
Abstract
Objective:
This study evaluated the contributions of clinical, sociodemographic, and service use variables to the risk of early readmission, defined as readmission within 30 days of discharge following hospitalization for any medical reason (mental or physical illnesses), among patients with mental disorders in Quebec (Canada).
Methods:
In this longitudinal study, 2,954 hospitalized patients who had visited 1 of 6 Quebec emergency departments (ED) in 2014 to 2015 (index year) were identified through clinical administrative databanks. The first hospitalization was considered that may have occurred at any Quebec hospital. Data collected between 2012 and 2013 and 2013 and 2014 on clinical, sociodemographic, and service use variables were assessed as related to readmission/no readmission within 30 days of discharge using hierarchical binary logistic regression.
Results:
Patients with co-occurring substance-related disorders/chronic physical illnesses, serious mental disorders, or adjustment disorders (clinical variables); 4+ outpatient psychiatric consultations with the same psychiatrist; and patients hospitalized for any medical reason within 12 months prior to index hospitalization (service use variables) were more likely to be readmitted within 30 days of discharge. Patients who made 1 to 3 ED visits within 1 year prior to the index hospitalization, had their index hospitalization stay of 16 to 29 days, or consulted a physician for any medical reason within 30 days after discharge or prior to the readmission (service use variables) were less likely to be rehospitalized.
Conclusions:
Early hospital readmission was more strongly associated with clinical variables, followed by service use variables, both playing a key role in preventing early readmission. Results suggest the importance of developing specific interventions for patients at high risk of readmission such as better discharge planning, integrated and collaborative care, and case management. Overall, better access to services and continuity of care before and after hospital discharge should be provided to prevent early hospital readmission.
Introduction
Early hospital readmission, defined as readmission within 30 days of previous discharge, is considered the most accurate measure of the quality of care provided during the previous hospitalization, according to the Organization for Economic Cooperation and Development mental health (MH) Panel 1 –3 and also the best indicator of effectiveness for postdischarge services offered in the community. 4 Readmission within 30 days of hospital discharge represents a negative clinical outcome 4,5 revealing discontinuity in care. Early readmission is associated with high health care costs 6,7 and increased wait times for access to inpatient units. 8
Patients with mental disorders (MD) have the highest readmission rates of all hospitalized patients. 9,10 The risk for readmission is particularly high in the immediate postdischarge period. 11 –14 Previous studies found that 5% to 15% of patients hospitalized for MD had an early readmission. 6,15 –17 Other studies have identified associations between MD and risk of early readmission due to physical illnesses 18 –22 such as heart failure, 19,20,22 chronic obstructive pulmonary disease, 19,21 pneumonia, 22 or diabetes. 19
Studies suggest that previous hospitalization was the only variable consistently associated with early readmission among patients with MD. 11,23 –27 Mixed results emerged between length of hospitalization and early readmission, most studies finding associations between longer stay and reduced readmission, 6,24,28,29 while others 30,31 found the opposite, likely due to different benchmarks for length of stay. Other service use variables associated with early readmission were lack of discharge planning, 11 health insurance, 26 and follow-up soon after discharge. 8,32 Concerning clinical variables, higher risk of early readmission was identified in association with schizophrenia, 5,33 bipolar disorders, 5,33,34 alcohol use disorder, 6 drug use disorders, 34 co-occurring physical and/substance-related disorders (SRD), 35 co-occurring MD/SRD, 30,35 symptom acuity, 11,36 and lower functionality, 26 while other studies found no associations between early readmission and clinical variables. 32,37 Sociodemographic variables associated with early readmission in the literature included homelessness or unstable housing, 16,26 unemployment and poverty 25 lack of social support, 7,16 living alone, civil status, and legal problems. 7 Regarding age, studies on patients with MD found positive associations between age and early admission in the 25 to 34, 35 to 44, 7 and younger age groups. 11 Overall readmission rates were similar between men and women. 6,29
To our knowledge, no prior studies have assessed factors associated with early hospital readmission for any medical reason, whether mental or physical conditions, among patients with MD. Moreover, most previous research on early admission among patients with MD assessed very few variables. Service use variables in particular have been understudied, such as type of region where the patient was hospitalized and continuity of care, including number of visits with the same general practitioner (GP) or the same psychiatrist, and number of psychosocial interventions provided in public primary care. Moreover, the relative weight of clinical, sociodemographic, and service use variables in early readmission have yet to be identified, which may help decision makers and clinicians charged with planning postdischarge services identify and implement more targeted interventions that may help reduce early readmission.
This study evaluated the respective contributions of sociodemographic, clinical, and service use variables to early hospital readmission for any medical reason among patients with MD in Quebec. Having included several service use variables not previously tested, we hypothesized that early readmission for any medical reason among these patients would be more strongly associated with variables involving service use, access or continuity of health care, than with clinical or sociodemographic variables.
