
Abstract
Objective:
Mental health awareness (MHA) campaigns have been shown to be successful in improving mental health literacy, decreasing stigma, and generating public discussion. However, there is a dearth of evidence regarding the effects of these campaigns on behavioral outcomes such as suicides. Therefore, the objective of this article is to characterize the association between the event and suicide in Canada’s most populous province and the content of suicide-related tweets referencing a Canadian MHA campaign (Bell Let’s Talk Day [BLTD]).
Methods:
Suicide counts during the week of BTLD were compared to a control window (2011 to 2016) to test for associations between the BLTD event and suicide. Suicide tweets geolocated to Ontario, posted in 2016 with the BLTD hashtag were coded for specific putatively harmful and protective content.
Results:
There was no associated change in suicide counts. Tweets (n = 3,763) mainly included content related to general comments about suicide death (68%) and suicide being a problem (42.8%) with little putatively helpful content such as stories of resilience (0.6%) and messages of hope (2.2%).
Conclusions:
In Ontario, this national mental health media campaign was associated with a high volume of suicide-related tweets but not necessarily including content expected to diminish suicide rates. Campaigns like BLTD should strongly consider greater attention to suicide-related messaging that promotes help-seeking and resilience. This may help to further decrease stigmatization, and potentially, reduce suicide rates.
Keywords
Introduction
Mental health awareness (MHA) campaigns have been shown to be successful in improving mental health literacy, decreasing stigma and generating public discussion. 1 –3 They may also result in improved health outcomes. For example, MHA campaigns have been associated with an increase in the use of inpatient and outpatient mental health services. 4,5 However, despite the global proliferation of MHA campaigns, the effects on suicide of awareness campaigns that do not explicitly focus on safe suicide messaging and/or suicide prevention have not been characterized. Indeed, there is even a dearth of evidence regarding campaigns explicitly aimed at educating the public about suicide which have been shown to produce modest improvements in knowledge but not necessarily improved health outcomes. 6
Bell Let’s Talk is a Canadian organization that promotes mental health and well-being, managed by the major telecommunications company Bell Canada. 7 Its 4 aims are to fight stigma, improve access to mental healthcare, support research, and improve mental health in the workplace. 7 Since January 2011, Bell Let’s Talk has launched an annual social media–based MHA campaign, known as Bell Let’s Talk Day (BLTD). 7 On BLTD, Bell Canada donates $0.05 toward mental health initiatives for each text message or phone call made on the Bell Canada network and for engagement with Bell Let’s Talk on social media. Despite being primarily a social media–based campaign, BLTD also involves initiatives including television/radio marketing and university campus activities.
The Twitter content published on BLTD is vast; according to the event organizers, #BellLetsTalk has been the most used hashtag in the world on the day of the event and the top Twitter trend in Canada. 8 It is well known that sensationalized and romanticized reports of suicide can trigger additional suicides across a population, a phenomenon known as the Werther effect. 9 Alternatively, media reports emphasizing coping and resilience in the face of suicidal crises can be associated with fewer suicides across a population, a phenomenon known as the Papageno effect. 10 –12 Based on social learning theory, we would expect that Werther narratives disseminated as part of MHA campaigns like BLTD could cause harm while Papageno narratives might confer benefit.
A single study has evaluated behavioral outcomes of the BLTD campaign; Booth et al. conducted a cross-sectional time series analysis to analyze the association between the 2012 BLTD campaign and the use of outpatient mental health services. 5 They found an associated increase in the use of these services, but that study did not consider the social media content related to BLTD. A formal analysis of the suicide-related content of texts/social media postings related to BLTD has not been conducted, limiting our ability to anticipate whether harm or benefit to suicide rates might arise, and any such impacts on suicide have also not been characterized.
Methods
Study Design and Setting
This study examined social media and suicides in Ontario, Canada. It involved (a) a content analysis of suicide-related social media (Twitter) posts associated with the 2016 BLTD campaign geolocated to Ontario and (b) an analysis to determine whether there was an associated change in suicides during and immediately following BLTD campaign (2011 to 2016).
