
Abstract
Objectives
The COVID-19 pandemic has contributed to a shift from in-person to remote mental health care. While remote care methods have long existed, their widespread use is unprecedented. There is little research about mental health care user and provider experiences with this transition, and no published studies to date have compared satisfaction between these groups.
Methods
Canadian mental health care users (n = 332) and providers (n = 107) completed an online self-report survey from October 2020 to February 2021 hosted by the Canadian Biomarker Integration Network in Depression. Using a mixed-methods approach, participants were asked about their use of remote care, including satisfaction, barriers to use, helpful and unhelpful factors, and suggestions for improvement.
Results
Overall, 59% to 63% of health care users and 59% of health care providers were satisfied with remote care. Users reported the greatest satisfaction with the convenience of remote care, while providers were most satisfied with the speed of provision of care; all groups were least satisfied with therapeutic rapport. Health care providers were less satisfied with the user-friendliness of remote care (P < 0.001) than users, while health care users were less satisfied than providers with continuity of care (P < 0.001). The use of a video-based platform was associated with remote care satisfaction among health care users (P < 0.02), and qualitative responses support the importance of visual cues in maintaining therapeutic rapport remotely. The majority of users (55%) and providers (87%) reported a likelihood of using remote care after the pandemic.
Conclusions
Remote mental health care is generally accepted by both users and providers, and the majority would consider using remote care following the pandemic. Suggestions for improvement include greater use of video, increased attention to body language and eye contact, consistency with in-person care, as well as increased provider training and administrative support.
Introduction
Remote mental health care, also known as telepsychiatry, telemental health, or virtual care, refers to the delivery of mental health services through telephone or video communication methods. Previous research demonstrates good comparability to in-person services, 1 with high patient and provider satisfaction, cost-effectiveness, and similar quality of clinical interaction to face-to-face care.2–4 Patients have reported high satisfaction with the care, convenience, and comfort of remote visits,1,5 although views on technical quality lag slightly behind. 1 An early randomized pilot study of televideo versus in-person psychiatric care in Ontario reported high levels of satisfaction and therapeutic rapport among both patients and providers, though provider satisfaction ratings were significantly lower than those of patients. 6
Until recently, uptake of remote mental health care has been poor3,7 and its use has historically been limited to the subset of health care users who had difficulty attending visits in person. However, the COVID-19 pandemic triggered rapid transitions from in-person to remote services due to associated lockdowns and physical distancing restrictions. Despite an abundance of research on telepsychiatry under conventional circumstances, literature on telepsychiatry during COVID-19 remains scarce and it is unclear how health care users and providers are adapting to this unexpected and largely compulsory shift. Early reports suggest positive uptake8,9 and satisfaction10–13 among users and providers separately. However, no studies to date have directly compared user and provider satisfaction, and there is scant research on Canadian experiences with this transition.14,15
Thus, the aim of this study is to evaluate the experiences of Canadian mental health care users and providers with remote care during COVID-19, including satisfaction, attitudes, barriers, and suggestions for improvement.
Methods
This study was conducted within the Canadian Biomarker Integration Network in Depression (CAN-BIND) 16 and consisted of an online self-report survey that collected both quantitative and qualitative data. Responses were captured between October 8, 2020, and February 4, 2021. All study procedures were approved by the Unity Health Toronto Research Ethics Board (REB #20-177). This mixed-methods study adopted a concurrent triangulation design, 17 using a validating quantitative data model 18 whereby survey responses are validated and enhanced by the inclusion of open-ended questions. Methods and results are reported in line with the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) framework (full checklist in Supplemental Material). 19
Participants
Two participant groups from across Canada were recruited: mental health care users and mental health care providers. Participants in the user group: (1) had been offered an appointment for remote mental health care after March 1, 2020; (2) were ≥18 years of age; and (3) lived in Canada. Participants in the provider group: (1) were currently licensed to practice medicine as a psychiatrist or family physician in Canada and (2) provided mental health care to some or all of their patients. Both groups were required to have internet or telephone access to complete the survey. Importantly, the survey was also open to health care users who had been offered a remote appointment but had not participated, as well as providers who had chosen not to offer remote visits. Participants were recruited through targeted emails to mental health organizations nationwide (e.g., Canadian Mental Health Association branches), provincial psychiatric and family physician associations, hospital newsletters, existing participant networks within CAN-BIND, and social media.
Health care users were asked about their remote care experiences with all mental health care providers, but the provider participant group was limited to psychiatrists and family physicians, as we aimed to evaluate government-funded remote care platforms (e.g., Ontario Telemedicine Network [OTN]) available to physicians.
For participants in the user group, satisfaction was assessed separately for visits with an MD provider and another health care provider, to facilitate more direct comparisons with the provider group (MD-only) and assess potential differences between visit types. This resulted in the following groups for certain analyses: (1) User-MD: mental health care users who saw an MD provider (psychiatrist or family physician); (2) User-HCP: mental health care users who saw another mental health care provider (e.g., psychotherapist); and (3) Provider-MD: psychiatrists or family physicians who provide mental health care.
Survey
After providing voluntary informed consent online, participants completed an open self-report survey to assess various aspects of remote care use during COVID-19 (available in Supplemental Material). The survey was developed in consultation with the CAN-BIND Community Advisory Committee, composed of people with lived experience, to ensure questions were relevant and meaningful to health care users. Several questions were adapted from the NIMH Coronavirus Health Impact Survey 20 and COVID-19 Community Response Survey, 21 while others were developed for the current study. The usability and functionality of the survey were tested extensively by the research team prior to launching. Surveys were tailored to each group and included multiple-choice, Likert-scale, and open-ended free-text questions. The user version of the survey had a total of 112 items (24 general and 92 adaptive), while the provider version had 87 items (18 general and 69 adaptive). Broadly, the survey assessed satisfaction with remote care, barriers to use, likelihood of future use, helpful and unhelpful aspects, suggestions for improvement, and demographic information. The survey was anonymous and took ∼15 min to complete. Participants were invited to enter a gift card draw following survey completion.
