
Abstract
Objective:
To describe in what forms, with whom, where, when, and why Canadians experience sexual orientation and gender identity and expression change efforts (SOGIECE).
Methods:
This qualitative study is grounded in a transformative paradigm. We conducted semi-structured interviews with a purposive sample of 22 adults recruited from across Canada who have experienced “conversion therapy.” Directed content analysis was used, employing deductive and inductive coding approaches, to synthesize the findings and address 5 policy-relevant questions.
Results:
What are SOGIECE? Formal and informal methods of SOGIECE were used, including pharmacologic interventions, denial of gender-affirming care, and coaching to repress sexual orientation and/or gender identity and expression. With whom did SOGIECE occur? Practitioners included religious leaders, licenced health-care professionals (e.g., psychiatrists and psychologists), peers, and family members. Where did SOGIECE occur? SOGIECE occurred in 3 predominant settings: faith-based, health care, and social life. When did SOGIECE occur? SOGIECE rarely occurred over a restricted time frame; often, SOGIECE began while participants were adolescents or young adults and continued multiple years under various forms. Others described SOGIECE as a context in which their life was embedded for many years. Why did people attend SOGIECE? Cisheteronormative social and religious expectations taught participants that being non-cisgender or non-heterosexual was incompatible with living a good and respectable life.
Conclusions:
SOGIECE are not a circumscribed set of practices. Our study shows that SOGIECE are a larger phenomenon that consists of intentional and explicit change efforts as well as heterosexual- and cisgender-dominant social norms expressed and enforced across a wide range of settings and circumstances. This study provides critical context to inform contemporary social and health policy responses to SOGIECE. Policies should account for the overt, covert, and insidious ways that SOGIECE operate in order to effectively promote safety, equity, and health for sexually diverse and gender-diverse people.
Introduction
Non-heterosexual orientations and gender identities that do not align with sex assigned at birth are often pathologized by society as deviant and abnormal and therefore seen as requiring intervention to suppress or control them. Homosexuality was included in the Diagnostic and Statistical Manual of Mental Disorders (DSM) until 1973 1 and, in Canada, was criminalized until 1969. 2 Over 70 jurisdictions worldwide continue to view homosexuality as criminal. 3 Transgender and gender-diverse (trans) people remain pathologized (e.g., classification of gender dysphoria in the DSM-V), and their gender identity dismissed or disbelieved in Canada as well as criminalized around the world. 3 Biomedical and psychiatric “treatments” for those exhibiting homosexual and gender non-conforming traits have been (mis)named “conversion therapies,” despite being ineffective at conversion and not therapeutic, by most accounts. 4
Despite advancing policies to protect two-spirit, lesbian, gay, bisexual, trans, and other queer (2SLGBTQ+) people from discrimination, sexual orientation and gender identity and expression change efforts (SOGIECE), including practices referred to as “conversion therapy,” continue worldwide. 5 SOGIECE are a set of practices that attempt to change or suppress a person’s sexual orientation, gender identity, or gender expression to align with cisheteronormative notions of sexuality, gender, and gender expression. 5 –7 Cisheteronormativity refers to cissexism and heterosexism, which assume cisgender gender identities and heterosexual sexual orientations are more natural and legitimate than those of 2SLGBTQ people.
Contentious debates have ensued around definitions of “conversion therapy,” 8 which tend to capture only a fragment of practices that might be considered SOGIECE. Given the difficulty delineating between conversion therapy practices and SOGIECE, we use “SOGIECE” as an umbrella term to encompass the wide range of practices that attempt to alter or suppress one’s sexual orientation and/or gender identity and/or expression.
SOGIECE have been denounced as illegitimate by dozens of professional bodies. 9,10 Growing numbers of national and sub-national (e.g., state-wide or provincial) jurisdictions have enacted or proposed legislation to restrict or ban SOGIECE. 11 These laws have varied widely in how they have defined what constitutes SOGIECE. 6,12 Data from the United States and Canada demonstrate that between 5% and 20% of 2SLGBTQ+ people have experienced SOGIECE in their lifetime with some variation across age and geography. 7,13 –17 U.S. studies demonstrate that SOGIECE occur in religious settings, counsellor’s offices, and medical settings with health-care providers. 13,14,18 In the current context, trans people commonly experience SOGIECE in clinical settings and lesbian, gay, and bisexual people in religious settings, through practices targeting sexual orientations and gender identities. 13,14,18,19 These practices have ranged from physically invasive procedures, such as lobotomies and electroshock therapy, to psychological interventions, such as talk “therapies.”
