
Abstract
Background:
Many people experience early signs and symptoms before the onset of psychotic disorder, suggesting that there may be help-seeking prior to first diagnosis. The family physician has been found to play a key role in pathways to care. This study examined patterns of primary care use preceding a first diagnosis of psychotic disorder.
Methods:
We used health administrative data from Ontario (Canada) to construct a population-based retrospective cohort. We investigated patterns of primary care use, including frequency and timing of contacts, in the 6 years prior to a first diagnosis of psychosis, relative to a general population comparison group matched on age, sex, geographic area, and index date. We used latent class growth modeling to identify distinct trajectories of primary care service use, and associated factors, preceding the first diagnosis.
Results:
People with early psychosis contacted primary care over twice as frequently in the 6 years preceding first diagnosis (RR = 2.22; 95% CI, = 2.19 to 2.25), relative to the general population, with a sharp increase in contacts 10 months prior to diagnosis. They had higher contact frequency across nearly all diagnostic codes, including mental health, physical health, and preventative health. We identified 3 distinct service use trajectories: low-, medium-, and high-increasing usage.
Discussion:
We found elevated patterns of primary care service use prior to first diagnosis of psychotic disorder, suggesting that initiatives to support family physicians in their role on the pathway to care are warranted. Earlier intervention has implications for improved social, educational, and professional development in young people with first-episode psychosis.
Background
The prodrome to psychotic disorder is the period that begins with a deviation from a person’s previous behavior and extends to the onset of overt psychosis. 1,2 This prodromal phase can range from several weeks up to several years in duration. 3 It is determined retrospectively after a first diagnosis of psychosis and is characterized by the presence of heterogeneous and nonspecific symptoms including depression, anxiety, social withdrawal, and attenuated positive and negative symptoms. 4 This suggests that there may be help-seeking for mental health problems several years prior to the first diagnosis of psychotic disorder—indeed, prior research suggests that people with psychotic disorders were in contact with the mental health system for a median of 6 years preceding first diagnosis, 5 with missed opportunities for early detection and intervention. 3 Efforts to diagnose and minimize the duration of untreated psychosis during the early phase of illness—referred to herein as early psychosis—are essential for improving long-term outcomes. 6 –10
Pathways to care are the modes by which patients with mental health problems access help, including the help-seeking behavior of both the patient and family, the accessibility of mental health services, and the identification of and response to symptoms by each contact on the pathway to care. 11 For young people in the early stages of psychotic illness, pathways to care are complex, with multiple diverse contacts and associated treatment delays. 11,12 Young people with early psychosis often make multiple help-seeking attempts across providers and may experience negative and aversive pathways to care involving the criminal justice system, emergency department (ED), or inpatient unit. 13 –15 These contacts are associated with poor patient experience, disengagement from services, and high costs. 14
We know that collectively, family physicians play an important role in the pathways to care for people with early psychosis. 16 We have previously shown that nearly two thirds of young people with early psychosis make help-seeking attempts in primary care in the 6-month period preceding first diagnosis, and 1 in 3 people receive their first diagnosis from a family physician. 17 Involvement of a family physician on the pathway to care reduces negative and aversive service contacts (i.e., police, ambulance, and the ED) and inpatient admission 14,16,18,19 and therefore is beneficial for improving service-related outcomes. 20 However, early psychosis is still a relatively infrequent occurrence in primary care, due to the low incidence of psychotic disorders, 21 and family physicians estimate that they may only see 1 or 2 patients per year with the signs and symptoms of first-episode psychosis. 22 Consequently, the importance of the family physician in early detection and intervention for psychotic disorder has gone largely unrecognized, and there is a need for early psychosis intervention services to more actively engage with the primary care sector. 23 However, there is a notable lack of literature on patterns of primary care use for young people with first-episode psychosis. Of exception, 2 prior studies have used health administrative data to look at help-seeking from a family physician before the first diagnosis of psychosis, showing that people with psychotic disorders have elevated contact rates in primary care up to 6 years prior to first diagnosis 24 and that consultation patterns may be used to identify high-risk subgroups who might benefit from further assessment and monitoring. 25 Because these patterns of service use will be highly dependent on the health system context, there is a need for Canadian data on this topic to highlight the important role of Canadian family physicians in pathways to care and identify opportunities for early psychosis intervention.
