
Abstract
Objective:
This study examines whether depression is associated with the development of physical illness and multimorbidity, after controlling for socioeconomic, behavioral, and other potential confounders.
Methods:
This is a retrospective cohort study in which adult respondents to three nationally representative population health surveys were linked to health administrative databases in Ontario, Canada, and followed for 10 years from survey index. Respondents with any of the study outcome conditions at baseline were excluded to create a final cohort of 29,838 participants. The main exposure of interest was depression, measured using the Composite International Diagnostic Interview–Short Form for Major Depression. We controlled for age, body mass index, marital status, immigrant status, annual household income, smoking, alcohol consumption, physical activity, health status, and having a regular doctor. The outcome measure was the development of physical illness over 10 years of follow-up, defined as 1 of 15 common chronic conditions using administrative data.
Results:
Among the 29,838 participants (15,259 [51%] female), 8% of females and 4% of males had depression at baseline. In this cohort with no comorbidities at baseline, even in the fully adjusted model, depression increased the risk of developing a first physical illness for females (hazard ratio [HR] 1.16; 95% CI, 1.07 to 1.26) and males (HR 1.20; 95% CI, 1.07 to 1.36) and increased the risk of developing a second physical illness for females (HR 1.16; 95% CI, 1.02 to 1.33) over 10 years of follow-up.
Conclusions:
For individuals with no prior comorbidities, depression is associated with a greater risk of developing subsequent physical illness and multimorbidity over time. Thus, depression identifies a population of people who may benefit from early identification, additional screening, and intervention. Further study needs to be done to determine whether interventions to manage and support people with depression can prevent or delay the increased risk of multimorbidity.
Introduction
Multimorbidity, defined as the coexistence of multiple chronic conditions in an individual, is a significant challenge facing patients, clinicians, and the health-care system. Multimorbidity is associated with complex health needs, increased health-care utilization, high costs, poor quality of life, poor health outcomes, and premature mortality. 1 –6
Multimorbidity with combined physical and mental illness is associated with poorer health and higher costs relative to physical multimorbidity alone. In a large, international study by the World Health Organization, having a physical illness comorbid with depression had the worst health scores of all combinations of chronic diseases. 7 In other studies, multimorbid patients with mental health conditions had higher health care utilization and costs than other multimorbid and high-cost patients. 5,6,8,9 Understanding and addressing multimorbidity is thus an increasingly important research, clinical, and policy priority.
Previous studies have found an association between depression and specific physical illnesses 7,10 –12 as well as depression and number of chronic conditions. 13 –17 While much of the literature on depression and multimorbidity is cross-sectional, there are a few studies that have examined the relationship between depression and the development of physical illness. However, some of these use a broad administrative definition of mental health that may not capture depression specifically. 18,19 Others have not adjusted for potential behavioral confounders such as smoking or physical activity. 7,14,16,20,21 Moreover, several studies from the United Kingdom have highlighted the importance of including indicators of socioeconomic status, showing that the complex relationship between depression and multimorbidity appears to be influenced by socioeconomic factors. 16,20 –22
This study examines whether depression is associated with the development of physical illness and multimorbidity in a large, population-based sample with no comorbidities at baseline over a 10-year follow-up period. It uses validated measures for identifying cases of depression and physical illnesses, and controls for socioeconomic, behavioral, and other potential confounders. While the relationship between depression and physical illness is complex and multidirectional, this study focuses on the particular temporal pathway where depression occurs first and there is subsequent diagnosis of physical illness.
Design and Methods
Study Population
The study population consisted of pooled respondents to the National Population Health Survey (1996 to 1997) and Canadian Community Health Survey cycles 1.1 (2000 to 2001) and 2.1 (2003). These surveys, administered by Statistics Canada using similar methodology, are representative of more than 97% of the Canadian population aged 12 and above. 23 Detailed survey methodology is available elsewhere. 23 This study included adults aged 18 and above living in the province of Ontario, Canada’s most populous province, who consented to having their survey responses linked to health administrative databases. The databases at the Institute for Clinical Evaluative Sciences (ICES) contain longitudinal, person-level data on health care services covered by Ontario’s publicly funded universal health insurance plan. All participants were followed in the administrative data for 10 years from their survey index date.
