
Abstract
Objectives:
Exposure to adverse childhood experiences (ACEs) is associated with increased risk of criminal justice involvement and repeated victimization among homeless individuals. This study aimed to (1) examine whether the relationship between cumulative ACE score and odds of experiencing criminal justice involvement and victimization remains significant over time after receiving the Housing First (HF) intervention and (2) investigate the moderating effect of cumulative ACE score on the effectiveness of the HF intervention on the likelihood of experiencing these outcomes among homeless individuals with mental illnesses.
Methods:
We used longitudinal data over the 2-year follow-up period from the At Home/Chez Soi demonstration project that provided HF versus treatment as usual (TAU) to homeless adults with mental illness in five Canadian cities (N = 1,888).
Results:
In all 4 follow-up time points, the relationship between cumulative ACE score and both outcomes remained significant, regardless of study arm (HF vs. TAU) and other confounding factors. However, cumulative ACE score did not moderate intervention effects on odds of experiencing either outcome, suggesting that the effectiveness of HF versus TAU, with regard to the odds of being victimized or criminal justice involvement, did not differ by cumulative ACE scores over the course of study.
Conclusions:
Findings suggest that providing services for homeless individuals with mental illness should be trauma informed and include specialized treatment strategies targeting the experience of ACEs and trauma to improve their treatment outcomes. An intensive approach is required to directly address the problem of criminal justice involvement and victimization in these individuals.
Introduction
Homeless individuals with mental illnesses are at greater risk of criminal justice involvement (CJI) and victimization compared to their housed counterparts. 1 Exposure to adverse childhood experiences (ACEs), such as abuse and neglect, plays a critical role in subsequent CJI (e.g., criminal activities, arrest, incarceration) 2,3 and repeated victimization 4,5 among homeless individuals. Our recent systematic review of 20 studies on the association between childhood maltreatment and subsequent CJI and victimization among homeless individuals indicated that experiences of childhood maltreatment, and in particular childhood physical and sexual abuse, are associated with increased risk of both CJI and victimization among homeless persons. 6 This association was significant regardless of important factors such as demographic characteristics (e.g., age, ethnicity, gender), diagnosis of psychiatric disorders, problems with family, age first living on own, deviant subsistence strategies, deviant peers, and substance use. 6
Various factors may contribute to these heightened risks. In particular, one study found that ACEs was the primary reason for running away from home and early homelessness, 7 which may consequently elevate the risk of involvement with antisocial peers, substance abuse, and engaging in survival behaviors/subsistence strategies among homeless individuals. 8,9 However, the strength and nature of the relationship between ACEs and the risk of CJI and victimization among homeless individuals with mental illnesses is not clear. Many cases of CJI among homeless persons, particularly for homeless individuals with mental illness, are attributable to the visibility of homelessness rather than the volitional violation of any law or regulation. Therefore, there is a need for longitudinal studies that investigate the change in CJI and victimization among homeless individuals with histories of ACEs after receiving housing. 1,10,11
A recent study using the baseline data from the At Home/Chez Soi project (N = 1,888) indicated that the rates of both CJI and victimization are significantly higher among homeless individuals with mental illness who have a history of exposure to ACEs. 12 The effect of cumulative ACE score (total ACE score) on the 2 outcomes was significant after controlling for sociodemographic factors, duration of homelessness, and diagnoses of mental illnesses 12 ; the only exception was the relationship between cumulative ACE score and CJI when controlled for the diagnoses of post-traumatic stress disorder (PTSD) and substance dependence. 12 The first aim of this study was to extend these findings by examining the impact of cumulative ACE score on the odds of experiencing CJI and victimization among homeless individuals with mental illness over a period of 2 years after receiving the Housing First (HF) intervention.
The Effect of HF on Victimization and CJI in Homeless Individuals
HF is a recovery-oriented and complex intervention to ending homelessness in individuals with mental health problems. 13 –17 HF has been found to increase housing stability and reduce some adverse outcomes among individuals who are considered difficult to house. 15 –18 A recent review of 31 studies on the effectiveness of HF for homeless populations indicated that HF is strongly successful in improving housing retention and reducing services usage (e.g., emergency shelters, emergency health services, and criminal justice system). 18 However, its utility for reducing chronic or long-term homelessness, and associated adverse outcomes, such as substance use, is unclear, mixed, and inconclusive. 18,19 In particular, limited work has been done to examine the effectiveness of HF intervention on CJI and victimization outcomes.