Suicide Data and Analysis
The primary outcome of interest was the association between the BLTD campaign and suicide. To assess the relationship, counts of suicide in Ontario obtained from the Office of the Chief Coroner were compared between “exposure” and “control” windows in 2011 to 2016 (i.e., years in which the campaign occurred) according to previously established procedures. 12,13,14 Exposure windows were predefined as 7-day epochs spanning day 0 to day +6 with day 0 specified as BLTD in each year. Two control windows of the same length (day −14 to day −8 and −21 to −15) were used as comparators. Control windows in close temporal proximity to exposure windows were chosen in order to prevent impact of seasonal effects and other sociopolitical circumstances. However, days −7 to −1 were excluded to account for the possibility that promotion and marketing surrounding BLTD might have had an impact during the week prior. Note that 94% of suicide-related BLTD tweets were posted on January 27 or 28, and only 15 such tweets were posted prior to day −8. Counts during exposure and control windows 2011 to 2016 were compared using independent samples t-tests. A sensitivity analysis was conducted only including suicides occurring in those aged 10 to 30 years given that people in this age-group account for roughly half of all Twitter users, 15,16 and data from BLTD organizers suggest that the campaign may have had the greatest impact on awareness and attitudes in young people. 8
Twitter Data
All suicide-related tweets geolocated to Ontario, posted from July 1, 2015, to June 30, 2016, were identified by a media-tracking company (Infomart) for a larger study examining Twitter content and suicide. 13 Note that a comprehensive set of tweets were only available to our research team for this 1-year epoch (in contrast to suicide data which was available for 6 years—see below). Tweets were determined to be suicide-related according to an automated search of the word suicide and a series of related terms according to previously published methods (see Online Supplementary File full details). 17 The company identified the top suicide-related Twitter events by tweet volume over the course of the 1 year span. 13 The top event was BLTD with 3,763 tweets including a reference to “#BellLetsTalk” of which 3,447 were posted on the actual day of the event (January 27, 2016). The 3,763 tweets comprised 629 unique tweets and 3,134 retweets. Note that nearly all of these tweets were posted by users of limited influence (<1% were posted by major journalists, news organizations, A list celebrities, athletes, sports teams and hospitals combined).
Two investigators (Author A and Author B) coded the 3,763 tweets for content in 25 domains (see Online Supplementary File full details) under the supervision of senior investigators (Authors C and D). These domains included: Specific Populations; General Comments About Suicide, Physician-Assisted Death and/or Self-Harm; Personal Experiences with Suicide; Tweet Focus Vis-À-Vis Suicide as a Problem and/or Solution (as determined by an overall impression by the coder as to whether the tweet focused on suicide as a problem for people, society and/or the world, solutions to suicide, both or neither); Information About Suicide/Advocacy Against Stigma; Causes of suicide; Monocausal Suicide (simplistic cause and effect); Harmful Messages About Suicide; Suicide as a Way of Solving Problems; Critical of Others Who Have Contemplated or Died from Suicide; Suicide Notes; Personal Resiliency/Suicide Mastery; Someone Saved a Life; Message of Hope; Suicide in the Media; Tweet or Retweet from Mainstream Media; Tweet or Retweet from Celebrity or Mental Health Expert/Organization; Providing External Link or Attachment to Information About Suicide; Support for Suicide Survivors; Suicide Method; Popular References and Quotations; Criticizing Others for Being Insensitive of Others Who Die by Suicide or Showing Intolerance for Harmful Messages About Suicide; Personal Powerlessness/Helplessness; Black Humour; Flippant Remarks About Suicide. An initial interrater reliability test with a sample of 100 tweets showed a high degree of reliability (Krippendorff’s α > 0.9 for most variables), and coders were in regular contact with each other and the rest of the research team to discuss any points of uncertainty. All qualitative data on tweet content are provided descriptively with each type of content expressed as a proportion of all BLTD tweets.
Results
Suicide Counts
There was no significant difference in overall suicide counts in Ontario in the week subsequent to BLTD compared to the control period (exposure 24.7 ± 4.4 vs. control 23.6 ± 5.8; t = 0.401, df = 16, P = 0.69; see Online Supplementary Table 1 for additional details). There was also no difference when the analysis was restricted to only those 10 to 30 years old (exposure 5.2 ± 1.7 vs. control 5.6 ± 2.1; t = −0.417, df = 16, P = 0.68; see Online Supplementary Table 2 for additional details).
Twitter Content
General tweet characteristics are summarized in Table 1. Very few tweets were related to one’s personal experience with suicide/suicidality (either in the person tweeting or someone they know) with the exception of the suicide death of a relative, acquaintance or friend which was noted in 268 (7.1%) tweets. The problem of suicide was highlighted in 1,610 (42.8%) tweets compared to only 321 (8.5%) tweets that described solutions to suicide.
General Characteristics of Suicide-related Tweets from Bell Let’s Talk Day 2016.