Research on SOGIECE has tended to focus on addressing the prevalence, efficacy, and associated harms of these practices. 20 –22 Yet, there remain gaps in knowledge about the distinct manners and contexts in which SOGIECE occur, thereby challenging capacity to develop appropriate policy responses. Qualitative research is suited to addressing these shortcomings and to informing pertinent policy design strategies, as these approaches can provide in-depth characterizations of how SOGIECE are experienced as well as the broader contexts in which they occur. The purpose of this study was therefore to qualitatively explore the social context of SOGIECE in Canada and to describe why people experience SOGIECE, in what form, with whom, where, and when. The results of this study are intended to inform political conversations about how to intervene effectively and end SOGIECE.
Methods
This study is grounded in a transformative paradigm with explicit social justice aims of advancing health equity for 2SLGBTQ+ people. 23 Community engagement occurred throughout the research process, starting with development of research questions at a community-based event in fall 2019. 24
All authors have training and experience in qualitative methods. We adopt a reflexive stance to strengthen rigour of the study and arrive at this work given our personal experience and/or allyship with 2SLGBTQ+ communities and with varying experiences of SOGIECE. 25 –27 Our social identities and personal and professional relationships have led us to have close ties to 2SLGBTQ+ and conversion therapy–impacted communities with whom we have collectively worked for decades.
Following ethics approval from Université de Montréal (#CERSES-20-048-D) and Simon Fraser University (#2019s0394), we recruited 22 people with experience of “conversion therapy” using purposive sampling to maximize diversity on gender and sexual orientation. Participants were recruited through advertisements in English and French distributed through 2SLGBTQ+-serving community organizations’ listservs and social media as well as word-of-mouth through advocates for 2SLGBTQ+ communities. 28 Recruitment efforts included advertisements explicitly recruiting women and trans people and focused recruitment of Indigenous and 2-spirit people to increase sample diversity. Eligible participants were at least 19 years old, lived in Canada, spoke English or French, and reported to have experienced conversion therapy. The definition of conversion therapy used for recruitment was as follows: practices that try to change sexual attraction to people of the same gender (e.g., felt identity as lesbian, gay, bisexual, queer, etc.) or gender identities that are different from sex at birth (e.g., transgender).
In-depth, semi-structured, voice-recorded interviews lasting 60 to 150 minutes were conducted by D. J. K., T. G., and E. D. between January 31 and July 29, 2020. Recruitment ended after 7 months as analysis occurred iteratively with data generation, and information power was satisfied. 29 Participants provided verbal and/or written informed consent and sociodemographic information according to their preference—self-completed or during the interview—prior to or following the interview. Interviews began with a broad, open-ended prompt: “In your own time, tell me your story about experiencing [SOGIECE*].” The present analysis focusses on data primarily collected from this portion of the interviews. Four interviews were conducted in person and 18 via videoconferencing, given constraints of the COVID-19 pandemic.
Interviews were transcribed verbatim by a transcriptionist and checked for accuracy and deidentified by D. J. K., T. G., and E. D. NVivo12™ was used to manage transcripts during analysis. Directed content analysis was used to identify responses that might inform questions posed of the data, such as why, what, with whom, where, and when SOGIECE occur. 30 Specifically, we, D. J. K., T. G., and E. D., familiarized ourselves with the transcripts by carefully re-reading and discussing them in-depth, followed by an initial round of deductive coding, labelling content based on predetermined structural codes related to our research questions, our aim to understand the context of SOGIECE (e.g., who), and our knowledge of the subject and interviews. 31 The first author performed a second round of inductive coding using descriptive labels (e.g., religious leader) within the structural codes to identify patterns and organize the transcript data. During this round of coding, particular attention was given to contextual elements to identify the nuance and complexities of SOGIECE. Co-authors T. G. and E. D. reviewed the codes and labels assigned to data segments for accuracy and appropriateness in relation to the research question. During analysis, the research team met every 2 weeks to discuss the analytic process and review and discuss the analyst’s conceptual propositions to come to a consensus. Discussion of analysis in team meetings led to grouping findings into 3 primary themes (see Figure 1) with additional subthemes based on our predetermined structural codes. Findings are supported with verbatim quotations (Table 1).
