
Abstract
Objective
Mental illness is a common medical condition to onset during adolescence. Young people who leave for postsecondary life are at an especially challenging period of lifetime when many will leave home and familiar environments for prolonged periods of time. These new circumstances may put young people at risk of developing mental health problems or disorders or exacerbate existing mental disorders. Alternatively, some young people may misinterpret the normal negative emotional states occurring as a result of these new challenges as a mental disorder requiring professional intervention. We conducted a quasiexperimental cohort study to investigate the effectiveness of a mental health literacy intervention Transitions with blended life skills to address these challenges for first-year postsecondary students.
Methods
Students (n = 2,397) from five Canadian postsecondary institutions were assigned to the intervention or the control group and were administered a survey at baseline, postintervention, and at 2-month follow-up (September 2017 to February 2018). We applied generalized linear mixed effects (PROC Mixed procedure) to test the between-group difference in the post—pre/follow-up—pre and to determine the predicted least-square mean values.
Results
The findings showed that students who were exposed to the Transitions intervention significantly improved their mental health knowledge, decreased stigma against mental illness, improved help-seeking attitudes and behaviours, and decreased perceived stress when compared to students who had not been exposed to the intervention. However, we did not identify significant changes in general health. This may be due to the relatively short follow-up time (2 months) to determine participants’ general health status.
Conclusions
Transitions delivered to first-year postsecondary students may be a beneficial intervention to help young people adjust to their new postsecondary life and improve their mental health.
Introduction
Mental illness is the most common medical condition to onset during adolescence, with ∼50% of mental disorders onset by age 14 years and 75% by age 24 years. 1 Furthermore, life-long health-promoting behaviours are often solidified by the end of the second decade of life. 2 Postsecondary school students are therefore a cohort of interest and concern regarding mental health and mental illness.
Research indicated that 31% to 35% of postsecondary students were screened positive for at least one of the common lifetime/12-month disorders assessed. 3 In Canada, the prevalence of mental disorders among youth aged 15 to 24 is estimated to be 10% to 15%.4-6 Mental disorders during adolescence have significant negative impacts, including impairment in daily functioning, intimate interpersonal relationship difficulties, poor learning outcomes and academic success, higher risk of alcohol and drug use, poorer vocational achievement, and reduced life expectancy.7,8 Suicide, commonly associated with mental disorders,9,10 is the second leading cause of death among youth.11-13 Despite the prevalence and life consequences of mental illness, help-seeking behaviours in this population are low, with estimates of 25.3% to 36.3% help-seeking rates for mental disorders and 29.5% to 36.1% for suicide thoughts and behaviours. 14
Further, studies have identified that many young people in postsecondary institutions endorse a variety of negative emotions and coping challenges.15-21 These results have been often interpreted as a “mental health crisis” and an “epidemic of mental disorders” on campus with calls for more therapy and other mental health speciality services as a response,22-27 despite the fact that the prevalence of mental disorders among young people has been relatively stable over decades.28-32
These data reporting high rates of increases in perceived mental disorders in the face of stable prevalence suggest that some young people may not be able to distinguish normal existential stresses from a mental disorder due to a lack of mental health literacy.33-35 Similarly, this suggests that providing young people who are transitioning to postsecondary schooling with information that could enhance their mental health literacy while concurrently addressing the common and normal stress-inducing situations that they are likely to experience may be a useful mental health intervention. Mental health literacy entails four interrelated components: capacity to obtain and maintain good mental health; knowledge about mental health and mental disorders; stigma reduction; and help-seeking efficacy.34,35 A curriculum-integrated mental health literacy approach has been extensively applied and researched in secondary school settings to improve mental health literacy outcomes.36-39 However, the application of such curriculum-embedded approaches in postsecondary settings may not be feasible and alternative methods suitable for the particular contexts of postsecondary settings should be considered. This should be based on the reality of normal developmental challenges occurring during this time.