We are not aware of any published study that examined the impact of HF on victimization outcomes among homeless individuals. With regard to CJI outcomes, a recent systematic review indicated that HF has little impact on reduction of CJI and did not systematically address criminogenic needs other than substance abuse in homeless persons with a mental illness. 20 However, results of studies using other selected subsamples of homeless individuals indicated that HF exposure decreases some of the CJI outcomes. For example, HF reduced jail time and bookings in chronically homeless individuals with severe alcohol problems, 21 arrests and incarcerations in persons with chronic homelessness and work-limiting disabilities, 22 the amount of criminal activity in individuals with chronic homelessness, 23 and number of days incarcerated for homeless individuals with severe mental disabilities. 24 Using linked administrative data, previous findings from the At Home/Chez Soi project in Vancouver site (n = 297) revealed that randomization to scattered site HF was associated with 70% fewer convicted offenses than treatment as usual (TAU) over 2 years of follow-up; however, the effect of receiving congregate HF versus TAU was only marginally significant. 25 Results from the At Home/Chez Soi Toronto site (n = 197) indicated that the reduction of self-reported arrests in individuals who received HF supported by an assertive community treatment team (HF + ACT) was significantly higher compared to TAU at the 24-month follow-up assessment. 26 Neither of these studies incorporated a focus on ACEs or cumulative trauma.
It has been reported that psychiatric patients with ACEs respond poorly to standard treatment strategies and may not sufficiently benefit from the traditional mental health treatment. 27,28 Therefore, it is important to examine the effect of ACEs on health outcomes in the evaluation of services and supports for homeless individuals and particularly for those individuals also living with mental illness.
This Study
This study aimed to examine (1) whether the relationships between cumulative ACE score and the odds of experiencing CJI and victimization remain significant over time after receiving the HF intervention and (2) whether cumulative ACE score moderates the impact of HF intervention on the odds of experiencing CJI and victimization among homeless individuals with mental illnesses. The results of this study will inform models of care in the process of providing services for homeless individuals to improve treatment outcomes and reduce the incidence of CJI and victimization among homeless individuals with mental illnesses.
Methods
Participants
This study was part of the At Home/Chez Soi project, which included 2,255 homeless individuals with mental illnesses. 13 Participants were recruited in five Canadian cities (i.e., Toronto [25%], Vancouver [22%], Winnipeg [22%], Montreal [20%], and Moncton [9%]) from a wide variety of settings, including the street, shelters, day centers, and hospital referrals between October 2009 and June 2011. The inclusion criteria were (1) being over 18 or 19 years of age, depending on the province; (2) being absolutely homeless or precariously housed with a recent history of homelessness; and (3) being diagnosed with a serious mental disorder at the time of enrollment. Participants were excluded from the study if (1) they had no legal status as a Canadian resident, landed immigrant, refugee, or refugee claimant as; and/or (2) were currently a client of another intensive case management (ICM) or assertive community treatment (ACT) team. ICM and ACT are community-based mental health teams, which provide psychiatric treatment, rehabilitation, and social integration and support services to individuals with severe mental illnesses. Homeless people with higher needs receive ACT, and people with moderate needs receive ICM.
Participants who did not provide any responses on the ACEs questionnaire items (n = 367; 28% female) were excluded from this study (16% of the total sample). Thus, our final sample included 1,888 participants. Analyses indicated that excluded participants showed a lower percentage of alcohol and drug dependence (χ2 = 4.33, P < 0.05; χ2 = 5.05, P < 0.05, respectively) and a higher percentage of psychotic disorders (χ2 = 5.08, P < 0.05) compared to those who provided responses to the ACEs questionnaire. However, they were not significantly different from others in terms of other sociodemographic and clinical characteristics including duration of homelessness.