Quality control
Several quality control (QC) questions were included as safeguards to identify invalid responses or inattentive respondents. This included a CAPTCHA, instructed-response items (e.g., “Please select option 3 for data quality control”), bogus items in which all participants would be expected to answer the same way (e.g., “Have you ever used a computer or telephone?”), and contrasting items to which attentive respondents should answer in opposite ways (e.g., “I required assistance” and “I did not require assistance”).22–24 To account for momentary attention lapses among otherwise valid participants, participants were excluded if they answered ≥2 QC questions incorrectly.
Statistical Analysis
Analyses were conducted using SPSS (Version 27, IBM Corp, Armonk, NY, USA) for quantitative data and NVivo (Version 12, QSR International, 2018) for free-text responses. Descriptive statistics were used to summarize data; means are reported with standard deviations (SDs). Likert-scale measures were used in their original 7-point form for some data visualizations, and were also condensed to form binary measures (e.g., satisfied vs. dissatisfied) for further analysis: for these binary measures, neutral responses were not included in either category. Chi-square tests were used to evaluate potential associations between satisfaction status (Y/N) and other binary variables (e.g., high-risk status for COVID-19). Spearman correlations were conducted between satisfaction level and other ordinal variables. Qualitative content analysis was used to synthesize free-text responses.
Results
Participants
Participants were included if they met eligibility criteria, completed ≥1 block of satisfaction questions, and passed QC cut-offs. The full analysis set consisted of 332 users and 107 providers: a participant flow diagram is available in Supplementary Figure S1. Demographics and referral sources are presented in Table 1. The vast majority of users (97%) and all providers had engaged in remote care since March 1, 2020. Most providers were psychiatrists (92%), with a smaller proportion of family physicians (8%).
Participant Demographics.
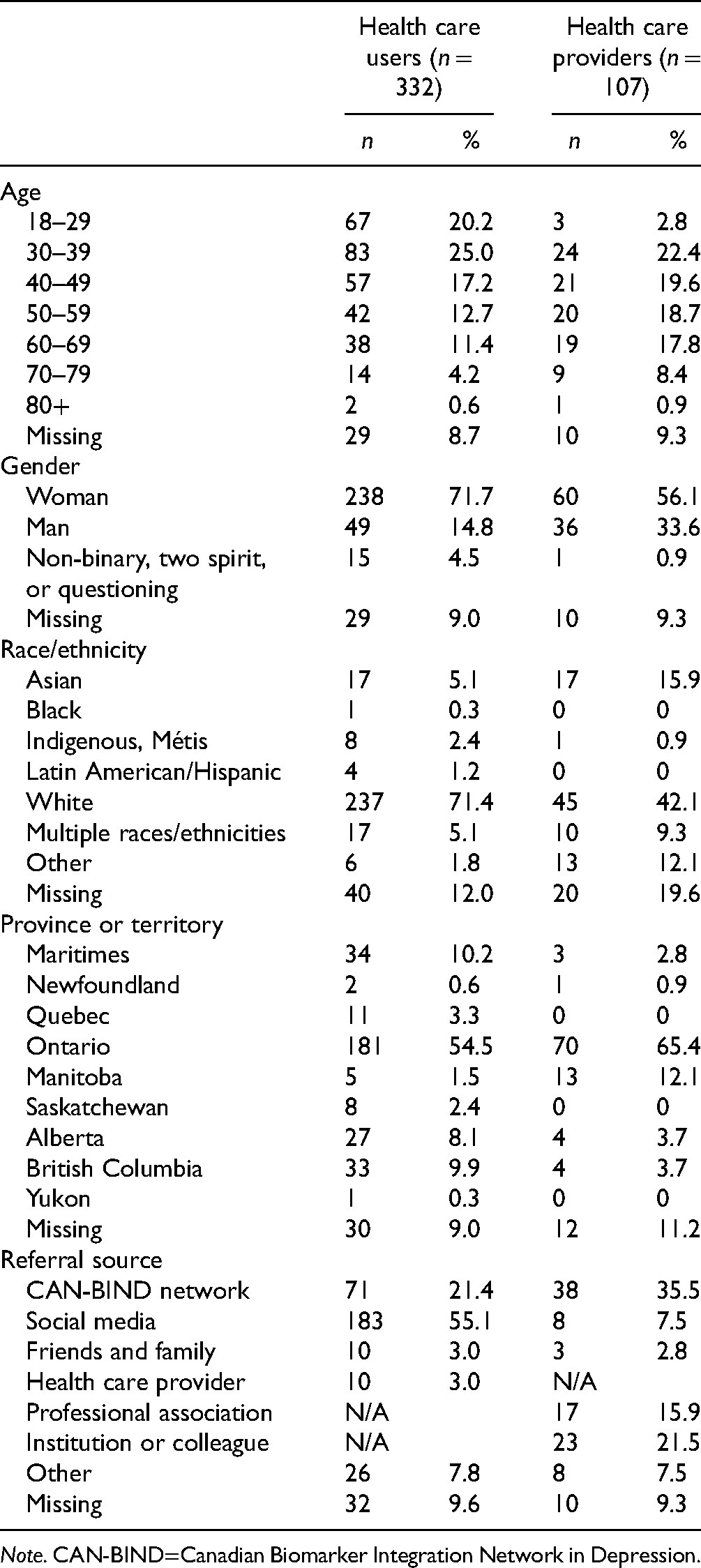
Note. CAN-BIND=Canadian Biomarker Integration Network in Depression.