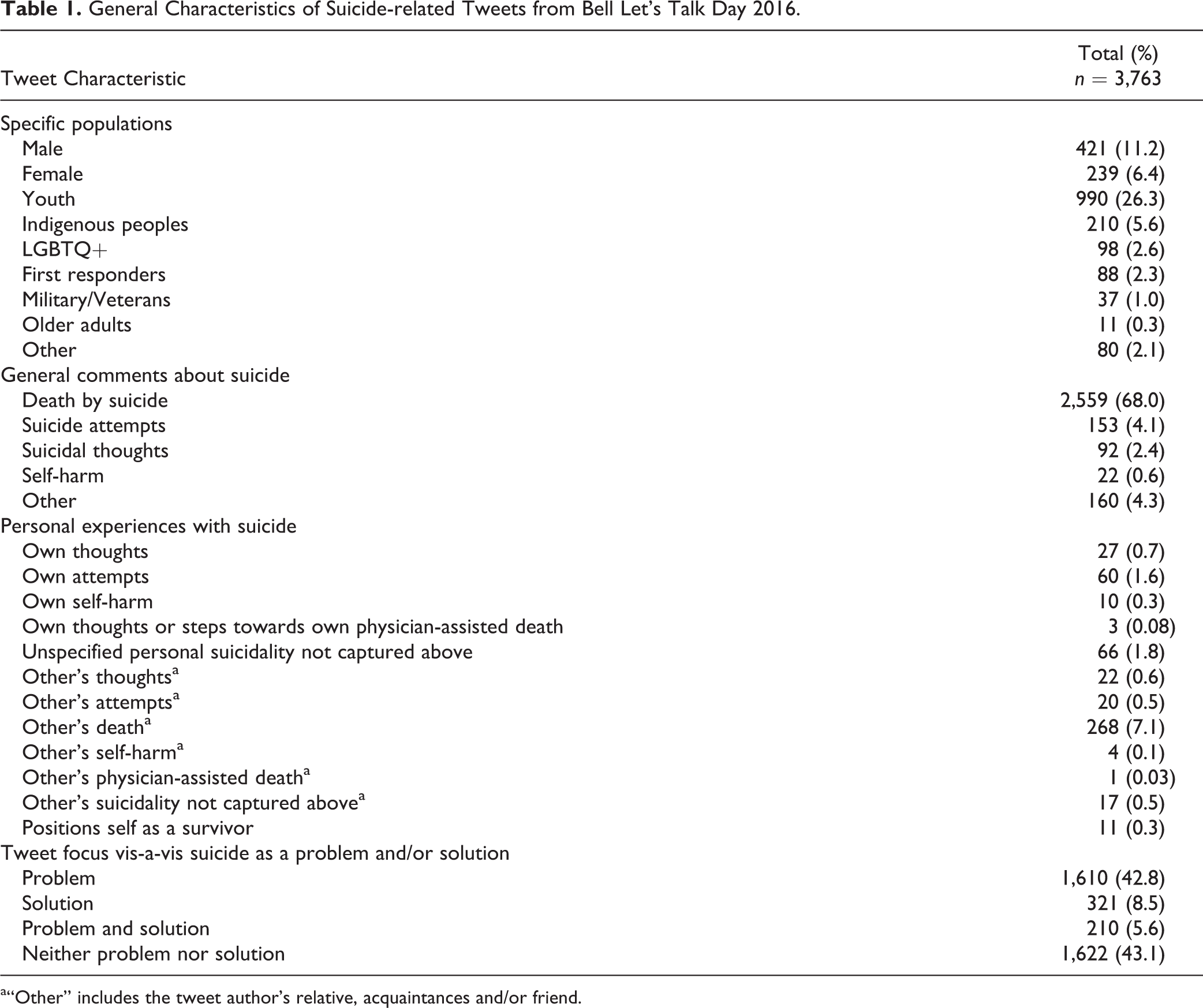
a“Other” includes the tweet author’s relative, acquaintances and/or friend.
More specific tweet characteristics are shown in Table 2. The connection between mental health and suicide was noted in 25.7% of tweets, 9.6% provided information and resources for how to prevent suicide, and 5.7% described how to approach someone who is suicidal. In terms of “causes” of suicide, a mental health problem was listed in 79 (2.1%) tweets, while the most commonly highlighted psychosocial factor was some form of bullying (21 tweets; 0.6%). Only 1.2% of tweets noted that suicide may arise from a single cause.
Detailed Characteristics of Suicide-related Tweets from Bell Let’s Talk Day 2016.