Measures
Sociodemographic and background information
Sociodemographic characteristics (age, gender, ethnicity, education level, and marital status) and duration of homelessness (lifetime homelessness, longest single period of homelessness, and age at first homelessness) were collected at baseline with the Demographics, Housing, Vocational, and Service Use History questionnaire, which was developed for the demonstration project. 13 The Mini-International Neuropsychiatric Interview (MINI) 6.0 was used during enrollment to assess the presence of Axis I psychiatric disorders. 29
ACEs
The ACEs questionnaire 30 retrospectively assesses exposure to 10 types of childhood adversity that occurred before the age of 18, including neglect (physical and emotional), abuse (emotional, physical, and sexual), and household/familial dysfunction (household mental illness, household substance abuse, mother treated violently, parental separation/divorce, incarcerated family members). The ACEs questionnaire provides dichotomous (yes/no) responses for each item. To create a cumulative ACEs score, responses from all 10 items on the questionnaire were summed. 30
CJI and victimization
The sections on use of justice services, arrest, court appearances, and victimization of the Health, Social, and Justice Service Use (HSJSU) inventory, which was also developed for the study, 13 were used to assess the occurrence of CJI and victimization in the past 6 months. Two dichotomous dependent variables were created: CJI and victimization. CJI referred to any involvement in the past 6 months (vs. no involvement) and was computed aggregating the presence/absence of detention by police without being held in a cell, held in a police cell for 24 hours or less, arrest, and court appearance. Any victimization in the past 6 months (vs. no victimization) was computed from aggregating the scores for having been victim of robbery, threatened, victim of a physical assault, and victim of a sexual assault.
Procedure
We used data from all five cities for all participants who provided a response on the ACEs and written informed consent to the full study. In-person interviews were conducted at baseline and at 6-month intervals thereafter for 21 or 24 months (4 follow-ups). The MINI was completed at enrollment; the HSJSU, demographic and background information were collected at baseline and 4 follow-ups every 6 months. Participants completed the ACEs questionnaire at the 18-month follow-up interview. The assessment of fidelity to the HF model achieved a high level of adherence across 5 sites. 31 Ethics approval was obtained from all affiliated universities and health-care organizations nationally and for each site. For a detailed description of study procedures, participant characteristics, and outcomes of the study, please see. 13,32
Of 1,888 participants included in this study, 1,111 were randomized to the HF intervention and 777 to TAU. There were no significant differences between groups on major study variables. 32 Participants in the HF group were provided with housing and either ICM or ACT based on their level of need (i.e., higher-need participants received ACT).
The rate of attrition in the At Home/Chez Soi project was 14% excluding 79 people known to have died. 33 Other reasons included not being able to locate the participant and participant refusal. Attrition was significantly lower in HF (8% vs. 21% in TAU), in 1 site (Montreal) than elsewhere, among those with substance dependence (13% vs. 18%) than without, and among those enrolled earlier in the study. 33 Results suggested that the study factors were more important determinants of retention compared to participant characteristics. 33
Data Analyses
All statistical analyses were conducted using SPSS for Windows Version 24.0. Data preparation included standardization of continuous variables. Categorical variables were coded as 0 and 1. Of 1,888 participants, 336 persons had some missing items for certain categories of ACEs with most of them having only missed 1 (57.4%) or 2 to 3 (16.7%) of 10 items. We did a sensitivity analysis similar to the primary ACE study 30 in which all analyses were conducted with (i.e., where missing information for a category of ACE was considered as no exposure) and without the persons who did not respond to certain questions about ACEs. We found that our results are not affected by the decision to exclude these individuals. Therefore, we decided to maintain these individuals in our analyses.
We used independent samples t test (for age at enrollment and cumulative ACE scores) and χ2 test (for dichotomized variables) to test group differences in baseline characteristics of HF and TAU samples.
To address the first aim of the study, a series of multivariate logistic regression analyses were conducted using cumulative ACE score as the predictor and CJI, and victimization outcomes in each postintervention assessment follow-up as the dependent variable, adjusting for potential confounders (sociodemographics, duration of homelessness, and diagnoses of psychiatric disorders). The main aim here was to assess the strength of relationship between cumulative ACE score and outcome measures at individual follow-up time points. We first examined the bivariate association of each factor with each outcome. Each candidate predictor variable associated with a measure of baseline CJI and victimization outcome at P < 0.10 in bivariate analyses was retained and included in multivariate logistic regression (age, which was dichotomized based on being in an older age-group, gender, ethnicity, age at first homelessness, lifetime homelessness, and diagnoses of PTSD, alcohol and drug dependence). In addition to these factors, all multivariate logistic regression analyses controlled for study arm (HF = 1 vs. TAU = 0) and baseline CJI and victimization rates.
