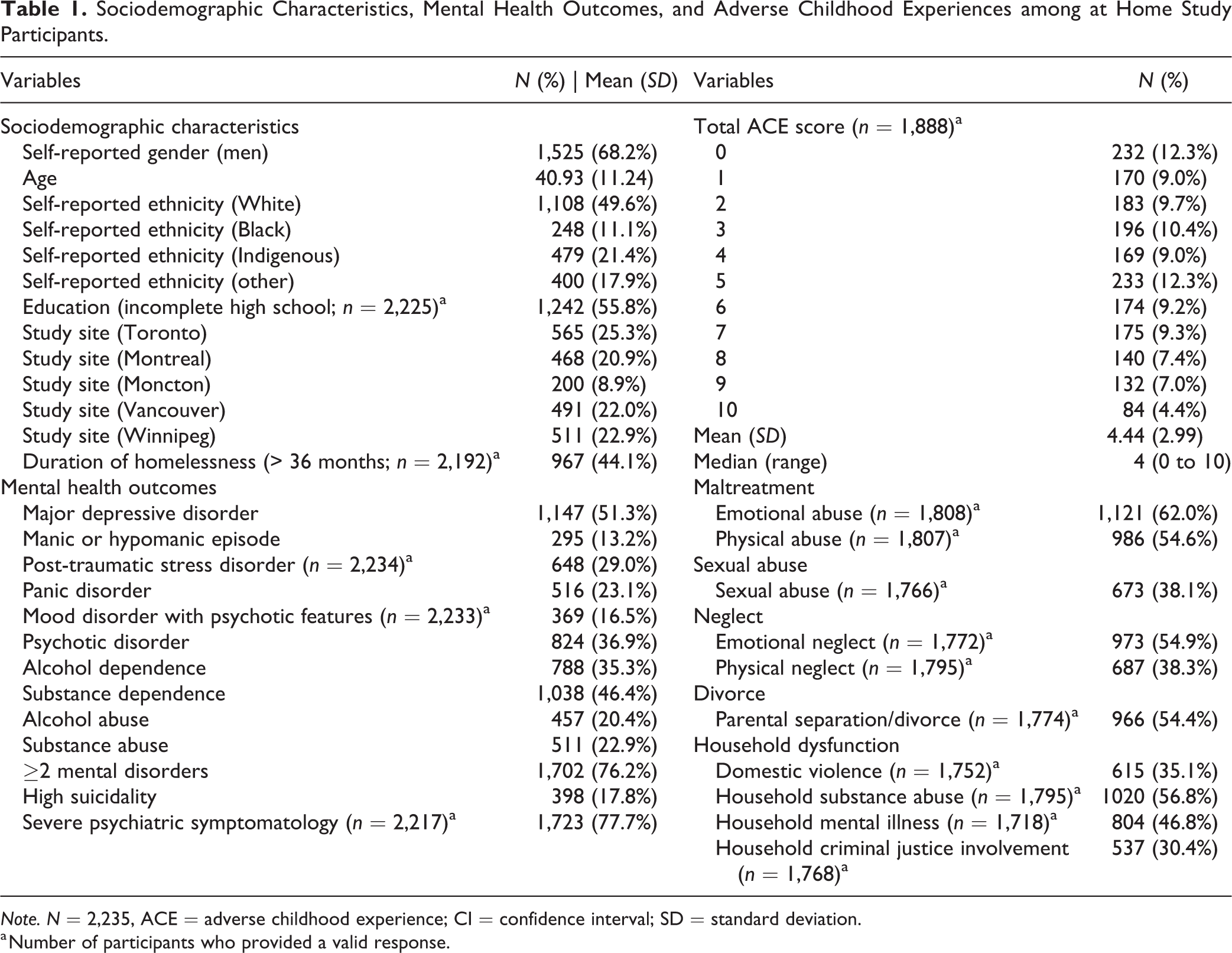
Note. N = 2,235, ACE = adverse childhood experience; CI = confidence interval; SD = standard deviation.
a Number of participants who provided a valid response.
