
Abstract
Objectives:
Patients admitted to psychiatric emergency services (PES) are highly heterogenous. New tools based on a transdiagnosis approach could help attending psychiatrists in their evaluation process and treatment planning. The goals of this study were to: (1) identify profiles of symptoms based on self-reported, dimensional outcomes in psychiatric patients upon their admission to PES, (2) link these profiles to developmental variables, that is, history of childhood abuse (CA) and trajectories of externalizing behaviours (EB), and (3) test whether this link between developmental variables and profiles was moderated by sex.
Methods:
In total, 402 patients were randomly selected from the Signature Biobank, a database of measures collected from patients admitted to the emergency of a psychiatric hospital. A comparison group of 92 healthy participants was also recruited from the community. Symptoms of anxiety, depression, alcohol and drug abuse, impulsivity, and psychosis as well as CA and EB were assessed using self-reported questionnaires. Symptom profiles were identified using cluster analysis. Prediction of profile membership by sex, CA, and EB was tested using structural equation modelling.
Results:
Among patients, four profiles were identified: (1) low level of symptoms on all outcomes, (2) high psychotic symptoms, (3) high anxio-depressive symptoms, and (4) elevated substance abuse and high levels of symptoms on all scales. An indirect effect of CA was found through EB trajectories: patients who experienced the most severe form of CA were more likely to develop chronic EB from childhood to adulthood, which in turn predicted membership to the most severe psychopathology profile. This indirect effect was not moderated by sex.
Conclusion:
Our results suggest that a transdiagnostic approach allows to highlight distinct clinical portraits of patients admitted to PES. Importantly, developmental factors were predictive of specific profiles. Such transdiagnostic approach is a first step towards precision medicine, which could lead to develop targeted interventions.
Introduction
Following deinstitutionalization in the mid-90s, psychiatric emergency services (PES) have become the new gate of entry for psychiatric and psychological services in Canada and the United States. 1 For many patients with severe psychopathology, PES has become their primary mental healthcare service. 2 –5 Patients visiting PES are a highly heterogeneous group, all consulting in a context of crisis, but presenting with different needs. 6 –8 Comorbidity between symptoms of depression, anxiety, drug/alcohol abuse, and psychosis is highly frequent among PES patients. 6,9,10 Women are more likely to receive diagnoses of mood and anxiety disorders and men diagnoses of antisocial personality and substance use disorders. 11 Since multiple diagnostic categories share the same symptoms and that symptoms are multi-determined, the likelihood of misdiagnosis is high upon admission to PES. 12,13 To offer optimal and personalized treatment, new approaches must be developed that do not rely solely on categorical diagnoses. 14 To do so, we propose to identify transdiagnostic psychosocial profiles of PES patients using both dynamic (i.e., current self-reported symptoms) and static (i.e., developmental vulnerabilities) indicators of psychopathology.
Dimensional Approach to Psychiatric Diagnoses
Decisions made during PES visits will affect subsequent treatment plans for patients and can influence the evolution of their psychopathology. Reasonable doubt exists about the clinical utility of psychiatric diagnoses in making these decisions. Studies have found that diagnoses made in the context of emergency services, both for generalist 13 and for psychiatric services, 15,16 are unreliable with the diagnosis often changing once the patient reaches the treatment unit. 17 Since there are many ways to meet criteria for a categorical diagnosis, patients with very different clinical presentations or even not sharing any symptoms can still receive the same label, resulting in a diagnostic heterogeneity. 18 –21 Moreover, since symptoms overlap between diagnostic categories, comorbid diagnoses are the norm rather than the exception. 22 –24 The resulting heterogeneity can further overshadow the evaluation of etiological and aggravating factors between patients with similar symptoms. 18 Finally, evaluating symptom intensity is also the occasion to identify relevant but subclinical symptomatology that can be at first overlooked but could devolve into full blown symptoms if not attended. 25,26 As such, diagnostic categories have limited clinical utility for identifying intervention and prevention targets, and, ultimately, prognosis. 27,28
A complementary approach to categorial diagnosis focusing on the transdiagnostic evaluation of symptoms, similar to the Research Domain Criteria (RDoC) approach proposed by the National Institute of Mental Health (NIMH), could help offer more targeted treatment to PES patients. 29,30 By cutting across diagnostic categories to focus on areas of functioning ranging from normal to pathological, the RDoC approach aims to identify the underlying common causes of mental health disorders. 31,32 As symptoms are more easily evaluated in terms of dimensions, this focus could not only help to identify areas of functioning requiring treatment or prevention interventions regardless of diagnosis but also to quantify the severity of the pathology, thus helping prioritizing resources toward patients with the biggest needs. As evaluating dimensions is more easily done using standardized self-reported measures than diagnostic interviews, it could be easily implemented in PES intake evaluations. Self-reported measures offer good measurement precision, can be used with non-clinical participants and patients regardless of their diagnosis, can be used in longitudinal designs, and have been found to be highly reliable. 33,34
A Developmentally Informed Approach to Diagnosis
Targeted interventions for PES patients require to be trauma-informed, as stressors and developmental adversity will affect how symptoms are expressed in patients and how they respond to treatment. 35 Chronic, severe stress, such as one resulting from childhood abuse (CA), can affect the development of neurobiological, cognitive, emotional, and behavioural systems. 36 In turn, these changes will shape adaptation or maladaptation to future stressful contexts, increasing the risk of a problematic developmental trajectory, from affect regulation problems to behavioural dysregulation. 37 As such, CA is one of the strongest predictors of different forms of adult psychopathology and non-specific clinical symptoms (e.g., anxiety, depression, psychosis, suicide risk, rule-breaking and substance abuse). 38 –41 While not specific to one form of psychopathology, cumulative CA is associated with symptom severity in adulthood, 42 accounting for 45% of the variance for psychopathologies with an onset during childhood and for 26% to 32% for those with a later onset. 39,43 Especially for boys, the most consistent impact of CA is the development of externalizing behaviours (EB), 44 –48 such as aggression, oppositionality, property violations, and status violations. Given that EB can change over time in terms of their severity and form, studies have favoured the use of a developmental perspective that includes several measurement points. 49 –52 As such, the more severe and chronic EB trajectories throughout the lifespan are predictive of the most severe mental health problems in adulthood compared to decreasing or increasing trajectories. 53 –55 Although these studies have highlighted the link between CA and EB, it is less clear how CA may exacerbate the development of EB in adolescence and psychopathology in adulthood. 56 To date, no studies have assessed the influence of CA and EB trajectories on clinical manifestations of mental illness at the time of admission to PES. Yet, hospitalization can be a stressful experience that can leave patients more vulnerable to develop pathologies, particularly for psychiatric patients who are still struggling with the consequences of prior adversity. 57,58 Including developmental trauma into PES intake evaluations could help treatment receptivity and lead to better prognosis and quicker patient release.