To address the second aim of the study, we conducted 2 separate logistic generalized estimating equations (GEE) for binary data using an autoregressive correlation structure. GEE accounts for the correlation among repeated measures and examines the relationships between different variables within the model at multiple time points simultaneously. 34 Outcome analyses tested whether the reported CJI and victimization rates differed between HF versus TAU groups over the 2-year period, using outcomes from 6, 12, 18, and 24 months when the interaction of cumulative ACE score and HF intervention (i.e., Cumulative ACE × HF) was entered as the moderator. The main aim of these analyses was to investigate overall impact of the intervention across the full 2-year trial rather than the outcomes at individual time points. Both GEE analyses controlled for cumulative ACE score, baseline CJI and victimization rates, and the same confounding variables in previous analyses.
Results
Results from descriptive analyses indicated that there was no significant difference between the baseline characteristics of participants in HF versus TAU groups, except for the baseline victimization rate which was higher in the TAU group (60% vs. 55%; see Table 1).
Baseline Characteristics for Housing First (HF) and Treatment As Usual (TAU) Samples (N = 1,888).
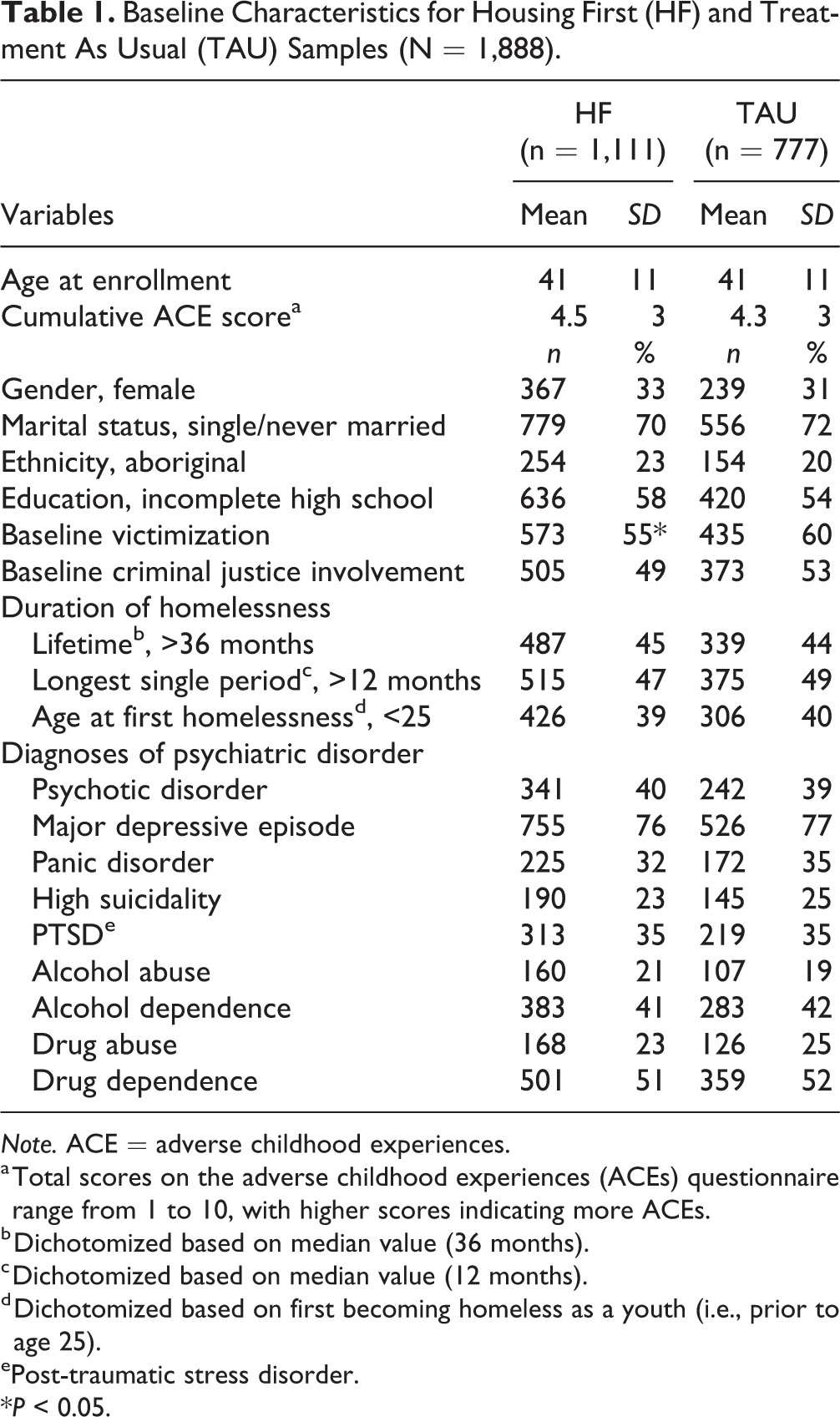
Note. ACE = adverse childhood experiences.