Methods
Study Population and Design
In this longitudinal study, 2,954 patients diagnosed with MD and hospitalized for any medical reason (whether mental of physical conditions) in 2014 to 2015 (index year) were identified through clinical administrative databanks. Participants were 12 years or older and eligible for Quebec health insurance (Régie d’Assurance Maladie du Québec [RAMQ]) during the study period: 2012 to 2015. They had visited 1 of 6 selected emergency departments (ED) located in university and peripheral health regions at least once during the index year: April 1, 2014, to March 31, 2015. The first patient hospitalization in 2014 to 2015 was considered and may have taken place in any Quebec hospital. The Access to Information Commission of Quebec and the ethics committee of a MH university institute approved the study protocol.
Data Sources
Medical administrative data were collected from the RAMQ databanks, which include billing systems for most physician services, only 6% of which occur outside the public health insurance system. 38 Demographic and socioeconomic information, including material and social deprivation indices, were also available, 39 as were data from the hospitalization/discharge databank (Maintenance et exploitation de données pour l’étude de la clientèle hospitalière [MED-ECHO]). The Quebec emergency databank (Banque de données commune des urgences [BDCU]) provided additional information on, for example, patients with family physicians, illness acuity, and reasons for ED use. The local community health service center databank (Système d’information clinique et administrative des centres locaux de services communautaires), also used for this study, contained data on biopsychosocial and MH services offered in public primary care, including medical interventions provided by salaried GP.
Variables
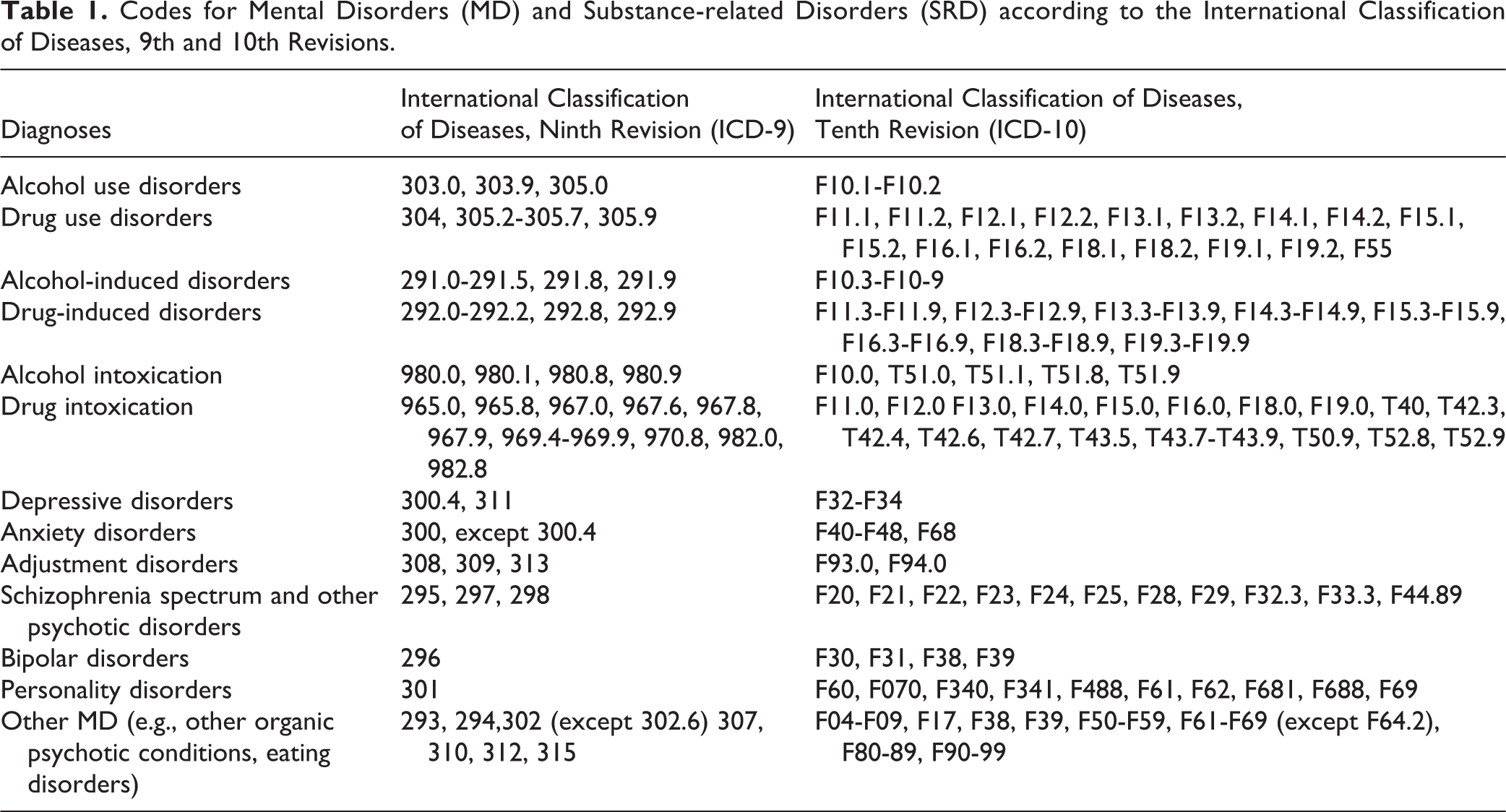
The dichotomous dependent variable was hospital readmission (yes/no) within 30 days of discharge following the index (first) hospitalization for any medical reason in 2014 to 2015. Independent variables, including clinical, sociodemographic, and service use variables, are shown in Figure 1 and linked to their specific databanks. Clinical variables included MD including SRD, chronic physical illnesses, co-occurring disorders, reasons for the ED visit leading to index hospitalization: suicidal ideation or attempt (suicide behaviors), violent behavior or social issues, and illness acuity. MD as designated in the RAMQ databank were based on the International Classification of Diseases