Figure 1 shows how the final cohort was constructed. We included adult Ontario residents who were eligible for the provincial health insurance plan at the survey index date and had contact with the health care system at some point in the previous 5 years to ensure they were likely still residing in the province. If respondents participated in more than one of the surveys, only their responses to the first survey were included. Participants were excluded if they were missing a value for depression at baseline in the survey since this was a key explanatory variable. The depression module was optional in the surveys and was not selected by every health region in Ontario for all surveys. Participants were also excluded if they were missing values for other explanatory variables at baseline, with the exception of household income and body mass index (BMI), for which categories for respondents with missing data were created. See eTable 1 in the Supplement for a summary of the participants included in the study cohort and excluded due to missing observations. To create a healthy cohort, free of physical illness, the administrative data were used to exclude respondents with any of the 15 outcome study conditions at baseline (prevalent cases dating back to 1991). In this study, a cohort free of comorbidities at baseline was selected to better isolate the effect of depression and reduce the risk of confounding from other clinical diagnoses—for example, preexisting hypertension and diabetes would be known risk factors for coronary artery disease.
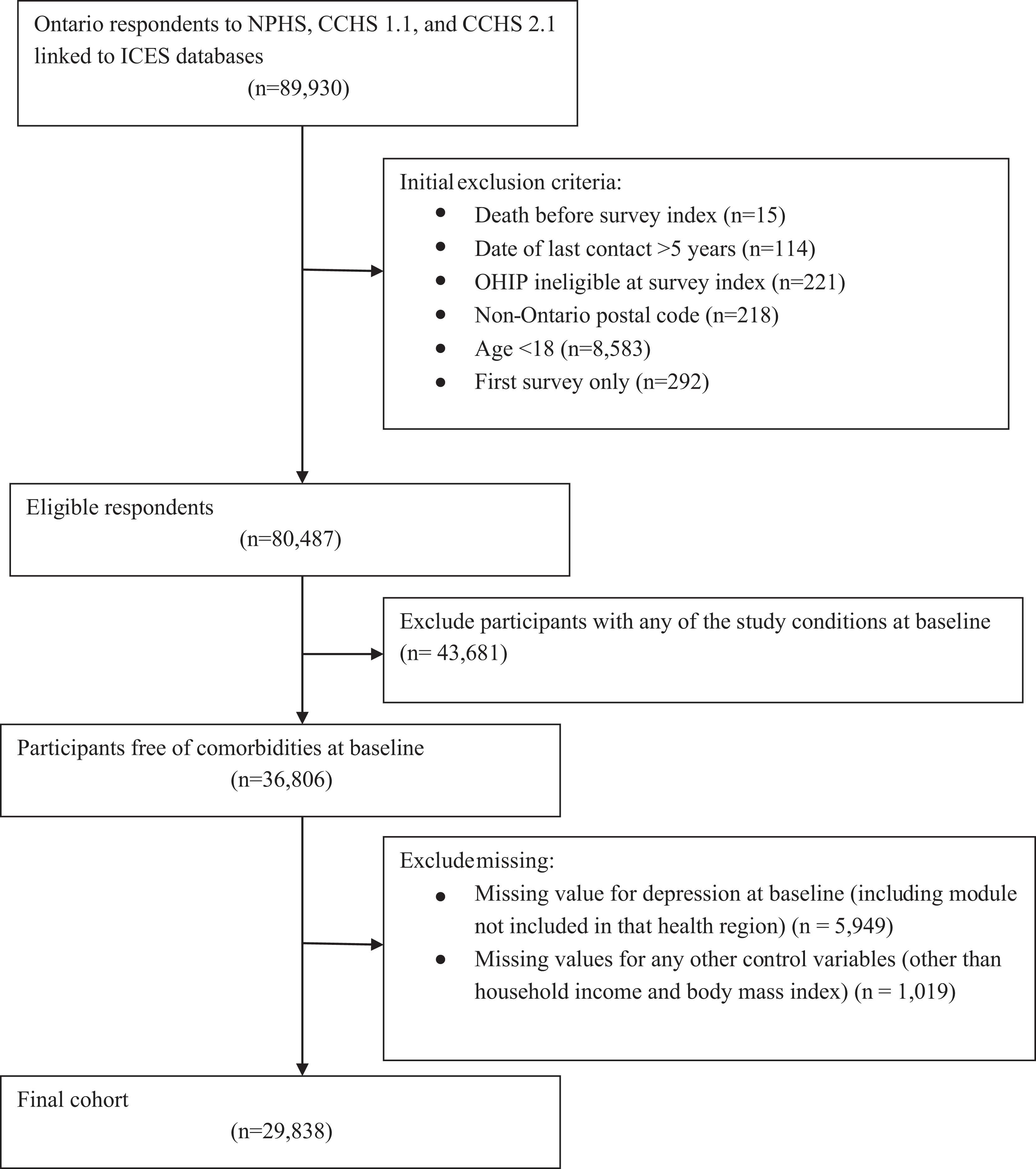
Constructing the cohort.