Many young people may head off to postsecondary institutions, leaving home for prolonged periods of time. These new circumstances create normal existential stresses, which may exacerbate existing mental disorders or demand coping strategies not yet developed. Concomitantly, young people may not realize that the difficulties they are experiencing could be due to a mental disorder rather than simply a reaction to life changes. Thus, they may not seek appropriate assistance with the result that early intervention and effective treatment do not occur expeditiously. Alternatively, young people may misinterpret the normal negative emotional states occurring as a result of these new challenges as a mental disorder requiring professional intervention. Therefore, providing information about mental health and mental illness in the context of other important issues that characterize this transition period may both enhance support to young people during this critical period and improve their ability to cope with these stresses, identify a mental disorder if it is on-setting and to seek help appropriately if needed.
This study investigated the impact of a mental health intervention Transitions that embeds mental health literacy into a comprehensive life skills resource for young people transitioning from secondary to postsecondary schooling. This most recent version of the Transitions updated the previous edition by including input from first-year university/college students, mental health experts, student-services staff, and faculty members. Building on previous research using earlier versions of Transitions that had demonstrated preliminary evidence on the improvements in mental health literacy,40-42 this current study applied a more robust research design with control groups in a large cohort that included both university and college students in five institutions of higher learning in Canada. This study hypothesized that mental health literacy embedded in a life skills resource for first-year students in postsecondary settings would promote student's understanding about mental health, improve their attitudes toward mental illness, reduce stigma against mental illness, improve their help-seeking efficacy and general health, and reduce perceived stress. This study was approved by the principal investigator's institution (# 2017-4174) and each of the participating institutions.
Methods
Participants and Recruitment
This study applied a quasiexperimental design with purposefully selected participants in each institution to participate in either the intervention group (participants who received Transitions) or the control group (participants who waited to receive Transitions). They were compared before Transitions was delivered, immediately after its delivery, and at 2-month follow-up. This design allowed the assignment of participants to the intervention or control group with similar demographic characteristics in this study. 43 Given the significance level of α = 0.05, power 1 − β = 0.80, the number of predictors n = 4, and the medium effect size f2 = 0.15 for the multivariate analysis based on a similar study, 44 we needed a total sample of n = 85 to achieve 80% power.
The study population was first-year undergraduate students enrolled in September 2017 from five institutions. We focused on Maritime provinces (Nova Scotia, New Brunswick, and Prince Edward Island) for study. We sent out invitation of the project participation to all universities and colleges across these three provinces and received confirmation of participation from five volunteering universities and colleges. We ended up recruiting over 2,000 students, representing ∼11% of the first-year university/college student population between 2017 and 2018 in these provinces, a quite large sample although it may not represent the whole student population in Canada. Each institution made its own decision on whether it would recruit students for both intervention or control groups or just for one study group depending on its contexts. Each institution designated specific staff to recruit participants.
At institutions 1 (n = 475) and 2 (n = 515), students were recruited by administrators within specific programs, intervention (n = 180 in institution 1; n = 265 in institution 2), and control (n = 295 in institution 1; n = 250 in institution 2) campuses were geographically distinct, thus decreasing the likelihood of cross-site contamination.
At institutions 3 to 5, faculty members who chose to participate in the study recruited students. At institution 3, 211 participants were drawn from a psychology course section (n = 84 control; n = 128 intervention). At institutions 4 (n = 243) and 5 (n = 952), students were drawn from various programs, all participating in the intervention only (see Figure 1).
