
Abstract
Objective:
Although there is evidence of effective stigma reduction by various psychological and educational interventions, the mechanisms of change remain unclear. In this article, we examine hypothesized processes that might have mediated reductions in stigma observed among Asian men who had received in mental health promotion interventions in Greater Toronto Area, Canada.
Method:
Our sample consisted of 495 Asian men, who received either acceptance and commitment therapy (ACT; n = 133), contact-based empowerment education (CEE; n = 149), combination of ACT and CEE (n = 152), or psychoeducation (n = 61). Group differences on intervention outcomes, including stigmatizing attitudes (Community Attitudes toward the Mentally Ill), internalized stigma (Internalized Stigma of Mental Illness), valued living (Valued Living Questionnaire), and attitudes to engage in social change (Social Justice Scale) were hypothesized to be due to the impact of the different interventions and mediated by changes in specific underlying psychological processes. These process-related changes were modelled using measures of mindfulness (Freiburg Mindfulness Inventory), psychological flexibility (Acceptance and Action Questionnaire version II), and empowerment (Empowerment Scale [ES]). Their pre- and post changes were analyzed with repeated measures analysis of variance, and mediational analyses were performed.
Results:
Findings from mediational analyses suggest that empowerment (ES) mediated a significant portion of the effects observed in reduction in stigmatizing attitudes and internalized stigma across intervention groups (t = 3.67 to 3.78 for CEE groups, and t = 4.32 to 4.56 for ACT groups). For the ACT groups, reduction in internalized stigma might also have been partly mediated by psychological flexibility, an intervention-specific psychological process.
Conclusions:
Results from the current study suggest that different stigma reduction interventions may be mediated by increased empowerment as a common mechanism of change, while intervention-specific mechanism of change, improved psychological flexibility through ACT, may also contribute to improvement in internalized stigma.
Introduction
Background
Mental illness stigma and discrimination is a significant challenge in mental health care. 1 Whether embodied by individuals, affecting interpersonal relationships, or embedded at the societal or structural levels, the impact of mental illness stigma can be wide-ranging, leading to direct mental health distress as well as inequities and disparities in the social determinants of health such as job opportunities and housing, access to and the quality of health-care and social services, and potentially violent traumatic experiences with the law reinforcement and the criminal justice system. Mental illness stigma also results in delayed help seeking, influencing timely diagnosis and treatment for various mental disorders.
For the diverse Canadian society, sociocultural factors need to be considered, as mental illness stigma is often interwoven with diverse cultural beliefs about mental illness as well as the experience of racism and the complex histories of migration. 1 Asian Canadians, including South, South-East, and East Asian Canadians, are the largest and fastest growing visible minority group in Canada. Evidence suggests that compared to other ethnic groups, they have more severe mental illness when presenting for hospitalization, 2 report lower help-seeking behaviour, and have poorer self-rated mental health, 3 highlighting the urgency to develop stigma reduction intervention for this particular population.
There is a variety of evidence-supported approaches toward mental illness stigma reduction. 4,5 One of the most supported approach is contact-based education, which facilitates face-to-face contact between individuals and people with lived experience of mental illness to challenge misconceptions and stereotypes about mental illness. 6 –8 To address the intersections of ethnicity and migration, it is also important to engage with the lived experiences of diversity, including discrimination, acculturative stress, cultural differences in values and meaning making, and issues arising from power relations between service providers and users. 9 For marginalized, disadvantaged, and/or culturally diverse populations, contact-based approaches incorporating an additional lens of social justice and empowerment education have been particularly helpful in addressing both internalized (i.e., absorption and embodiment of negative stereotypical views and beliefs as applied to oneself 10 ) and external forms of social stigma such as stigma against HIV. 7,11
A relatively more recent evidence-based approach for stigma reduction is acceptance and commitment therapy (ACT). 12 –14 Unlike some of the other strategies, it promotes awareness and acceptance of having stigmatizing thoughts and assumptions rather than focusing on correcting or eliminating them. As a mindfulness-based intervention, it promotes psychological flexibility by expanding the individual capacity to become aware of thoughts and feelings in the here and now non-judgmentally, observe and defuse from stigmatizing narratives, be in touch with individual and cultural values related to promoting individual and community mental health, and build a persistent pattern of committed actions toward values, including the promotion of mental health. 15,16 Early examination of the acceptability and feasibility of ACT for Asian American populations have highlighted the cultural congruence between its underlying processes and Asian culture and philosophy. 17
The Strength in Unity (SiU) Project
To explore the effectiveness of these 2 evidence-informed interventions, the SiU Project is a multi-site Canadian study aimed at mobilizing Asian men to reduce stigma of mental illness, 10 –12 with the recognition that culture and gendered expectations may make this group particularly reluctant to seek help. 18 Participants were randomized to receive contact-based empowerment education (CEE), acceptance and commitment training (ACT), both ACT and CEE, or psychoeducation. We previously reported our outcomes with 495 Asian Canadian men in Ontario, including significant reductions in mental illness stigmatizing attitudes and increase in social justice activism from pre to post with all intervention groups. 19 While there were no significant outcome differences distinguishing the interventions, subscale trends observed suggested that CEE may be more broadly effective in reducing mental illness stigmatizing attitudes, while ACT may be more specifically effective in reducing internalized stigma.
