
Abstract
Objective:
To determine the cost-effectiveness of 2 strategies for post-discharge suicide prevention, an Enhanced Contact intervention based on repeated in-person and telephone contacts, and an individual 2-month long problem-solving Psychotherapy program, in comparison to facilitated access to outpatient care following a suicide attempt.
Methods:
We conducted a cost-effectiveness analysis based on a decision tree between January and December 2019. Comparative effectiveness estimates were obtained from an observational study conducted between 2013 and 2017 in Madrid, Spain. Electronic health care records documented resource use (including extra-hospital emergency care, mortality, inpatient admission, and disability leave). Direct cost data were derived from Madrid’s official list of public health care prices. Indirect cost data were derived from Spain’s National Institute of Statistics.
Results:
Both augmentation strategies were more cost-effective than a single priority outpatient appointment considering reasonable thresholds of willingness to pay. Under the base-case scenario, Enhanced Contact and Psychotherapy incurred, respectively, €2,340 and 6,260 per averted attempt, compared to a single priority appointment. Deterministic and probabilistic sensitivity analyses showed both augmentation strategies to remain cost-effective under several scenarios. Enhanced Contact was slightly cost minimizing in comparison to Psychotherapy (base-case scenario: €−196 per averted attempt).
Conclusions:
Two post-discharge suicide prevention strategies based on Enhanced Contact and Psychotherapy were cost-effective in comparison to a single priority appointment. Increasing contacts between suicide attempters and mental health-care providers was slightly cost minimizing compared to psychotherapy.
Introduction
Nonlethal suicidal behavior is a leading reason for emergency medical care, responsible for 1.36% of the total disability-adjusted life years globally. 1 Recent reports suggest that the incidence of suicidal behaviors is increasing, at least in Europe and North America. 2,3 Reversing this trend constitutes a major public health challenge.
Because up to 35% of individuals who attempt suicide will eventually engage in self-harm again, 4 and most reattempts take place shortly after hospital discharge, 2,5 substantial attention has been directed toward the period following an attempt as a window of opportunity for individual-level prevention efforts. Effective post-discharge clinical interventions are also critical to prevent death by suicide, since engaging in any form of self-inflicted harm is the single most important predictor of death by suicide, 6 and the risk of suicide is especially high during the first month following a suicide attempt. 7,8
Most post-discharge suicide prevention strategies bolster contact between attempters and mental health-care providers. 9 –12 The rationale behind contact interventions is 3-fold. First, repeated contacts allow for repeated assessments of imminent suicide risk. Second, they provide emotional support and reduce the sense of social isolation, a major risk factor for suicidality. 13 Third, they increase treatment compliance and reduce disengagement from care, 14 probably enhancing the odds that the patient will seek help in the event of a new suicidal crisis. Individual psychotherapeutic interventions can also prevent suicidal behaviors among recent attempters. 15,16 However, whether psychotherapy provides additional value as compared to simpler, less costly, and more practicable contact interventions remains unanswered.
According to the World Health Organization, conducting accurate economic evaluations of interventions for suicidal behaviors is essential for the development of suicide prevention strategies. 6 Cost-effectiveness studies are particularly important in resource prioritization for service planning. Nevertheless, there is very limited information on the cost-effectiveness of interventions for suicide prevention. 17 Thus far, no study has conducted a head-to-head real-world comparison between a facilitated contact intervention and a psychotherapeutic program.
Our study uses real-world data to estimate the comparative cost-effectiveness of 3 interventions for post-discharge suicide prevention: (1) a single priority outpatient appointment within 1 week after hospital discharge, (2) a single outpatient appointment plus a series of in-person and telephone follow-ups, and (3) a single outpatient appointment plus a 2-month program of weekly individual psychotherapy sessions based on problem-solving therapy.
Methods
Study Setting, Design, and Subjects
Spain provides free, universal medical care through a tax-funded National Health Service. In the Community of Madrid, there are 25 catchment areas, each including a General Hospital and a Psychiatry Department that coordinates in- and outpatient mental health care facilities. Routinely, psychiatric emergency visits take place in each general hospital’s emergency department, and follow-up visits are held in Community Mental Healthcare Centers (CMHC).
In 2012, a specific Suicide Risk Prevention Program (ARSUIC is the Spanish acronym) was universally deployed; it is currently considered Treatment as Usual (TAU) across the Community of Madrid. This program seeks to prioritize access to preventive care for suicide attempters. It consists of priority access to an appointment with a CMHC psychiatrist within 1 week after discharge following a suicide attempt. We obtained data from patients receiving TAU in a catchment area located in the Northern area of Madrid.