Objectives and Hypotheses
The main objective of this study was to identify psychosocial profiles of individuals presenting at PES by integrating results from different self-report clinical measures rather than relying on categorical psychiatric diagnoses. Second, this study aimed to explore the influence of developmental factors (i.e., CA and EB) on these profiles. Given the important sex differences with regards to the development of psychopathology, the third objective was to test whether the association between these developmental factors and profiles was moderated by sex. More specifically, we propose that CA would lead to more severe symptom profiles through the development of high, chronic EB and that this effect would be stronger for men than women.
Methods
Participants
Participants for this study were recruited as part of the Signature Biobank project (https://www.banquesignature.ca) of the Institut universitaire en santé mentale de Montréal (IUSMM), a specialized psychiatric institution in the province of Quebec, Canada. The Signature Biobank project aims to create a large psychiatric database by systematically collecting biological and psychosocial measures from all patients of the IUSMM upon their admission to the PES. All adult patients (i.e., aged 18 and above) admitted to the PES who were apt to provide consent were invited, with approval from their treating psychiatrist, to take part in this project by a nurse. Participants were excluded if they presented an intellectual or cognitive disability (such as dementia) limiting their ability to participate. Because of this last criterion, there are slightly less participants aged over 65 recruited in the Signature Biobank compared to the patient population of the IUSMM. The proportion of men who accepted to participate in the project is slightly higher than the IUSMM patient population. From its creation in November 2012, more than 65% of those approached for the study accepted to take part in the Signature project, for a total of 1,926 clinical participants recruited at the time of doing our analyses (May 2019), plus 157 comparison participants from the community (see below).
Clinical Sample
Based on a power analysis, a total of 402 participants (181 men) were selected randomly from the Signature Biobank to create our clinical sample. Weighted sampling stratified on sex was used to ensure that our sample matched the entire Biobank population on sociodemographic variables. As hair samples were also collected as part of a bigger project (not discussed in the current article), participants were excluded if they were unable to provide such samples (46.7%). While some differences between the current sample and the Signature Biobank population can be found on age, diagnoses, and scores on the self-reported measures, their small effect sizes (d ranging from .12 to .25) suggest that the representativeness of the sample was adequate (see Supplemental Tables 1 and 2).
Community Sample
A comparison group of 92 healthy participants from the community was recruited. Participants were matched to the Signature Biobank on age, sex, and socioeconomic status. Individuals were excluded based on the following criteria: (1) having done rehab in the last year for alcohol or drug abuse, (2) having used PES in the last 5 years, (3) presenting psychotic symptoms on the Community Assessment of Psychic Experiences-Positive, 59 or (4) reporting bipolar symptoms in the last 12 months, as assessed by the Mood Disorder Questionnaire. 60 As participants in the Signature Biobank had to provide biological samples, they were also excluded if they were pregnant, currently breastfeeding, or taking cortisone-based medication to ensure the validity of these samples.
Measures
Sociodemographic and psychiatric variables
Biological sex and age were included in our statistical models as predictors. For descriptive purposes, psychiatric diagnoses, established by the attending psychiatrist following the admission evaluation, were obtained by reviewing each participant’s patient files.
Developmental factors
Experiences of CA perpetrated by adults before the age of 16 were assessed using the abbreviated version of the Childhood Experiences of Violence Questionnaire. 61,62 The Brown-Goodwin Lifetime History of Aggression (BGHA) questionnaire 63,64 was used to evaluate EB during four stages of life: early childhood (i.e., < 12 years old), early adolescence (i.e., between 12 and 15 years old), late adolescence (i.e., between 16 and 17 years old), and adulthood (i.e., ≥ 18 years old).