Objective and Hypothesis
In this article, we will examine deeper the interventions’ potential main mechanisms of change (see Figure 1). Based on theory, we hypothesize the impact of ACT to be mediated by an increase in psychological flexibility and mindfulness. 12,20 Psychological flexibility, the target of ACT intervention, has been defined as “the ability to fully contact the present moment and the thoughts and feelings it contains without needless defense, and, depending upon what the situation affords, persisting in or changing behavior in the pursuit of goals and value.” 21 The impact of CEE is hypothesized to be mediated by an increased sense of empowerment, strengthening participants’ capacity to identify and challenge social inequities. 22 Empowerment has been defined as the process of “gaining control over one’s life and influencing the organizational and societal structures in which one lives.” 22 By extension, the effects of receiving both ACT and CEE may complementarily tap into both mechanisms of change.
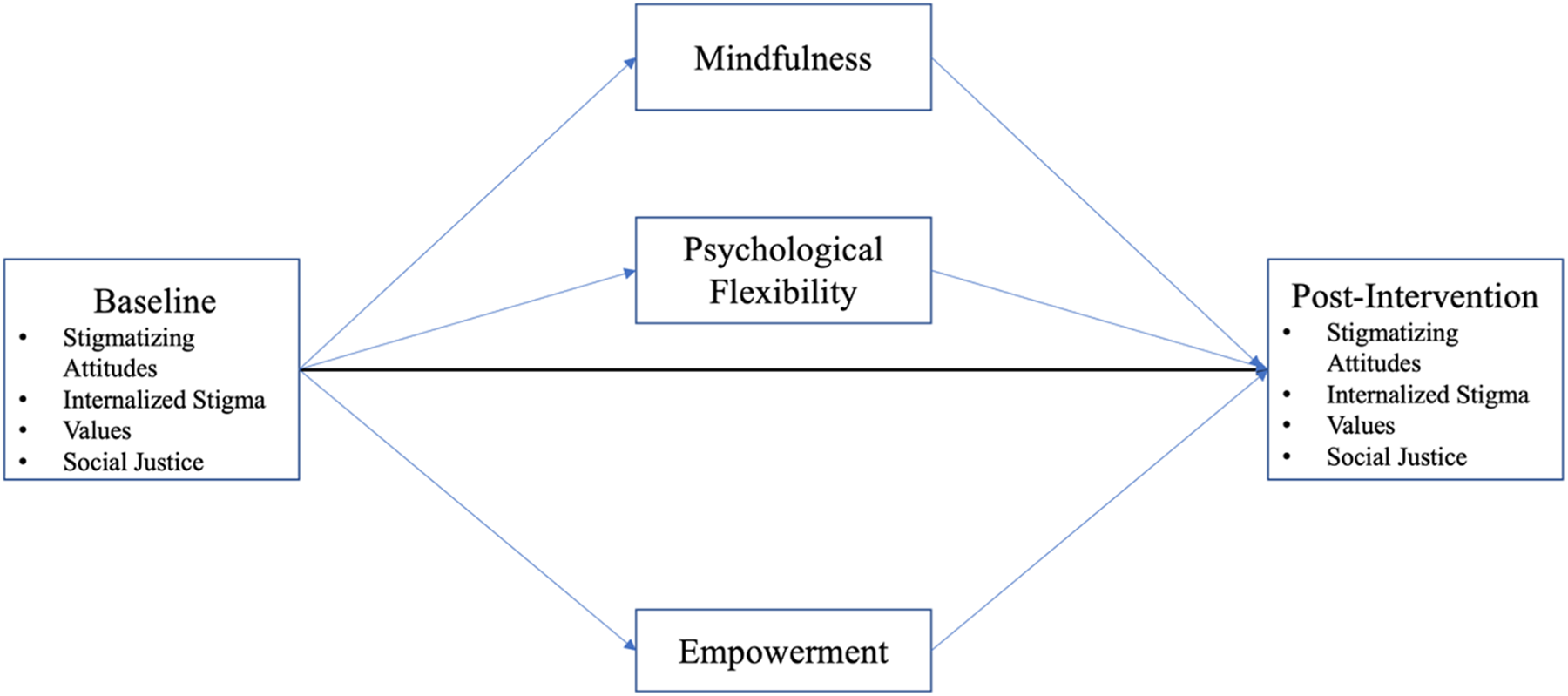
Hypothesized path diagram of intervention-specific mechanisms of change.