Definitions and Measures
Depression was identified at baseline from the survey data using the Composite International Diagnostic Interview–Short Form for Major Depression (CIDI-SFMD). The CIDI-SFMD is a brief, structured interview to identify a major depressive episode in the previous 12 months. 24 The CIDI-SFMD identifies cases of a major depressive episode in a probabilistic fashion based on the number of symptoms reported in a 2-week period in the past year. For this study, the CIDI-SFMD was scored at the 90% predicted probability using the values provided by the surveys. 25 The CIDI-SFMD has been used in other Canadian studies. 12,19,26
Other baseline explanatory variables were selected based on a review of the multimorbidity literature and were derived from the survey data. These included biological factors (age, BMI), socioeconomic factors (marital status, immigrant status, annual household income), behavioral factors (smoking status, alcohol consumption, physical activity), and health care factors (having a regular medical doctor). In this study, an individual was classified as a current smoker if they reported being a daily or occasional smoker. Heavy alcohol consumption was defined as >15 drinks for men and >10 drinks for women in the last week, consistent with the Canadian low risk drinking guidelines and other studies. 27,28 The physical activity variable was based on energy expenditure calculated from frequency and duration of leisure time physical activities using the predefined categories from Statistics Canada and was divided into active (including active and moderately active, ≥1.5 kcal/kg/day) and inactive (<1.5 kcal/kg/day). 19,25
Although the study cohort was free of any of the 15 study conditions at baseline, underlying health status was also included as a control variable, using Aggregated Diagnosis Groups (ADGs). In this study, ADGs were calculated using a 2-year look-back period from interview date. This study used quintiles of the ADG score, a weighted score based on ADGs that has previously been validated in Ontario. 3,29
The main outcome measure in this study was the development of physical illness, derived from ICES administrative databases reflecting diagnoses in both the inpatient and outpatient settings. See eMethods and eTable 2 in the Supplement for a summary of the algorithms and diagnostic codes used. Fifteen chronic conditions were selected for their high population burden and cost: acute myocardial infarction, asthma, cancer, cardiac arrhythmia, chronic coronary syndrome, chronic obstructive pulmonary disease, congestive heart failure, dementia, diabetes, hypertension, osteoarthritis, osteoporosis, renal failure, rheumatoid arthritis, and stroke. 30 This set of conditions has previously been used in many Canadian studies. 4,30 –33 Furthermore, these conditions were included in the recommended list of core morbidities from a 2011 systematic review of multimorbidity studies. 34
Data Analysis
The baseline characteristics for the cohort were summarized for all covariates. All analyses were stratified by sex, as there is evidence in the literature of sex differences in depression prevalence, medical illness risk factors, onset, rates, and patterns of multimorbidity, as well as health care utilization. 1,19,21,28,35 –39
Using Cox proportional hazards regression models, age-adjusted and fully adjusted analyses looked at a composite outcome of time to the development of any of the 15 study conditions over the 10-year follow-up period. We looked at the time to development of a first condition in this cohort initially free of comorbidities and time to development of a second condition among those who developed a first condition. Sensitivity analysis in which behavioral risk factors (smoking, alcohol use, and physical activity) were omitted from the model was also performed. Individuals were right-censored when any of the following endpoints were reached: end of the study period, date of death, or became ineligible for provincial health insurance. Tests of proportionality were performed, and the assumption was found to be valid. For all analyses, a P value <0.05 was considered statistically significant. All analyses were performed using Stata Version 13.1.
This study received approval from the research ethics board at the University of Toronto.
Results
The final sample included 29,838 participants (15,259 [51%] female). Sample characteristics are summarized in Table 1. In this study, 8% of women and 4% of men had depression at baseline. The cohort was young, with almost 80% of men and women being under the age of 50. More than half of the cohort was married or common-law. Around 80% of the cohort was born in Canada. About 44% of women and 37% of men reported an annual household income under CA$50,000, with around 10% of the sample having missing values for income. Roughly one-third of men and one-quarter of women reported being current smokers, while close to 10% of men and 4% of women were heavy drinkers. Approximately half the sample reported being physically inactive, and 30% of women and 51% of men were overweight or obese. Around 92% of women and 85% of men had a regular medical doctor.
Sample Characteristics.