Clinical symptoms
Problematic alcohol and drug use in the last 12 months were assessed using, respectively, the Alcohol Use Disorders Identification Test 65,66 and the Drug Abuse Screening Test. 67,68 Impulsivity was measured using the Impulsive Behavior Scale, 69,70 with scores averaged across its 5 subscales. Trait anxiety was measured using the short version of the State-Trait Anxiety Inventory, rescaled to the original form. 71 Depressive symptomatology was assessed using the self-administered version of the Patient Health Questionnaire-9. 72,73 Finally, positive psychotic symptoms were measured using the Psychosis Screening Questionnaire 74 (see Table 1 for more details on these scales).
Details about the Self-reported Questionnaires.
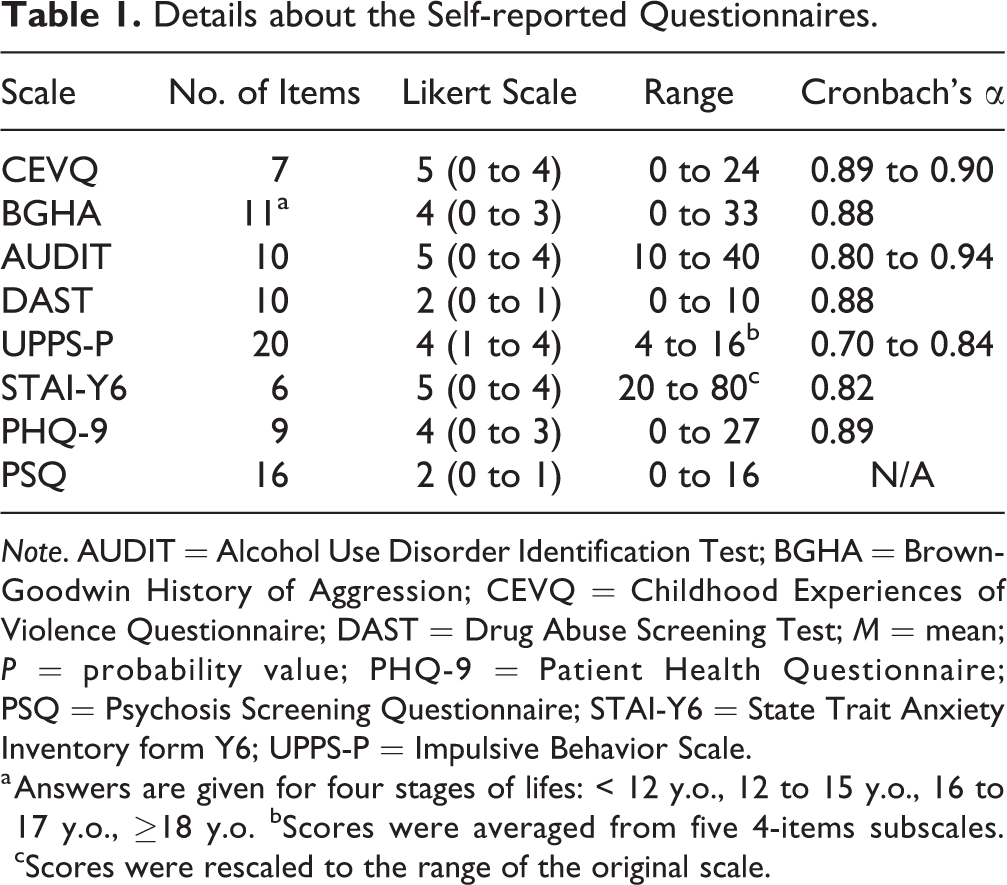
Note. AUDIT = Alcohol Use Disorder Identification Test; BGHA = Brown-Goodwin History of Aggression; CEVQ = Childhood Experiences of Violence Questionnaire; DAST = Drug Abuse Screening Test; M = mean; P = probability value; PHQ-9 = Patient Health Questionnaire; PSQ = Psychosis Screening Questionnaire; STAI-Y6 = State Trait Anxiety Inventory form Y6; UPPS-P = Impulsive Behavior Scale.
a Answers are given for four stages of lifes: < 12 y.o., 12 to 15 y.o., 16 to 17 y.o., ≥18 y.o. bScores were averaged from five 4-items subscales. cScores were rescaled to the range of the original scale.
Procedure
After giving a written consent, participants had to answer the battery of self-reported psychosocial questionnaires the day upon their admission to the PES. Questionnaires were answered on a customized iPad application, with data securely linked to the database. Questionnaires were administered and biological samples were collected by trained research nurses. Participants received $20 CAD for their participation. All procedures were approved by the Institutional Review Board of the IUSMM.
Statistical Analyses
First, independent samples t tests and χ2 tests were used to compare both groups on sociodemographic and all outcome variables. Then, developmental trajectories of EB, based on behaviours reported by the participants on the four stages of life of the BGHA, were identified using latent class growth analyses. Also, following a dimensional conception of psychopathology, latent class analyses were performed to identify psychosocial profiles that integrate the following variables: depression, anxiety, psychotic symptoms, impulsivity, alcohol, and drug use. The optimal number of clusters was identified using ensemble learning clustering, which generated clusters based on the agreement in group attribution of each participant between three different clustering techniques (i.e., k-means, hierarchical clustering, and Gaussian mixture model). Finally, the links between CA, EB, and psychosocial profiles were explored using structural equation modelling with logit link. More specifically, we aimed to determine whether the psychosocial profile membership of individuals presenting at PES was predicted by CA and EB (both as direct and indirect effects) while adjusting for age and sex. To test whether differences were observed based on biological sex, moderation analyses were performed using multi-group method. Analyses were computed using Mplus 7.3 and the ClusterR 75 on R. Significance level was set at 0.05 for all analyses.