Methods
Participants and Procedure
A total of 606 self-identified East Asian, South Asian, or South-East Asian Canadian men living in the Greater Toronto Area, with or without prior experiences with mental illness, were recruited. Participants were randomly assigned to intervention groups or active comparator (psychoeducation) on a 2:1 ratio. 23 A total of 495 (81.68%) completed the intervention and the pre-, immediate post-, and 6-month post-intervention measures (totalling approximately 45 min), including ACT (n = 133), CEE (n = 149), both ACT and CEE (n = 152), and psychoeducation (n = 61). The average age was 46, and the average residency in Canada was 15 years. Detailed protocol of study design, baseline characteristics of sampled population, and pre- and post-intervention changes are described in prior publications. 19,23,24
Brief Description of Interventions
CEE focuses on psychoeducation that includes storytelling by a community leader living with or affected by mental illness, dialogue about structural determinants of mental health, critical dialogue on mental illness, capacity-building on strategies to address stigma, and identification of challenges and opportunities for stigma reduction and activism. 6,7 One aim is that participants become educated and empowered, increasing their self-efficacy in affecting change, improving community support, and increasing optimism. 23,24
ACT focuses on increasing mindfulness skills and psychological flexibility. Through group experiential exercises, it increases 6 underlying psychological processes: defusion, letting go of and decreasing attachment to thoughts and feelings; acceptance, non-avoidance of thoughts or feelings; present moment, contacting with the here and now; self-as-context, being in touch with a transcendent sense of self rather than limiting labels or descriptions; values, being in touch with what and who matters in life; and committed action, engaging in behavioural patterns consistent with values.
Psychoeducation consisted of lecture-based learning thematically organized into discussion of the spectrum of mental health and illness, the social determinants of health, effects of culture and stigma, and identification and explanations of major types of mental illnesses and treatment approaches. 23,24
Process-related Measures
ACT measures
The Acceptance and Action Questionnaire version II (AAQ-II) measures psychological flexibility. 25 It is a 7-point Likert-type scale with higher total scores indicating lower psychological flexibility. An assessment of the internal consistency of this measure via Cronbach α for the sample was excellent, α = .91.
The Freiburg Mindfulness Inventory (FMI) measures mindfulness, including awareness of and paying attention to the present moment non-judgementally. 26 In the short form, participants rate 14 items on a 4-point Liker-type scale. The Cronbach α for the sampled population was good, α = .84.
CEE measures
The Empowerment Scale (ES) is a 28-item scale developed originally for mental health service users. 27 Its subscales include Self-Efficacy, Power/Powerlessness, Community Activism, Optimism and Control Over Future, and Righteous Anger. It is a 4-point Likert-type scale. The Cronbach α for the sample was acceptable, α = .79.
Outcome Measures
Mental health stigma
The Community Attitudes toward the Mentally Ill (CAMI) is a 40-item Likert-type scale used to measure mental illness stigma. 28 It has 4 subscales: (a) Authoritarianism, perceiving people with mental illness as inferior and needing custodial care; (b) Benevolence, compassion and goodwill toward individuals with mental illness; (c) Social Restrictiveness, perceiving people with mental illness as threats to society; and (d) Community Ideology, seeing the therapeutic value of community and accepting deinstitutionalization. For our sample, the Cronbach α were authoritarian α = .60, benevolence α = .67, social restrictiveness α = .61, and community ideology α = .81.
Internalized stigma
The Internalized Stigma of Mental Illness (ISMI) Scale is a 29-item measure on a 4-point Likert-type scale used to measure the personal experience of stigma from having mental illness. 29 It has 5 subscales: Alienation, feeling less than a full member of the community; Stereotype Endorsement, agreeing with negative ideas about people with mental illness; Discrimination Experience, perception of how one is being treated; Social Withdrawal, different ways of disengaging self from others; and Stigma Resistance, ability to resist or be unaffected by stigma. The scale is included as an optional measure for all participants, with instructions directing those who self-identify as having personal lived experiences of mental illness or mental illness stigma to complete it (n = 174). The Cronbach α for the sample was acceptable, α = .79.
Values
The Valued Living Questionnaire (VLQ) assesses the perceived importance of 10 life domains (e.g., family, recreation, work, community, and spirituality) and the consistency of participants’ actions with how much they value these domains. 30 Ratings were on 10-point scales. The change in self-reported committed actions in the service of the participants’ chosen values was used as an outcome indicator. The Cronbach α for the sampled population was good, α = .88.