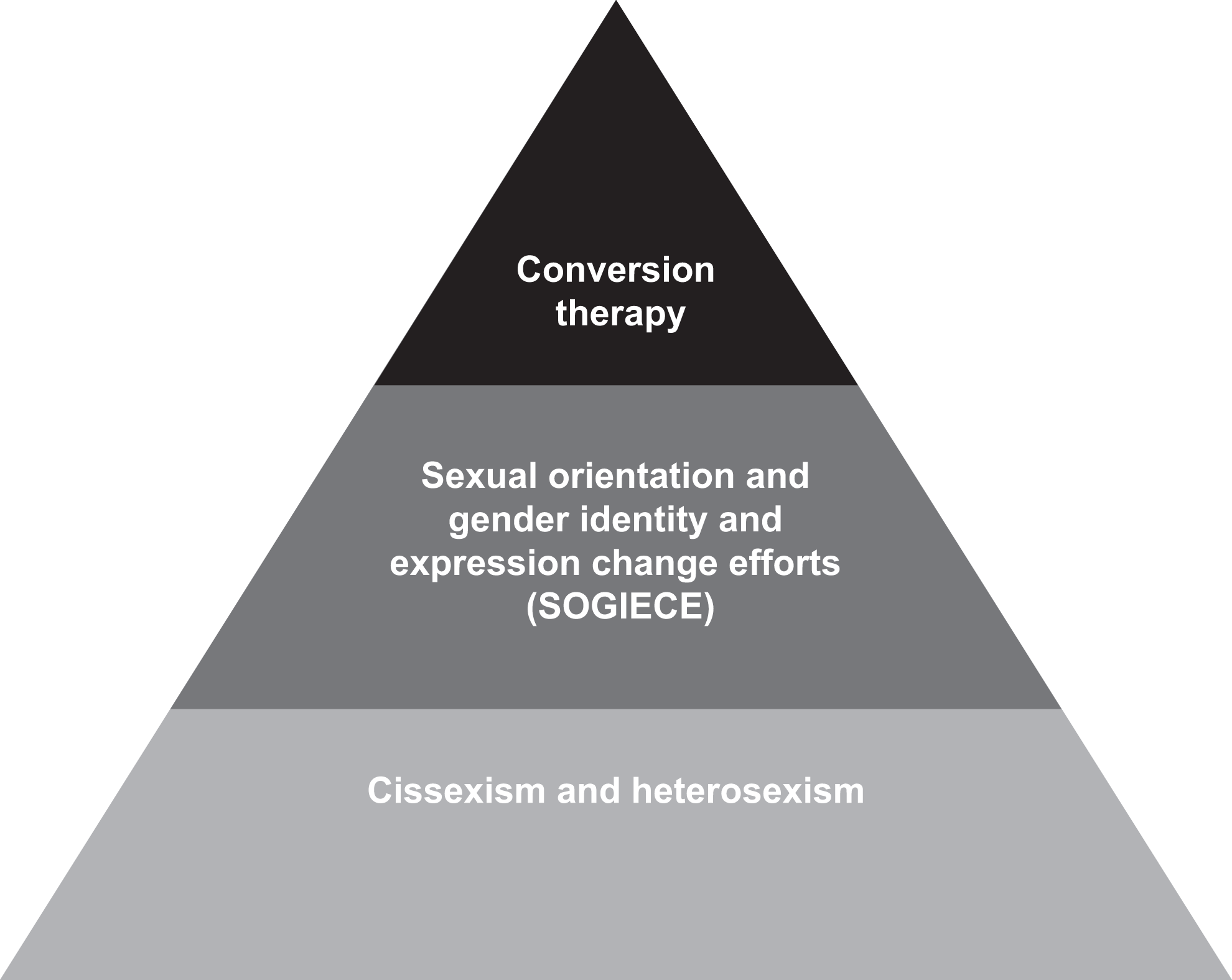
The sexual orientation and gender identity and expression change efforts (SOGIECE) pyramid, Canada, 2020.
Quotations from Participants in Study of Conversion Therapy, Canada, 2020.