Results
Descriptive Analyses
Sociodemographic information as well as mean and standard deviations for all outcomes can be found in Table 2 (see Supplementary Table 3 for the main psychiatric diagnoses of the clinical group). Both groups were similar on age and sex distribution. The clinical group scored significantly higher than the comparison group on all self-reported clinical symptoms. They also reported higher EB across all stages of life as well as more frequent and severe forms of CA relative to the comparison group.
Sociodemographic Variables and Main Outcomes for the Clinical and Comparison Groups.
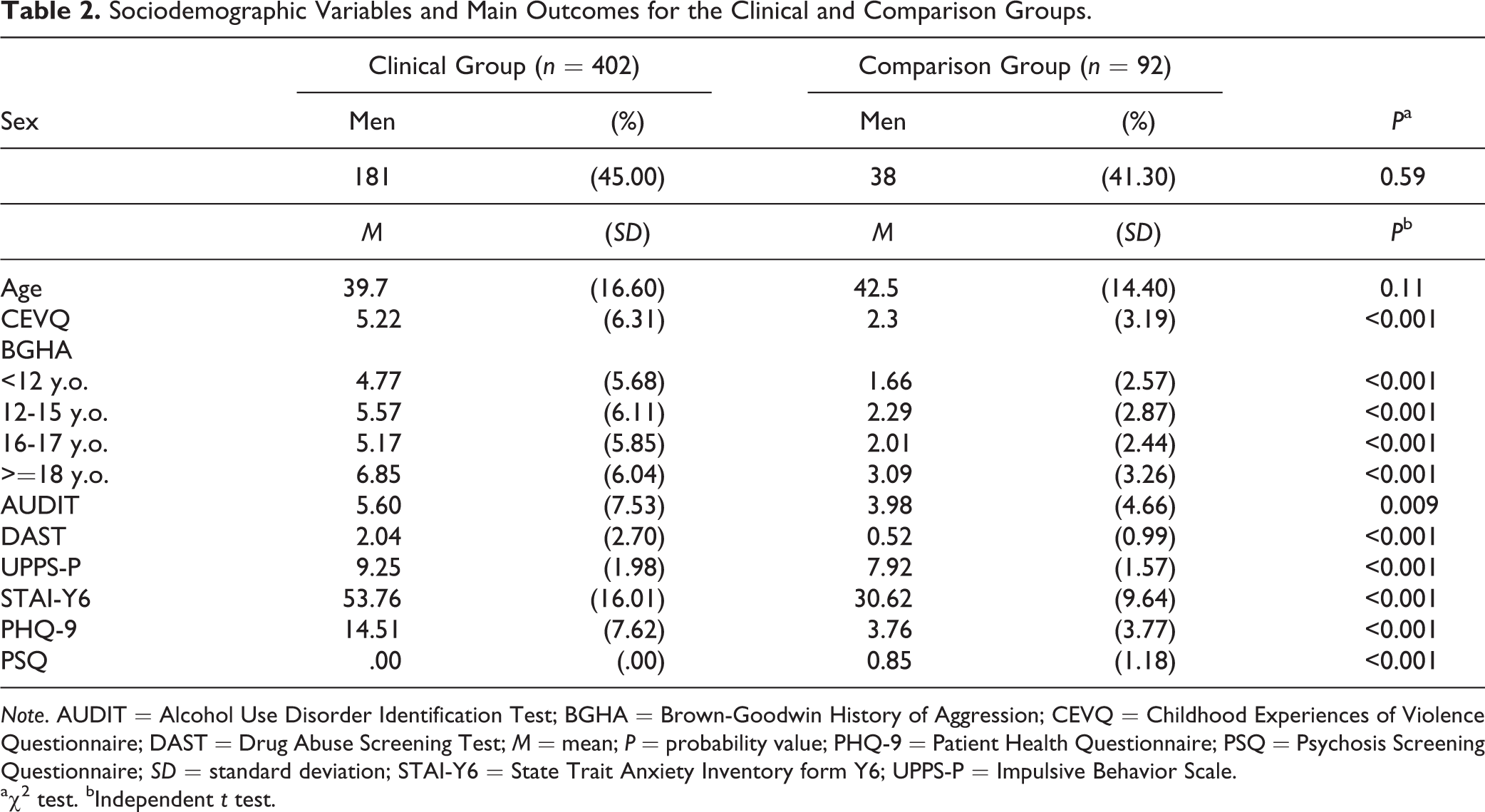
Note. AUDIT = Alcohol Use Disorder Identification Test; BGHA = Brown-Goodwin History of Aggression; CEVQ = Childhood Experiences of Violence Questionnaire; DAST = Drug Abuse Screening Test; M = mean; P = probability value; PHQ-9 = Patient Health Questionnaire; PSQ = Psychosis Screening Questionnaire; SD = standard deviation; STAI-Y6 = State Trait Anxiety Inventory form Y6; UPPS-P = Impulsive Behavior Scale.
aχ2 test. bIndependent t test.