Social justice
The Social Justice Scale (SJS) is a 44-item Likert-type scale measuring attitudes and beliefs regarding various aspects of social justice and change. Confirmatory factor analysis identified 4 subscales: (a) Attitudes Toward Social Justice, endorsement of social justice values, goals and behaviours; (b) Perceived Behavioural Control, self-efficacy in social justice–related goals; (c) Subjective Norms, support or discouragement in engaging in social change; and (d) Behavioural Intentions, intention to engage in social change. 31 The SJS was adapted to focus on social changes related to decreasing mental illness stigma. The Cronbach α for the sample was excellent, α = .94.
Data Analysis
To examine the mechanisms of change, we first assessed for changes in the proposed mediators pre-/post-intervention. Missing data were filled using multiple imputation method. 32 To determine changes in process-related variables, within-subjects repeated measures analysis of variance (R-ANOVA) was used, with time as within-subject variable and psychological flexibility, mindfulness, and empowerment as dependent variables. Pairwise comparisons and parameter estimates were used to delineate significant findings. Multivariate R-ANOVA was used to assess changes in individual domains of values and empowerment pre- and post-intervention.
The MEMORE macro by Montoya and Hayes was used to estimate the total, direct, and indirect effects of X (time/intervention) on Y (mental health stigma, values, and social justice) outcomes through mediators M (psychological flexibility, mindfulness, and empowerment). 33 Analyses were conducted using a within-subjects repeated measures design, where Y and M are measured at baseline and post-intervention. The 95% confidence intervals of the indirect effects were generated using bias-corrected bootstrapping technique with 10,000 samples and are considered significant if the CIs do not cross 0. The proposed mediator variables were first pooled together to examine their global impact on outcome measures concurrently as a single model. The mediation models were then tested based on their hypothesized relevance and importance in relation to the intervention processes.