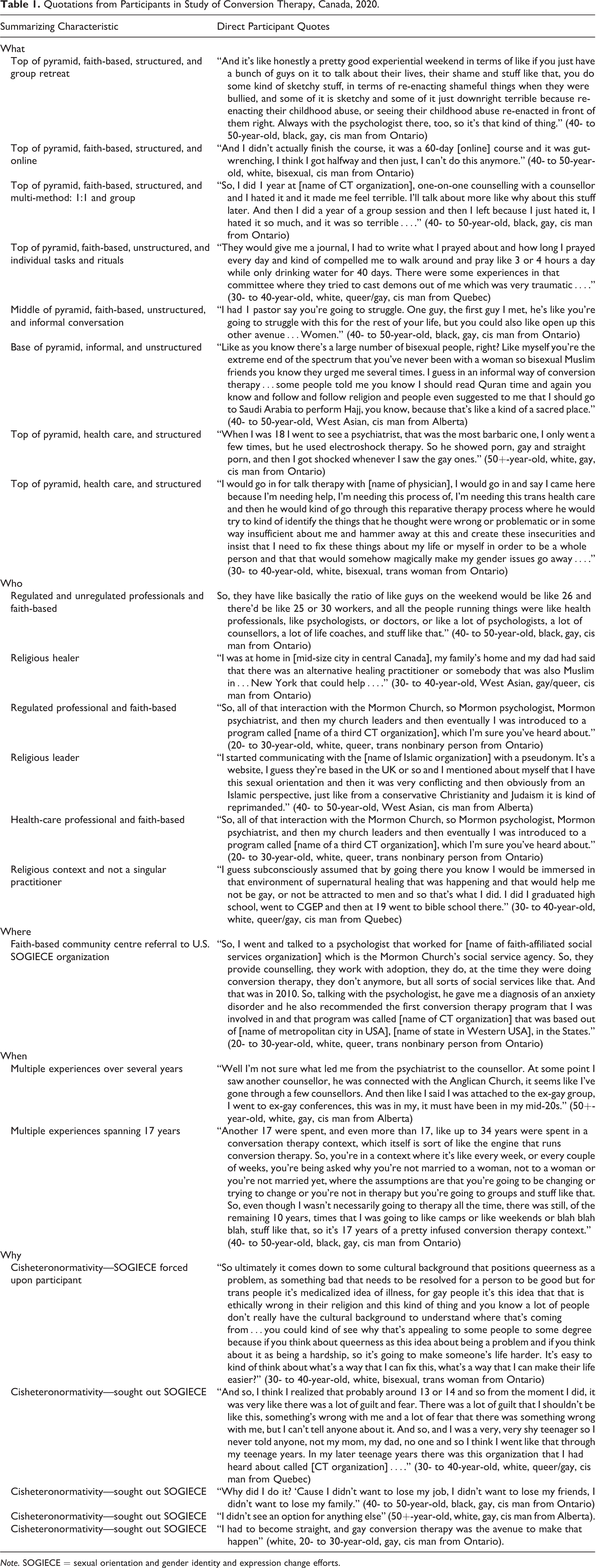
Note. SOGIECE = sexual orientation and gender identity and expression change efforts.
Results
SOGIECE occurred across religions, sexualities, genders, and races (Table 2). Participants described SOGIECE occurring through formal intervention, such as 1:1 or group counselling, as well as informal social intervention, such as family-based discrimination and encouraging cisnormative and heterosexual lifestyles. The forms of SOGIECE described by participants can broadly be categorized into 2 levels: conversion therapy (formal practices) and SOGIECE (including conversion therapy and less delineated efforts), both of which are undergirded by pervasive societal cissexism and heterosexism (Figure 1). These forms of SOGIECE reinforce one another and are not mutually exclusive. Participants shared stories of conventional conceptions of conversion therapy such as structured programming with the intention to suppress or change their “same-sex attraction.” Beyond this, participants shared experiences of attending physicians, psychologists, or religious leaders for at-times less formal but nonetheless explicit suppression or change (e.g., prescribing medication to reduce sex drive).
Participant Demographics, Canada, 2020.
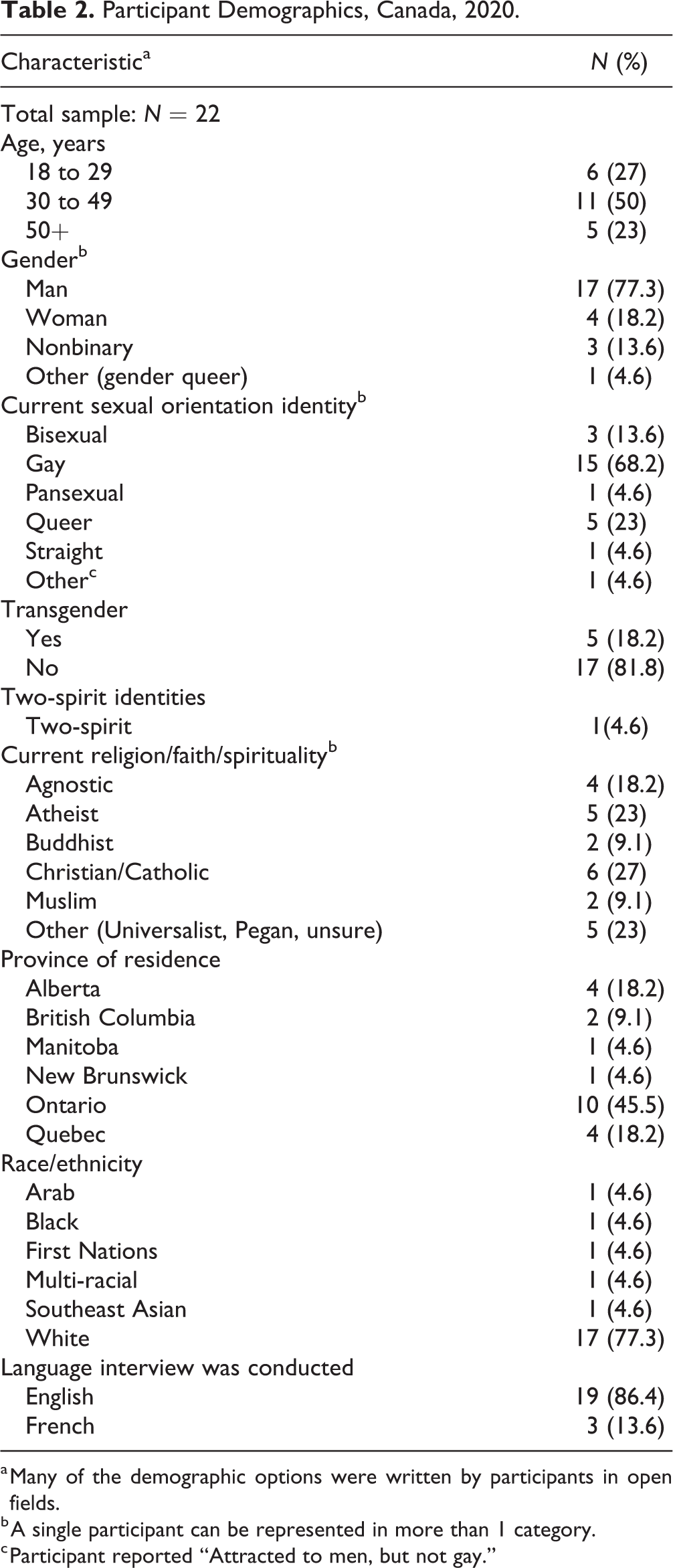
a Many of the demographic options were written by participants in open fields.
b A single participant can be represented in more than 1 category.
c Participant reported “Attracted to men, but not gay.”
Experiences shared also point to a broader social structure that sustain SOGIECE. Cissexism and heterosexism not only led participants to the experiences described but also resulted in social change efforts by family, friends, and community (e.g., telling someone to ignore their desires/identities and act in line with cisgender and heterosexual norms). Despite the intervention, SOGIECE primarily stemmed from beliefs that diverse sexual orientations and gender identities can and should be “fixed” or suppressed to conform to heterosexual and cisgender norms. Further, when participants were asked how they refer to or label their SOGIECE experience, most used “conversion therapy” or “reparative therapy” regardless of the form of SOGIECE. The reasons why participants experienced SOGIECE were varied, with overlap and differences between change efforts targeting gender identity and those targeting sexual orientation. Some trans participants encountered SOGIECE when seeking out gender-affirming health care, while many cisgender participants sought out SOGIECE based on religious convictions with a desire to change sexual orientation.