Descriptive summaries of ACE exposure, mental health outcomes, and covariates were generated using the observed data. Comparisons of these variables between gender groups were conducted using Pearson chi-square tests.
Multiple Imputation by Chained Equations was used to infer missing data pertaining to PTSD (1 missing), mood disorder with psychotic features (2 missing), CSI (18 missing), and individual ACE categories (443 to 531 missing); 100 data sets were generated to improve estimation precision and minimize Monte Carlo error. All variables used in the present analyses were included in the imputation process.
Multivariable logistic regression analyses were used to create 2 models. Model 1 assessed the adjusted associations between total ACE score with mental health outcomes. Model 2 assessed the adjusted associations between each of the 5 ACE dimensions with mental health outcomes. Models were adjusted for self-reported gender, age, ethnicity (White, Black, Indigenous, or other), and study site (Toronto, Montreal, Moncton, Vancouver, or Winnipeg). To study gender-specific associations, the models were recreated for data sets stratified by gender (men and women).
All P values are 2-sided. No adjustments for multiple testing were applied to avoid type II error rate inflation given the exploratory nature of the study. 30,31 Moreover, in accordance with current guidelines, effect sizes are reported as adjusted odds ratios (AORs) with 95% confidence intervals (CIs). 32 All analyses were conducted using R-3.6.3 and STATA 16.
All procedures involving human participants were approved by the Research Ethics Board of St Michael’s Hospital in Toronto. Written informed consent was obtained from all participants.
Results
Table 1 presents a summary of baseline sociodemographic characteristics, outcomes, and ACE exposure for the full AH/CS sample. In the overall baseline sample, the majority of participants were men (68.2%) and almost half were White (49.6%); the mean age at enrollment was 40.93 years (standard deviation [SD]: 11.24). Additionally, 55.8% of participants did not complete high school and 44.1% had experienced a lifetime duration of homelessness exceeding 36 months. The least common ACE reported was having household criminal justice involvement (30.4%), while the most common was emotional abuse (62.0%); 38% of participants had been sexually abused. Over half (59%) of participants experienced 4 or more ACEs and only 12.3% of participants had never experienced an ACE. The mean total ACE score was 4.44 (SD: 2.99).
The AOR and 95% CI for associations between mental health outcomes with total ACE score (Model 1) and ACE dimensions (Model 2) are presented in Table 2. Model 1 shows that total ACE score was positively associated with the following mental health outcomes: major depressive disorder (AOR, 95% CI: 1.12, 1.08 to 1.16), PTSD (1.20, 1.16 to 1.25), panic disorder (1.10, 1.05 to 1.14), mood disorder with psychotic features (1.12, 1.07 to 1.18), alcohol dependence (1.12,1 .08 to 1.16), substance dependence (1.11, 1.07 to 1.14), co-occurring mental disorders (1.13, 1.08 to 1.18), high suicidality (1.15, 1.10 to 1.20), and severe psychiatric symptomatology (1.20, 1.15 to 1.25). Total ACE score was negatively associated with psychotic disorder (0.90, 0.87 to 0.93).