Results
Changes in Process and Outcome Measures over Time
Overall
Multivariate ANOVA revealed an overall significant within-subjects effect of time on measures via Pillai trace, F(3, 440) = 15.39, P < 0.001, partial η2 = .10. Follow-up univariate testing also found a significant effect of time in all process-related measures, including psychological flexibility (AAQ-II), F(1, 442) = 5.63, P = 0.018, partial η2 = .01; mindfulness (FMI), F(1, 442) = 37.14, P < 0.001, η2 = .08; and empowerment (ES), F(1, 442) = 18.30, P < 0.001, η2 = .04. After the interventions, psychological inflexibility significantly decreased, while mindfulness and empowerment increased (see Table 1). We conducted paired t tests with subscales of ES and domains of VLQ among intervention groups to examine changes pre- and post-intervention (Tables 1 and 2). Changes of all other outcome variables, CAMI, ISMI, and SJS, were all significant post-intervention, as previously reported. 19
Pre–Post Means of Process Variables among Interventions.
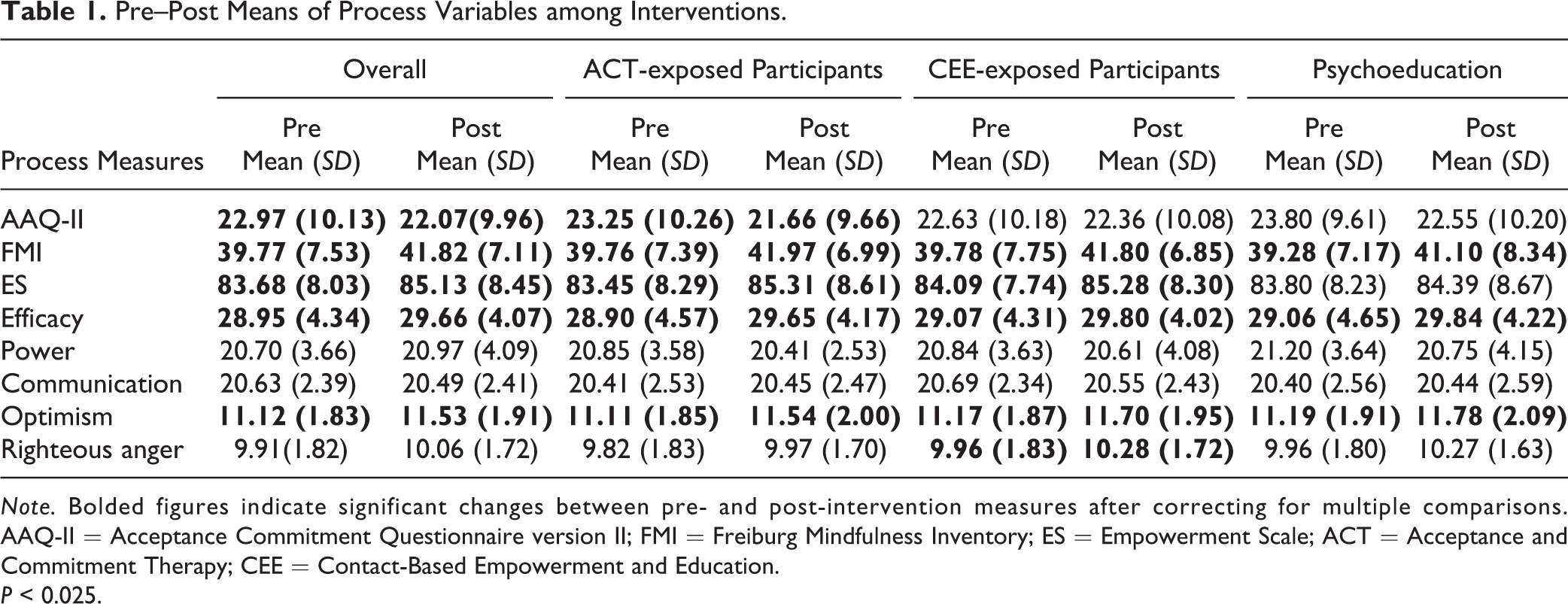
Note. Bolded figures indicate significant changes between pre- and post-intervention measures after correcting for multiple comparisons. AAQ-II = Acceptance Commitment Questionnaire version II; FMI = Freiburg Mindfulness Inventory; ES = Empowerment Scale; ACT = Acceptance and Commitment Therapy; CEE = Contact-Based Empowerment and Education.
P < 0.025.
Pre–Post Changes among Value Domains.
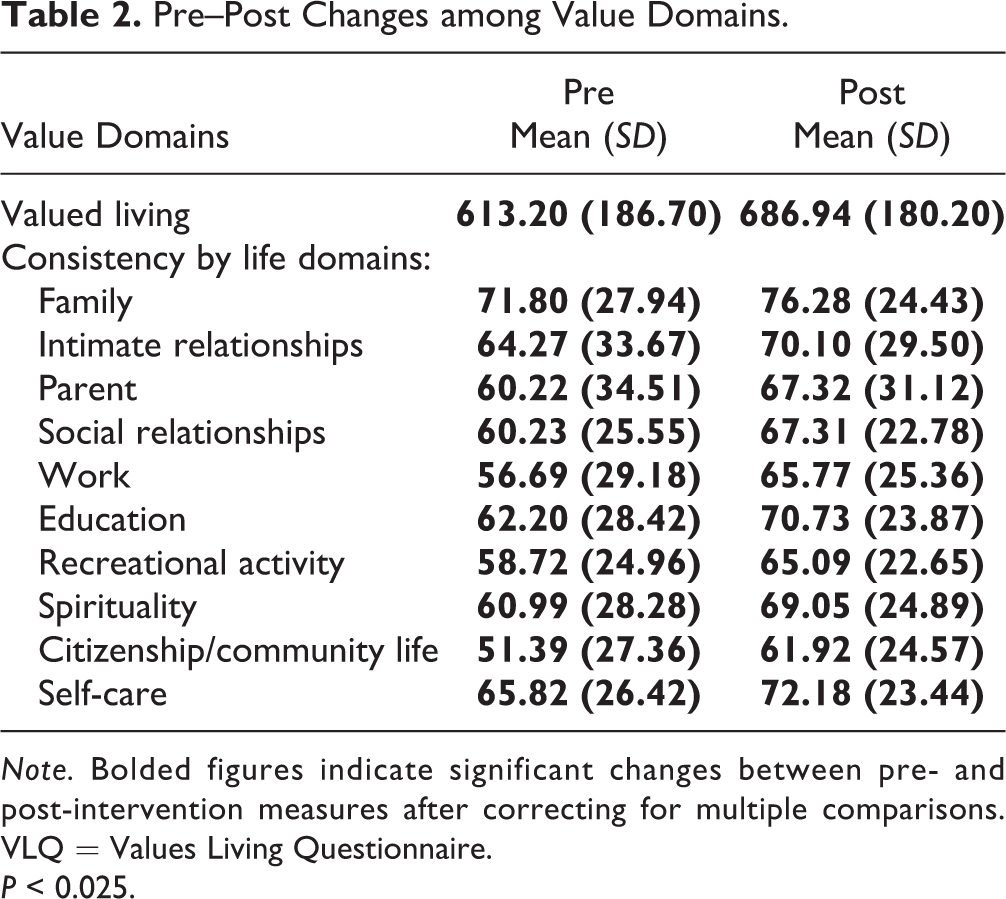
Note. Bolded figures indicate significant changes between pre- and post-intervention measures after correcting for multiple comparisons. VLQ = Values Living Questionnaire.