We present further detail of the results corresponding to questions often asked by legislators 8 : What does SOGIECE look like? Where is it happening and by whom? When do people go—is this an issue of minors and adults? Why do SOGIECE continue to happen? A summary can be found in Table 3.
SOGIECE Setting, Canada, 2020.

Note. SOGIECE = sexual orientation and gender identity and expression change efforts.
a Most participants experienced SOGIECE in Canada. In addition, many participants attended SOGIECE conferences, workshops, or camps internationally. Therefore, a single participant can be represented in more than 1 category.
b It was common for participants to share that though the aim of SOGIECE was to change their sexual orientation, this took the form of working on the way that gender was expressed. Therefore, a single participant can be represented in more than 1 category.
c It was common for participants to discuss working with health-care providers within faith-based contexts. Therefore, a single participant can be represented in more than 1 category. Further, participants frequently experienced more than 1 “type” of SOGIECE. Further, these categories do not encompass the settings where SOGIECE is experienced through social interventions.
What Does SOGIECE Look like, Where Does It Take Place, and Who Delivers it?
Conversion therapy
SOGIECE occurred in faith-based and secular settings, including licensed health-care offices, in person and remotely, and across Canada. Formal, structured forms of SOGIECE were observed targeting sexual orientation, gender expression, and gender identity. Further, SOGIECE targeting sexual orientation would often additionally address gender identity and/or expression. Participants described formal interventions as 1:1 counselling with a religious leader, group sessions held at churches or religious institutions, camp/retreat weekends, or conferences. Participants spoke of attending various types of “therapy” predominantly informed by ideology that “same-sex attraction” is a result of early sexual assault, an absentee father/domineering mother, a void in one’s life, or some religious groups claiming demonic possession.