Logistics of Remote Care Use
Of mental health care users who had engaged in remote care, 80% (n = 259) saw a psychiatrist or family physician (User-MD group), 61% (n = 196) saw another mental health care provider (User-HCP group), and 42% (n = 137) saw both MD and other providers. Of those who saw an MD provider, 57% saw a psychiatrist most frequently, while 43% saw a family physician more often for mental health care. Participants in the User-HCP group reported most frequently seeing a psychotherapist (30%), social worker (28%), certified psychologist (23%), case manager (4%) or other provider (16%).
Frequency of use
The mean number of remote visits since March 1, 2020, for User-MD and User-HCP participants was 7.4 (SD 5.8) and 9.7 (6.6), respectively. In contrast, providers reported delivering a mean of 22.5 (15.5) remote appointments per week. Among providers, only 16% of clinical work was done remotely prior to March 2020. Subsequently, monthly averages rose from 69% to 75%. Roughly equal proportions of providers reported that their weekly caseload increased (34%), decreased (34%), and remained unchanged (33%) from before to during the pandemic.
Platforms
Video platforms were used most frequently by 34%, 57%, and 52% of User-MD, User-HCP, and Provider-MD participants, respectively (Supplementary Table S2). Across all groups, there was no significant difference in video versus telephone use among those aged ≥50 versus <50 years.
Satisfaction with Remote Care
Figure 1 presents satisfaction scores for all groups. Overall, ∼60% of users and providers expressed satisfaction with remote care. Providers were significantly less satisfied with the user-friendliness of remote care than users (Provider vs. User-MD: U = 10,028, P < 0.001; Provider vs. User-HCP: U = 7,913, P < 0.001), while users were significantly less satisfied with continuity of care than providers (Provider vs. User-MD: U = 9,952, P < 0.001; Provider vs. User-HCP: U = 7,790, P < 0.001).
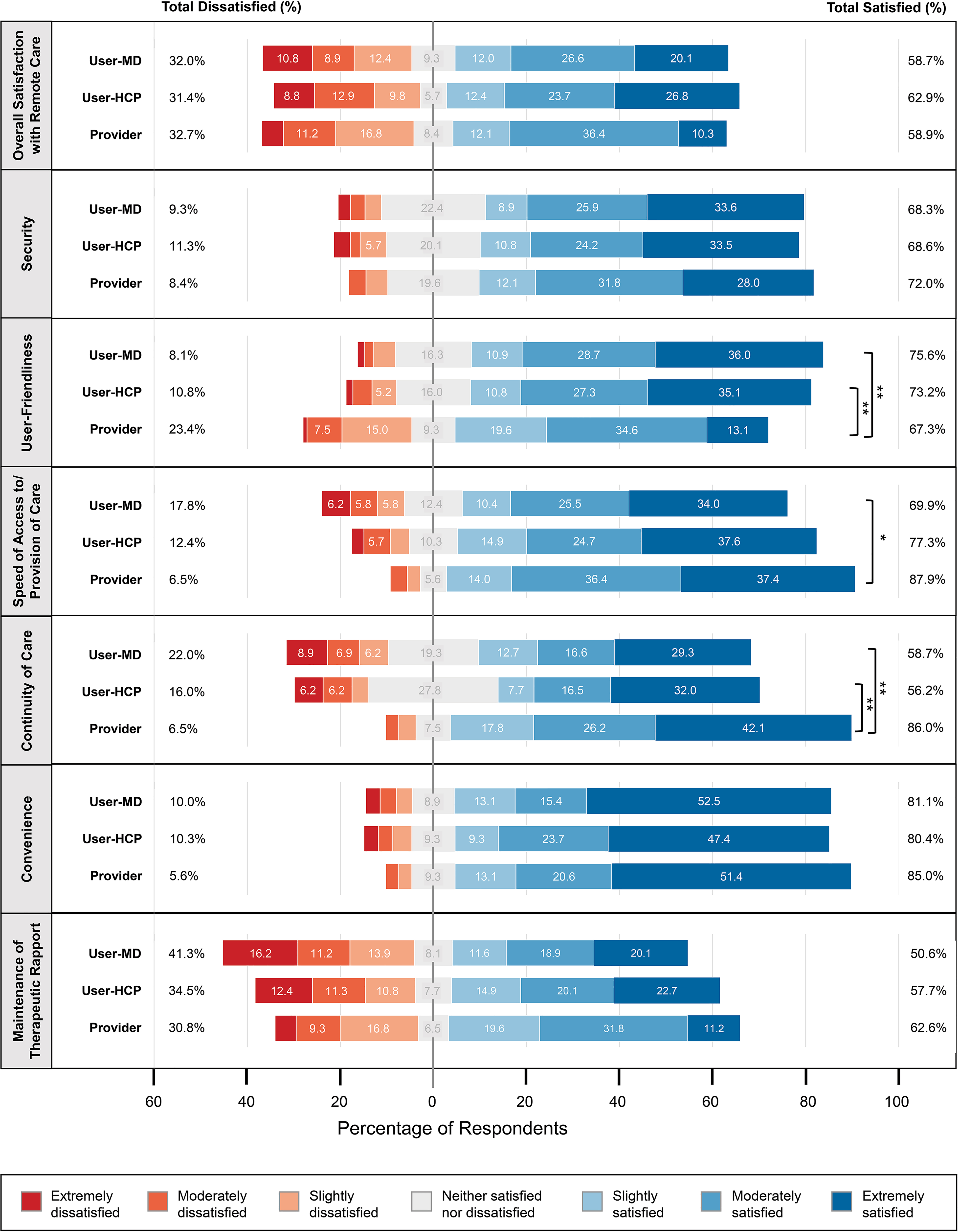
Health care user and provider satisfaction with remote care. User-MD: mental health care users who saw an MD for their remote visit (n = 259); User-HCP: mental health care users who saw another health care provider (n = 194); Provider: health care provider (n = 107). Percentages ≥5.0% are written on the bars in the figure. Significance refers to the difference in mean scores between groups. *P < 0.05, **P < 0.001.