Ninth Revision (ICD-9), and those in the MED-ECHO and BDCU databanks, from the Tenth Revision (ICD-10-CA). MD included anxiety disorders, depressive disorders, adjustment disorders (common MD); bipolar disorders, schizophrenia spectrum, and other psychotic disorders (serious MD); and personality disorders. SRD comprised alcohol-related disorders (alcohol use disorders, alcohol induced disorders, alcohol intoxication) and drug-related disorders (drug use disorders, drug induced disorders, drug intoxication). Diagnostic codes for MD and SRD are shown in Table 1. Based on the Elixhauser comorbidity index, 40 having chronic physical illnesses or not and level of severity (0 to 3+) were recorded. Different combinations of co-occurring disorders involving SRD and chronic physical illnesses were included. SRD and MD had to be recorded at least once prior to the index year (in 2012 to 2013 or 2013 to 2014); and chronic physical illnesses either twice yearly in the RAMQ databank or once in the MED-ECHO as established in previous research. 41 Suicidal, social, or violent behavioral issues and reasons for ED visit leading to index hospitalization were extracted from the 2014 to 2015 BDCU. The Canadian Triage Acuity Scale 42 was used to measure illness acuity at the ED visit prior to index hospitalization, ranging from levels 1 to 2 (immediate and very urgent), 3 (urgent), to 4 to 5 (less urgent and non-urgent care). Levels 4 and 5 indicate the appropriateness of outpatient treatment over ED. 42
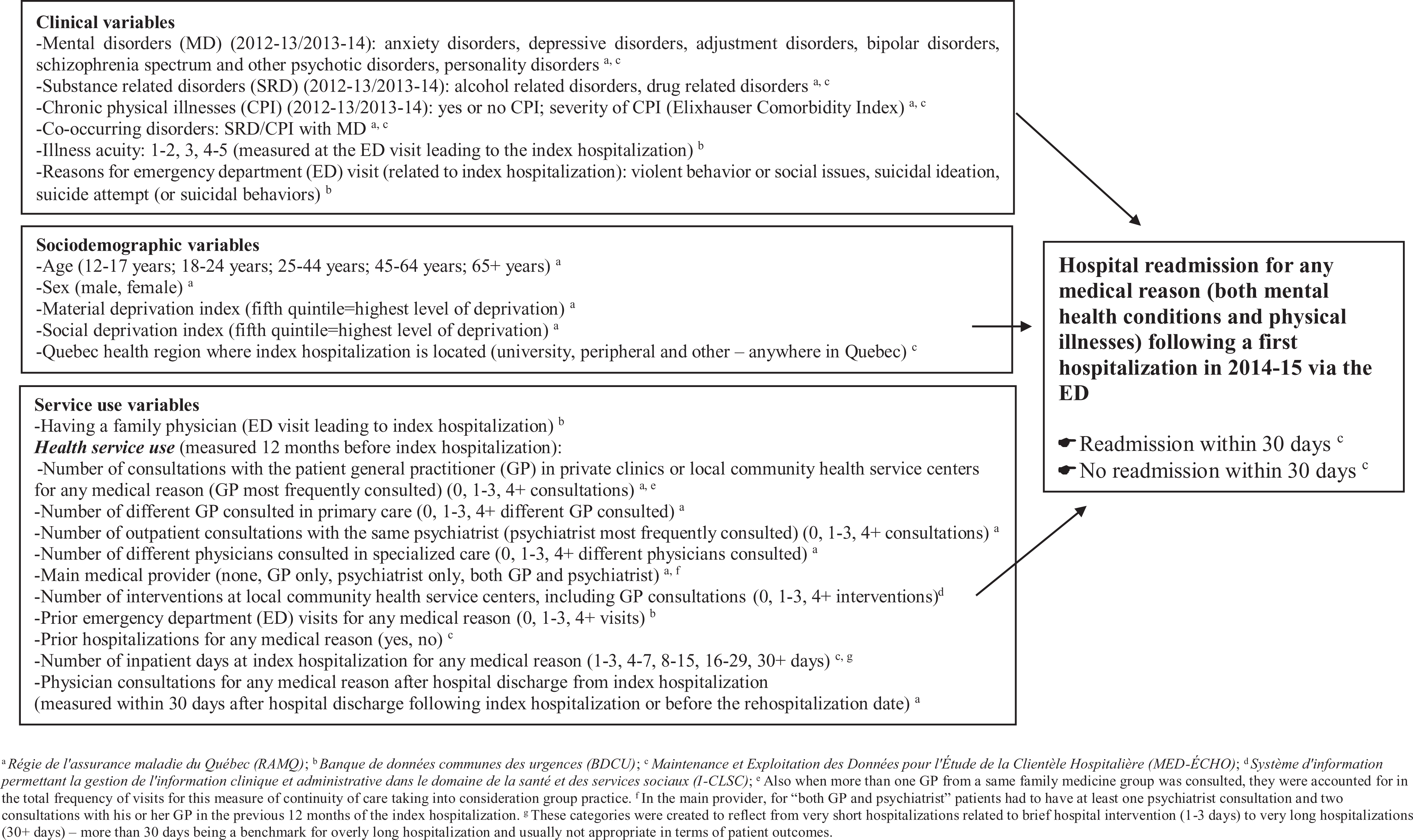
Conceptual framework: variables tested for association with rehospitalization/no rehospitalization within 30 days of discharge following a first hospitalization in 2014 to 2015 for any medical reason among patients with mental disorders.
Codes for Mental Disorders (MD) and Substance-related Disorders (SRD) according to the International Classification of Diseases, 9th and 10th Revisions.
Sociodemographic variables included sex (male, female), age (categorized as 12 to 17, 18 to 24, 25 to 44, 45 to 64, and 65+ years), health regions, and material and social deprivation derived from the Canadian census (2011). 39 Quebec health regions were measured for the index hospitalization and classified as university, peripheral, and other regions (intermediary and remote regions). The material deprivation index considers individual to population employment ratios, proportion of individuals without a high school diploma, and average income. 39 The social deprivation index includes data on individuals living alone, single-parent families, and civil status. 39 Both indices are classified in quintiles, with the fifth quintile representing highest level of deprivation.