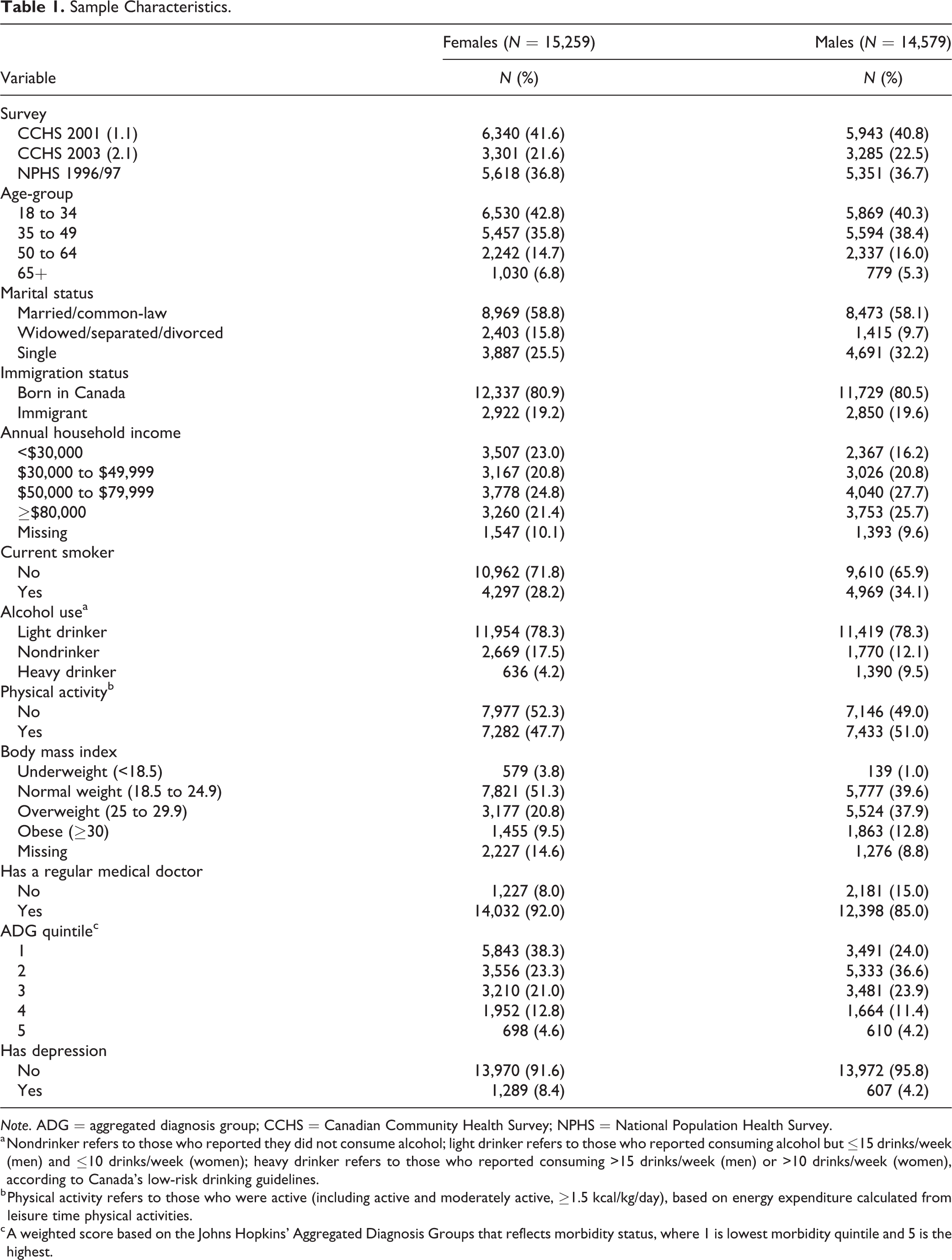
Note. ADG = aggregated diagnosis group; CCHS = Canadian Community Health Survey; NPHS = National Population Health Survey.
a Nondrinker refers to those who reported they did not consume alcohol; light drinker refers to those who reported consuming alcohol but ≤15 drinks/week (men) and ≤10 drinks/week (women); heavy drinker refers to those who reported consuming >15 drinks/week (men) or >10 drinks/week (women), according to Canada’s low-risk drinking guidelines.
b Physical activity refers to those who were active (including active and moderately active, ≥1.5 kcal/kg/day), based on energy expenditure calculated from leisure time physical activities.
c A weighted score based on the Johns Hopkins’ Aggregated Diagnosis Groups that reflects morbidity status, where 1 is lowest morbidity quintile and 5 is the highest.