a Total scores on the adverse childhood experiences (ACEs) questionnaire range from 1 to 10, with higher scores indicating more ACEs.
b Dichotomized based on median value (36 months).
c Dichotomized based on median value (12 months).
d Dichotomized based on first becoming homeless as a youth (i.e., prior to age 25).
ePost-traumatic stress disorder.
*P < 0.05.
Table 2 presents the results from multivariate logistic regression analyses. In all follow-up time points, cumulative ACE score was found to have a significant direct relationship with both CJI and victimization outcomes, regardless of study arm (HF vs. TAU), baseline outcome measure (CJI or victimization depending on the model), and other confounding variables. The relationship between cumulative ACE score and victimization appeared stronger compared to CJI at each follow-up assessment.
Logistic Regression Models Predicting Criminal Justice Involvement and Victimization in Each Post-Intervention Assessment Follow-Up Point among Homeless Individuals with Mental Illness.
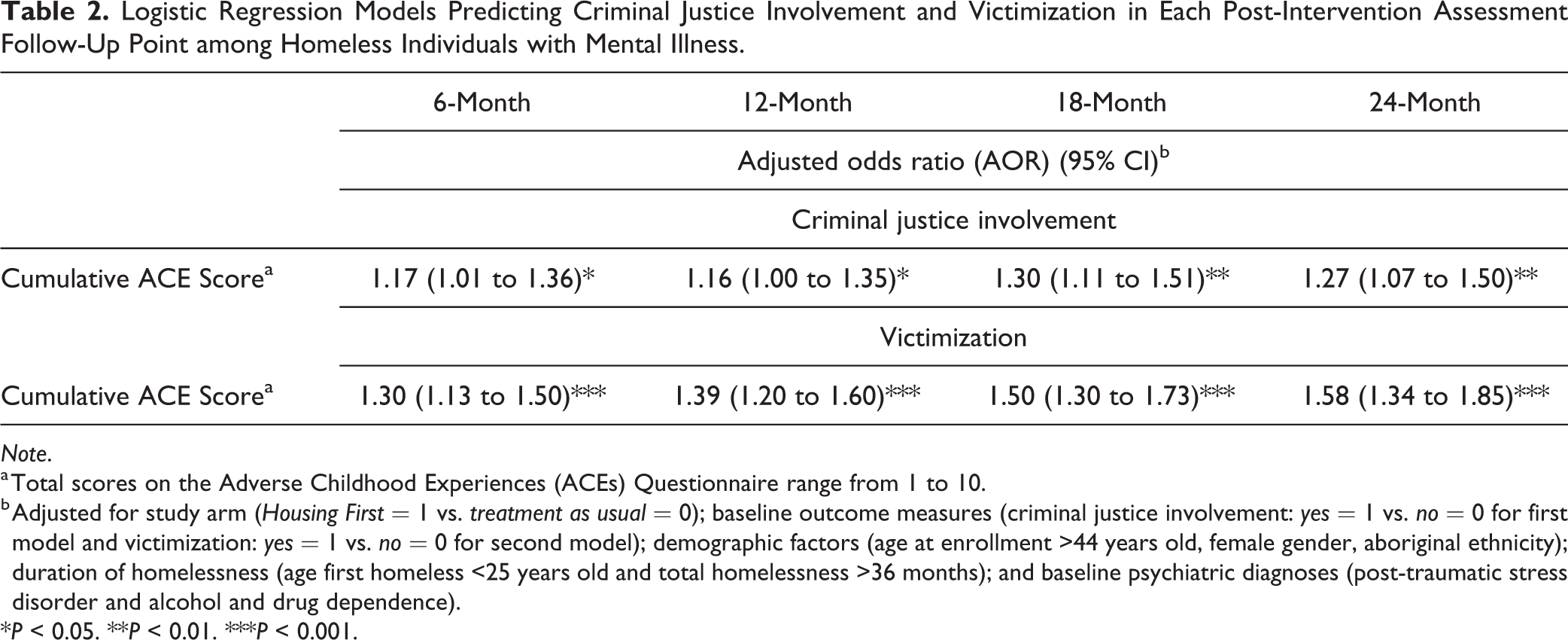
Note.