Psychosocial Profiles
Latent class analysis for the clinical sample was performed on the standardized scores of the psychosocial measures. Results from the specific clustering techniques used can be found in the Supplementary Figure 1. Ensemble learning clustering converged towards a solution with 5 groups. Yet, a 4-group solution, which combined 2 groups distinct only on their alcohol and drug use from the previous solution, was also tested. This more parsimonious solution was kept for further analyses (see Supplementary Figure 2 for the 5 group solution).
Means of each profile and the comparison group on the psychosocial measures can be found in Figure 1. The first profile (n = 134) was characterized by low levels of symptoms on all scales. A second profile (n = 44) was associated with high positive psychotic symptoms (e.g., delusions or hallucinations). The third profile (n = 117) presented with an anxio-depressive symptomatology. Finally, the fourth profile (n = 94) had alcohol and/or substance abuse problems combined with high levels of symptoms on all other scales. The comparison group was similar to the first clinical profile with even lower reported anxio-depressive symptoms (see Supplemental Table 4 for proportions of profiles by diagnostic categories).
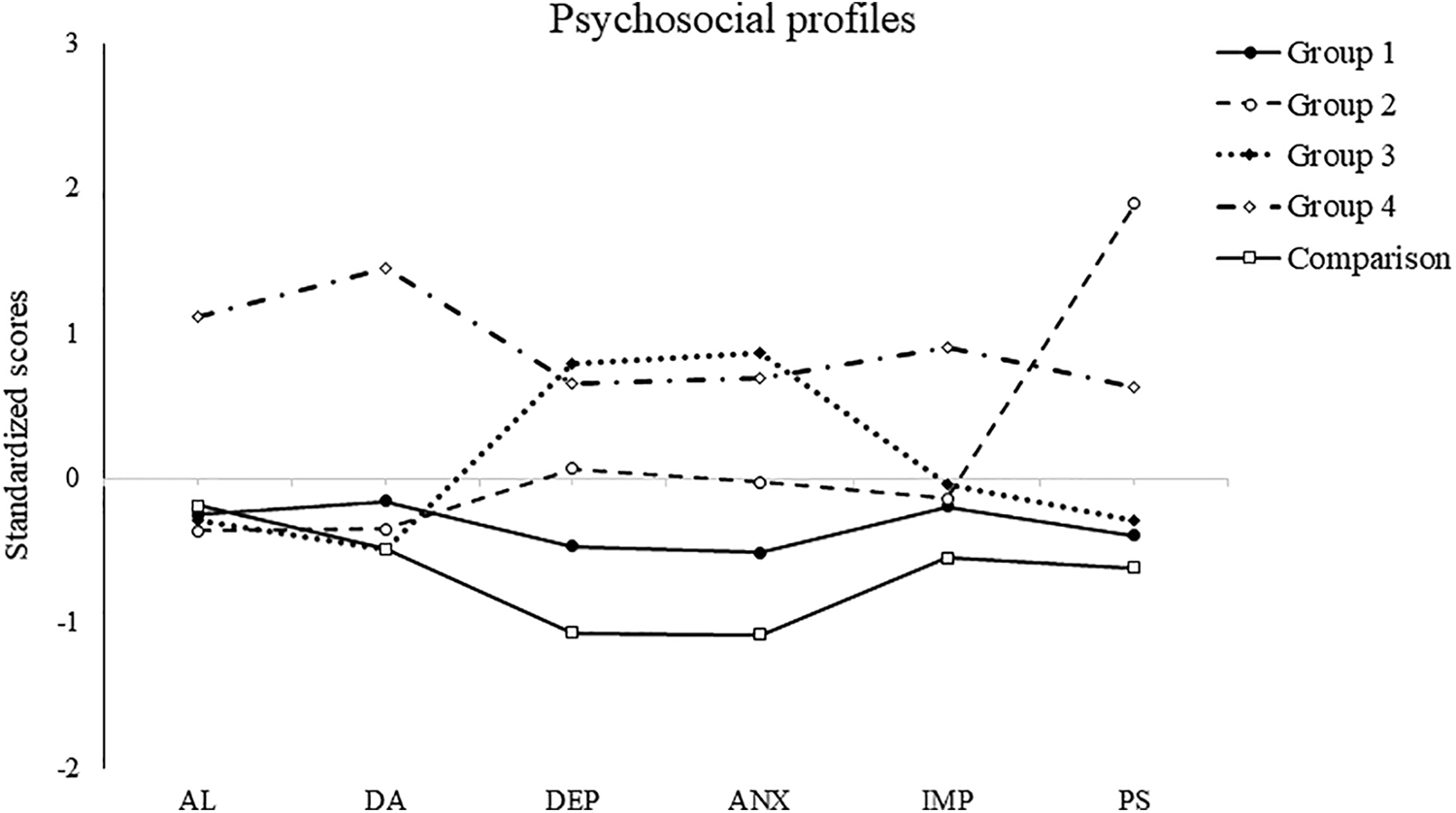
Psychosocial profiles of the clinical group. Note. AL = alcohol abuse; ANX = anxiety symptoms; DA = drug abuse; DEP = depressive symptoms; PS = positive symptoms.
Externalizing Behaviours Trajectories
Models with 1 to 5 trajectories of EB through the 4 stages of life were tested and compared on fit indices (see Supplementary Figure 3 for the fit indices of each model). The model with the best data fit was composed of 4 distinct trajectories (see Figure 2): (1) low EB throughout the lifespan (n = 81), (2) increasing frequency of EB throughout adolescence and adulthood (n = 148), (3) high frequency of EB in childhood decreasing throughout adolescence and adulthood (n = 27), and (4) high, chronic EB throughout the lifespan (n = 146). The comparison group’s trajectory was similar to that of the low EB clinical group.