In Madrid, 2 catchment areas developed specific augmentation interventions. In the Southern catchment area, in addition to the 7-day priority visit, patients received an individual psychotherapy program, based on a problem-solving therapy approach, and tailored to each patient’s preferences (Psychotherapy). This intervention is structured in 8 weekly sessions held with a clinical psychologist at the hospital before definitive referral to CMHC. In the Western catchment area, the intervention consisted on an enhanced contact maintenance strategy, which included an earlier appointment within 3 days after discharge, 12 months of outpatient visits at an intensified frequency with a specially devoted psychiatrist with specific training in suicide prevention (on average, patients received 3 additional visits compared to TAU), and 15-minute long follow-up telephone calls at months 1, 6, and 12 (Enhanced Contact). The 3 catchment areas under study are roughly similar in terms of area-level socioeconomic and public health indicators (Supplementary Table 1).
We conducted an observational study that included all 1,492 patients aged
Cost-effectiveness Calculations
We conducted a cost-effectiveness analysis based on a decision tree model.
Effectiveness
Our outcome of interest was suicide reattempt within 1 year of follow-up after hospital discharge defined as being treated again at the emergency department for a suicide attempt following the same definition. For patients with >1 suicide attempt over the follow-up period, we included only the first reattempt. Time to reattempt was calculated using each hospital’s electronic records. Comparisons used TAU as the reference group and were adjusted using multivariable Cox regression models and expressed as hazard ratios (HR) with 95% confidence intervals (95% CI). 19 We derived adjusted proportions of reattempt (95% CI) for Enhanced Contact and Psychotherapy by multiplying the proportion of reattempts among the TAU group by the adjusted HR (95% CI) of the Enhanced Contact and the Psychotherapy groups. Then, we calculated effectiveness (as 1—the probability of suicide reattempt) for each intervention. In addition, we obtained estimates of the head-to-head comparison between Enhanced Contact and Psychotherapy, expressed as HR (95% CI).
Resource use and costs
We considered a societal perspective that includes the health care perspective (all direct medical and nonmedical costs) as well as the indirect costs due to work productivity lost because of disability leave or death.
Unit costs were obtained from the official list of public health care prices and fees that the Community of Madrid uses to fund medical providers. 20 In this list, extra-hospital emergency care interventions and emergency department/outpatient visits are valued on a flat rate basis, while in-patient medical costs are calculated based on diagnostic-related groups. These costs were combined with rates of service use due to receiving the intervention or reattempting suicide.
We calculated the rate of service use per intervention based on information retrieved from electronic healthcare records (EHRs) for TAU and on the protocol for Enhanced Contact and Psychotherapy for each individual. The assumption underlying this choice is that the cost for each participant pertaining to the Enhanced Contact and Psychotherapy groups equaled the cost of TAU plus the cost of each intervention’s per-protocol service use, regardless of participants’ adherence. Hence, the cost of TAU was estimated as the cost of a first high-priority outpatient visit plus 4 follow-ups (the average rate of service use incurred by TAU participants); the cost of Enhanced Contact was estimated as the cost of TAU plus the cost of 3 specialized visits and 3 telephone calls; and the cost of Psychotherapy was estimated as the cost of TAU plus the cost of 8 psychotherapy sessions.
All reattempts were considered to incur a minimum cost due to emergency department visit unless the attempt had been fatal. Unfortunately, EHRs from the 3 areas where the different interventions were implemented do not contain the same information regarding key variables. Of note, Madrid’s tax-funded health system provides universal health care coverage to the entire population, and 2 public entities (namely SAMUR-Protección Civil and SUMMA-112) are responsible for all extra-hospital emergency procedures, including ambulance transportation, across catchment areas. 21,22 Because of this, we used EHRs from the Psychotherapy catchment area to calculate the probability of receiving extra-hospital care and ambulance transportation, and EHRs from the Enhanced Contact catchment area to calculate the probability of hospital admission (including admission to an intensive care unit, a medical or surgical ward, or a psychiatric ward). This decision assumes that the proportions of extra-hospital care and ambulance transportation and of hospital admission after emergency department visit, as well as the distribution of costs after hospital admission, were similar across study centers.
These data, that represent the health care perspective, were combined with estimates of the indirect costs due to death and disability leave to obtain the societal perspective. Again, in this case, not all EHRs contained enough information regarding the probability of death and work disability, and we had to assume a similar distribution across centers. The probability of death per reattempt was obtained from the EHRs of the Psychotherapy area. The probability of disability leave per reattempt, as well as the distribution of days of work disability, was obtained from the EHRs of the Enhanced Contact area. To consider the cost of death, we used the present value of lifetime earnings (PVLE) methodology, hence assuming a loss of productive years calculated considering Spain’s current average retirement age, 65 and 23 the mean age of the deceased participants. Despite valid critiques to this methodology, we consider that it yields conservative, conceptually comprehensible estimates. Costs of death based on PVLE and indirect costs due to disability were estimated based on Spain’s average annual monthly wage over the study period (€1,880). 24 As a sensitivity analysis, we repeated our calculations using the recommended value of a statistical year lost as suggested by the European Commission Impact Guidelines 25 as cost of death. We did not have to impute any cost or probability based on the literature. Given the 1-year long follow-up, we did not include any discount rate or inflation in cost calculations.