a Total scores on the Adverse Childhood Experiences (ACEs) Questionnaire range from 1 to 10.
b Adjusted for study arm (Housing First = 1 vs. treatment as usual = 0); baseline outcome measures (criminal justice involvement: yes = 1 vs. no = 0 for first model and victimization: yes = 1 vs. no = 0 for second model); demographic factors (age at enrollment >44 years old, female gender, aboriginal ethnicity); duration of homelessness (age first homeless <25 years old and total homelessness >36 months); and baseline psychiatric diagnoses (post-traumatic stress disorder and alcohol and drug dependence).
*P < 0.05. **P < 0.01. ***P < 0.001.
Table 3 presents the results from GEE models of the intervention effects on the CJI and victimization outcomes when the moderator variable (i.e., Cumulative ACE Score × HF) was included in the analysis. Cumulative ACE score did not moderate intervention effects on odds of either CJI and victimization, suggesting that the effectiveness of HF versus TAU, with regard to the odds of being victimized or involved in criminal justice system, did not significantly differ by cumulative ACE scores over the 2-year follow-up. However, there was a significant treatment effect on the odds of experiencing victimization over the 24-month follow-up, regardless of confounding factors. That is, the odds of experiencing victimization was significantly reduced by 18% in those receiving HF intervention over 2 years (P = 0.022), regardless of their cumulative ACE scores. No significant treatment effect was found on the odds of CJI over the 24-month follow-up.
Generalized Estimating Equations Predicting Criminal Justice Involvement and Victimization among Homeless Individuals with Mental Illness.
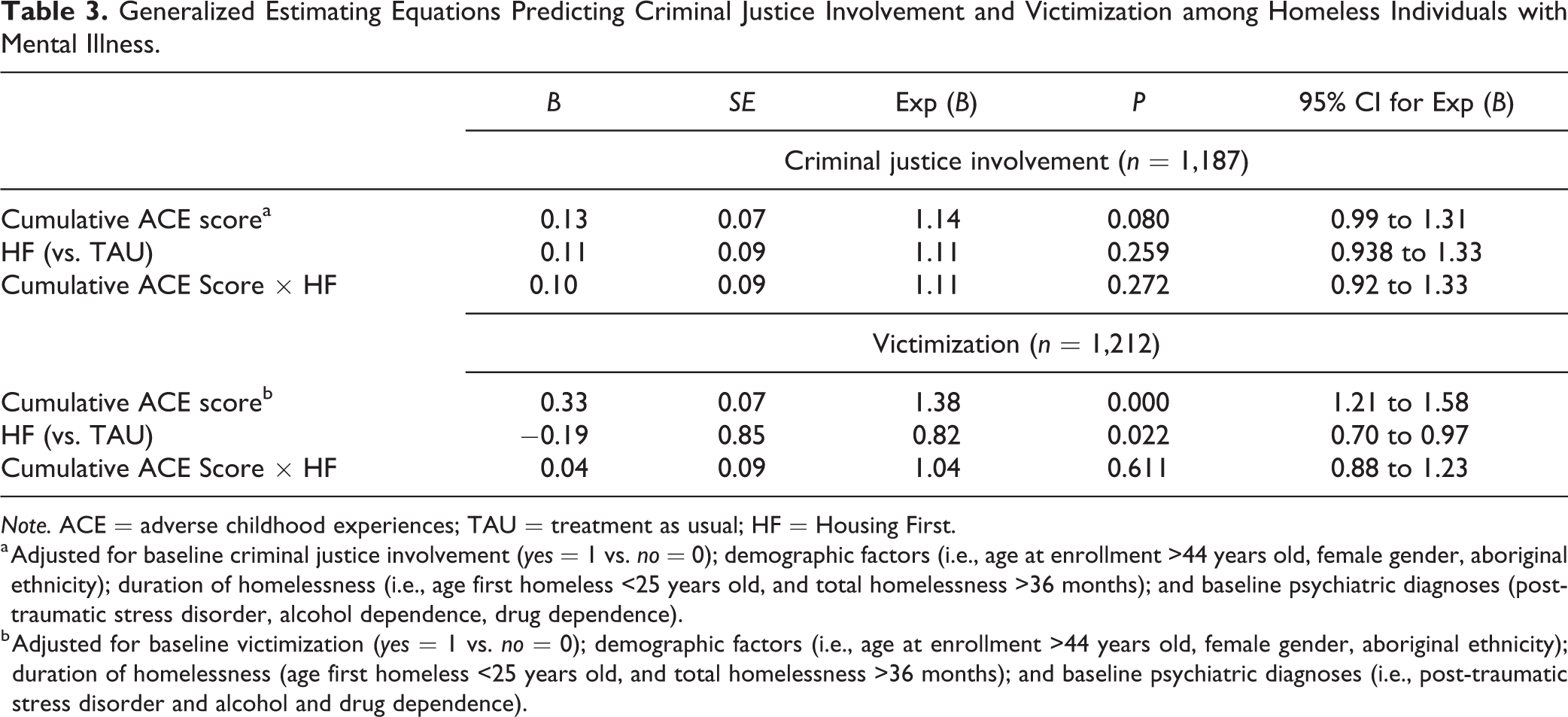
Note. ACE = adverse childhood experiences; TAU = treatment as usual; HF = Housing First.
a Adjusted for baseline criminal justice involvement (yes = 1 vs. no = 0); demographic factors (i.e., age at enrollment >44 years old, female gender, aboriginal ethnicity); duration of homelessness (i.e., age first homeless <25 years old, and total homelessness >36 months); and baseline psychiatric diagnoses (post-traumatic stress disorder, alcohol dependence, drug dependence).
b Adjusted for baseline victimization (yes = 1 vs. no = 0); demographic factors (i.e., age at enrollment >44 years old, female gender, aboriginal ethnicity); duration of homelessness (age first homeless <25 years old, and total homelessness >36 months); and baseline psychiatric diagnoses (i.e., post-traumatic stress disorder and alcohol and drug dependence).
Discussion