In this cohort that was initially free of any comorbidities, 52% of women with depression at baseline and 51% of those without, and 46% of men with depression and 44% without developed at least one physical illness over 10 years. The most common first physical illnesses for both men and women were osteoarthritis, hypertension, and cancer (eTable3 in Supplement). Table 2 shows the risk of developing a first physical illness in this cohort. Even after adjusting for demographic, socioeconomic, and behavioral factors, being depressed at baseline was associated with a higher risk of developing a first physical illness over 10 years for women (hazard ratio [HR] 1.16; 95% CI, 1.07 to 1.26) and men (HR 1.20; 95% CI, 1.07 to 1.36). When the behavioral risk factors (smoking, alcohol use, and physical activity) were omitted from the model, the estimates were virtually identical.
Hazard of Developing a First Physical Illness in Cohort Free of Comorbidities at Baseline.
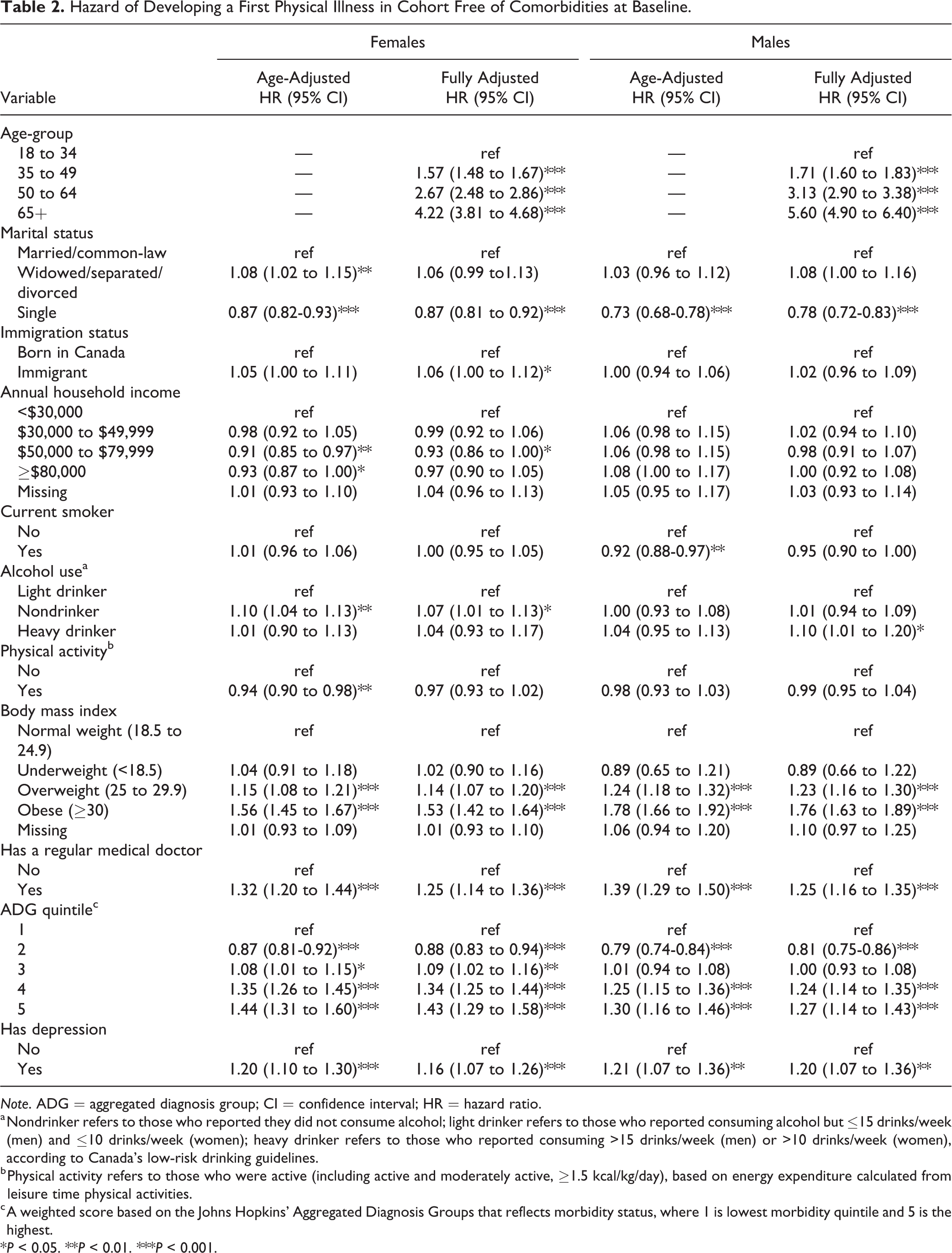
Note. ADG = aggregated diagnosis group; CI = confidence interval; HR = hazard ratio.