Cost-effectiveness and sensitivity analyses
We calculated incremental cost-effectiveness ratios (ICERs: incremental cost divided by the incremental effectiveness) comparing Enhanced Contact versus TAU and Psychotherapy versus TAU (see below Formula 1). In these calculations, we weighted each possible cost (death; medical care including extra-hospital care, emergency visit, and admission to an intensive care unit or a medical or psychiatric ward; and disability leave) by the probability of its occurrence. For example, cost of death is weighted by the probability of reattempt and, in turn, by the probability of death per reattempt (Formula 2).
We conducted a deterministic sensitivity analysis to estimate the role that uncertainty may have on our cost-effectiveness estimates. To that end, we considered 3 potential scenarios: base case (Formula 1), most favorable (Formula 3), and least favorable (Formula 4) to the studied interventions, using the 95% CI upper and lower limits (UL and LL, respectively) of the effectiveness estimates, and adding and subtracting 15% to the estimates of the costs. To calculate ICERs in the most and least favorable scenarios, we used the lowest cost estimate and the highest effectiveness estimate (most favorable scenario), and the highest cost estimate and the lowest effectiveness estimate (least favorable scenario). Because Enhanced Contact and Psychotherapy showed identical performance regarding clinical effectiveness, we compared them from a cost-minimization approach. Economic analyses were conducted in Microsoft Excel version 2004 for PC.


Where,
C = cost; E = effectiveness; x∈{A, B}; ix = X intervention; D = death; R = reattempt; A = admission; and DL = disability leave


Finally, we conducted a probabilistic sensitivity analysis by running 10,000 simulations of the base-case scenario, varying all possible parameters at random based on the distribution of our data, following a widely used method. 26,27 We varied reattempt rates based on the β distribution, which is the most suitable for simulating proportion data, 27 and we varied costs based on the triangular distribution, considering half of the estimated cost as the minimum value and double as the maximum value. We used the rβ and rtri R functions to conduct all simulations, and the ggplot2 and dampack packages in R Studio to plot the simulations and construct a cost-effectiveness acceptability curve. Code for replication is available upon request.
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. Data were anonymized before extraction; therefore, according to the Spanish law, informed consent was not required. All procedures were approved by La Paz University Hospital’s Institutional Review Board (approval number PI-2116).
Results
Of the 1,492 participants, 788 received TAU, 523 received Psychotherapy, and 181 received Enhanced Contact. The 3 groups had similar age distributions, with average ages ranging between 40.3 and 42.6 years, as well as similar proportions of participants living alone (around 16%). The Enhanced Contact group had a higher proportion of women (77.4% vs. TAU’s 68.5% and Psychotherapy’s 68.8%) and immigrant individuals (83.4% vs. TAU’s 16.8% and Psychotherapy’s 32.4%). In terms of suicide risk factors, the Enhanced Contact group reported a higher prevalence of previously diagnosed psychiatric disorders (91.7%), personal history of previous suicide attempts (47.0%), and concurrent alcohol or drug abuse disorder (47.0%) than the groups receiving TAU (70.3%, 34.5%, and 35.7%, respectively) and Psychotherapy (48.8%, 27.7%, and 15.3%, respectively; see Martínez-Alés et al. 19 for further detail).
Effectiveness
For subjects who received TAU, the probability of reattempt over a 1-year follow-up was 11.4% (95% CI: 10.2 to 12.6). Using TAU as the reference group, multivariable-adjusted Cox models yielded HR estimates of 0.56 (95% CI: 0.31 to 0.98) for Enhanced Contact and 0.56 (95% CI: 0.37 to 0.87) for Psychotherapy. Accordingly, we calculated adjusted reattempt rates (95% CI), summarized in Table 1. Notably, the head-to-head comparison between Enhanced Contact and Psychotherapy showed practically identical effectiveness estimates (HR = 0.99; 95% CI = 0.51 to 1.96).
Comparative Effectiveness Estimates.