Use of a video-based remote care method was significantly associated with satisfaction among users (User-MD: X2[1, N = 235] = 6.1, P = 0.014; User-HCP: X2[1, N = 180] = 6.6, P = 0.010) but not among providers (X2[1, N = 98] = 0.1, P = 0.785). Among User-HCP participants, level of connectedness with loved ones (as measured by frequency of texting, talking by phone or video, or meeting in person in public or at one's home) was positively correlated with overall remote care satisfaction (r[187] = 0.197, P = 0.007) and satisfaction with therapeutic rapport (r[187] = 0.155, P = 0.034). Living with others was also significantly associated with remote care satisfaction in the User-HCP group (X2[1, N = 177] = 5.8, P = 0.016). Satisfaction was significantly greater in the User-MD subgroup from Ontario than those from other provinces (X2[1, N = 215] = 3.9, P = 0.047). There were no significant associations between user satisfaction and high-risk status for COVID-19, frequency of internet use, number of people living in the home, or age (≥50 vs. <50 years). Qualitative responses relating to overall user satisfaction fell into 4 themes (Figure 2a): accessibility/convenience, provider factors, continuity of care, and visit logistics.
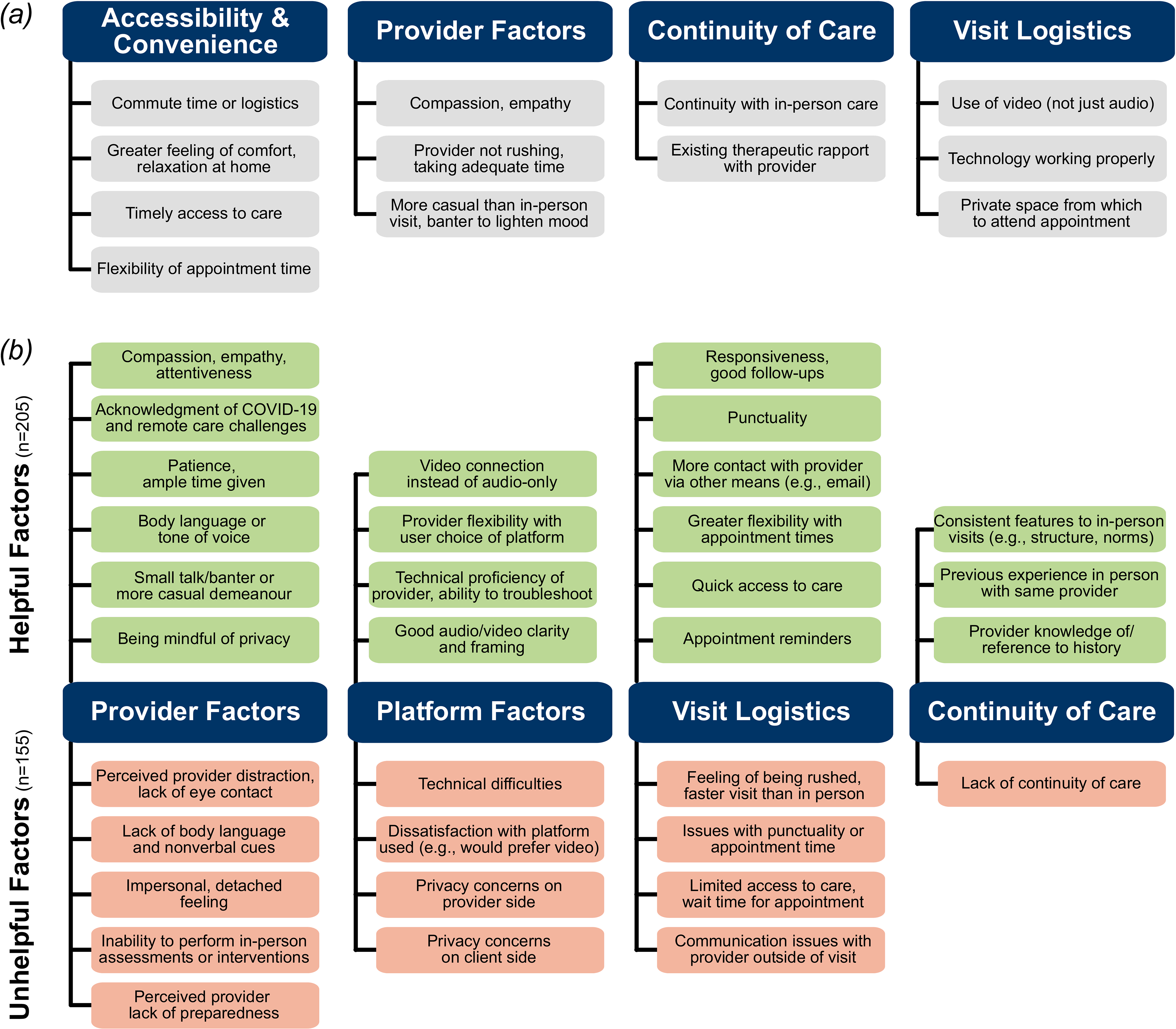
Health care user survey qualitative responses. (a) Self-reported factors contributing to overall user satisfaction with remote care; (b) helpful and unhelpful factors in maintaining therapeutic rapport or sense of connection with a health care provider.
Quality of Remote Care
The majority of User-MD (79%) and User-HCP (70%) participants agreed that their provider seemed to know their recent psychiatric history and had access to relevant records, and over half agreed that remote visits were as thorough as in-person visits (User-MD: 56%; User-HCP: 59%). In contrast, approximately half of providers agreed they had all resources needed to provide the same quality of care as in-person (45%) and adequate support from their department or institution (50%).