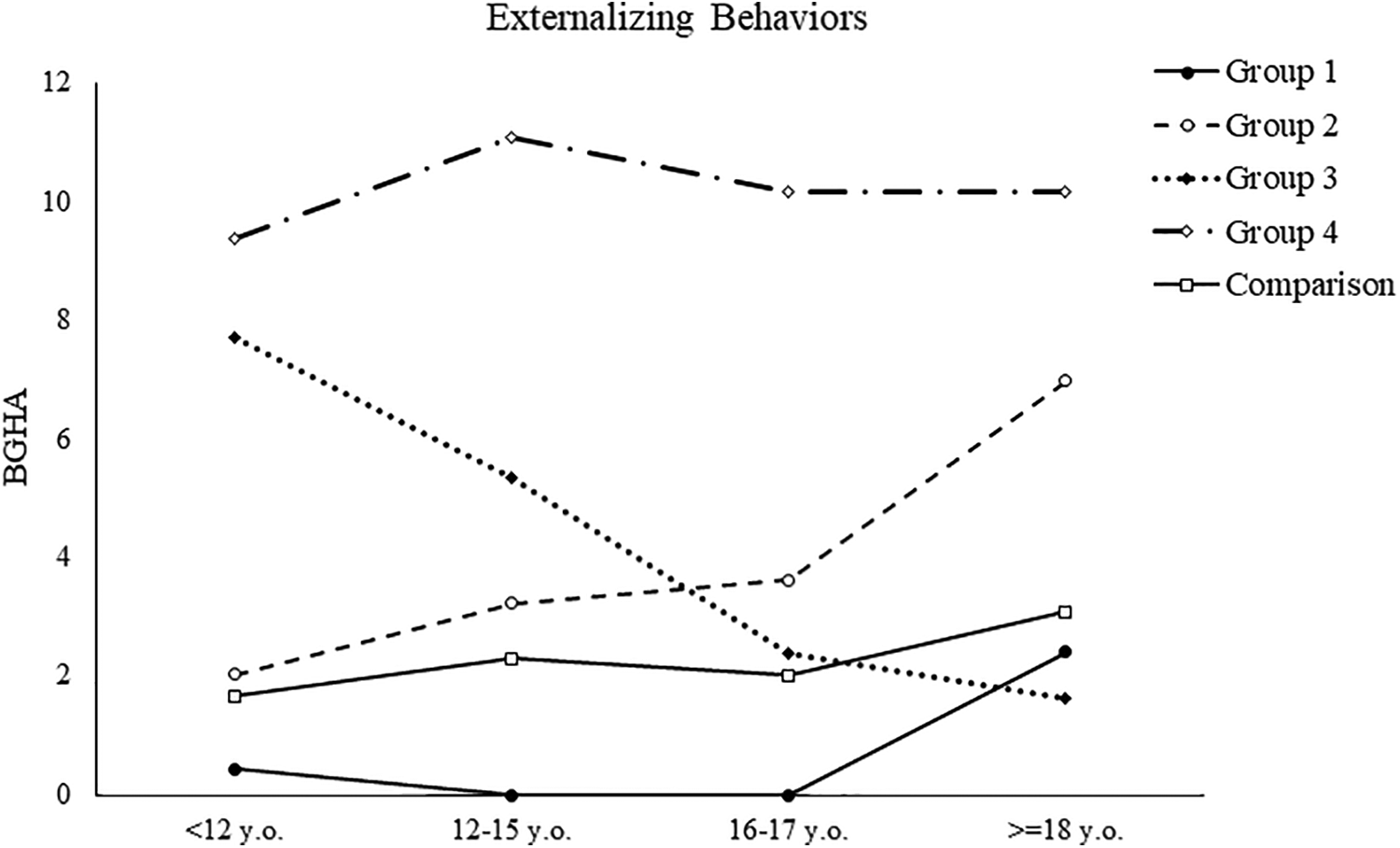
Externalizing behaviours trajectories from childhood to adulthood for the clinical group. Note. BGHA = Brown-Goodwin History of Aggression.
Predicting Profile Membership
The structural equation model of profile membership, with the low symptoms profile as the reference group, can be found in Figure 3 (see Supplementary Figure 4 for the 5 group solution). EB were entered in the model with the high chronic trajectory as the reference category, and sex with men as the reference.