Previously reported findings from the At Home/Chez Soi project have indicated that exposure to cumulative ACEs increases the risk of victimization and CJI incidents at baseline before entering the HF intervention. 12 Results from this study extend these findings, indicating that the significant negative effects of ACEs remain persistent over time; in all follow-up points, regardless of study arm (HF vs. TAU), baseline victimization and CJI rates, and other confounding factors. These findings are in line with a growing body of research confirming that a history of ACEs is associated with subsequent higher rates of CJI and victimization among homeless adolescents and adults, regardless of other important factors. 6 These results also provide support for prior studies indicating that exposure to ACEs has an enduring negative effect on brain functioning and physical and mental health 35,36 and that the standard mental health care for individuals with psychiatric illnesses may not be sufficient for those with histories of ACEs (see 27 ). Continued exposure to victimization and CJI may hinder recovery from mental illnesses and inhibit an individual’s ability to transition out of homelessness.
Results from the GEE analyses indicated that participants in HF versus TAU groups did not significantly differ by cumulative ACE score over 2-year follow-up with regard to the odds of victimization or CJI (i.e., no moderating effect). However, among those who received HF intervention we saw a significant reduction (i.e., 18% reduction) in the odds of experiencing victimization over the 2-year follow-up. That is, participants equally benefited from HF intervention regarding their odds of experiencing victimization over 2-year follow-up, regardless of their cumulative ACE score. A plausible explanation for this finding is that the living situations of individuals receiving HF was safer because of them having secure private space as a result of stable housing. Previous research has found individuals in HF programs reporting a greater improvement in quality of life relating to safety. 37,38
No significant treatment effect was found on the odds of experiencing CJI over the 24-month follow-up for those in HF intervention. This finding is somehow in contrast with some previous studies with other subsamples of homeless individuals (e.g., 23,24 ) and the previous findings with the At Home/Chez Soi data in single sites (i.e., in Vancouver 25 and in Toronto 26 ) which reported a moderate improvement in CJI outcomes in those receiving HF compared to TAU. One reason might be the differential assessment methods used in these studies. For example, the study in Vancouver site linked administrative data concerning convicted offenses to the At Home/Chez Soi trial data, 25 and the study in Toronto site used a single question regarding history of arrest in the past 6 months. 26 We used self-report items reporting on any CJI in the past 6 months (including being held in a cell, held in a police cell for 24 hours or less, arrest, and court appearance) which may be the reason for different outcomes. Nonetheless, the odds of experiencing CJI were similarly reduced in both HF and TAU participants over the 2-year follow-up. This similar reduction in the odds of experiencing CJI might be due to the other support and services that individuals in TAU received over the 2 years of the study. Further research is needed to better understand the nature of this relationship in other populations of homeless individuals.