Logistic Regression Analyses for Mental Health Outcomes Based on Total ACE Scores and ACE Dimensions in the Overall Sample.a
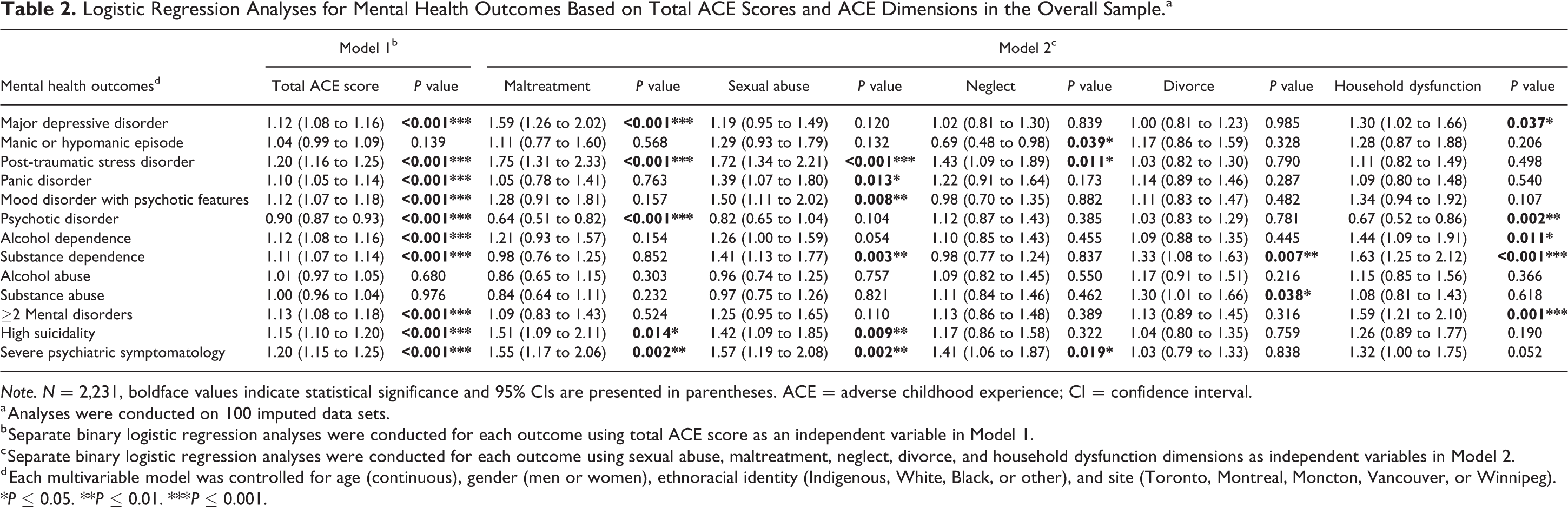
Note. N = 2,231, boldface values indicate statistical significance and 95% CIs are presented in parentheses. ACE = adverse childhood experience; CI = confidence interval.
a Analyses were conducted on 100 imputed data sets.
b Separate binary logistic regression analyses were conducted for each outcome using total ACE score as an independent variable in Model 1.
c Separate binary logistic regression analyses were conducted for each outcome using sexual abuse, maltreatment, neglect, divorce, and household dysfunction dimensions as independent variables in Model 2.
d Each multivariable model was controlled for age (continuous), gender (men or women), ethnoracial identity (Indigenous, White, Black, or other), and site (Toronto, Montreal, Moncton, Vancouver, or Winnipeg).
*P ≤ 0.05. **P ≤ 0.01. ***P ≤ 0.001.
Model 2 demonstrates that specific ACE dimensions were associated with specific mental health outcomes. Maltreatment was positively associated with major depressive disorder (AOR, 95% CI: 1.59, 1.26 to 2.02), PTSD (1.75, 1.31 to 2.33), high suicidality (1.51, 1.09 to 2.11), and severe psychiatric symptomatology (1.55, 1.17 to 2.06) and negatively associated with psychotic disorder (0.64, 0.51 to 0.82). Sexual abuse was positively associated with PTSD (1.72, 1.34 to 2.21), panic disorder (1.39, 1.07 to 1.80), mood disorder with psychotic features (1.50, 1.11 to 2.02), substance dependence (1.41, 1.13 to 1.77), high suicidality (1.42, 1.09 to 1.85), and severe psychiatric symptomatology (1.57, 1.19 to 2.08). Neglect was positively associated with PTSD (1.43, 1.09 to 1.89) and severe psychiatric symptomatology (1.41, 1.06 to 1.87) and negatively associated with manic or hypomanic episode (0.69, 0.48 to 0.98). Parental separation/divorce was positively associated with substance dependence (1.33, 1.08 to 1.63) and substance abuse (1.30, 1.01 to 1.66). Finally, household dysfunction was positively associated with major depressive disorder (1.30, 1.02 to 1.66), alcohol dependence (1.44, 1.09 to 1.91), substance dependence (1.63, 1.25 to 2.12), and co-occurring mental disorders (1.59, 1.21 to 2.10) and negatively associated with psychotic disorder (0.67, 0.52 to 0.86).