Specific interventions included fasting, intensive prayer sessions, naked holding of other men, burning sentimental photos, practicing embodiment of stereotypical masculine qualities or engaging in masculine activities, persistent (psychological) assessment and denial of patient-determined gender identity in a medical setting, confronting parents for their role in why they (the participant) were “same-sex attracted,” re-enacting experiences of trauma and rebirth, sharing victories and failures of suppressing/avoiding non-heterosexual outcomes (e.g., “gay” porn), and psychoanalysis attempting to understand why someone was sexually diverse (i.e., where a parent was too present/absent or at what point during childhood they were molested).
The majority of these experiences occurred in person, though some participants spoke about completing courses online and reading literature which were intended to facilitate change independent of in-person interventions. Participants independently accessed and engaged with books on healing and/or changing one’s sexual orientation and fasted, prayed, repented, and read scripture in anticipation of facilitating change. Participant experiences promoted suppression and learning not to act on “same-sex temptations” and “urges” (Table 1—“what”).
Participants discussed leaving rural or suburban towns to access SOGIECE in urban centres in Canada and internationally. Participants often accessed SOGIECE from well-known U.S.-based conversion therapists, who came to conferences/events held in Canada. Likewise, participants travelled to the United States to engage in SOGIECE retreats and camps. Participants experienced SOGIECE through integrated health-care and faith-based services where psychologists and counsellors volunteered or worked for faith-based organizations. Faith-based SOGIECE practitioners included peer volunteers, religious leaders, and other religious life coaches, counsellors and health-care professionals, and support persons (Table 1—“where” and “who”).
SOGIECE
Participants also described SOGIECE in less formal ways, where religious leaders conducted exorcisms, psychiatrists performed electroshock therapy and hypnosis, and physicians denied gender-affirming care or prescribed medication to suppress sexual desires, all with the intention of correcting or suppressing one’s sexual orientation or gender identity. These experiences ranged from single occurrences to recurring “treatments” and were experienced as active change efforts (Table 1—“what”).
Exorcisms not only took place in formal change efforts described above but were also practiced in university and church service settings, where participants described immersion in “conversion therapy contexts” (i.e., conversion therapy under the guise of “spiritual healing”). Several participants spoke about attending U.S. and Canadian faith-based universities in order to access conversion therapy or immerse themselves in a setting that promoted spiritual healing.
Medical-based settings targeted 2SLGBTQ+ people in different ways, with two-spirit and trans participants describing consistently being denied gender-affirming care in health centres. Some trans participants left rural areas to seek gender-affirming care in urban health-care settings but were denied this care by providers that did not respect their gender identities or expression. Participants, where sexual orientation was the focus, experienced treatment from psychiatrists and physicians in clinic settings and were prescribed psychotropic medication and electroshock therapy to alter or suppress their sexual urges/preferences. Further, some sexually diverse participants sought international counsel by seeking advice from an Imam online or being unwillingly taken to the U.S. for support in the form of prayer and spiritual advice (Table 1—“where” and “who”).
Cissexism and heterosexism
SOGIECE occurred through social-level interventions that participants experienced regularly in their daily lives, both within formalized change efforts and insidious everyday interactions. Participants described experiencing overt cissexism and heterosexism asserted onto them as informal SOGIECE. This occurred through family members, friends, religious leaders, or health-care professionals telling participants to marry someone of the “opposite gender,” repress their feelings for the same gender, express their gender in ways that were inconsistent with how one felt (e.g., ascribe to stereotypical masculine characteristics), or encouraging someone not to come out or act in ways that affirmed their sexual orientation, gender identity, or gender expression. For example, a non-binary trans woman was told to suppress their gender identity by cutting their hair, changing their wardrobe, and reading bible verses. One cisgender gay man spoke about cultural pressures from religious family to marry a woman and have children while also being told by his friends to be bisexual so that he could maintain a family and be sexually satisfied outside of that arrangement despite having no attraction to women. Finally, another participant shared that he would frequently be told to walk and talk differently by family members in order to present himself as more masculine (Table 1—“what”).
When Do Individuals Experience SOGIECE?
Sexually diverse participants tried to deny their sexual orientations for years, having known something was different about them compared to their peers from a young age. They often entered SOGIECE as they were beginning to navigate their sexual orientation and/or gender identities. For some, this occurred in adolescence and others as young adults.
Many participants experienced SOGIECE over a number of years, sometimes taking long breaks followed by attending different forms of SOGIECE. One gay cisgender man discussed entering SOGIECE at the age of 17, experiencing 4 forms of SOGIECE at different times between the ages of 17 and 34. Some participants left SOGIECE after completing a time-specific program, and others were subjected for over a decade.