Service use variables included having a family physician and health service use in the 12 months preceding the index hospitalization, that is, number of consultations with the patient GP (i.e., the GP mostly frequently consulted) for any medical reason in primary care (0, 1 to 3, 4+); 43 number of consultations with the patient outpatient psychiatrist (the one mostly seen; 0, 1 to 3, 4+); number of different GP consulted in primary care (0, 1 to 3, 4+); number of different physicians consulted in specialized care (0, 1 to 3, 4+); main medical provider (none, GP only, psychiatrist only, both GP and psychiatrist); 44 number of interventions at local community health service centers including GP consultations (0, 1 to 3, 4+); prior consultations at ED (0, 1 to 3, 4+); prior hospitalizations for any medical reason (yes/no); and number of inpatient days at the index hospitalization for any medical reason (1 to 3, 4 to 7, 8 to 15, 16 to 29, 30+). Finally, physician consultations for any medical reason after discharge from the index hospitalization were measured within 30 days of discharge or before readmission if prior to 30 days.
Statistical Analyses
Only 0.5% of the data were missing, so the complete cases were used for the multivariable regression. Descriptive analyses were performed including 2-way frequency tables for independent variables, in association with the dependent variable (yes/no for readmission within 30 days of discharge). As the effect of clustering at the hospital-center level (62 hospital units) was small (intraclass correlation coefficient: 0.096), a multilevel model was not needed. Collinearity statistics were tested using variance inflation factors (VIF) and tolerance tests, with 5 as the maximum level of VIF. Independent variables without collinearity were entered in the model at alpha value P < 0.10. Hierarchical logistic regression was conducted, with clinical variables introduced first into the model, as the variables most highly correlated with ED visits and hospitalizations according to the literature, followed by sociodemographic variables, then service use variables. 45 –47 A stepwise forward method was also used for the estimation of parameters in the hierarchical logistic regression model. Odds ratios were calculated with 95% confidence intervals. The reference category was patients not hospitalized within 30 days of hospital discharge. All analyses were performed using SPSS 24.0.