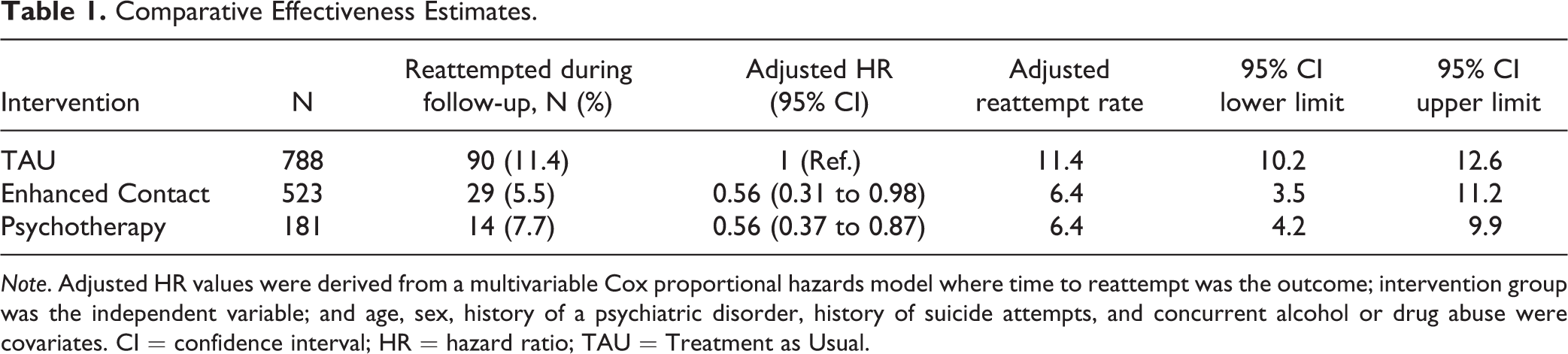
Note. Adjusted HR values were derived from a multivariable Cox proportional hazards model where time to reattempt was the outcome; intervention group was the independent variable; and age, sex, history of a psychiatric disorder, history of suicide attempts, and concurrent alcohol or drug abuse were covariates. CI = confidence interval; HR = hazard ratio; TAU = Treatment as Usual.
Costs
Annual intervention costs incurred by each patient receiving TAU, Enhanced Contact, and Psychotherapy were, respectively, €311, €779, and €975. Table 2 summarizes all direct (medical and nonmedical) and indirect cost estimates. Figure 1 shows the decision-analytic model of distribution of costs.
Probabilities and Costs Used in the Sensitivity Analyses.
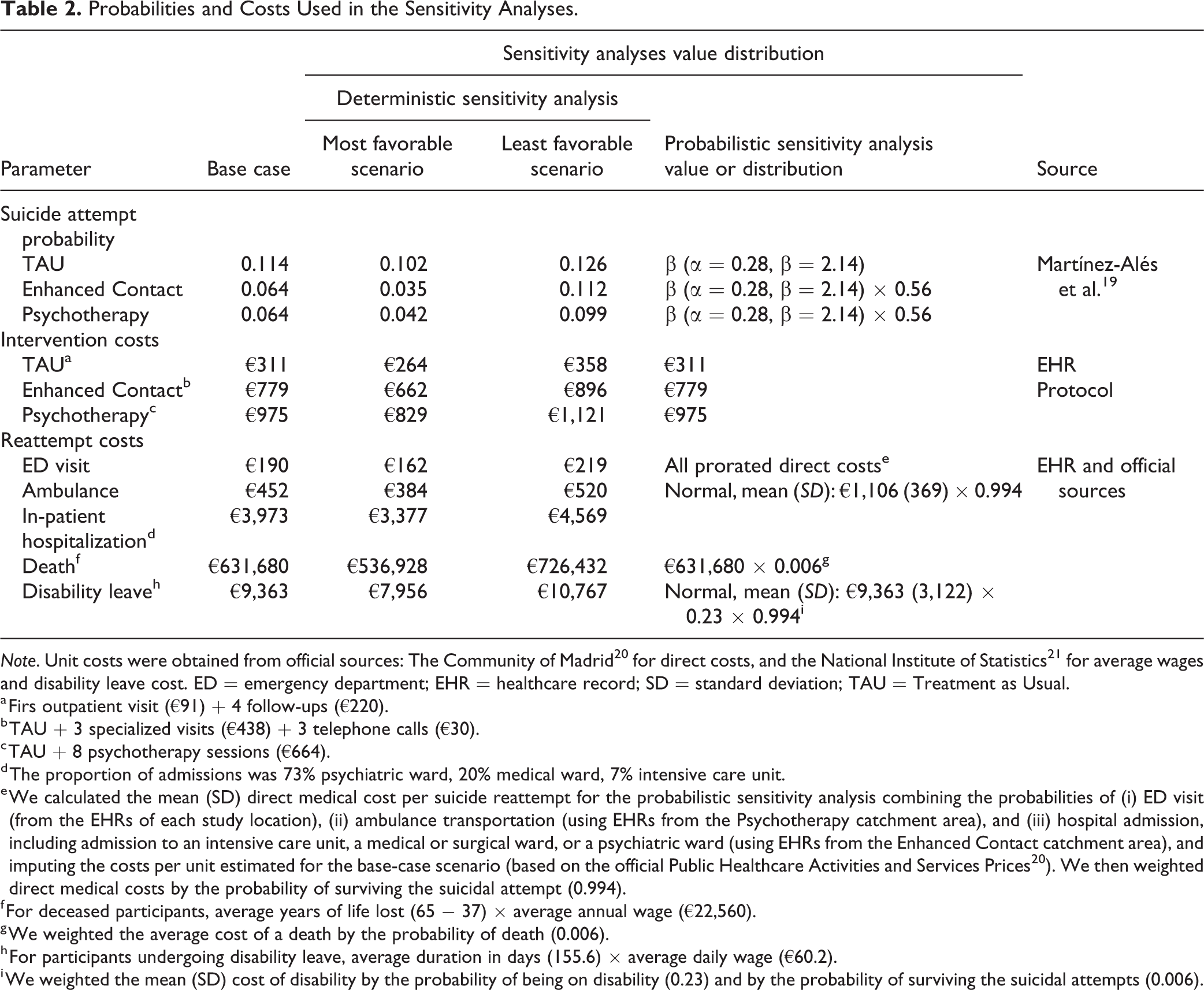
Note. Unit costs were obtained from official sources: The Community of Madrid 20 for direct costs, and the National Institute of Statistics 21 for average wages and disability leave cost. ED = emergency department; EHR = healthcare record; SD = standard deviation; TAU = Treatment as Usual.
a Firs outpatient visit (€91) + 4 follow-ups (€220).
b TAU + 3 specialized visits (€438) + 3 telephone calls (€30).
c TAU + 8 psychotherapy sessions (€664).
d The proportion of admissions was 73% psychiatric ward, 20% medical ward, 7% intensive care unit.