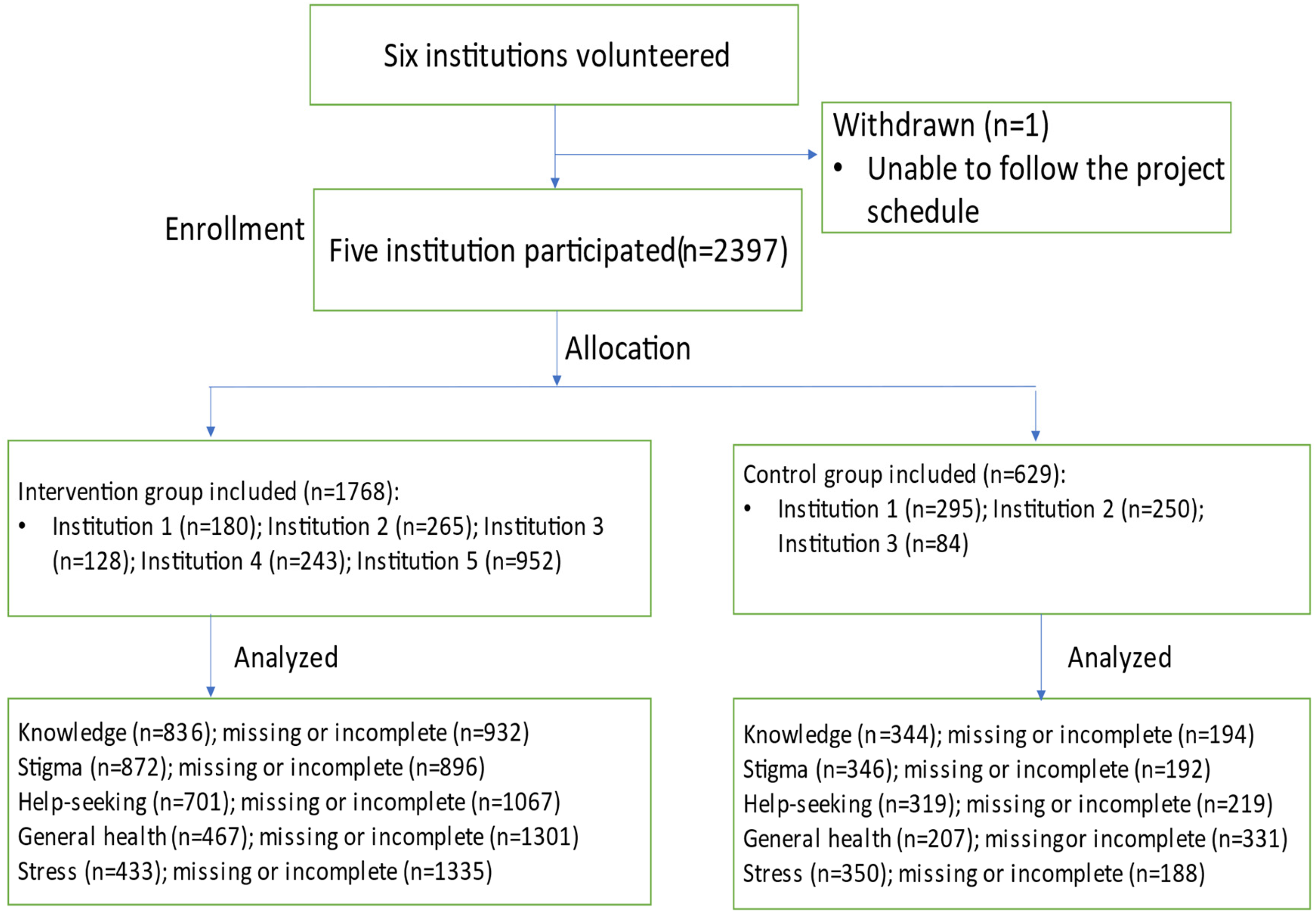
Recruitment process.
Procedure
Transitions (http://mentalhealthliteracy.org/product/transitions/) provides participants with information in five areas: information related to academic life, such as learning skills, class selection, preparing exams, and dealing with procrastination; knowledge about mental health and common mental disorders, stress management, treatment options, help-seeking resources, and sexual health; building multiple identities based on factors such as ethnicity, culture, gender, personality, values, spirituality and faith, and sexuality; building healthy relationships (e.g., friendship, romantic relationships, roommates, international students, and conflict resolution); and (mental) health help-seeking information and resources on campus. The delivery of Transitions was flexible depending on the context of the participating institution.
In all institutions, either a research assistant or a faculty member volunteering to facilitate the project administered an anonymous survey to students in both the intervention and control group at baseline. Then, the intervention group received a copy of Transitions and was given a 2-week period to read the Transitions resource. Reading took place after classes and in some cases, during classes. After this 2-week period, the research assistant or the faculty member administered the survey again, and at 2 months following the second survey in both the intervention and control groups. The study took place between September 2017 and February 2018.