a Nondrinker refers to those who reported they did not consume alcohol; light drinker refers to those who reported consuming alcohol but ≤15 drinks/week (men) and ≤10 drinks/week (women); heavy drinker refers to those who reported consuming >15 drinks/week (men) or >10 drinks/week (women), according to Canada’s low-risk drinking guidelines.
b Physical activity refers to those who were active (including active and moderately active, ≥1.5 kcal/kg/day), based on energy expenditure calculated from leisure time physical activities.
c A weighted score based on the Johns Hopkins’ Aggregated Diagnosis Groups that reflects morbidity status, where 1 is lowest morbidity quintile and 5 is the highest.
*P < 0.05. **P < 0.01. ***P < 0.001.
Table 3 shows the risk of developing a second physical illness, among those who developed a first illness during the 10 years of follow-up. For women, having depression at baseline was associated with an increased risk of developing a second condition when adjusting for age only and in the fully adjusted model (HR 1.16; 95% CI, 1.02 to 1.33). A significant relationship was not seen for men.
Hazard of Developing a Second Physical Illness among Those Who Developed a First Physical Illness.
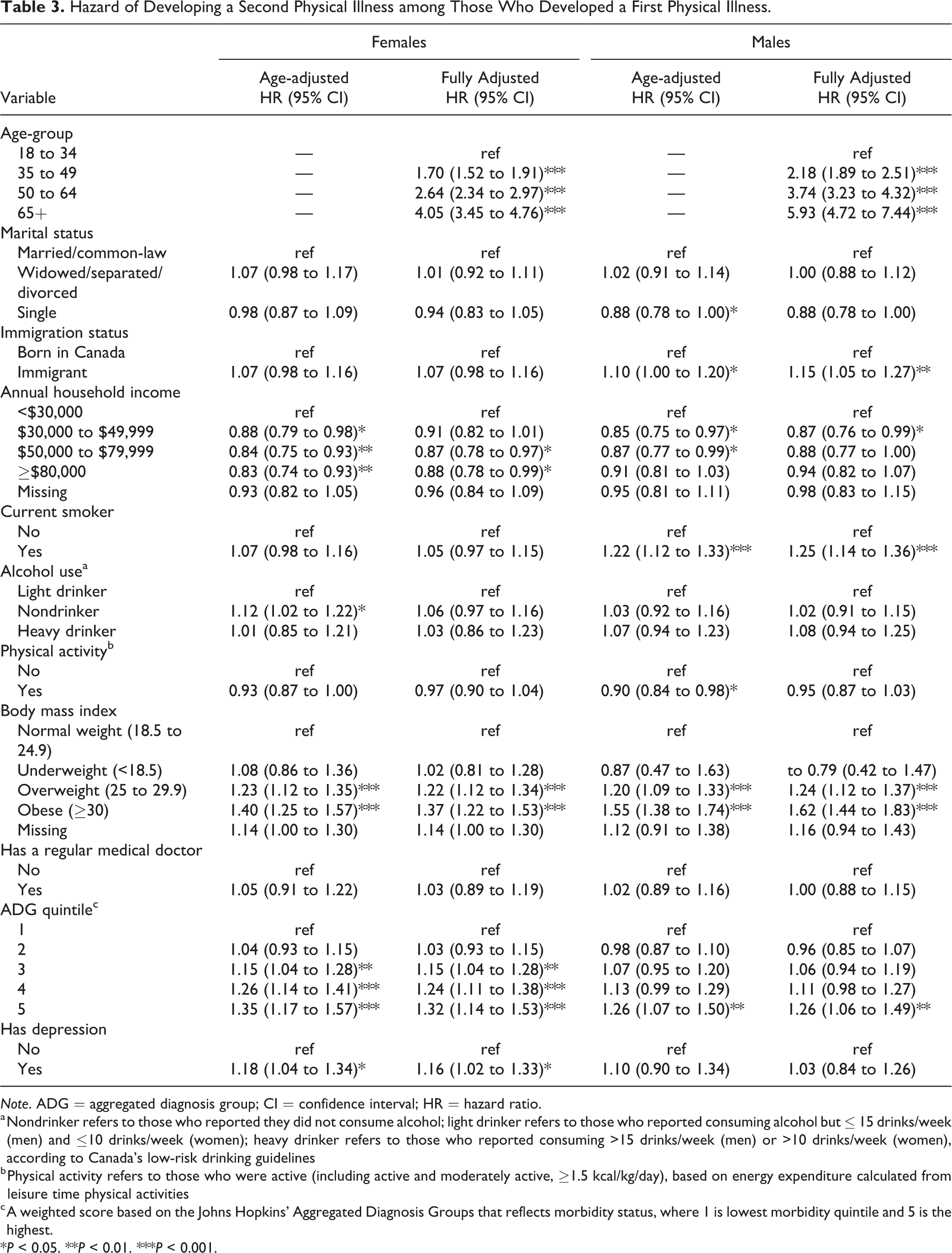
Note. ADG = aggregated diagnosis group; CI = confidence interval; HR = hazard ratio.