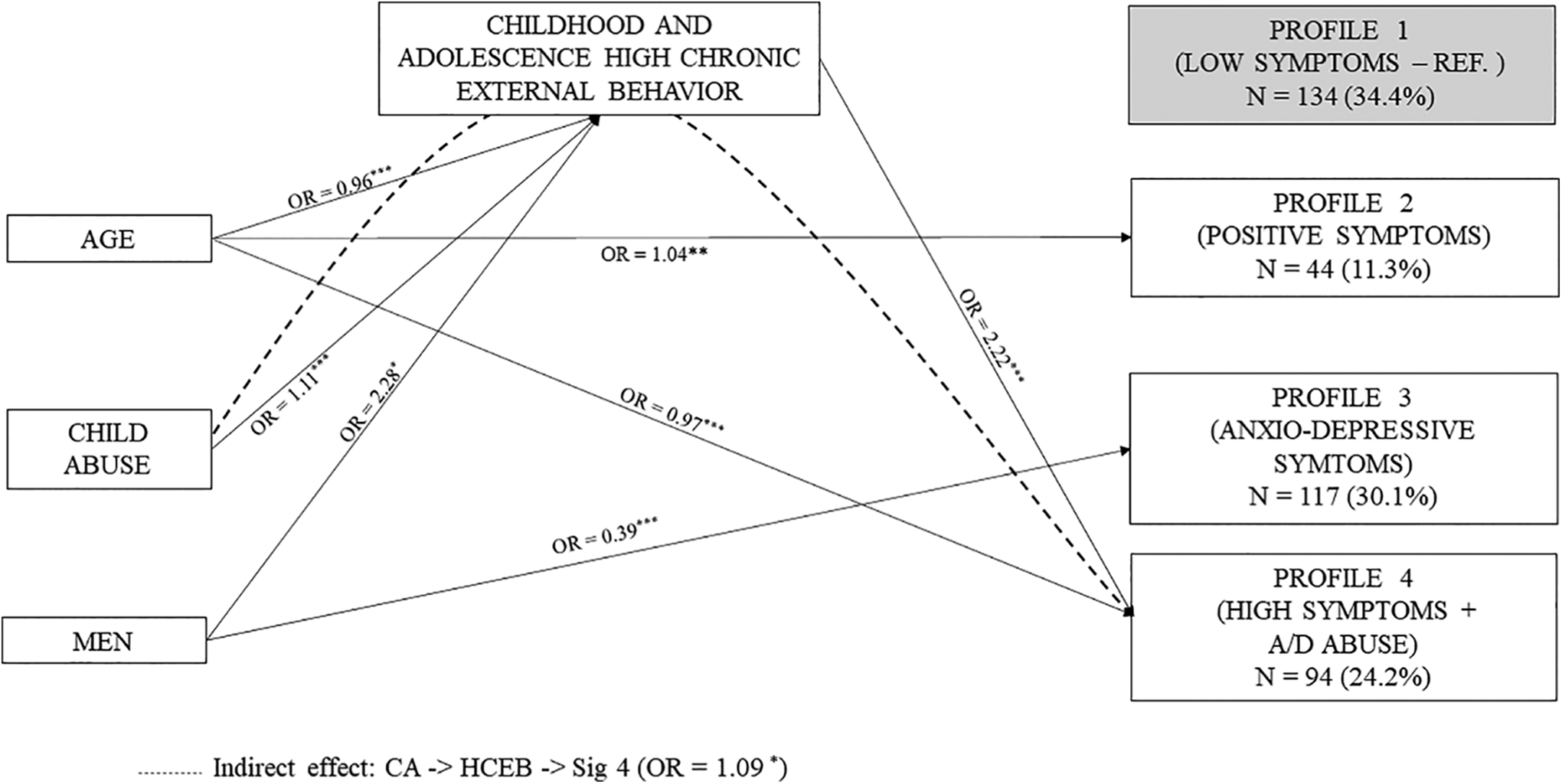
Prediction of psychosocial profile membership. Note. Only significant links are presented. A/D = alcohol/drug; OR = odds ratio; REF = reference category.
As expected, higher experience of CA was predictive of high, chronic EB (OR = 1.11). In turn, these behaviours were significantly predictive of membership to the profile characterized by high symptoms of alcohol/substance abuse (OR = 2.22). Mediation analysis revealed a significant indirect effect, as membership to this last profile was explained by CA through EB trajectories (OR = 1.09). While men were more likely to report high, chronic EB (OR = 2.28) and less likely to present an anxio-depressive symptomatology (OR = 0.39), sex was not a significant moderator of the link between EB trajectories and profile membership.
Discussion
The main goal of this study was to go beyond psychiatric diagnoses by identifying psychosocial profiles of patients admitted to PES using dimensional, self-reported measures and to link these profiles to developmental indicators of mental health problems (i.e., CA and trajectories of EB). Confidence in the identified profiles was improved by using ensemble learning clustering technique, that is, selecting a solution based on the agreement of different techniques rather than only one. While other studies used similar techniques in the general population (e.g., El-Gabalawy et al., Olino et al., Vaidyanathan et al., and Weich et al. 76 –79 ) our study is the first to do so using a randomly selected clinical sample of 402 patients admitted to PES. As expected, the clinical group scored significantly higher on clinical symptoms, CA, and EB than the comparison group. Four distinct constellations of symptoms were identified within the clinical group: (1) low level of symptoms on all outcomes, (2) high psychotic symptoms, (3) high anxio-depressive symptoms, and (4) alcohol and/or drug abuse combined with high levels of symptoms on all other scales. While we were unable to replicate the link found in the literature between CA and psychopathology severity when we attempted to predict profile membership, our results identified a more complex relationship. A significant indirect effect of CA was found through EB trajectories: patients who experienced the most severe and frequent form of CA were also those who showed high, chronic trajectories of EB from childhood to adulthood, which in turn predicted the most severe symptoms profile, that is, alcohol and/or drug abuse combined with high symptoms on all other scales. Sex differences were found, with men being more likely to present high, chronic EB trajectories and less likely to belong to the anxio-depressive profile. Yet, the link between EB trajectories and profile membership was not moderated by sex.