Additionally, at institution 1, when students read Transitions, they were also provided with a short, in-classroom presentation by a research assistant that described Transitions and identified the different components in it. At institution 2, Transitions was provided to students as part of their course work, mostly assigned as readings for “homework” but the mental health portion was instructor-delivered in-class using a prepared presentation by a psychologist.
At institution 3, the intervention group participated in a 75-min in-class seminar, led by research assistants who developed a board game-Thrive-based on the Transitions content. At institutions 4 and 5, faculty members introduced Transitions in the classroom and students were asked to read Transitions after the class, and faculty members were available for support. We did not control how Transitions was implemented in each institution since it is impossible to implement such an intervention exactly the same manner in postsecondary institutions. The diversity of the delivery format evaluated in this study may inform other institutions to customize their implementation to maximize the intervention up-taking.
Survey and Data Analysis
Five outcomes were observed: knowledge, stigma, help-seeking attitudes and behaviours, general health, and perceived stress (Appendix 1). Twenty knowledge questions investigated participants’ understanding about the content related to life skills and mental health. Participants chose one response (True, False, or Don't know) to each question. Each correct answer received a score of 1, and an incorrect answer, including “Don't know” received a score of 0. The total knowledge score was 20. The exploratory factor analysis demonstrated four factors (knowledge about mental health, mental disorders, and life challenges; stress and resilience; mental health treatment; and brain functions) addressing 42.45% of the variances with the current data. The internal consistency of the measure was α = 0.67 for the current data. We expected a relatively low internal consistency of the measure as it is a multidimensional scale covering various aspects of healthy life.
Twelve statements on stigma measured how participants perceived mental health and mental illness. Each statement had a score range of 1 to 7 on a Likert scale. Higher scores represented more positive attitudes, indicating lower stigma. Each participant received a total score between 7 and 84. The factor analysis identified one factor indicating the perceived stigma construct, with a total of 43.25% variances explained by the factor. The internal consistency reliability of the current data was α = 0.85.
For the attitudes toward help-seeking, there were five 7-point Likert scale statements with each response assigned a value between 1 and 7. Higher scores indicated more positive attitudes. Each participant received a total score of between 5 and 35. The factor analysis with the current data identified one factor indicating the help-seeking intentions construct, with a total of 69.29% variances explained by the factor. The internal consistency reliability of the current data was α = 0.81. Help-seeking behaviours were investigated with one question on whether participants in the past 2 months went to see a health professional for mental health problems or disorders.
For the general health outcome, there were 12 7-point Likert scale statements with each response assigned a value between 0 and 3. Higher scores indicated more severe health concerns. Each participant received a total score of between 0 and 36. General health measure has demonstrated strong reliability and validity in previous studies. 45 The internal consistency reliability of the scale on the current data was α = 0.88.
For the perceived stress outcome, there were 10 7-point Likert scale statements with each response assigned a value between 0 and 4. Higher scores indicated more perceived stress. Each participant received a total score of between 0 and 40. The stress measure has demonstrated strong reliability and validity in previous studies. 46 The internal consistency reliability of the scale on the current data was α = 0.79.
Descriptive statistics were reported as counts and percentages for categorical variables, means and standard deviation for normally distributed continuous variables, and medians and interquartile ranges for nonnormally distributed continuous variables. Baseline differences between the intervention group and control group were examined using chi-square test, Fisher's exact test, t-test, and/or Wilcoxon rank-sum test, as appropriate.
The dependent variable was the survey score for each of the five outcomes. Generalized linear mixed effects (PROC Mixed procedure) were used to test the between-group difference at each study time point and to determine the predicted least-square (LS) mean values. Study group (intervention or control) and time point of the survey were included in each model as fixed effects and institution as a random effect. Study group by time point interaction was included in each model as well as a condition with each additional demographic covariate including gender, previous mental health education, previous mental health treatment, and international student status. Variables and interactions found to be statistically significant at P < 0.1 in the univariate model analysis were included in the multivariate model.
The intraclass correlation coefficient (ICC) was applied to investigate variability in response across institutions. The log-linear analysis was applied to compare the number of students who opted to seek help at pretest and follow-up. All analyses were conducted using SAS/STAT software, with a significance level of α = 0.05.