a Nondrinker refers to those who reported they did not consume alcohol; light drinker refers to those who reported consuming alcohol but ≤ 15 drinks/week (men) and ≤10 drinks/week (women); heavy drinker refers to those who reported consuming >15 drinks/week (men) or >10 drinks/week (women), according to Canada’s low-risk drinking guidelines
b Physical activity refers to those who were active (including active and moderately active, ≥1.5 kcal/kg/day), based on energy expenditure calculated from leisure time physical activities
c A weighted score based on the Johns Hopkins’ Aggregated Diagnosis Groups that reflects morbidity status, where 1 is lowest morbidity quintile and 5 is the highest.
*P < 0.05. **P < 0.01. ***P < 0.001.
Discussion
This cohort study found depression to be a significant risk factor for the accumulation of multimorbidity. Depression increased the risk of developing a first and second physical illness in a cohort with no comorbidities at baseline, even after controlling for socioeconomic, behavioral, and other potential confounders.
While the relationship between mental and physical illness has been posited to be bidirectional, 10,13 this longitudinal study examined the particular temporal pathway where depression occurs first and suggests that depression is an independent risk factor for the subsequent development of physical illness and multimorbidity among individuals with no such comorbidities at baseline. This finding is consistent with other studies that have examined the relationship between depression and physical illness from this direction. 40,41 The current study adds to this literature by using a specific and validated method to identify those with depression and linking survey respondents to administrative data in order to explore a range of outcome conditions over a 10-year follow-up period. Another strength of this study was the ability to control for behavioral and socioeconomic risk factors. Moreover, this study included a cohort that was free of other comorbidities at baseline, which improved the validity of the results by reducing the risk of confounding from preexisting conditions known to be risk factors for other diseases. Further exploratory analyses examining depression and the development of each individual condition, as well as the development of subsequent conditions in a cohort that included comorbidities at baseline, have been conducted and reported elsewhere online. 42
While different mechanisms for the relationship between mental illness and the development of physical illness have been suggested, 10 the underlying mechanism remains unknown. Firstly, depression may exert a biological effect, whether through serotonin metabolism, cortisol metabolism, inflammatory processes, or cell-mediated immunity. 10 Secondly, the relationship between depression and physical illness may be related to the association between depression and common risk factors for physical illness such as smoking, physical activity, and obesity. In one Canadian study, current or past smokers and women with high BMI had higher rates of depression. 17 In this study, we were able to control for some of these common risk factors and the association between depression and the development of physical illness persisted after adjustment. However, we were only able to capture values for each risk factor at baseline in the survey. Thirdly, depression may lead to different relationships with health care. People with depression may experience barriers to accessing care, different quality of care, delayed help-seeking, or problems with adherence to preventative measures, which put them at increased risk of developing physical illness. Conversely, people with depression may have more contact with the health care system as a result of their depression and thus may have greater opportunity to be diagnosed with a physical illness, leading to a form of detection bias. While we controlled for participants having a regular doctor, we did not control for number or type of visits with their doctor or the broader health care system.