e We calculated the mean (SD) direct medical cost per suicide reattempt for the probabilistic sensitivity analysis combining the probabilities of (i) ED visit (from the EHRs of each study location), (ii) ambulance transportation (using EHRs from the Psychotherapy catchment area), and (iii) hospital admission, including admission to an intensive care unit, a medical or surgical ward, or a psychiatric ward (using EHRs from the Enhanced Contact catchment area), and imputing the costs per unit estimated for the base-case scenario (based on the official Public Healthcare Activities and Services Prices 20 ). We then weighted direct medical costs by the probability of surviving the suicidal attempt (0.994).
f For deceased participants, average years of life lost (65 − 37) × average annual wage (€22,560).
g We weighted the average cost of a death by the probability of death (0.006).
h For participants undergoing disability leave, average duration in days (155.6) × average daily wage (€60.2).
i We weighted the mean (SD) cost of disability by the probability of being on disability (0.23) and by the probability of surviving the suicidal attempts (0.006).
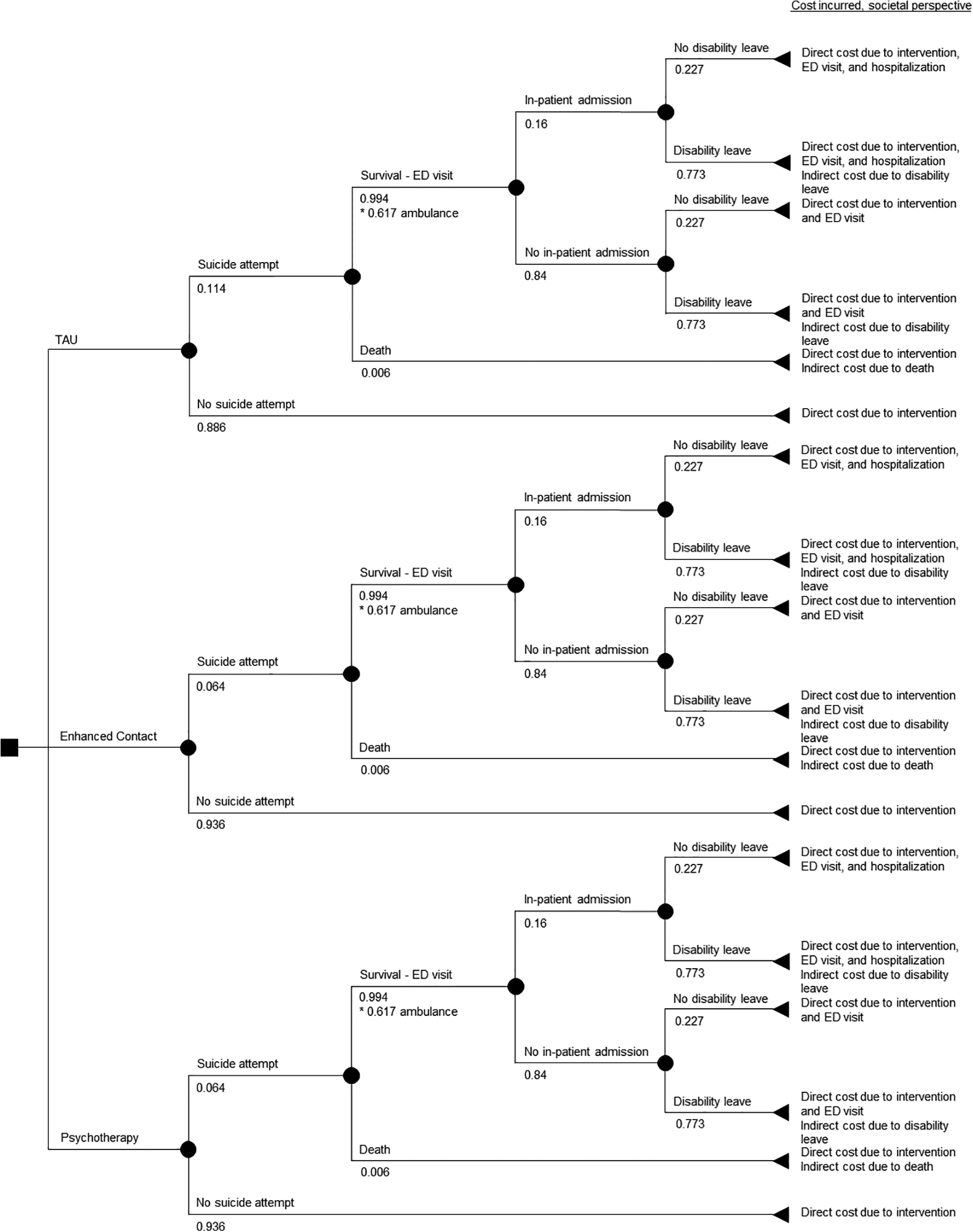
Decision tree structure for each suicide prevention strategy. Intermediate nodes include the probability of each potential outcome. Final nodes include the cost incurred from a societal perspective.
Cost-effectiveness and Sensitivity Analyses
Under the base-case scenario, Enhanced Contact entailed an ICER of €2,340 per averted attempt compared to TAU, a figure that rose to €6,260 for Psychotherapy. As the 2 augmentation strategies were similarly effective, the cost-minimization analysis indicated that Enhanced Contact was slightly cost-saving compared to Psychotherapy (€−196 per participant).