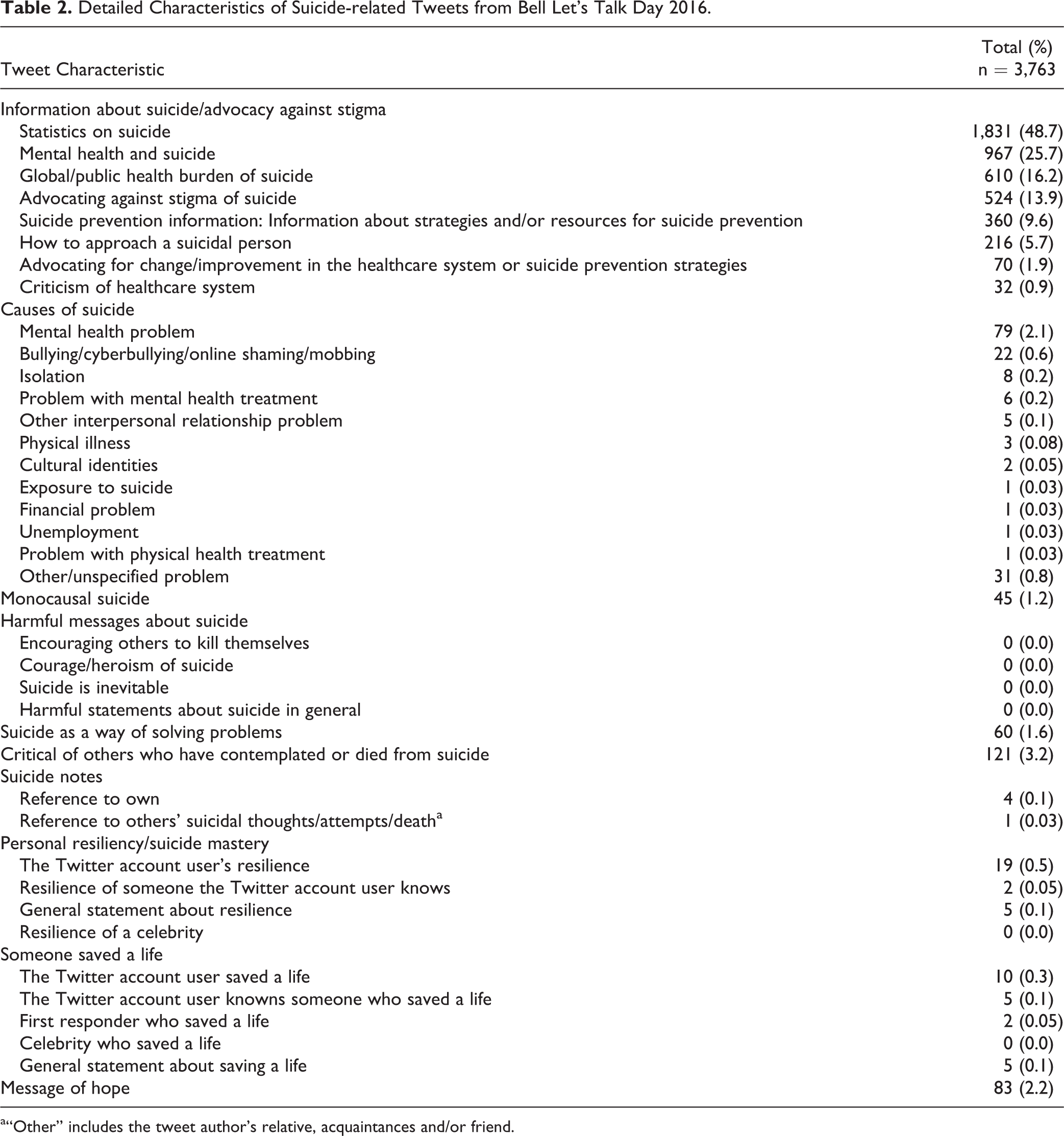
a“Other” includes the tweet author’s relative, acquaintances and/or friend.
There were no tweets with explicitly harmful messages about suicide. However, only 2.2% of tweets included a message of hope and stories of personal resilience/masters as well as those showing people’s lives being saved were present in less than 1% of tweets.