The vast majority of participants (User-MD: 92%; User-HCP: 91%; Provider-MD: 84%) agreed they felt confident with their technical skill in using remote care. This was not accounted for by the prevalent telephone use in our sample, as agreement was similar among the subgroup who used video (User-MD: 96%; User-HCP: 91%). The overwhelming majority of users did not require assistance to use remote care (User-MD: 94%; User-HCP: 94%), while 36% of providers did.
Difficulties
Despite high confidence in their technical skill level, nearly all providers had at least some technical difficulty accessing the remote care platform (97%), and with their patients accessing the system (91%). Technical difficulties were significantly less frequently reported by users (User-MD: 47%; U = 5,315, P < 0.001; User-HCP: 62%; U = 4,784, P < 0.001).
Finding a private space to engage in remote care was an issue for both users and providers (User-MD: 53%; User-HCP: 61%; Provider-MD: 42%), with users reporting this difficulty significantly more frequently than providers (Provider-MD vs. User-MD: U = 10,935; P = 0.01; Provider-MD vs. User-HCP: U = 7,513, P < 0.001).
Helpful and Unhelpful Factors
Health care users provided free-text responses about helpful (n = 205) and unhelpful (n = 155) factors associated with maintenance of therapeutic rapport or sense of connection with their provider (Figure 2b).
Helpful factors
Four themes of helpful factors were identified: provider factors, platform factors, visit logistics, and continuity of care. Several users appreciated their provider acknowledging the unique challenges of remote care and COVID-19, as one participant described: “[she] frequently checked-in on my experience with remote therapy as part of our sessions….” Helpful platform factors (17%) included a strong preference for video methods: “The ability to see the provider helped a great deal, versus a voice on a telephone….” Helpful factors related to visit logistics (22%) and continuity of care (31%) were also identified. Similarities to in-person care were recognized as helpful, whether by keeping the same appointment structure, norms, or even physical environment, as one respondent noted: “[having] her plants in the background [helped] to emulate the clinical office setting that I was used to.” Several participants (11%) identified unique factors outside of these categories, noting that remote care made it easier for them to discuss sensitive or anxiety-provoking issues: “the ‘one degree of separation’ that OTN provides has allowed me to talk about issues I struggled to [address] when I saw him in person….”
Unhelpful factors
Unhelpful factors in maintaining therapeutic rapport followed similar themes to the helpful factors above. Provider factors (39%) included perceived distraction and lack of nonverbal cues. One participant noted the difficulty in maintaining eye contact virtually: “Hard when she takes notes, since all that is visible on my side is that she has looked down away from the camera….” Several participants also noted the limited ability to conduct full-body assessments (e.g., for eating disorder symptoms) or engage in certain interventions (e.g., EMDR). Unhelpful factors related to the remote care platform (23%) included technical difficulties and preference for video over the telephone. Participants also reported privacy concerns, both in their own environment and their provider's: “[hearing] other people in the background made me question the privacy of our appointment….” Unhelpful factors related to visit logistics (39%) included feeling rushed or having a shorter appointment than usual.
Barriers to Use
Health Care Users
Ten participants (3.0%) were offered an appointment but did not engage in remote care. The most commonly endorsed barriers (Supplementary Table S3) were the feeling that remote visits would be impersonal (8 of 10), followed by privacy concerns about both the home/work environment (7 of 10) and the remote care platform itself (6 of 10). In free-text responses about changes that would be needed before using remote care, factors identified by ≥2 participants were the need for private space, technological literacy, and preference for the qualities of in-person sessions, as one participant described: …the comforting silence that can occur during real life meetings can be misconstrued as technological difficulties … Internet speed is also an issue because it may interrupt someone mid-sentence and they will have to repeat themselves on a topic that may have already been difficult enough saying the first time.
Health Care Providers
All providers delivered remote care; however, perceived challenges or barriers were still assessed through a free-text question (Figure 3a). Technical (64%), logistical (34%), and provision of care (28%) issues were commonly identified. A smaller proportion of providers (17%) identified a single issue outside of these categories, such as patient preference (n = 3) or physician fatigue and burnout (n = 2).