This study provides evidence that depression is an independent risk factor for the development of multimorbidity and thus identifies a group of people who are at risk. Moreover, people with depression are already on the pathway to multimorbidity since they already have one condition. It is possible that clinical interventions that target the treatment of depression may reduce the risk of developing multimorbidity. While a 2015 randomized trial found that an evidence-based depression management program mitigated the combined effect of multimorbidity and depression on mortality in older adults in a primary care setting, 43 more research is needed to clarify the effect of treating depression on the development of subsequent illness. What is clear, however, is that the current study demonstrates that individuals with depression are at increased risk of developing multimorbidity over time, and this is known to be associated with complex and costly care. Additional screening for depression may be beneficial not only for depression case-finding and treatment but also for identifying a population at higher risk of developing further comorbidities. These patients may benefit from identification and aggressive management of other risk factors for the development of chronic medical conditions such as obesity and smoking. Thus, further research should examine whether policies, investments, and programs focused on screening for and managing depression may be beneficial to prevent or delay the development of multimorbidity.
Limitations
This study had several limitations. The cohorts and baseline covariates were derived from survey data. While the surveys are representative of more than 97% of the Canadian population, they do not include certain populations such as First Nations communities on reserve or the homeless. Self-report data can be subject to recall bias and social desirability bias. This could be of particular concern for variables capturing behaviors such as smoking, alcohol use, and physical activity. A stigmatized condition such as depression may have been underreported in the survey. Since depression was measured using the CIDI-SFMD and not self-reported diagnosis of depression, this was less likely to be an issue in this study. However, the CIDI-SFMD does not distinguish major depressive episodes that may have occurred in the context of a bipolar disorder or comorbid with another mental illness, which may have overestimated the effect of depression on the development of physical illness. The fact that the outcome measure was development of any of the 15 study conditions does not take into account that each condition can have different severity and impact on the patient and the health care system. However, it is common practice in multimorbidity studies to use a count of conditions as a useful abstraction, and condition count or burden has been associated with important outcomes such as cost, quality of life, and premature mortality. 1 –9
Another key limitation of this study was the fact that the covariates were only captured at baseline from the survey data, even though the participants were followed for 10 years. It is highly likely that many of these variables would have changed for each participant over the course of the follow-up period. In particular, depression status may have changed. However, a previous study found that a depressive episode carried an elevated risk of mortality that persisted for as long as 2 decades. 44 Thus, even if the participants with depression at baseline did not have depression throughout the study period, the depressive episode may have had long-term effects on the development of physical illness and subsequent multimorbidity. Furthermore, while other covariates such as physical activity or smoking status may have changed in either direction over the follow-up period, it is possible that baseline depression status leads to different uptake of these risk factors over time. Using the survey data source, it was not possible to use time-varying covariates in this study, although this would have given more reliable estimates and could help clarify the mechanism of association between depression and multimorbidity in future studies.
Conclusions
This retrospective cohort study linked the adult respondents to three Statistics Canada surveys to health administrative databases in Ontario and followed them over 10 years. Depression was found to be a significant risk factor for the development of subsequent physical illness in a cohort free of other comorbidities at baseline, even after controlling for individual-level socioeconomic, behavioral, and health care factors.
Multimorbidity is a significant problem facing patients, clinicians, and the health care system. Multimorbidity involving both mental and physical illness adds further burden, complexity, and cost. This study’s findings suggest that people with depression are at higher risk of developing subsequent physical illness, putting them on the pathway of multimorbidity. Thus, depression identifies a population of people who may benefit from early identification, additional screening, intervention, and management of other risk factors for chronic disease. More research needs to be done to determine whether and how interventions to manage and support people with depression can prevent or delay the increased risk of multimorbidity.
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720974832 - Depression as a Risk Factor for Physical Illness and Multimorbidity in a Cohort with No Prior Comorbidity: La Dépression Comme Facteur de Risque de Maladie Physique et de Multimorbidité Dans Une Cohorte Sans Comorbidité Antérieure
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720974832 for Depression as a Risk Factor for Physical Illness and Multimorbidity in a Cohort with No Prior Comorbidity: La Dépression Comme Facteur de Risque de Maladie Physique et de Multimorbidité Dans Une Cohorte Sans Comorbidité Antérieure by Allanah Li, Laura C. Rosella, Paul Kurdyak and Walter P. Wodchis in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
Data for this study are available at the Institute for Clinical Evaluative Sciences (ICES). The data are not publicly available due to the privacy restrictions at ICES and permission from ICES is required for access. The content is solely the responsibility of the authors. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred.
Acknowledgments
We gratefully acknowledge Luke Mondor from the Institute for Clinical Evaluative Sciences, for his help with creating the study cohort and data processing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Ontario Ministry of Health and Long-Term Care (MOHLTC) to the Health System Performance Research Network (HSPRN: fund #06034, recipient Wodchis), and by ICES, which is also funded by an annual grant from the Ontario MOHLTC.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.