Additional details of tweets are presented in Online Supplementary Table 3. Nearly all tweets about media reports on suicide referred to people who had died by suicide (372; 87.9% of tweets about media reports; 9.9% of all tweets) and were related to people who were not celebrities (379; 93.1% of tweets about media reports; 10.1% of all tweets). Celebrity suicide and “suicide celebrities” (i.e., people who became well known specifically because they died by suicide) accounted for only 10 (2.5% of tweets about media reports; 0.3% of all tweets) and 18 (4.4% of tweets about media reports; 0.5% of all tweets) tweets, respectively. An additional 203 (5.4%) tweets were posted by media organizations or professionals themselves.
Celebrities themselves accounted for 385 (10.2%) tweets of which all but 4 were retweets. Mental health experts and organizations accounted for 534 (14.2%) tweets of which all but 49 were retweets.
Only 182 tweets (4.8%) linked to the website of a suicide prevention organization, the World Health Organization and/or another health organization that disseminates scientific information on suicide prevention. One hundred eleven tweets (2.9%) linked to a picture or video of someone who displayed suicidal behavior or the bereaved, 94 (2.5%) linked to a symbolic picture or video of death, and only 7 (0.2%) linked to a symbolic picture or video of hope. A specific suicide method was mentioned in 0.4% of tweets. Only 0.6% of tweets highlighted resilience and mastery of suicidal crises.
Characteristics of unique tweets and retweets are shown in Online Supplementary Table 4. Tweets about suicide death accounted for 56.0% of unique tweets but were present in 70.4% of retweets. Tweets about suicidal ideation were present in 4.1% of unique tweets but only 2.1% of retweets. Links to symbolic pictures of death accounted for 0.2% of unique tweets and 3.0% of retweets. Links to symbolic pictures of hope were present in 0.5% of unique tweets but only 0.1% of retweets. Messages of hope were present in 4.0% of unique tweets and 1.9% or retweets.
Discussion
To our knowledge, this is the first study to examine the specific suicide-related content that arises on a social media platform (Twitter) as a result of a large national MHA campaign and also the first to examine the association between BLTD and suicide. It found that the content of tweets emphasized death and the problem of suicide. Further, there was no significant difference in suicide counts before and after BLTD. These findings should be of interest both to the organizers of BLTD and similar campaigns worldwide.
As previously described, social learning theory predicts that Werther narratives, if propagated through BLTD, could cause harm while Papageno narratives might confer benefit. 9 –12 Examining suicide counts, we did not find evidence of either a Werther or Papageno effect. It is, however, notable that tweets related to suicide much more commonly emphasized the problem of suicide and death by suicide than putatively protective/Papageno content. Similarly, most of these tweets included general comments about suicide with relatively few tweets about personal experience or celebrity suicide which might be most likely to result in imitative behavior.
What is clear is that the sort of content considered protective by suicide prevention experts and suggested in media recommendations including those in Canada 18 and those developed specifically for social media users 19 was largely absent. The finding that there was no change in suicide counts after BLTD may therefore not be surprising. Previous studies by our group have demonstrated that large, suicide-related Twitter events in Canada often did not include clear Werther or Papageno narratives and, like BLTD, were not associated with changes in suicide rates. 17 However, groups of tweets with specific putatively harmful and protective content were associated with subsequent increases and decreases in suicides respectively. 12 Therefore, the results presented here identify a potential opportunity for BLTD organizers and others promoting large mental health–related events on social media to improve discourse surrounding suicide and its prevention. This may be especially important given that people who experience suicidal ideation, particularly youth, are often social media users and frequently use it as a platform to communicate distress. 20 –23 Thus, social media platforms like Twitter have been proposed as important venues for intervention/disseminating suicide prevention information. 13,24 –26
The results of this study suggest that BLTD and similar campaigns should consider revisiting and augmenting their aims over time. It seems beyond doubt that BLTD has contributed to increased awareness of issues related to mental health in Canada and the willingness of Canadians to discuss these issues openly. However, the suboptimal content of many suicide-related tweets posted in relation to BLTD indicates that future efforts should place greater emphasis on educating social media users, and Canadians in general, on how to improve this discourse. Specifically, people should be encouraged to avoid posting putatively harmful content and instead to share more messages of hope, help-seeking, and survival. Mental health and suicide prevention experts should actively provide campaign organizers with responsible media recommendations and ought to engage with them to inform these efforts.