Results
After removal of the 100 patients (3.3%) not hospitalized via ED, the remaining cohort included 2,954 patients with MD hospitalized for any medical reason via the ED, 51% for MH conditions and 49% for physical illnesses. Of these, 243 (8%) were readmitted within 30 days of discharge. Table 2 presents sample characteristics. Concerning clinical variables for the 2 years prior to the ED visit leading to index hospitalization, 55% of patients had common MD (depressive disorders, anxiety disorders, adjustment disorders), 58% serious MD (schizophrenia spectrum and other psychotic disorders, bipolar disorders), and 25% SRD. Forty-five percent were diagnosed with chronic physical illnesses, yet severity levels were low in 65% of cases (index 0), according to the Elixhauser comorbidity index. Co-occurring SRD/chronic physical illnesses were identified for 17% of patients. Thirty-three percent presented with suicide ideation and 11% with suicide attempt. Six percent visited ED for violent behavior and 2% for social issues. Before hospitalization, most patients (40%) presenting at ED were registered at illness acuity level 3 (urgent).
Characteristics of Patients with Mental Disorders (MD) Hospitalized in 2014 to 2015 for any Medical Reason (Index Hospitalization) and Who Were Readmitted/Not Readmitted within 30 Days of Discharge.
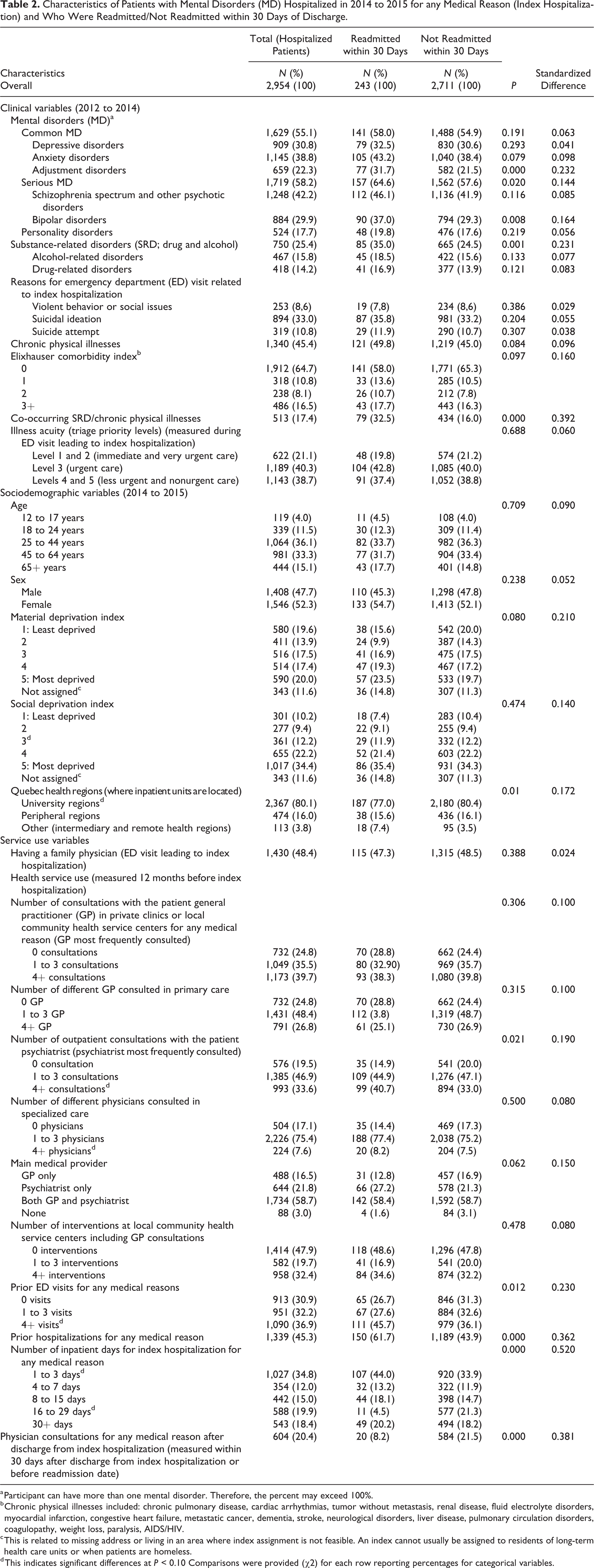
a Participant can have more than one mental disorder. Therefore, the percent may exceed 100%.
b Chronic physical illnesses included: chronic pulmonary disease, cardiac arrhythmias, tumor without metastasis, renal disease, fluid electrolyte disorders, myocardial infarction, congestive heart failure, metastatic cancer, dementia, stroke, neurological disorders, liver disease, pulmonary circulation disorders, coagulopathy, weight loss, paralysis, AIDS/HIV.
c This is related to missing address or living in an area where index assignment is not feasible. An index cannot usually be assigned to residents of long-term health care units or when patients are homeless.
d This indicates significant differences at P < 0.10 Comparisons were provided (χ2) for each row reporting percentages for categorical variables.