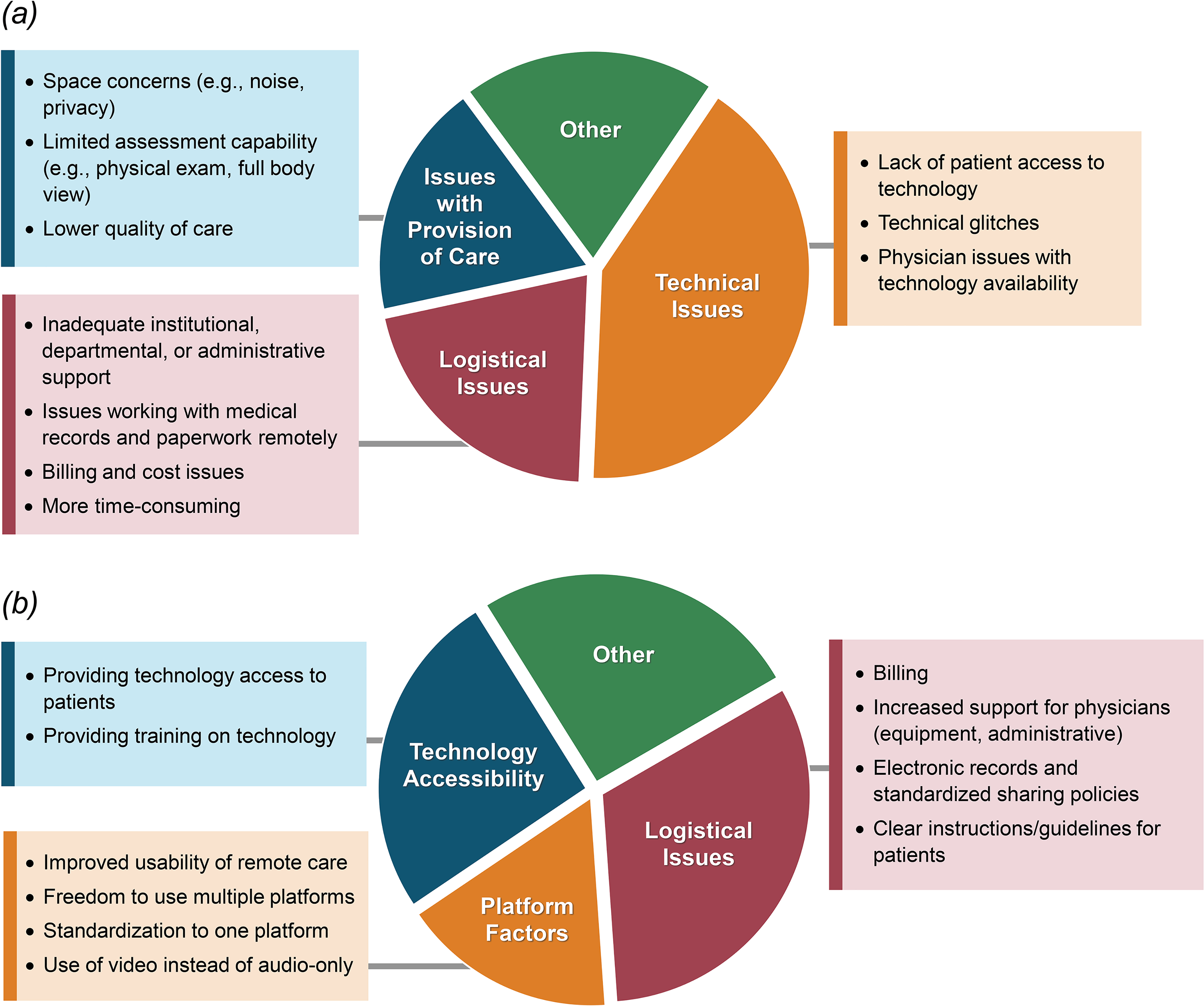
Health care provider survey qualitative responses. (a) Challenges and barriers to implementing remote care (n = 95); (b) suggestions for increasing success or uptake of remote care (n = 82).
Future Use
The majority of participants said they would likely use remote care again, both during and after COVID-19 (Table 2), preferring a combination of in-person and remote care, with video being a favoured method either alone or in combination with telephone.
Health Care User and Provider Attitudes Regarding Future Use of Remote Care.
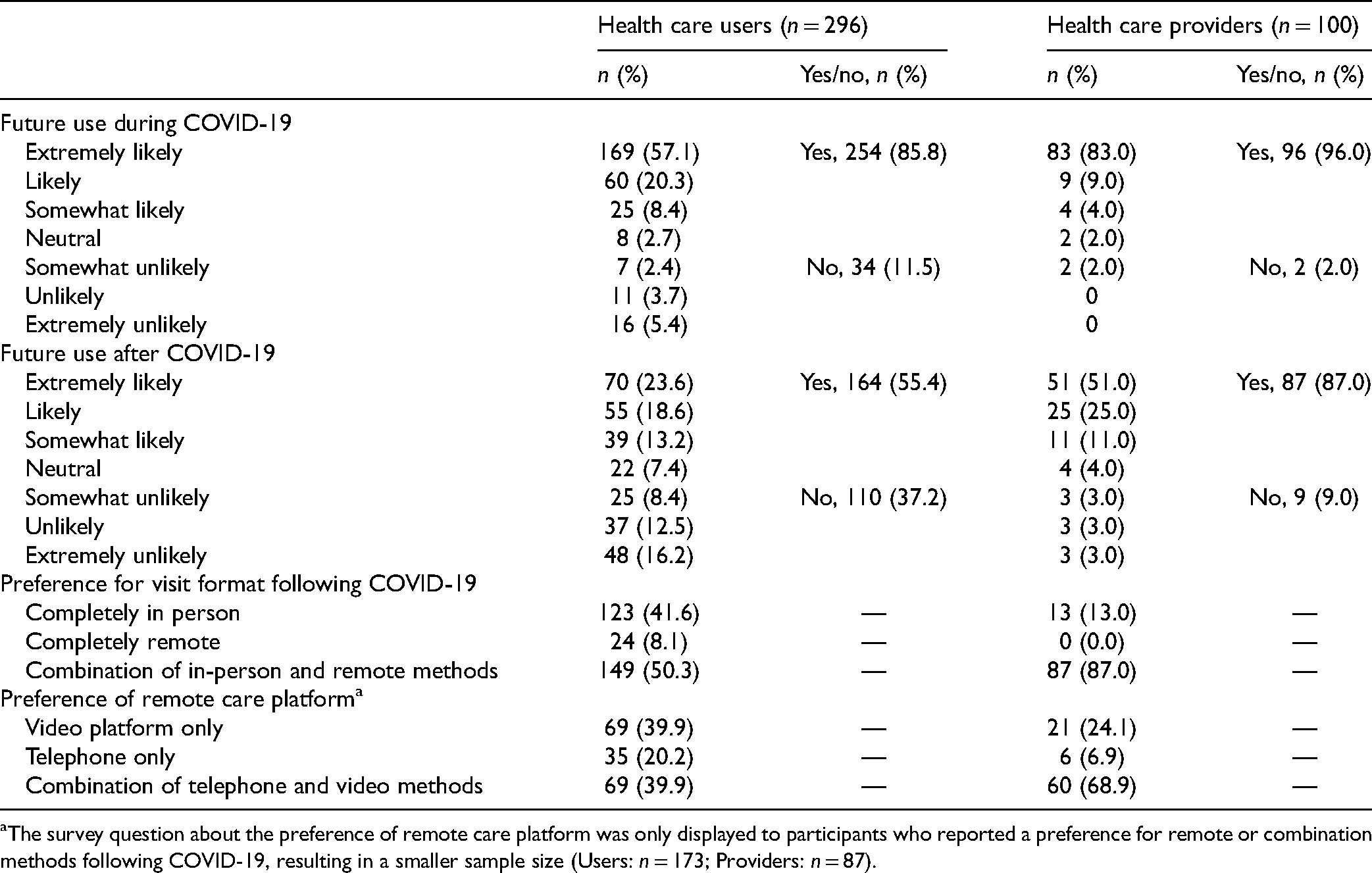
The survey question about the preference of remote care platform was only displayed to participants who reported a preference for remote or combination methods following COVID-19, resulting in a smaller sample size (Users: n = 173; Providers: n = 87).