This study had a number of limitations. First, BLTD is a large uncontrolled experiment, and we are unable to determine whether other factors impacted suicides in Ontario. Similarly, although this study found no association between BLTD and suicide in Ontario, BLTD is a national campaign and may have had different effects in other areas of the country. Second, it only examined tweets from a single year, and we cannot determine whether specific events in 2016 might have influenced the content/whether content might differ substantially in other years. Third, this study only examined tweets. While they are a focus of BLTD, we are unable to determine whether content of other social media platforms differed from that on Twitter. Note however that if such content did differ and if it had an influence on suicide rates, then that still could have emerged in our analysis of suicides, but no changes were detected. Fourth, this study examined individual aspects of tweet content as a proportion of the total and was not designed to identify whether certain kinds of content cluster within groups of tweets. That is, the study was not designed to identify whether specific tweet elements tended to occur together within individual tweets (e.g., suicide death and celebrities; youth and messages of hope) and that could be the subject of further study. Fifth, this study only examined suicide as an outcome. It did not examine other proxy measures relevant to mental health and suicide, for example, rates of help-seeking such as crisis line calls or emergency room presentations. Investigation of these outcomes should be the subject of further study. Sixth, the study only examined a 1-week exposure window. If the BLTD campaign had an acute impact on suicide rates, it would be expected to appear during that time span. Nevertheless, we cannot rule out that longer term effects could emerge that were not tested with this study design. Finally, during the epoch of this study, BLTD was a relatively new campaign. Therefore, we are unable to determine whether more recent discourse was more helpful.
Conclusion
The major finding of this study is that MHA campaigns like BLTD currently do not result in discussions emphasizing how people can cope with suicidal crises or alternatives to suicide, which is recommended yet underrepresented in public discourse. The impact of campaigns like BLTD might therefore be strengthened by greater attention to this issue. Accordingly, the organizers of BLTD and similar events should consider efforts to disseminate putatively protective messages about suicide both proactively and in response to user-generated content. Encouragingly, the most potentially harmful content, such as describing suicide as heroic, inevitable, or encouraging others to end their lives, was not present.
BLTD is now a decade old and, although this has not been formally demonstrated, it seems likely to have achieved at least part of its goal of reducing mental health–related stigma as surveys conducted by the organizers indicate that Canadians, and in particular youth, believe that attitudes are improving and that there is less stigma. 8 This study, however, identifies an untapped opportunity for BLTD and, potentially, similar MHA efforts to further improve discourse about suicide and suicide prevention specifically. BLTD does do a good job of generating discussion of suicide as a societal problem. However, the results here suggest that, without a comprehensive strategy and proactively planned suicide-related media messaging, users may not produce the sort of content that could model ways of coping with suicide crises and suicidal ideation and that might help to reduce suicide rates. Organizers of BLTD and similar MHA campaigns should take note of that and carefully consider suicide-related messaging when devising their campaigns.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720982428 - Suicide-related Twitter Content in Response to a National Mental Health Awareness Campaign and the Association between the Campaign and Suicide Rates in Ontario: Le contenu Lié au Suicide Sur Twitter en Réponse à Une Campagne Nationale de Sensibilisation à la Santé Mentale et à L’association Entre la Campagne et le Taux de Suicide en Ontario
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720982428 for Suicide-related Twitter Content in Response to a National Mental Health Awareness Campaign and the Association between the Campaign and Suicide Rates in Ontario: Le contenu Lié au Suicide Sur Twitter en Réponse à Une Campagne Nationale de Sensibilisation à la Santé Mentale et à L’association Entre la Campagne et le Taux de Suicide en Ontario by David Côté, Marissa Williams, Rabia Zaheer, Thomas Niederkrotenthaler, Ayal Schaffer and Mark Sinyor in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
Dr. Sinyor had full access to all the data in the study and had final responsibility for the decision to submit for publication. Data were obtained from Twitter and the Office of the Chief Coroner. Data from Twitter are publicly available. We do not have permission to share the data from the Office of the Chief Coroner.
Acknowledgments
We thank the staff at the Office of the Chief Coroner of Ontario including Andrew Stephen for providing us with suicide data. We thank the American Foundation for Suicide Prevention for their generous support of this work. We also thank Infomart (now Meltwater) for assisting us in identifying tweets.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors report no financial relationships with commercial interests of relevance to this study. Dr. Sinyor reports that he has received grant support from American Foundation for Suicide Prevention, the Ontario Ministry of Research and Innovation, Mental Health Research Canada, the Innovation Fund of the Alternative Funding Plan from the Academic Health Sciences Centers of Ontario, and the University of Toronto Department of Psychiatry Excellence Fund.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was also supported by the American Foundation for Suicide Prevention (YIG-0-136-15). This work was also supported in part by Academic Scholars Awards from the Departments of Psychiatry at the University of Toronto and Sunnybrook Health Sciences Centre.
Supplemental Material
The supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.