These results need to be considered in the light of several limitations. First, the findings are based on self-report questionnaires, retrospective assessments, and single-reporter accounts. Notably, we were not able to examine documented cases of ACEs or official reports of victimization or CJI (e.g., a police record), which could increase the reliability of participants’ responses. Because of the highly sensitive nature of reporting childhood adversity, victimization, and CJI, they might have been underreported. The retrospective assessment of variables may also have contributed to misreporting. Nevertheless, a validation study on the Vancouver At Home/Chez Soi sample compared self-report and administrative sources of information for health, justice, and social service use and found moderate to almost perfect levels of agreement. 39 Second, we did not assess important characteristics of ACEs, such as severity, duration, or age at occurrence, each of which may affect long-term outcomes. Although the ACEs questionnaire has been widely utilized in previous studies, the cumulative ACE score and its simplicity is subject to several types of criticism. Third, we cannot rule out the possibility that missing data in some items and total score of ACEs were not at random and because of unseen factors, which might potentially affect the outcomes of the study. Finally, the assessment of outcome variables was based on dichotomous variables, which indicated only the absence/presence of victimization or CJI during the past 6 months. Thus, we were unable to differentiate more specific aspects and characteristics of any incident (e.g., relationship with perpetrator, injury).
Despite these limitations, this study is the first investigation of the moderating influence of cumulative ACEs on the efficacy of HF for reducing CJI and victimization outcomes. Particular strengths of the design included using a randomized controlled design with a large sample of individuals with mental illnesses experiencing homelessness.
Although providing housing is a key first step in recovery for homeless individuals, and participants of this study who received the HF intervention also were provided with ACT or ICM services, these services are not necessarily equipped to address a history of ACEs or trauma as well, nor problems with CJI and/or victimization. Altogether, these findings suggest that a more targeted and intensive approach is required to directly address these problems in homeless individuals with mental illnesses.
Findings from this study provide concrete guidance for the development of models of care for homeless adults suggesting that interventions need to expand beyond traditional health services and include (1) screening and ongoing monitoring for acute victimization and trauma, (2) implementing universal trauma-informed practices, 40 (3) providing trauma-informed education and training for staff and health practitioners working within the supported housing context to better identify and respond to the complex needs of homeless individuals with maltreatment histories, and (4) providing specialized treatment strategies targeting the experience of ACEs and trauma for homeless individuals to improve treatment outcomes and reduce the incidence of CJI and victimization among homeless individuals with ACEs histories. Studies using documented cases of ACEs, CJI, and victimization (e.g., police records, data from child welfare services) and investigation of the effect of specific forms of ACEs to improve our understanding of the link between ACEs and these adverse outcomes. Future studies of the mediating and moderating processes in the link between the ACEs and risk of victimization and CJI would be of interest to guide the development of effective trauma-informed intervention programs for this vulnerable population.
Footnotes
Acknowledgments
The authors thank the At Home/Chez Soi Project collaborative at both national and local levels, including Jayne Barker, PhD, Cameron Keller, the late Paula N. Goering, RN, PhD, approximately 40 investigators from across Canada and the United States, 5 site coordinators, numerous service and housing providers, and persons with lived experience of mental illness. Dr. Edalati is supported through a postdoctoral fellowship by the Canadian Institutes of Health Research (CIHR). Dr. Nicholls is also grateful to the CIHR for her New Investigator award and foundation grant and to the Michael Smith Foundation for her Career Scholar award. The team is especially grateful to the study participants who shared their experiences and gave so generously of their time.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Health Canada and the Mental Health Commission of Canada.