Providers’ free-text suggestions for increased success or uptake of remote care (Figure 3b) addressed logistical issues (35%), technology accessibility (28%), and platform-specific factors (18%). A subgroup (28%) proposed unique suggestions outside of these categories, including a strategy of starting with in-person care and moving to remote methods (n = 2) and recognition that remote care has unique challenges but not presenting it as ‘lesser than’ in-person methods (n = 3).
Discussion
This national online survey assessed experiences with remote care during COVID-19 among Canadian mental health care users and providers. Overall, the majority of surveyed users and providers were satisfied with remote care. Users emphasized the convenience of remote care, while providers reported the greatest satisfaction with the speed of provision of care. Both groups were least satisfied with therapeutic rapport. Video use was significantly associated with satisfaction: this was supported by qualitative responses emphasizing the benefits of visual cues (e.g., body language and eye contact) in maintaining therapeutic rapport. Users reported significantly less difficulty than providers with technical issues, but significantly more with finding private space. Following the pandemic, over half of users and almost 90% of providers would continue using remote care methods, either alone or in combination with in-person visits.
Satisfaction rates in this study (∼60%) are lower than in previous reports of remote care satisfaction during COVID-19, where rates were 80% to 82% among users10,11 and 66% to 73% among providers. 12 We observed that User-HCP participants who lived alone reported lower satisfaction with remote care. A potential explanation is that those living alone may experience social isolation and boredom while restricted to their homes, for which in-person appointments may provide some relief. Additionally, those with home caregiving responsibilities may value the convenience of remote care over arranging childcare or other supports. Several qualitative subthemes are consistent with a previous qualitative report of service users and providers during COVID-19. 25
In this study, 41% to 64% of participants reported telephone as their most-used remote care method. This is surprising, as the majority of respondents lived in provinces in which government-funded platforms (e.g., OTN) are available. It is unclear whether this was due to patient preference or lack of video access, although a common sentiment in free-text user responses was a preference for video over telephone, consistent with the previous literature.26,27 Thus, this high prevalence of telephone use may explain the lower overall satisfaction in our sample. The greater user satisfaction we observed with video is also consistent with a Canadian survey of rural telemedicine users during COVID-19. 15 We found providers experienced significantly more technical difficulty than users. This may reflect the more frequent use among providers, presenting more opportunities for technical difficulties: users reported a mean of <10 remote care experiences throughout the entire pandemic, while providers reported, on average, over 20 remote visits each week.
Overall, 55% of users and 87% of providers said they would likely use remote care again after COVID-19. This is a notable increase from the 17% of users and 56% of providers who reported using remote care pre-pandemic and is consistent with previous reports,11,12,26,28 supporting predictions that the widespread shift to remote care during COVID-19 will transform mental health care delivery going forward.
While remote care methods have improved access to care for many during a time of widespread physical distancing, they also present critical issues of accessibility and equity for disadvantaged groups who may not have reliable access to telephone and/or internet, or a private space to attend appointments. 29 Indeed, qualitative responses from providers in our study commonly identified patient technology access as a barrier. Furthermore, the use of video-based platforms requires technology familiarity, which may disadvantage older users. 30 However, in contrast with a previous report which found individuals aged ≥44 years were more likely to use telephone for telepsychiatry during COVID-19, 26 we did not find a difference in video versus telephone use between those aged under and over 50 years.
This study has several limitations. First, though we tried to mitigate illegitimate responses with multiple QC checks, the survey's online self-report nature limits our ability to confirm response validity. Second, since qualitative responses were collected in survey format, we were unable to probe further as would be possible in an interview. Third, the small number of respondents who did not engage in remote care limits comparative analysis, and the low rate of reported barriers to use may be skewed: only one participant reported technological limitations as a barrier, and none reported unmet accessibility needs. It is possible that in part due to its online recruitment method, this survey failed to capture experiences in communities where reliable access to technology is unavailable, who may have differing perspectives on remote care. Fourth, the provider survey was restricted to psychiatrists and family physicians; future work should assess a broader range of mental health care providers. The limited gender and racial/ethnic diversity of our sample may also limit generalizability. Further, while responses suggest all remote visits took place in an outpatient setting, we cannot rule out the possibility of inpatient use which may increase sample heterogeneity. Finally, sample representation was skewed across Canada, with the majority from Ontario. Among User-MD participants, we did find a significant association between living in Ontario and remote care satisfaction. As Ontario has been among the provinces with the highest COVID-19 case numbers and strictest lockdown restrictions, this increased satisfaction may reflect the greater need for exclusively remote methods of care in Ontario.