P < 0.025.
Mediational Analysis of Process Variables
Pre- and post-intervention scores of AAQ, FMI, and ES were used in the overall model to estimate the indirect effects of all process-related variables on outcome variables (Figure 1). There were significant mediational effects detected for all subscales of the CAMI; the discriminating experiences, social withdrawal, and stigma resistance subscales of the ISMI; the VLQ; and the behavioural control subscale of the SJS, P < 0.05 (see Table 3).
Estimates of Mediation Model and Total Effects of Mediators on Outcome Measures.
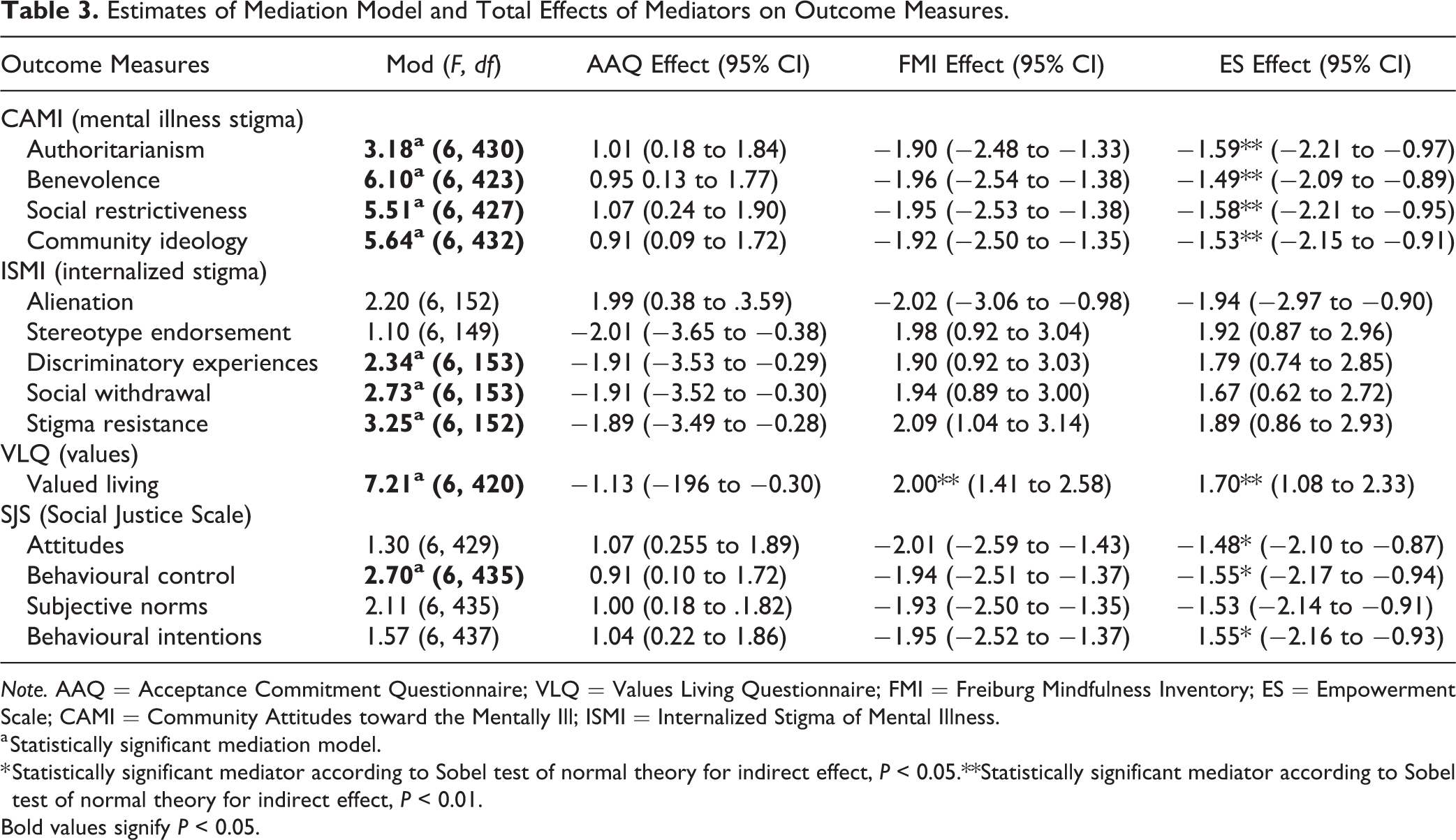
Note. AAQ = Acceptance Commitment Questionnaire; VLQ = Values Living Questionnaire; FMI = Freiburg Mindfulness Inventory; ES = Empowerment Scale; CAMI = Community Attitudes toward the Mentally Ill; ISMI = Internalized Stigma of Mental Illness.
a Statistically significant mediation model.