Regarding sociodemographic variables, most patients (36%) were between 25 and 44 years of age, and 52% were female. Material deprivation levels varied little. However, 68% of patients lived in the most socially deprived area (4 to 5) or areas not assigned. Eighty percent were hospitalized in university health regions.
Regarding service use variables, 48% of patients reported having a family physician. In the 12 months prior to index hospitalization, 36% of patients had 1 to 3 consultations with the same GP in primary care, 40% had 4+, and 25% had none. Regarding primary care medical consultations in general, 48% had seen 1 to 3 different GP, and 27% 4+. Of the 81% who consulted their outpatient psychiatrist, 47% had 1 to 3 consultations, and 34% had 4+. In terms of specialized care provision, 75% were seen by 1 to 3 different medical specialists, and 8% by 4+. Nearly 59% of patients had been seen by both a GP and a psychiatrist 12 months prior to index hospitalization, 16% by GP only and 22% by psychiatrist only (3% by neither). Nearly half (48%) of patients did not consult local community health service centers; 32% visited ED 1 to 3 times, and 37% 4+ times, while 45% had prior hospitalizations for any medical reason. At the index hospitalization, 35% of patients were hospitalized for 1 to 3 days, 12% for 4 to 7 days, 15% for 8 to 15 days, 20% for 16 to 29 days, and 18% for 30+ days. Within the 30-day period before readmission, 20% of patients consulted a physician for any medical reason. Independent variables significantly associated with frequency of readmission within 30 days of the index hospital discharge in the bivariate analyses are also presented in Table 2.
Table 3 presents results for the hierarchical binary logistic (multivariate) regression. Concerning clinical variables (first model), patients with adjustment disorders, serious MD, or co-occurring SRD/chronic physical illnesses were more likely to be readmitted early. These variables remained significant in the final model. Adding sociodemographic variables (Model 2) revealed that patients hospitalized within 30 days of discharge were more likely to be hospitalized in health regions other than those with university-affiliated hospitals. However, with further introduction of service use variables (Model 3), the significant associations for health regions disappeared. In terms of service use variables, patients who consulted the same outpatient psychiatrist 4 times+ and were hospitalized for any medical reason in the 12 months prior to index hospitalization were more likely to be readmitted within 30 days of discharge. Those who made 1 to 3 ED visits in the 12 months before the index hospitalization remained in hospital 16 to 29 days during the index hospitalization, and those who consulted a physician for any medical reason within a 30-day period after discharge or prior to readmission were less likely to be readmitted within 30 days of discharge. Clinical variables accounted for 52% of the total variance explained in the model, while service use variables contributed for 42% and sociodemographic variables 6%.
Predictors of 30-day Hospital Readmission for Patients with Mental Disorders Hospitalized for Any Medical Reason (Index Hospitalization in 2014 to 2015).
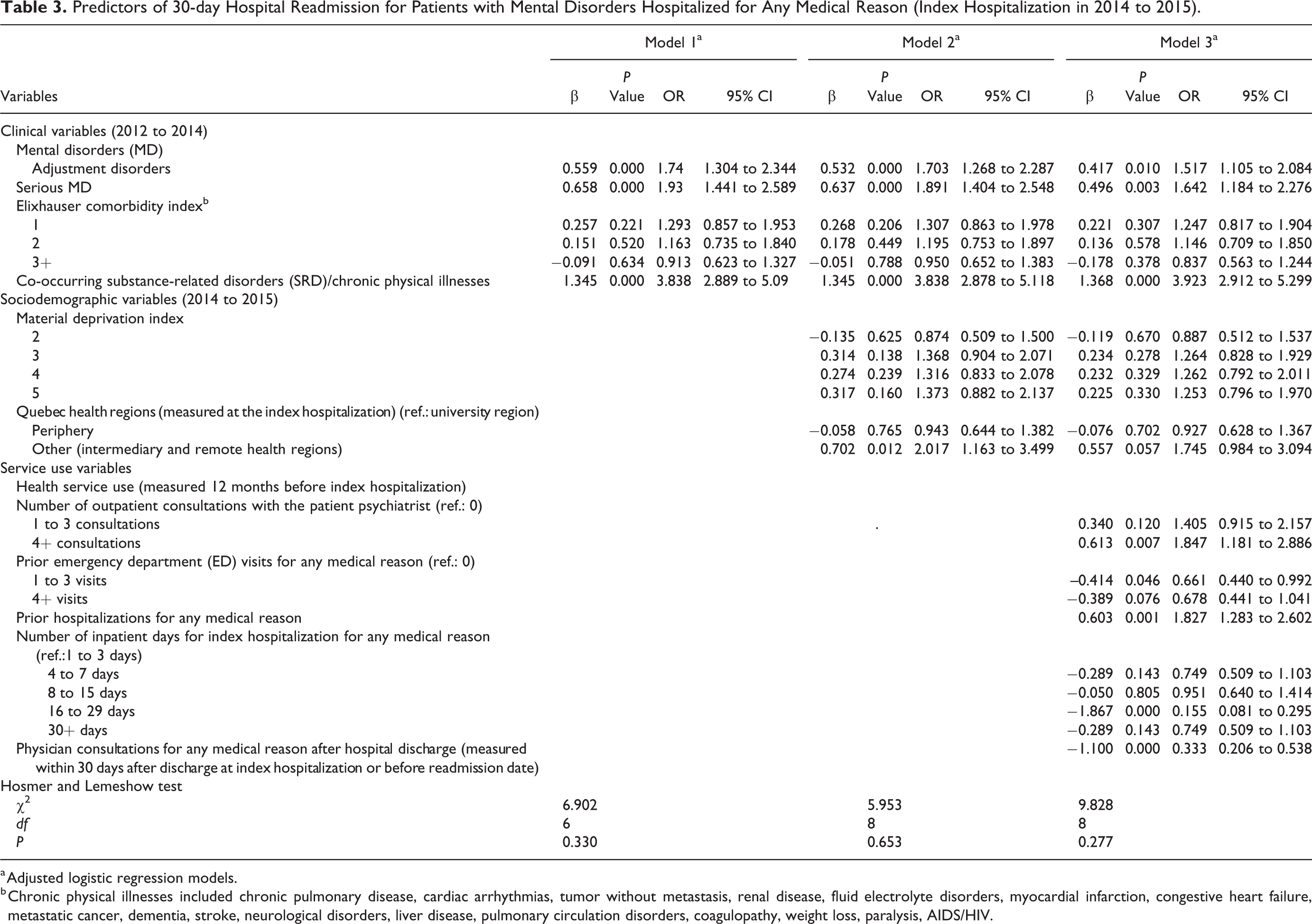
a Adjusted logistic regression models.
b Chronic physical illnesses included chronic pulmonary disease, cardiac arrhythmias, tumor without metastasis, renal disease, fluid electrolyte disorders, myocardial infarction, congestive heart failure, metastatic cancer, dementia, stroke, neurological disorders, liver disease, pulmonary circulation disorders, coagulopathy, weight loss, paralysis, AIDS/HIV.
Discussion
The study results showed that 8% of patients were readmitted within 30 days of hospital discharge, falling in the “5% to 15%” or low range as established in previous studies on early readmission after discharge for patients with MD. 6,15,16 Results did not confirm our hypothesis that early hospital readmission would be most strongly associated with service use variables. Clinical variables contributed most to the total variance in the final model but closely followed by service use variables. Sociodemographic variables were weakly associated with early readmission, as in most previous studies that included variables such as age 7,11 and sex. 6,29