Conclusion
Remote care comes with both opportunities and challenges: convenience and access to care may be improved, but there also exists a potential for decreased therapeutic rapport and assessment quality. Overall, we found most mental health care users and providers were satisfied with remote care. Based on user feedback, recommendations to improve therapeutic rapport remotely include video usage, increased attention to body language (e.g., looking at webcam instead of screen) and privacy, and acknowledgment of challenges associated with COVID-19 and remote care. From provider perspectives, increased administrative support, streamlined billing, and technology availability and training would be key steps to increase remote care success and uptake and are consistent with previous reports. 31 It is unclear what role remote platforms will play in mental health care post-pandemic, but the reported willingness by both users and providers to use them in future suggests a lasting impact. Future studies evaluating clinical outcome and service utilization data during COVID-19 will also be valuable to understand the broader implications of shifting to remote care.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437211070656 - Supplemental material for “One Degree of Separation”: A Mixed-Methods Evaluation of Canadian Mental Health Care User and Provider Experiences With Remote Care During COVID-19
Supplemental material, sj-docx-1-cpa-10.1177_07067437211070656 for “One Degree of Separation”: A Mixed-Methods Evaluation of Canadian Mental Health Care User and Provider Experiences With Remote Care During COVID-19 by Amanda K. Ceniti, Wegdan R. Abdelmoemin, Keith Ho, Yudi Kang, Franca Placenza, Rachel Laframboise, Venkat Bhat, Jane A. Foster, Benicio N. Frey, Raymond W. Lam, Roumen Milev, Susan Rotzinger, Claudio N. Soares, Rudolf Uher and Sidney H. Kennedy in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-2-cpa-10.1177_07067437211070656 - Supplemental material for “One Degree of Separation”: A Mixed-Methods Evaluation of Canadian Mental Health Care User and Provider Experiences With Remote Care During COVID-19
Supplemental material, sj-docx-2-cpa-10.1177_07067437211070656 for “One Degree of Separation”: A Mixed-Methods Evaluation of Canadian Mental Health Care User and Provider Experiences With Remote Care During COVID-19 by Amanda K. Ceniti, Wegdan R. Abdelmoemin, Keith Ho, Yudi Kang, Franca Placenza, Rachel Laframboise, Venkat Bhat, Jane A. Foster, Benicio N. Frey, Raymond W. Lam, Roumen Milev, Susan Rotzinger, Claudio N. Soares, Rudolf Uher and Sidney H. Kennedy in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-3-cpa-10.1177_07067437211070656 - Supplemental material for “One Degree of Separation”: A Mixed-Methods Evaluation of Canadian Mental Health Care User and Provider Experiences With Remote Care During COVID-19
Supplemental material, sj-docx-3-cpa-10.1177_07067437211070656 for “One Degree of Separation”: A Mixed-Methods Evaluation of Canadian Mental Health Care User and Provider Experiences With Remote Care During COVID-19 by Amanda K. Ceniti, Wegdan R. Abdelmoemin, Keith Ho, Yudi Kang, Franca Placenza, Rachel Laframboise, Venkat Bhat, Jane A. Foster, Benicio N. Frey, Raymond W. Lam, Roumen Milev, Susan Rotzinger, Claudio N. Soares, Rudolf Uher and Sidney H. Kennedy in The Canadian Journal of Psychiatry
Supplemental Material
sj-docx-4-cpa-10.1177_07067437211070656 - Supplemental material for “One Degree of Separation”: A Mixed-Methods Evaluation of Canadian Mental Health Care User and Provider Experiences With Remote Care During COVID-19
Supplemental material, sj-docx-4-cpa-10.1177_07067437211070656 for “One Degree of Separation”: A Mixed-Methods Evaluation of Canadian Mental Health Care User and Provider Experiences With Remote Care During COVID-19 by Amanda K. Ceniti, Wegdan R. Abdelmoemin, Keith Ho, Yudi Kang, Franca Placenza, Rachel Laframboise, Venkat Bhat, Jane A. Foster, Benicio N. Frey, Raymond W. Lam, Roumen Milev, Susan Rotzinger, Claudio N. Soares, Rudolf Uher and Sidney H. Kennedy in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The authors thank the CAN-BIND Community Advisory Committee for consultation and input into study design, Dr. Yvonne Bergmans for consultation on qualitative analysis, and the study participants for their time and effort in contributing to this research.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ms. Ceniti, Dr. Abdelmoemin, Mr. Ho, Ms. Kang, Dr. Placenza, Ms. Laframboise, and Dr. Bhat have no conflicts of interest. Dr. Lam reports receiving honoraria or research funds from Allergan, Asia-Pacific Economic Cooperation, BC Leading Edge Foundation, CIHR, CANMAT, Healthy Minds Canada, Janssen, Lundbeck, Lundbeck Institute, MITACS, Myriad Neuroscience, Ontario Brain Institute, Otsuka, Pfizer, Unity Health, and the VGH-UBCH Foundation. Dr. Milev reports receiving consulting and speaking honoraria from AbbVie, Allergan, Eisai, Janssen, KYE, Lallemand, Lundbeck, Otsuka, and Sunovion, and research grants from CAN-BIND, CIHR, Janssen, Lallemand, Lundbeck, Nubiyota, OBI and OMHF. Dr. Foster, Dr. Frey, Dr. Rotzinger, Dr. Soares, and Dr. Uher have no conflicts of interest. Dr. Kennedy reports research funding or honoraria from Abbott, Alkermes, Allergan, Boehringer Ingelheim, Brain Canada, Canadian Institutes for Health Research, Janssen, Lundbeck, Lundbeck Institute, Ontario Brain Institute, Ontario Research Fund, Otsuka, Pfizer, Servier, Sunovion, and Sun Pharmaceuticals, and holds stock in Field Trip Health.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted as part of CAN-BIND, an Integrated Discovery Program supported by the Ontario Brain Institute, which is an independent non-profit corporation, funded partially by the Ontario government. The opinions, results, and conclusions are those of the authors and no endorsement by the Ontario Brain Institute is intended or should be inferred.
Data Access
Data are available from the authors upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.