Table 3 shows the ICER estimates of each of the possible comparisons under the 3 proposed scenarios. Importantly, using the European Commission’s estimate of the value of life years lost as cost of death, both interventions under study were dominant (e.g., cost-saving) compared to TAU under all 3 scenarios (Supplementary Table 2). Figure 2 displays the distribution of the simulations obtained as a result of the probabilistic sensitivity analysis. We repeated all simulations using the normal instead of the triangular distribution for costs, following methods used elsewhere, 26 and obtained similar results (data not shown). Supplementary Figure 1 represents the resulting cost-effectiveness acceptability curve.
Incremental Cost-Effectiveness Ratios Estimates Per Reattempt Avoided: Societal Perspective.

Note. ICER = incremental cost-effectiveness ratio; TAU = Treatment as Usual.
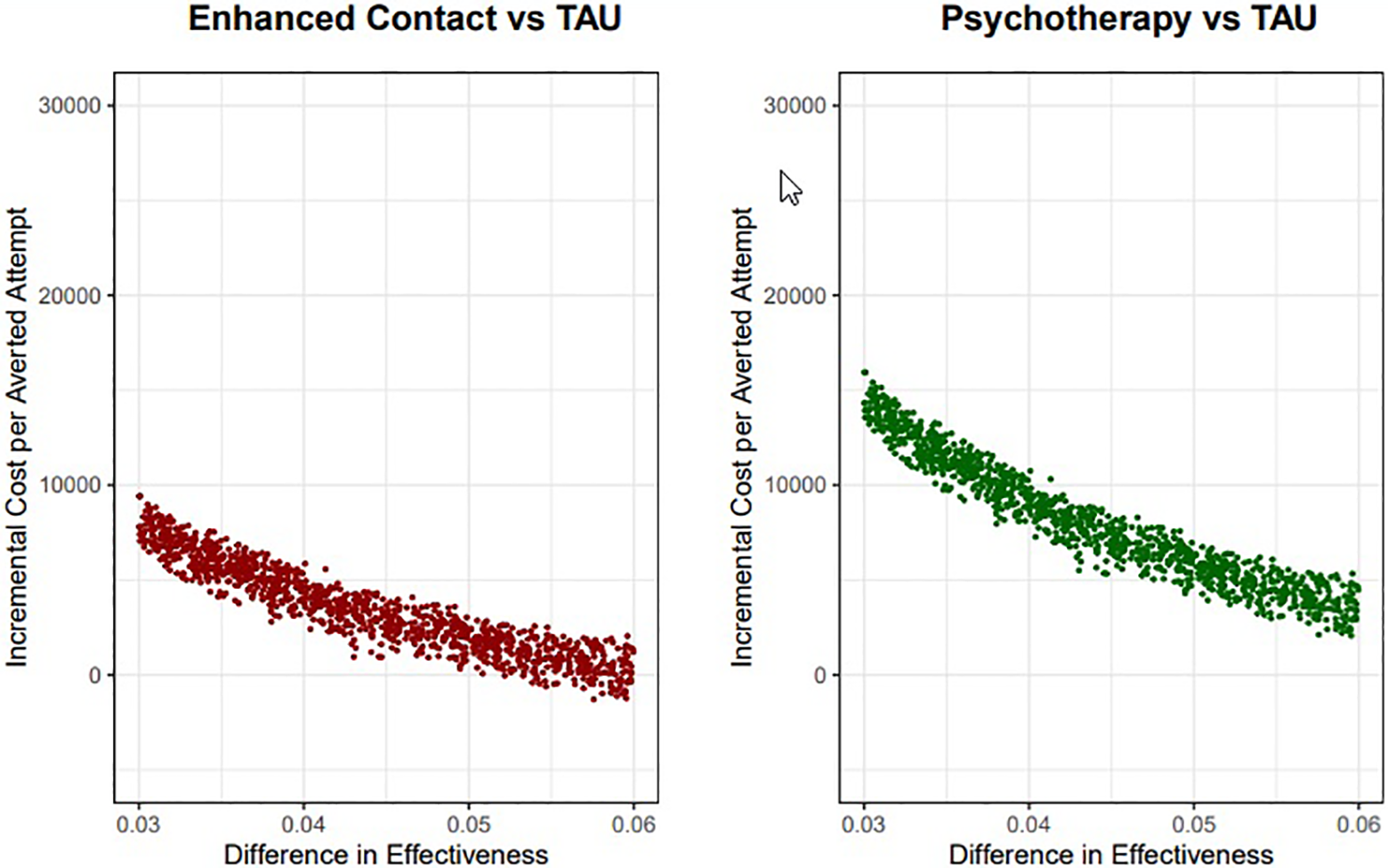
Results from the probabilistic sensitivity analysis, indicating the results of 10,000 simulations based on the parameters indicated in Table 2.
Discussion
To our knowledge, this is the first study to compare the real-world cost-effectiveness of a priority appointment, a contact intervention, and an individual psychotherapy program for postdischarge suicide risk prevention following an attempted suicide. Compared to a single emergency department-appointed priority visit within 1 week after hospital discharge (TAU), the 2 interventions under study (an Enhanced Contact schedule based on an increased frequency of visits and additional telephone calls and a 2-month long weekly problem-solving Psychotherapy