Results related to clinical variables indicated a key association between early readmission and illness severity. Co-occurring SRD/physical illnesses were the strongest variables associated with early readmission for patients with MD. This was logical as studies often describe these patients as frequent users of ED and inpatient hospital services. 48,49 Early readmission may have resulted from the absence of integrated MD/SRD services, 50 difficulty accessing ambulatory care, 51 or stigmatization from health care professionals. 52 Some studies also found that patients with substance misuse 53 or drug use disorders 34 often have difficulty accessing addiction treatment. Yet, it is possible that some patients were reluctant to use these services, as studies often show. 53 Overall, few services are available for patients with SRD in either community or hospital settings. 50,54 The implementation of SRD liaison nurses in ED 50 and integrated treatment 55 may help the screening of such patients and their coordination with appropriate services. Moreover, chronic physical illnesses (e.g., pulmonary disease, neurological disorders, liver disease) complicate treatment, reduce life expectancy and promote higher use of acute care, increasing the risks of readmission for patients with MD and/or SRD. 19,34,56 Collaborative care between MH services and primary care would be particularly appropriate for this clientele experiencing multiple health problems. 57 The association between early readmission and serious MD was previously reported. 7,16,27 One explanation may be that patients with serious MD may have problems with medication adherence. 7 They also may not receive adequate support from services or from their families after discharge, increasing risks of rehospitalization. 7 Patients with serious MD need expedited access to care and intensive follow-up, as offered by assertive community treatment, intensive case management teams or day hospitals 58 to avoid readmission. The association between adjustment disorders and early readmission has rarely been observed. Yet, adjustment disorders are a frequent diagnosis among patients at first hospitalization, mainly among adolescents or young adults; and for some, the diagnosis may change at rehospitalization. 59,60 As well, adjustment disorders are strongly associated with repeated suicidal behaviors, which may explain the high prevalence of affected patients in acute care hospital services. 61,62 For this common MD, brief psychological interventions may be the most appropriate treatment. 63
Results on service use variables also demonstrated a systemic deficit in access to and continuity of care among study participants readmitted early. Among service use variables positively associated with early readmission, previous hospitalization was strongest, which coincides with results in previous studies related to psychiatric hospitalization. 11,25,64 However, our study also included previous hospitalization for medical reasons other than MD. The association between having 4+ outpatient consultations with patient psychiatrist before the index hospitalization and readmission within 30 days of discharge contradicts previous research claiming that greater access to outpatient services helped reduce the risk of frequent ED use or readmissions. 65 However, most studies did not control for frequency of visits, suggesting that the intensity of previous outpatient consultations or quality of care (e.g., type of treatment) may have been inadequate to meet patient needs, contributing to readmissions. This also confirms the great severity of psychiatric symptoms experienced by patients with 4+ outpatient consultations. Patients making frequent psychiatric consultations tend to be those with more complex or serious MD and co-occurring health and social problems, 66,67 whose needs are often characterized as unmet, 68 –70 and requiring very intensive, fully integrated biopsychosocial care. 70,71