The comparisons of the prevalence of specific mental health outcomes and ACE exposure between gender groups are presented in Supplemental Appendix Table 2. Women were more likely to have been exposed to all ACE categories, with the exception of parental separation/divorce, household substance abuse, and household criminal justice involvement.
The results for the gender-stratified analyses are presented in Table 3. The following summarizes the most significant association differences observed between men and women. For men, maltreatment was uniquely positively associated with high suicidality (AOR, 95% CI: 1.84, 1.23 to 2.77) and severe psychiatric symptomatology (1.61, 1.16 to 2.24) and uniquely negatively associated with psychotic disorder (0.64, 0.49 to 0.85); sexual abuse was uniquely positively associated with panic disorder (1.45, 1.05 to 2.01), substance dependence (1.52, 1.16 to 1.99), high suicidality (1.39, 1.01 to 1.93), and severe psychiatric symptomatology (2.00, 1.35 to 2.88); neglect was uniquely positively associated with PTSD (1.51, 1.08 to 2.10) and uniquely negatively associated with manic or hypomanic episode (0.63, 0.41 to 0.96); household dysfunction was uniquely positively associated with major depressive disorder (1.40, 1.05 to 1.86) and alcohol dependence (AOR: 1.42, 1.04 to 1.95) and uniquely negatively associated with psychotic disorder (0.64, 0.49 to 0.86). For women, sexual abuse was uniquely positively associated with mood disorder with psychotic features (1.83, 1.07 to 3.14); parental separation/divorce was uniquely positively associated with substance dependence (AOR: 1.73, 1.19 to 2.52).
Gender-specific Associations between Total ACE Scores and ACE Dimensions with Mental Health Outcomes.a
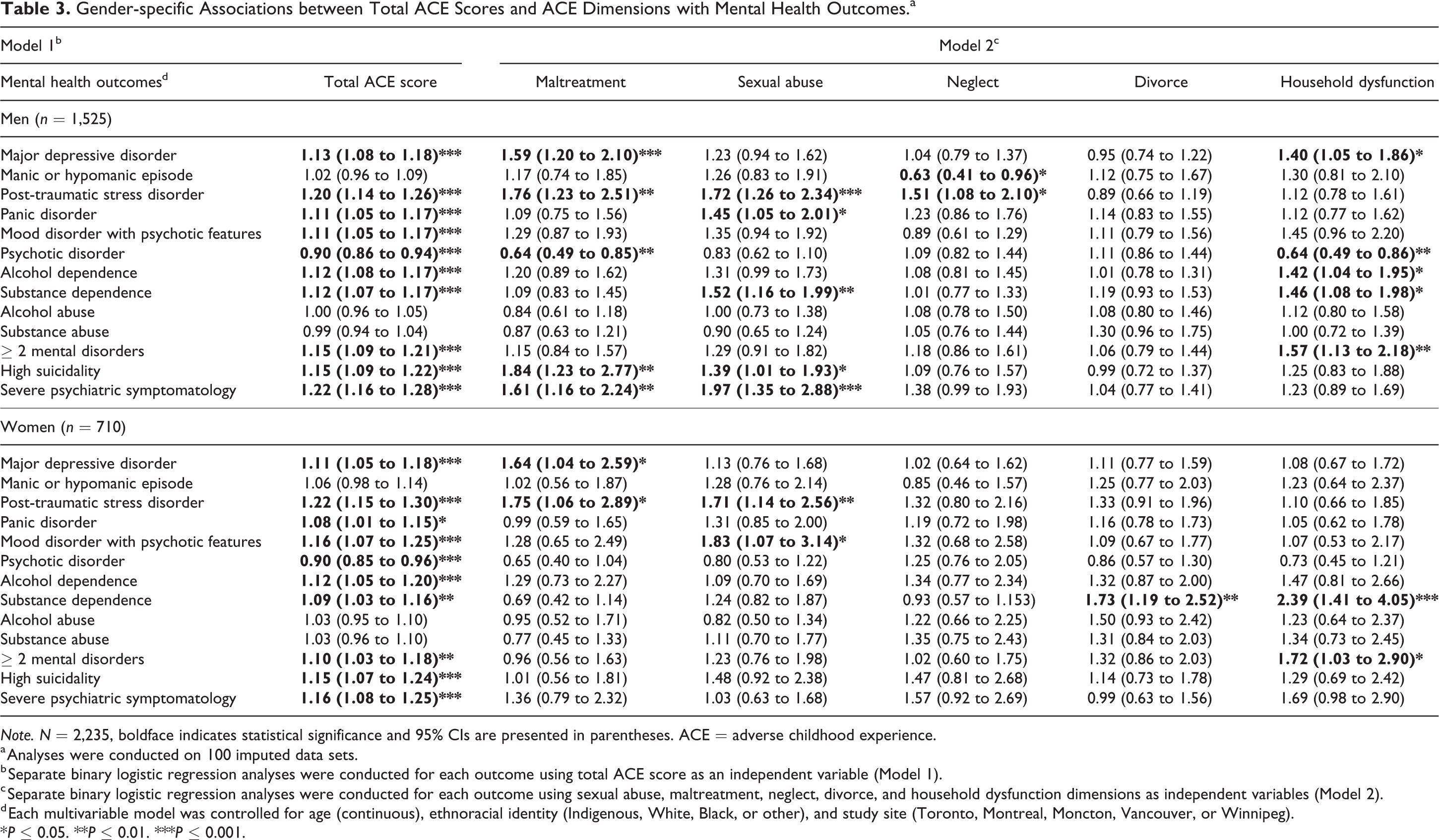
Note. N = 2,235, boldface indicates statistical significance and 95% CIs are presented in parentheses. ACE = adverse childhood experience.
a Analyses were conducted on 100 imputed data sets.
b Separate binary logistic regression analyses were conducted for each outcome using total ACE score as an independent variable (Model 1).