Results
Out of 2,397 students, 1,768 students were assigned to the intervention group and 629 students as controls (Figure 1). Of this, 1,183 students completed both pretest and posttest (49%); 939 students completed both pretest and 2-month follow-up surveys (40%). Of 2,397 students, 223 students reported help-seeking behaviours at both pretest and 2-month follow-up (9.3%). The pre–post analysis measured: knowledge, stigma, and help-seeking attitudes. The pretest and 2-month follow-up analysis evaluated: help-seeking behaviours, general health, and perceived stress as it took time to measure changes in these outcomes. Generalized linear mixed models were used to model the data with data points entered into the models separately at pre and post time points. This enables data points to be included in the model whether or not the student reported answers at each time point thus reducing the amount of information lost.
Table 1 presents participants’ demographics. A chi-square test revealed significant differences between group by gender, with significantly more female participants (56.7%) than expected in the Transitions group (χ2(1) = 5.14, P = 0.02); by student nationality, with significantly more Canadian participants (93.2%) than expected in the control group (χ2(1) = 63.83, P = 0.000); and by previous treatment of oneself or their family members, with significantly more participants (49.3%) than expected who had previous treatment in the control group (χ2(1) = 6.41, P = 0.01); however, not by previous mental health education (χ2(1) = 2.03, P = 0.15). Demographic differences were factored in the PROC mixed model and controlled in the data analysis.
Demographics.
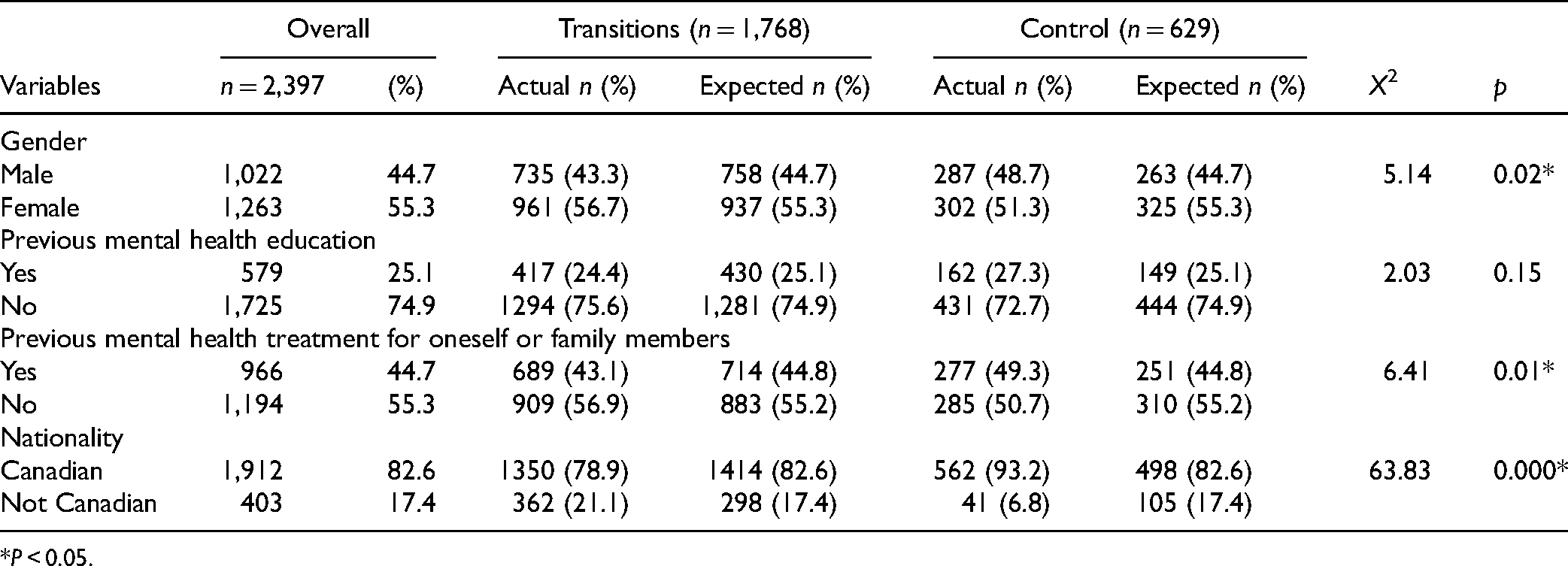
*P < 0.05.