* Statistically significant mediator according to Sobel test of normal theory for indirect effect, P < 0.05.**Statistically significant mediator according to Sobel test of normal theory for indirect effect, P < 0.01.
Bold values signify P < 0.05.
Among the mediators, empowerment (ES) emerged as a significant mediator for changes in stigmatizing attitudes. For measures of internalized stigma, no single mediator alone emerged as statistically significant, though the overall mediation model with all 3 mediators accounted for significant changes in variance. Shifts in valued living (VLQ) were significantly mediated by increases in mindfulness (FMI) and empowerment (ES). Finally, only ES accounted for significant mediation in the Behavioural Control subscale of the SJS.
Intervention-specific Mediational Analysis
We tested mediational models with each intervention: ACT process-related mediation in all ACT-exposed groups (ACT and ACT + CEE; n = 308) and CEE process-related mediation in all CEE-exposed groups (CEE and ACT + CEE; n = 322). Finally, we tested mediational mechanisms in the psychoeducation group.
Mediation analysis of ACT-trained groups
Mediation analyses estimated a significant mediating effect of empowerment (ES) on all CAMI subscales, including Authoritarianism (t = 4.56; CI, 1.16 to 2.91), Benevolence (t = 4.48; CI, 1.07 to 2.75), Social Restrictiveness (t = 4.49; CI, 1.14 to 2.93), and Community Ideology (t = 4.32; CI, 1.05 to 2.82). With internalized stigma, decreased psychological inflexibility mediated decreased feelings of alienation (t = -3.16; CI, -5.95 to -1.36), while increased empowerment mediated the increase in resistance to mental illness stigma (t = 2.77; CI, 0.62 to 3.79). Increases in VLQ were significantly mediated by increased empowerment (t = 4.78; CI, 1.28 to 3.08). Finally, on subscales of social justice, increased empowerment mediated increased sense of behavioural control (t = 4.43; CI, 1.09 to 2.84).
Mediation analysis of CEE trained groups
Mediation analyses estimated a significant mediating effect of empowerment on all CAMI subscales, including Authoritarianism (t = 3.67; CI, = 0.68 to 2.26), Benevolence (t = 3.70; CI, 0.70 to 2.28), Social Restrictiveness (t = 3.78; CI, 0.74 to 2.34), and Community Ideology (t = 3.68; CI, 0.68 to 2.25). Increased mindfulness also mediated increased benevolence (t = 4.94; CI, 1.17 to 2.72). With internalized stigma, mindfulness mediated social withdrawal (t = 2.99; CI, 0.74 to 3.66) and empowerment mediated stigma resistance (t = 3.03; CI, 0.65 to 3.09). Increased mindfulness (t = 4.79; CI, 1.11 to 2.67) and empowerment (t = 3.85; CI, 0.77 to 2.38) mediated increased valued living (VLQ). No mediational effects were found on social justice subscales.
Psychoeducation group
Mediation analyses detected no indirect effects of process-related variables on outcome measures of CAMI, ISMI, and SJS (P > 0.05). There was a significant mediation effect observed with mindfulness on values (t = 2.56; CI, 10.41 to 3.33).
Discussion
The Toronto SiU study explored the effectiveness of CEE, ACT, and psychoeducation in reducing mental illness stigma and increasing social justice activism. Participants receiving CEE, ACT, and a combination of both reported significant reductions in stigmatizing attitudes. Examining changes in psychological processes hypothesized to be the main mechanisms of change can further elucidate how they may be effective. Extending our previous findings, 19,24 we found significant improvements in psychological flexibility, mindfulness, and empowerment from pre- to post-intervention, suggesting that they may be important underlying processes that deserve further study in anti-stigma research.
In mediational analysis, our results did not consistently distinguish specific psychological mechanisms between active interventions. Across all interventions, empowerment, the perception of having the capacity to influence social structures and affect changes, emerged as a common factor mediating reductions in stigmatizing attitudes and the intention to engage in social change. This suggests that the interventions may have some functional overlap and may not be completely distinct. In our study with Asian Canadian men, mental illness stigma might have been associated with experiences of disconnection, marginalization, disempowerment, and powerlessness. 34,35 Whether it is through ACT exercises or exposure to stories from people with lived experiences through CEE, the opportunity to reflect on shared vulnerability and lived experiences of diversity while building strategies for individual and collective optimism might have increased their sense of empowerment, which, in turn, might have increased their capacity for empathy toward all people living with mental illness. 20 Thus, redressing power imbalances through the process of empowerment may be important in developing anti-stigma interventions, especially for marginalized groups. This highlights the critical issue of attending to embedded inequities at the individual and the structural levels when addressing the interlocking issues of stigma, social and health disparities, and minority stress clinically and systemically. 4,36
As previously reported, only our ACT-exposed groups had significant improvement in internalized stigma. To challenge internalized self-stigma, previous research has identified empowerment to be one of the key processes. 20,35 Consistent with this, mediational analysis found that empowerment was a significant mediator for resistance against stigma. The other significant mediator was psychological flexibility, which mediated decreased feelings of alienation from others. 37 As predicted, only ACT-trained groups had significant increases in psychological flexibility. The ACT skills of defusion and self-as-context to decrease the impact of stigmatizing self-labels, along with the focus on enacting individual and community-oriented values through committed action, might have been effective in countering internalized stigma and the perception of ostracization from the community.