c Separate binary logistic regression analyses were conducted for each outcome using sexual abuse, maltreatment, neglect, divorce, and household dysfunction dimensions as independent variables (Model 2).
d Each multivariable model was controlled for age (continuous), ethnoracial identity (Indigenous, White, Black, or other), and study site (Toronto, Montreal, Moncton, Vancouver, or Winnipeg).
*P ≤ 0.05. **P ≤ 0.01. ***P ≤ 0.001.
Discussion
To our knowledge, this is the first study to examine associations between ACEs and mental health outcomes in a large national sample of homeless adults with mental illness. Total ACE score in this study was a strong predictor of several mental health outcomes and severity of psychopathology. Furthermore, using dimensions of early childhood adversities in the analyses produced more nuanced findings and revealed unique associations with specific mental health outcomes.
The ACE dimensions identified in this study are in congruence with those obtained from a CDC factorial analysis of ACE data available from 27,545 adults from the U.S. Behavioral Risk Factor Surveillance System (BRFSS) survey. 33 It is important to note, though, that the ACE module used in the 2010 BRFSS survey did not include questions assessing emotional and physical neglect. This dimensional approach to studying associations of ACEs with later-life outcomes has been implemented before, generating statistically superior models than those constructed with cumulative and selective ACE approaches. 34
The overall prevalence of ACEs among our national sample of homeless adults with mental illness was very high. The mean ACE score was 4.4, with 58.6% and 28.1% of participants having experienced 4 or more and 7 or more ACEs, respectively. These numbers are almost 5-fold and 32-fold higher than those of the original ACE study, with only 12% and 0.9% of housed participants having experienced 4 or more and 7 or more ACEs, respectively. 5 Several past studies have reported associations between cumulative ACEs and poor mental health outcomes among homeless adults. 9,35,36 However, evidence around associations between specific ACEs and specific mental health outcomes among homeless adults has been lacking.