An ICC analysis indicated nonsignificant institution differences regarding knowledge (ICC = 0.078), stigma (ICC = 0.006), help-seeking attitudes (ICC = 0.013), general health (ICC = 0.037), or stress (ICC = 0.156).
Knowledge
The univariate analysis of gender (p = 0.85) was not statistically significant and therefore gender was excluded in the multivariate model.
A multivariate analysis identified a statistically significant interaction between the groups and the knowledge score (P < 0.001). The LS mean estimate was calculated at three different mean population pretest scores: 5, 10, and 15. The LS mean difference estimate was statistically significant when comparing intervention group post to pre knowledge total, 1.85 (95% CI, 1.68 to 2.02). The intervention group estimate was 1.878 (95% CI, 1.53 to 2.22) higher post follow-up compared to the control group. There was no statistically significant difference between the intervention and control group at baseline, (experimental–control) −0.11 (95% CI, −0.43 to 0.21).
There was a statistically significant difference between those with previous mental health treatment and those without, 1.05 (95% CI, 0.83 to 1.26, P < 0.001). Those with previous mental health education had a higher LS mean estimate of knowledge score compared to those without previous mental health education, 0.49 (95% CI, 0.27 to 0.73, P < 0.001), and Canadian students had a higher LS mean estimate of the knowledge score, 1.72 (95% CI, 1.43 to 2.0,1 P < 0.001), compared to those who were international visa students.
Stigma
The univariate analysis demonstrated that demographics significantly predicted the pre–post change of stigma scores. A multivariate analysis demonstrated that the LS mean estimate in stigma was 1.22 (95% CI, 0.04 to 2.40, P = 0.042) greater for the intervention group compared to the control. There was no statistically significant difference between intervention and control at baseline, 0.114. This demonstrates greater improvements in stigma reduction in the intervention group.
It also showed no statistically significant interaction between gender and study groups, P = 0.136. However, there was a statistically significant difference in stigma LS difference estimate for women compared to men, 3.82 (95% CI, 2.64 to 4.99).
Pretest stigma, previous mental health treatment, previous mental health education, and international student status did not interact with the study groups, and therefore did not impact the pre–post change in stigma scores between the intervention and control groups (P > 0.05).
Help-Seeking Attitudes and Behaviours
The univariate modeling for help-seeking attitudes and international student status was not statistically significant (P = 0.75). A multivariate analysis demonstrated that the intervention group had an LS mean difference estimate of post–pre score 1.287 (95% CI, 0.94 to 1.63, P < 0.001) compared to 0.77 (95% CI, 0.24 to 1.30, P = 0.004) in the control group. The LS mean estimate for those with previous mental health treatment was 1.12 (95% CI, 0.68 to 1.57, P < 0.001) greater than for those without previous treatment (P = 0.011). Females had a greater LS mean estimate of 0.682 (95% 0.25, 1.11, P = 0.002) compared to males and those with previous mental health education has a greater LS estimate of 0.59 (95% CI, 0.12 to 1.06, P = 0.013).
We applied the three-way log-linear analysis (condition × pretest × follow-up) to observe the number of students who opted for help (either already spoke to a health provider or waited to see a health provider) against the number of students who did not at pretest and 2-month follow-up. Although the three-way interaction was not significant (χ2(1) = 1.45, P > 0.05), the two-way chi-square test indicated at 2-month follow-up there was a significant association between the group type (intervention or condition group) and help-seeking behaviours (χ2(1) = 20.65, P < 0.001). Based on the odds ratio, the odds of students in the intervention group seeking help were 2.75 times greater than students in the control group at the 2-month follow-up.
General Health
A univariate analysis showed no statistically significant association between post and prechange in general health with the study groups (P = 0.762) implying that the intervention did not influence the general health outcome among participants.