Unique to our culturally appropriate ACT protocol, both individual and community values and actions were explicitly explored. While valued living, the capacity to align actions with values, increased in all life domains, community life had the largest absolute mean increase. The perception that one belongs to a community and is empowered to contribute to it might have been a powerful antidote for internalized stigma. In an Ontario study, Chinese Canadians were found to have the lowest sense of belonging among various groups 2 , and with the staggering rise of anti-Chinese racism in Canada during the COVID-19 pandemic, 38 this underscores the importance of community-building and empowerment as we seek to decrease stigma and promote help-seeking behaviours for marginalized groups. Further, improved valued living across all domains suggests that the beneficial impact of anti-stigma reduction interventions and empowerment may be broader than merely stigma reduction.
Mindfulness, in addition to empowerment, mediated increased valued living. Mindfulness skills may help increase awareness of one’s values, while the non-judgmental acceptance of internal experiences may support persistence in pursuing value-driven actions in the face of barriers. 12 Consistent with previous studies, mindfulness may support marginalized individuals with negative thoughts to develop greater self-compassion and more actively engage with challenges, including interacting with psychoeducational material and engaging with the larger community. 39
Limitations
Recent advances in mediational analyses techniques have offered an opportunity to explore potential mechanisms of change in intervention studies, with the analytic procedure allowing for testing of multiple mediators in a repeated measure design. 33 More studies using this approach are needed in addition to outcome-focused studies. As there may be more congruence of the Asian population with ACT and our intervention protocols have included specific sociocultural considerations such as the discussion of sociocultural values, replication is needed to examine the applicability to other ethnocultural populations. Further, there are important limitations to consider in the interpretation of our results.
Our study found only partial support in intervention-specific mechanisms, such as psychological flexibility in ACT groups mediating the reduction of internalized stigma, while other processes, such as empowerment and mindfulness, appear to be common mediators of change across groups. It may be that the impact of interventions differs less than hypothesized. Recent meta-analytic evidence suggests that intervention-specific factors may account for limited amount of overall outcome variance. 40 From this perspective, more efforts should be spent on examining common factors or processes with interventions.
On the other hand, there may be conceptual and measurement limitations resulting in differences between interventions not being adequately captured. Psychological constructs are abstract with fuzzy boundaries and with potential overlap in conceptualization and measurement. Empowerment and stigma themselves are complex and multifaceted constructs, represented in various subscales, which add to the complexity of their measurement and analysis. The conceptual validity of these constructs as discrete processes and the validity and reliability of their scales need further study. It is difficult if not impossible to develop self-reported psychometric measures that are completely free of conceptual and statistical overlap. Stigma research utilizing repeated frequent measurements based on observable behavioural and biophysiological indicators is needed to supplement scales. 41 Further, a mixed method approach with qualitative data can strengthen a richer understanding of the interventions’ distinct impact, contributing to the iterative development of psychometric process measures and the understanding of complex, dynamic, and interactive systems in the real world. This can also help examine sociocultural factors and differences within and across various understudied minority groups. While Asian Canadian men do share some commonalities culturally and as immigrants, there is also much diversity within these socially constructed groupings, with unique differences in sociocultural, historical, and political experiences and contexts. Finally, participation in any intervention study, regardless of group assignment, may contribute to positive results, such as through a placebo or Hawthorne effect. An examination of the follow-up data is still needed in order to examine the durability of intervention effects and possible differences between intervention groups in the long term.
Conclusion
Our findings suggest that different stigma reduction interventions may converge in decreasing stigma through common psychological processes such as empowerment, and stigma reduction interventions may be more effective when participants can reflect on and address their own sense of vulnerability or disempowerment. This may be especially relevant for marginalized groups, and its significance for other groups merits further study. In addition, internalized stigma may be partly mediated by more specific psychological processes such as psychological flexibility. It is important that research continues to explore both common and specific factors that may help shed light into psychosocial interventions’ effects, which will ultimately inform ways of improving their effectiveness for diverse communities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Movember Foundation.