As some forms of SOGIECE are social and insidious, primarily categorized here in the base of the pyramid, SOGIECE was often described in ways that could not be restricted to a time frame. For instance, SOGIECE may have been experienced starting in childhood, continuing into adulthood, any time a participant entered a health-care setting, was surrounded by their family of origin or religious group, or was living in a context where they were not welcomed to live their authentic life. The point at which participants left SOGIECE can be described only for those who experienced SOGIECE in structured settings; however, for many, they continue to experience the cisheteronormativity that undergirds and sustains SOGIECE (Table 1—“when”).
Why Do People Continue to Experience SOGIECE?
Motivations for SOGIECE were multidimensional and derived from a variety of internal and external factors. Cisheterosexism, alongside years of internalized stigma, led participants to access various forms of SOGIECE. Participants often explained that they had entered SOGIECE voluntarily without explicit coercion. However, some participants shared fears of being kicked out, rejected from family, or feeling expectations and pressure to be straight that motivated them to access SOGIECE in adolescence and as adults. For some, they were directed to SOGIECE by their parents who felt that SOGIECE were in their child’s best interest. Further, participants spoke about societal and religious pressure to be straight, the inability to navigate faith and sexuality, and the fear and shame that accompanied their sexual identities. Cisheteronormative values were so embedded in participants’ upbringings that they did not consider non-cisgender or non-heterosexual life to be viable.
Participants were taught that to be sexually diverse was to be broken and in need of repair and that being trans was a mental illness necessitating treatment and “correction.” Participants frequently heard that homosexuality equated sexual deviance such as pedophilia or bestiality. They were also severely bullied for mannerisms or traits that were not conforming to gender roles or heard family members talk about sexually diverse “lifestyles” as disgusting. These experiences led to feelings of shame, fear, and grief that made SOGIECE a necessity.
Participants spoke about experiencing a need to conform to a circumscribed set of behaviours in order to maintain relationships with their communities of origin, whether that be religious, family, or friends. Further, some felt the need to hide and try to change their sexual orientation to keep employment, housing, and access to post-secondary education (i.e., through financial and/or material supports from family members). For example, 1 elementary school teacher, raised with egregious associations between homosexuality and pedophilia during his conservative upbringing, was fearful of accusations of pedophilia and dismissal if he identified as gay. This fear led him to seek out conversion therapy.
For some, participation in SOGIECE was not voluntary. Participants described seeking gender-affirming health care and encountering SOGIECE or having been coerced by family to see a religious healer. In these cases, participants did not express a desire to change their sexual orientation or gender identity but instead had others force SOGIECE upon them without consent (Table 1—“why”).
Discussion
Each dimension of the results elucidates the breadth and complexity of how SOGIECE are experienced. Rather than conceive of SOGIECE as a circumscribed set of practices that can be encompassed by a single definition, our study shows that we need to conceive of SOGIECE as a larger phenomenon that consists of intentional and explicit change efforts, both formal and informal, as well as heterosexual- and cisgender-affirming social norms expressed and enforced across a wide range of settings and circumstances. SOGIECE occurred through religious and health-care settings in what is conventionally understood as “conversion therapy” as well as less formal instances that included social contexts where 2SLGBTQ+ identities were devalued and cisgender and heterosexual identities were asserted. This demonstrates that SOGIECE are embedded in a deeper contemporary social structure that insidiously permits cisheteronormative interventions inclusive of conversion therapy.
Over half of the participants interviewed experienced SOGIECE in the last 10 years, echoing recent quantitative findings that SOGIECE remain prevalent in Canada. 16,17 Our findings indicate that SOGIECE take place in both regulated and unregulated settings, such as religious institutions and health care, similar to those found in international literature. 15,18 We add nuance to quantitative studies, showing how SOGIECE are often not framed as conversion therapy and even extend to instances of conversation with a persistent aim of persuading 2SLGBTQ+ people to deny or suppress their “same-sex attraction,” gender identity, and/or gender expression. Further, despite regulatory guidelines to restrict SOGIECE in licensed clinical settings, our research suggests that SOGIECE continues, especially through systematic denial of access to gender-affirming care for trans people—as documented elsewhere. 19,32
Participants were across Canada and diverse with respect to geography, age, religion, sexuality, and gender. We recruited a limited number of participants who experienced SOGIECE in medical settings, which may be a function of the relatively small number of trans-identified participants who have higher rates of SOGIECE when accessing health care. 15 Finally, all participants were adults, and most were no longer experiencing formal forms of SOGIECE, leading to findings that do not encompass experiences of youth or those currently experiencing formal forms of SOGIECE.