intervention) incurred incremental costs per suicide attempt averted that fall below what other researchers have considered acceptable thresholds, 26,27 and resulted dominant (e.g., cost-saving) when using the European Commission’s estimate of the value of life years lost as cost of death. In addition, given that both augmentation strategies had identical effectiveness, a cost-minimization analysis showed that Enhanced Contact was less costly for society than Psychotherapy. These results should provide decision-makers with key information for resource prioritization purposes, as economic assessments of suicide prevention strategies are still scarce in the literature. 17
These results do not lend themselves to easy interpretation, given the lack of consensus regarding the willingness-to-pay per averted suicide. In a recent study based on a randomized controlled trial, Park and colleagues 27 used a willingness-to-pay level of CHF30,000 (approximately €28,000) to evaluate the cost-effectiveness of a contact intervention based on a combination of in-person visits and personalized letters (the Attempted Suicide Short Intervention Program [ASSIP] intervention). Another study evaluated the cost-effectiveness of a brief cognitive behavioral therapy intervention for suicidal US Army soldiers, finding an ICER per averted suicide ranging between US$40,650 and US$44,530 (approximately €36,556 to €40,045) under the worst-case scenario. 26 We found that both Enhanced Contact and Psychotherapy fell below these thresholds of willingness-to-pay per averted suicide, in a variety of scenarios.