Patients having 1 to 3 prior 12-month ED visits were identified as less likely to be readmitted early. It may be that these patients, known to ED and specialized services, were provided with more intensive care that prevented readmission as well as their risk of becoming high ED users. Previous Quebec MH or SRD reforms reinforced programs such as assertive community treatment, intensive case management, 72 home treatment teams, 73 SRD liaison model at ED, 50,74 and community-based crisis interventions, 75 all of which are known to reduce ED visits and hospitalizations. Our results also demonstrated that patients hospitalized 16 to 29 days were less likely to be readmitted early, as compared to those hospitalize 1 to 3 days. While not a significant finding, this trend seems reversed for those hospitalized 30+ days. In general, patients with MD discharged after longer stays were found in previous studies to have more stable conditions 28 and were less likely to be readmitted. 6,28,29,76 However, hospitalizations exceeding 30 days is also considered an indicator of inadequate quality of care. 77 Finally, results show that physician consultation for any medical reason within 30 days of discharge was negatively associated with readmission. Studies recommend that physician consultations should occur within the first 10 to 21 days, 78 or at least within the first 30 days of discharge, 13,79 in order to have a protective effect. Previous studies also found that the risk of early readmission increased when patients did not attend their first outpatient consultation 12 or when consultations were not scheduled soon after discharge; 9,79 the same was true for early return to ED following discharge. 80
Limitations
This study had certain limitations. First, administrative databanks were primarily developed for financial purposes and not for research. They thus represent a proxy for patient service use and clinical conditions. Second, some key data such as race/ethnicity, medication compliance, health care professional use other than physicians, community-based services, or collaborative care that may have shown associations with early readmission were not available from Quebec databanks. Finally, results may be not generalizable to all hospitalized patients with MD, particularly in settings more outside university health regions and with health care systems without universal coverage.
Conclusions
Drawing on variables not previously analyzed, this study determined that readmission within 30 days of hospital discharge among patients with MD was more strongly associated with clinical variables, mainly co-occurring SRD/chronic physical illnesses and serious MD, which reflects the limits of health care services to treat patients with the most serious mental and physical health conditions. However, several service use variables were identified that may play a key role in preventing early readmission and should be prioritized in health policy and service planning. Thus, this study demonstrated the importance of ensuring a sufficiently long hospital stay (from 16 to 29 days) before discharge, and the benefit of consultations soon after discharge for avoiding early readmission. Results also show the usefulness of developing specific interventions for patients at high risk of readmission. SRD liaison nurse at the ED, integrated treatment, and collaborative care might be more widely deployed to facilitate treatment and follow-up for patients affected by co-occurring SRD and chronic physical illnesses. Best practices such as assertive community treatment, intensive case management, day hospital or home treatment, and community-based crisis services may be further harnessed for patient follow-up among those with serious MD. For adjustment disorders, brief psychological interventions are recommended. Overall, increased adequacy of access to health services and continuity of care before and after hospital discharge, including better discharge planning, would likely prevent early hospital readmission and should be more widely prioritized in future MH action plans.
Footnotes
Authors’ Note
The data sets analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We gratefully acknowledge the support of the Canadian Institutes of health Research (CIHR).We would also like to thank the the Fonds de la recherche en santé du Québec (FRQ-S) for awarding a postdoctoral fellowship to the first author. We would also like to thank Judith Sabetti for editorial assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of health Research (CIHR; Grant Number 8400997).