Our results represent a further step toward precision medicine for PES patients. 80 This is of particular importance as the usefulness of categorical psychiatric diagnosis upon admission to PES is limited, with studies showing low interrater reliability and suggesting that comorbidity is the rule rather than the exception. 22 –24 As misdiagnosis can mean unnecessary treatment leading to important human and financial costs, 81 it becomes important to identify intervention targets that are based on a continuum of symptoms ranging from normal to pathological. 14 By recruiting both a clinical sample and a community-based one, and by relying on dimensional measures of symptoms, we were able to identify profiles of psychiatric patients upon admission to PES. As these measures are self-administered, they could easily be added to the evaluation process as a transdiagnostic screening tool upon admission to PES: based on the severity of symptoms reported, a clinician could choose to further investigate with a clinical interview the psychopathology assessed and tailored their intervention according to the different dimensions of the psychopathology manifested by the patient. This could help to allocate resources by targeting clinical symptoms requiring priority intervention and subclinical symptoms needing preventive monitoring. It could also help clinicians to navigate through diagnostic heterogeneity by highlighting relevant clinical symptoms that could be overshadowed by a patient’s diagnosis. Future studies are needed to determine whether these profiles have any predictive value in terms of clinical care, such as treatment receptivity and prognosis or inpatient violence risk assessment.
Another implication of our results for targeted interventions is that not only current symptoms are important to identify profile membership but developmental factors could inform about the likelihood of belonging to specific profiles. While symptom presentation at intake is important, clinicians should also consider indicators of chronicity and severity such as CA and EB, which could be done, again, using self-reported measures. In fact, our results indicate that profiles with more severe symptoms coupled with substance abuse can be traced back to childhood and adolescence in the form of high, stable EB trajectories with CA as a likely starting point. While treating symptoms of the acute phase requires to identify proximal causes, targeting distal causes of mental health problems such as trauma would improve treatment efficacy by focusing more resources on patients with greater developmental difficulties. As the combination of CA and EB has been found to be predictive of readmission to psychiatric services in youth, 82 targeting these distal causes in adults could help prevent their rehospitalization in the long run. Trauma-informed interventions could also help improve treatment receptivity, as treating individual manifestations of psychopathology requires to understand past and present adversities experiences by this person. 83 Evidently, EB are only but one possible manifestation of CA and could be associated with different processes that could be individually targeted in treatment, for example, impulse control, anger management, or emotion regulation. Future research should include measures to identify such processes and how they relate to psychosocial profiles.
Limits
Some limits to our results should be mentioned. First, doubts from practitioners 84 and researchers alike 85 have been formulated about using self-reported outcomes with psychiatric patients, particularly those highly disorganized or in acute emotional distress. Yet, studies have found that answers on self-reported measures are reliable and valid for both psychiatric outpatients 86 and inpatients. 32 Still, using information from multiple sources with possible cross-confirmation would help improve confidence in our results. The same limit applies to how we measured EB trajectories which could be affected by a retrospective bias. Using a longitudinal design would not only improve the validity of the trajectories but also of the mediation analysis performed. Finally, by including only EB in our measures, we might have overlooked another important mental health indicator, namely, internalizing behaviours, which are more frequently observed in women. 11 Thus, it is possible that a more complex model could have been identified, for example, by linking less severe profiles with past internalizing behaviours or by identifying moderation effects of biological sex on the link between a possible internalizing/externalizing continuum 45,87 and psychosocial profile membership. Future studies should include both externalizing and internalizing behaviours as indicators.
Conclusion
This is the first study to identify psychosocial profiles in PES patients using dimensional, self-reported measures of symptom severity, CA, and EB. Our study is a first step towards precision medicine for PES patients and underscores the importance to evaluate acute clinical symptoms as well as developmental factors of psychopathology. By adding self-reported measures into their evaluation, clinicians could more easily offer treatments that are tailored to an individual’s profile by highlighting intervention and prevention targets outside of those based on categorial diagnosis alone. It could also improve treatment receptivity by identifying patients with potential past trauma that would need special attention.
Supplemental Material
Supplemental Material, sj-pdf-1-cpa-10.1177_07067437211018793 - Psychosocial Profiles of Patients Admitted to Psychiatric Emergency Services: Results from the Signature Biobank Project: Profils Psychosociaux de Patients Admis Dans des Services d’Urgence Psychiatrique : Résultats du Projet Banque Signature
Supplemental Material, sj-pdf-1-cpa-10.1177_07067437211018793 for Psychosocial Profiles of Patients Admitted to Psychiatric Emergency Services: Results from the Signature Biobank Project: Profils Psychosociaux de Patients Admis Dans des Services d’Urgence Psychiatrique : Résultats du Projet Banque Signature by Steve Geoffrion, Kévin Nolet, Charles-Édouard Giguère, Tania Lecomte, Stéphane Potvin, Sonia Lupien and Marie-France Marin in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
Acknowledgments
The authors would like to thank Sandra Favret and Janick Boissonneault, research coordinators for the Signature Biobank, as well as Carole Feltrin, Nabil Khiari Martha Françoise Ulysse, research nurses who collected the data. The authors would also like to thank all the patients from the IUSMM who accepted to be part of this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Bell Let’s Talk (#1024384), a major donor of the Fondation de l’IUSMM.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.