Perceived Stress
A univariate analysis showed no statistically significant association between study group and gender (P = 0.1429), previous mental health treatment (P = 0.5429), international student visa status (P = 0.77), and previous mental health education (P = 0.11).
The impact of the intervention varied depending on the time point. In the intervention group, the LS mean difference estimate (pre–post) was 3.451 (95% CI, 2.92 to 3.99, P < 0.001), compared to −0.64 (95% CI, −1.28 to −0.002, P = 0.049) in the control group.
Discussion
This is the first large-scale controlled study of an intervention blending life skills information with mental health literacy for postsecondary youth that addressed campus mental health and life. The findings showed that students in the intervention significantly improved mental health knowledge, decreased stigma against mental illness, increased positive attitudes toward help-seeking, improved help-seeking behaviours, and decreased perceived stress compared to the control group. However, we did not identify significant changes in the general health outcome. This may be due to the relatively short follow-up time (2 months) to determine participants’ general health status, implying the extension of follow-up time for this measure in the future.
These findings are consistent with the previous research on earlier versions of the Transitions, reporting it to be a helpful resource with demonstrated benefits for student postsecondary life.40-42,47 The findings described herein not only replicated those findings in short term and further at 2-month follow-up using a more robust research design on more validated outcomes across different institutions. The finding that students who had lower mental health knowledge scores at baseline improved most indicates that it may be especially beneficial to students with a poor understanding about mental health. Students also demonstrated greater help-seeking behaviours for mental health problems, which supports the potential clinical relevance of this finding because students may be more knowledgeable about their mental health status and about where to seek appropriate services, resulting in potential early identification and treatment of mental disorders. Furthermore, this study first demonstrated significantly less stress in the intervention group compared to the control group. This is consistent with approaches suggested by other researchers48,49 and addressed the challenges that young people endorse a variety of negative emotions and coping challenges during the transition period to postsecondary life.15-21 These results suggest that the application of the Transitions may be of benefit in addressing mental health in postsecondary students.
Although each institution applied Transitions differently, institutions performed similarly on outcomes. This indicates that Transitions may be delivered using flexible formats and it allows for campuses to tailor its implementation so that it can be integrated into different campus culture and context. However, some delivery methods may provide enhanced outcomes. For example, including mental health providers in delivery of the mental health sections may enhance outcomes.
We found that gender, previous mental health education, or previous treatment experience did not influence how participants performed on all outcomes except for gender difference on the stigma and previous mental health treatment on the knowledge outcome. This may imply that exposure to Transitions will produce a similar impact on students regardless of these demographics. However, students with aboriginal, African, and immigrant/international background were not well represented in this sample, warranting further studies with participants of diverse backgrounds.
The study did not apply a randomized controlled design and we chose the control group participants purposefully, which may have biased the study results. The control group included students mainly from two colleges and one university campus and may have not included adequate samples from university settings, leading to potential bias of the results. Further, the relatively high attrition rate at a 2-month follow-up may have biased the longer-term results and limited its generalizability.
Conclusions
While mental health literacy could be an important component of a campus-wide approach to mental health 50 —this has, to date not been widely applied due to a dearth of evidence-based interventions, even if policies exist.51-55 Thus, Transitions provides a tool that could be used as an evidence-based solution to campus mental health concerns raised in public.56,57
Supplemental Material
sj-sav-1-cpa-10.1177_07067437211037131 - Supplemental material for The Impact of Transitions, a Mental Health Literacy Intervention With Embedded Life Skills for Postsecondary Students: Preliminary Findings From a Naturalistic Cohort Study
Supplemental material, sj-sav-1-cpa-10.1177_07067437211037131 for The Impact of Transitions, a Mental Health Literacy Intervention With Embedded Life Skills for Postsecondary Students: Preliminary Findings From a Naturalistic Cohort Study by Yifeng Wei, Stan Kutcher, Erin Austen, Anne Comfort, Chris Gilham, Christiana MacDougall, Greg McKenna, Margaret McKinnon, Kara Thompson, Elizabeth Yeo, Michael Zhang, Andrew Baxter and Kara Matheson in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
We thank Rebecca Alaffe for her data clearance and input for the project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medavie Health Foundation.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.