The distinct associations between ACE dimensions and mental health outcomes reported in our study are in line with those previously reported for the general population. Several past studies—including meta-analyses and prospective studies—have also found that childhood sexual abuse is associated with a wide variety of psychopathologies, including PTSD, anxiety disorders, substance use disorders, and suicidality. 37,38 A meta-analysis also demonstrated strong associations of nonsexual childhood maltreatment with depressive disorders and suicidality. 15 The same study revealed an additional association with drug use, which might be attributed to omitted-variable bias given the strong associations between childhood maltreatment and other ACEs. A cross-sectional study in Brazil also found a strong association between childhood neglect and PTSD, even after accounting for childhood maltreatment subtypes. 39
Several studies have repeatedly shown that experiences of household dysfunction are risk factors for mood disorders and substance use disorders. 34,40 Contrary to past reports, our results demonstrate that maltreatment and household dysfunction are negatively associated with psychotic disorders. 41 One possible explanation is that ACEs and psychotic disorders are both strong risk factors for homelessness. 10,42 This could lead to a scenario in which ACE prevalence is lower among homeless people with psychotic disorders compared to homeless individuals without psychotic disorders.
Our study also uncovered gender-specific insights surrounding specific ACEs and mental health outcomes among homeless individuals. It has been well-documented in the literature that women are more likely than men to experience maltreatment, sexual abuse, and neglect. 43,44 This continues to hold true in this national sample of homeless adults. Higher ACE prevalence among homeless women is indicative of gendered vulnerability to early adversities and points to a need for more ACE prevention initiatives. Our gender-stratified analyses also reveal 2 patterns in regard to distinct gendered associations between ACE dimensions and mental health outcomes. The first is that men were more likely to demonstrate a relationship between maltreatment, sexual abuse, and household dysfunction and externalizing disorders and severe psychiatric symptomatology. The second is that associations with sexual abuse were present for a wider range of mental disorders for men in this study. These gendered association differences might be attributed to factors such as differing help-seeking tendencies and coping mechanisms between men and women. 45,46 Biological mechanisms such as differences in responses to stress and trauma between males and females might also play a role in observed association differences. 47
Our findings have important implications for policy makers, health care professionals, and service providers. Understanding the distinct associations between ACE dimensions and specific later mental health sequelae will aid early identification and appropriate treatment of mental health conditions among the homeless population. Given the high prevalence of ACEs among homeless adults, all practitioners working with this population should be trained to deliver trauma-informed care. To contextualize such care, ACE screening could be integrated into standard of care for this population. 48 However, ACE screening might be potentially distressing for some homeless clients, particularly those who experience multiple stigmatized identities. 49 Those engaged in screening efforts should use culturally sensitive tools, be appropriately trained, and have the capacity to refer clients to evidence-based services and interventions.
The high frequency of early adversities among this population should also inform how service providers engage and support homeless individuals. One intervention embodying trauma-informed principles is HF, which prioritizes client respect, strengths, choices, and safety by offering permanent housing without preconditions. 50 Still, many services and interventions for people experiencing homelessness such as HF are gender neutral. The results from this study reveal gendered vulnerability to early adversities for homeless men and women that should be considered by service providers. 21
The tremendous burden of ACEs among the homeless population places an emphasis on the primary prevention of early adversities. Early childhood adversity interferes with normal development and increases risk of exposure to future adversities, thereby setting the stage for poor outcomes across the life course, including homelessness and poor health. 51 Specific interventions such as the Triple-P Program and the Nurse-Family Partnership have helped expose at-risk children to safe environments and promote positive later-life outcomes. 52,53 More funding must be made available to such evidence-based interventions. The occurrence of ACEs is also tied to structural factors including poverty, systemic racism, intergenerational trauma, and housing instability. 54 -56 Given the significant personal, social, and economic consequences of ACEs, governments and policy makers should prioritize addressing the social factors driving ACEs. 12 Altogether, broad screening, prevention, and treatment efforts throughout the life course are necessary to alleviate ACE-associated sequelae, especially for people experiencing homelessness.