Notably, Park et al. found ASSIP to be cost-saving, 27 mainly through a shift toward less costly outpatient treatment in their participants’ pattern of resource use, a result somewhat different than ours (at least under the base-case and less favorable scenarios). Three characteristics of our study design may help explain this discrepancy. First, our control group received the ARSUIC intervention, an emergency department-scheduled outpatient follow-up visit within the first week following hospital discharge. Unlike their control intervention, a single suicide risk assessment, ARSUIC has been found to be effective at lowering the risk of subsequent suicide attempting in previous research. 28 Second, we only recorded each participant’s first reattempt over a 12-month follow-up, while Park et al. included all subsequent suicide attempts, including those carried out by heavy attempters. 27 Third, our models only considered costs that could be attributed to the first reattempt, while they computed all medical costs incurred during the follow-up period. These characteristics probably limited our ability to detect differences between the study groups: compared to Park et al.’s study, we estimated a lower reattempt rate among controls (11.4 per 100 participants) and a more modest mean of costs incurred over the follow-up (€7,020 per reattempt).
Our cost estimates are in line with previous research: A retrospective analysis conducted by Tsiachristas and colleagues 29 based on data collected in 2014 in the United Kingdom estimated an overall mean direct medical cost per suicide attempt of £809 (approximately €1,056 in consumer price index (CPI)-adjusted 2017 currency), and a report commissioned in 2005 by the government of New Zealand 30 calculated a loss of NZ$6,350 per attempted suicide in indirect costs (approximately €5,699 in CPI-adjusted 2017 currency). Taken together with the fact that our data come from an unselected patient sample from clinical practice, this suggests that our results can be viewed as realistic cost-effectiveness estimates that can help guide decision-making in comparable settings with universal health coverage. 31
Our study is subject to several limitations. First, our comparative effectiveness estimates were derived from an observational study, rather than a randomized trial, and some residual confounding due to unmeasured individual- and context-level covariables may have remained uncontrolled. Second, as our study only detected suicide reattempts at the emergency department level, it probably missed a proportion of reattempts not receiving hospital treatment and deaths by suicide occurring outside of the hospital. As a result, we probably underestimated the actual amount of costs per reattempt. We believe that this limitation did not vary by intervention, as we used a similar method for follow-up and detection across all centers. In addition, as noted by other authors, 32 in the Spanish health care system suicide attempters are systematically referred to the Emergency Department of the General Hospital designated for their catchment area. All in all, this limitation probably biased our results toward the null hypothesis, further reducing between-group differences. However, we should mention that we cannot rule out a certain degree of differential loss to follow-up across study locations. Third, we did not include data on the costs of training providers who deliver the interventions under study. Because only the psychotherapeutic program would plausibly entail additional, specific costs associated to training, it seems likely that including such data in our calculations would have yielded results differentially more positive for Enhanced Contact. Fourth, not all EHRs contained the full information regarding the probability of extra-hospital care, hospital admission, death, and disability leave. As a result, we had to adopt the untestable assumption that all potential outcomes distribute similarly across all study centers. Last, our effectiveness estimates only consider the first suicide reattempt: Future analyses should take into account repeated attempts conducted by heavy attempters, as they probably drive a great proportion of costs to health systems.
A natural next step would be to estimate the cost-effectiveness of psychotherapeutic interventions for specific subgroups of suicide attempters, as important phenotypic variation across these patients suggests at least 2 different patterns: stress-responsive and nonstress-responsive attempters. 33 It seems plausible that the latter subgroup, whose attempts are often planned over longer time spans and usually in the context of a major depressive disorder, may benefit more from a psychotherapeutic approach than the former, more impulsive subgroup. Also, further research is needed in order to explore the transportability of our results to different settings, and additional sources of indirect costs (such as other family members’ loss of productivity) should be computed to better understand the societal costs of suicide attempts and deaths by suicide.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720980135 - Cost-effectiveness of a Contact Intervention and a Psychotherapeutic Program for Post-discharge Suicide Prevention: Rentabilité D’une Intervention de Contact et d’un Programme de Psychothérapie Pour la Prévention du Suicide Après le Congé de L’hôpital
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720980135 for Cost-effectiveness of a Contact Intervention and a Psychotherapeutic Program for Post-discharge Suicide Prevention: Rentabilité D’une Intervention de Contact et d’un Programme de Psychothérapie Pour la Prévention du Suicide Après le Congé de L’hôpital by Gonzalo Martínez-Alés, José B. Cruz Rodríguez, Pablo Lázaro, Arce Domingo-Relloso, María Luisa Barrigón, Ricardo Angora, Beatriz Rodríguez-Vega, Eduardo Jiménez-Sola, Pilar Sánchez-Castro, Eva Román-Mazuecos, Lucía Villoria, Ana José Ortega, Mercedes Navío, Barbara Stanley, Robert Rosenheck, Enrique Baca-García and María Fe Bravo-Ortiz in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
GMA, EBG, and MBO had and continue to have access to the study data. Data can be shared under reasonable request.
Acknowledgments
The authors want to acknowledge Dr Samantha L. Bernecker for providing general assistance in some statistical procedures.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially funded by a personal training grant awarded by the “la Caixa” Foundation (G.M.A., grant number LCF/BQ/AA17/11610021).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.