Despite efforts to recruit trans participants and women, our study is limited with the insights it can draw around change efforts targeting trans people and those experienced by women. Further, due to our focus on the practice of SOGIECE in participant interviews rather than early life experiences, we were unable to comprehensively understand the nuance that leads to someone experiencing SOGIECE and the decisions or coercion to undergo such experiences, particularly among trans people. As illustrated by the conversion therapy pyramid (Figure 1), SOGIECE do not occur in isolation of the social environment, as behaviours (e.g., conversion therapy) are embedded within systems and broader culture. This suggests that future research would benefit from adopting eco-social models for understanding how SOGIECE are embedded within broader social ecologies. 33
Our study provides critical context to inform contemporary policy and public health interventions that could improve the lives of 2SLGBTQ+ people (Table 4). Policies should take into consideration the overt, covert, and insidious ways that SOGIECE operate to effectively promote safety, equity, and public health. Interventions that respond to SOGIECE and the structures that sustain such practices are urgently needed. We encourage researchers, advocates, and practitioners to continue to expand pertinent policy efforts—including legislative bans, regulatory enforcement, and public education—without delay.
Recommendations.
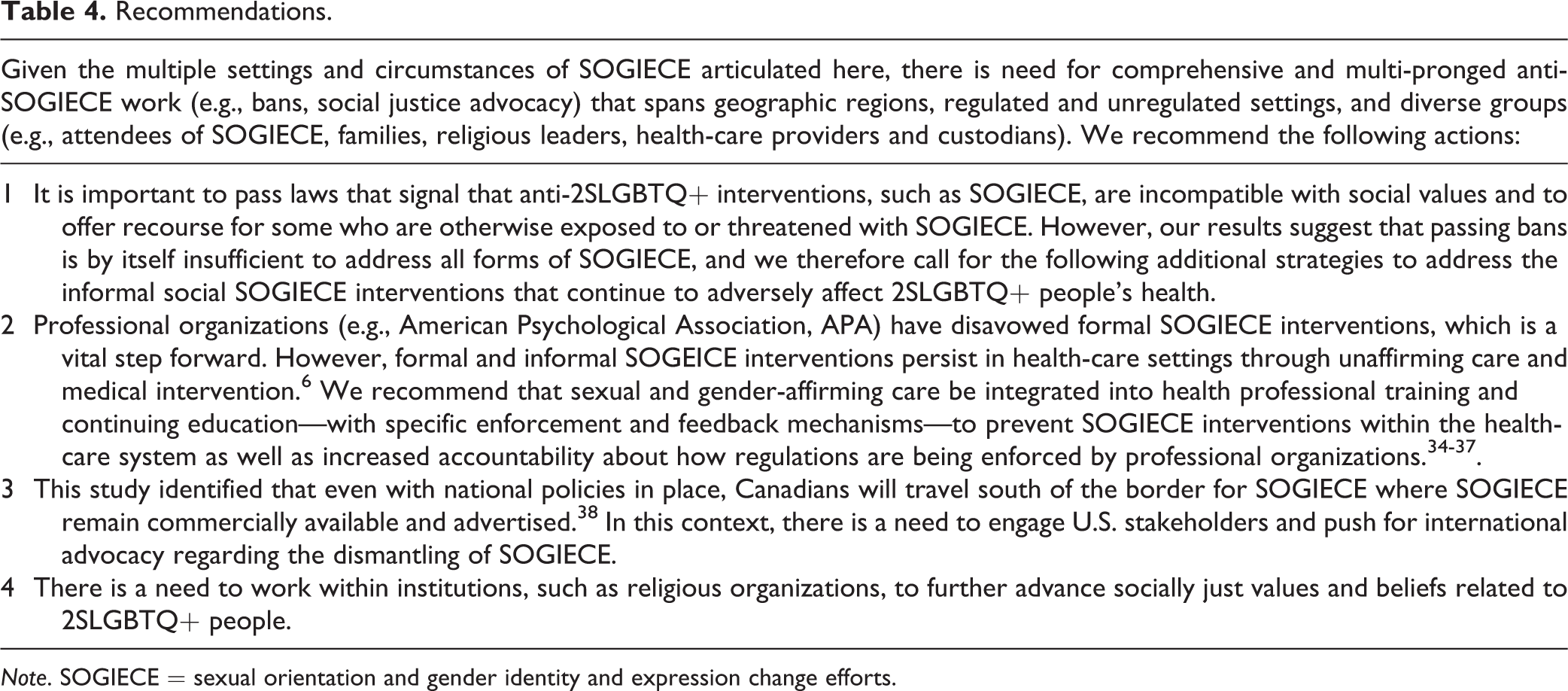
Note. SOGIECE = sexual orientation and gender identity and expression change efforts.
Footnotes
Authors’ Note
Data for this analysis are highly sensitive narrative accounts of personal experiences. Providing access to data is not ethical.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Simon Fraser University.