Limitations
First, this study is cross-sectional and cannot elucidate the causal pathways between ACE dimensions and studied mental health outcomes. Although ACEs occur early in life by definition, we cannot ascertain the temporal precedence of ACE exposure over onset of homelessness and mental illness as this information was not available. Second, mediators and moderators in the complex relationship between ACEs and mental health such as social support, perceived stress, and resilience should be further explored through future studies. Third, there are likely other mental health outcomes associated with ACEs that were not investigated in this study. For example, the MINI does not include most personality disorders—diagnoses that are prevalent among homeless adults and known to be associated with ACEs. 57,58 Fourth, this study used DSM-IV criteria given that the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition did not exist during the time of data collection. The criteria for several mental disorders such as substance-related disorders have changed between the 2 editions. Fifth, the associations between some ACE dimensions and mental health outcomes were relatively weak. This may be attributed to the co-occurrence of ACE dimensions and other risk factors such as victimization and traumatic brain injury that contribute to poor mental health outcomes among homeless individuals. 59,60 Finally, the findings from this study cannot be generalized to homeless adults with mental illness in other sociocultural contexts. Future studies should examine the ethnoracial-specific impact of ACEs, particularly for Indigenous individuals given that they are disproportionately represented in the Canadian homeless population. 61 Continuous oppression and forced assimilation of Indigenous individuals have resulted in high rates of early trauma and mental disorders among this population. 62 More research should also explore the impact of ACEs among gender nonconforming individuals, who are particularly vulnerable and overrepresented in the homeless population. 63,64
Conclusion
In the present study using both cumulative and dimensional ACE approaches, we identified unique associations between specific ACE dimensions and specific mental health outcomes among homeless adults with mental illness. Furthermore, gender-specific analyses revealed unique associations for men and women. These findings highlight the need for more research into the mechanisms underlying gender-specific associations of early adversities and mental health outcomes. A more precise and nuanced understanding of ACEs and their later mental health consequences will help inform more tailored screening, prevention, and treatment endeavors for this vulnerable population. Altogether, this study offers novel insights into the complex relationship between ACEs and lifelong mental health outcomes among the homeless population.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_0706743721989158 - Overall and Gender-specific Associations between Dimensions of Adverse Childhood Experiences and Mental Health Outcomes among Homeless Adults: Associations Générales et Sexospécifiques Entre les Dimensions des Expériences Défavorables de L’enfance et les Résultats de Santé Mentale Chez les Adultes Sans Abri
Supplemental Material, sj-docx-1-cpa-10.1177_0706743721989158 for Overall and Gender-specific Associations between Dimensions of Adverse Childhood Experiences and Mental Health Outcomes among Homeless Adults: Associations Générales et Sexospécifiques Entre les Dimensions des Expériences Défavorables de L’enfance et les Résultats de Santé Mentale Chez les Adultes Sans Abri by Michael Liu, Cilia Mejia-Lancheros, James Lachaud, Eric Latimer, Tim Aubry, Julian Somers, Jino Distasio, Vicky Stergiopoulos and Stephen W. Hwang in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
ML, SWH, CML, and JL conceived of and designed the study. ML performed the analysis, interpreted the results, and prepared the first manuscript draft. CML and JL provided guidance on the analysis and structuring of the first manuscript draft. All authors critically reviewed the manuscript. All authors contributed to and approved the final manuscript. The data that support the findings of this study are available on request from the corresponding author, SWH. The funding institutions had no role in the collection, analysis, and interpretation of the data, nor in the preparation, revision, or approval of the present manuscript. The views expressed in this publication are solely those of the authors.
Acknowledgments
The authors extend their sincere gratitude to all At Home/Chez Soi participants whose willingness to share their experiences and stories made this project possible. The authors also thank the At Home/Chez Soi project teams, site coordinators, and service providers for their tireless contributions to the study design, implementation, and follow-up. Finally, the authors acknowledge Rick Wang for his kind support with data preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Mental Health Commission of Canada, the Ontario Ministry of Health and Long-Term Care (HSRF 259), and the Canadian Institutes of Health Research (MOP-130405 and FDN-167263).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.