The objective of this study was to explore patterns of service use in primary care preceding a first diagnosis of nonaffective psychotic disorder. Using data from the provincial public health insurance plan in Ontario, Canada, we sought to compare the frequency and timing of primary care visits, and associated diagnostic categories, among people with early psychosis, relative to a matched comparison group from the general population. We also sought to identify distinct trajectories of service use in primary care and associated factors. This study uses a similar approach as Nørgaard and colleagues, 24 who analyzed primary care contacts among people with schizophrenia in Denmark, with additional analyses of the timing and trajectories of service use.
Methods
Study Design and Data Sources
We used population-based health administrative data to construct a retrospective cohort of people aged 14 to 35 years with newly diagnosed nonaffective psychotic disorder between April 2005 and March 2015 and a matched comparison group from the general population. We chose this age group because it is considered a priority population for early intervention by the Ontario Ministry of Health and Long-Term Care. 26 The linked databases are detailed in Online Appendix A and included information on basic sociodemographic characteristics, physician billings, hospitalizations, and ED visits. The data sets were linked using unique encoded identifiers and analyzed at ICES, which is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. We followed the Reporting of studies Conducted using Observational Routinely-collected Data (RECORD) guidelines for studies using health administrative data (Online Appendix B). 27
This study was based primarily on data from the Ontario Health Insurance Plan (OHIP), which contains physician billing claims paid for by the provincial public health insurance plan. The database includes information from approximately 94% of physicians in Ontario but excludes physicians paid by salary or other alternative practice models who do not submit shadow billings.
Cohort Definition
New cases of nonaffective psychotic disorder (i.e., schizophrenia, schizoaffective disorder, schizophreniform disorder, or psychosis not otherwise specified [NOS]) were identified by either a primary discharge diagnosis of nonaffective psychosis from an inpatient admission or at least 2 physician billing claims or ED visits with a diagnostic code for nonaffective psychosis in any 12-month period. A modified version of this algorithm has been validated using medical charts, 28 and this approach has been previously used to compute the incidence of nonaffective psychotic disorders in Ontario. 21,29 The index date was defined as the discharge date for cases identified from hospitalizations or the date of the first physician visit for cases identified from outpatient billings. People were excluded if they were missing data for age and sex variables (<1%).
All members of the general population who were eligible for OHIP and had no record of a psychotic disorder diagnosis were randomly assigned an index date from the distribution of index dates among the cases. We randomly selected 4 comparisons per case from the general population, matched on age at index date, sex, geographic area (based on first 3 digits of the postal code), and index date (± 6 months), using the greedy method without replacement. 30
Variable Definitions
Contact with primary care was defined as a visit with a family physician or pediatrician in an outpatient setting. We extracted information on all contacts with primary care for each person in the study cohort for the 6-year period preceding the index date. We generated counts for the total number of contacts, the number of contacts per year, and the number of contacts bimonthly over the observation period. We also computed the number of contacts per diagnostic code category and created a binary indicator variable to identify those who contacted primary care at least once with a given diagnostic code category over the observation period. Diagnostic code categories were further subdivided as mental health, physical health, and preventative health.
Sociodemographic variables included age at index date, sex, and rural place of residence. Age was categorized into groups by ICES (Table 1) to mitigate reidentification risk. Clinical factors included the type of psychotic disorder diagnosis (cases only, classified as schizophrenia spectrum or psychosis NOS), presence of an aggregated diagnosis group (ADG) chronic medical condition, and presence of an ADG chronic psychosocial condition. The Johns Hopkins Adjusted Clinical Group® System Version 10 31 categorizes illnesses into 32 diagnostic clusters, known as ADGs, with similar clinical criteria and expected need for health care resources based on International Classification of Disease codes, which are obtained from both physician billing claims and hospital discharge abstracts. 32,33 Finally, variables reflecting service use history in the previous 2 years were created to indicate whether each person had access to a regular family physician and whether each person had a psychiatric ED visit or hospitalization in the 2 years prior to the index date. All covariates were measured at the index date.
Sociodemographic, Clinical, and Service Use History Characteristics for Cases with Early Psychosis and the General Population Comparison Group.
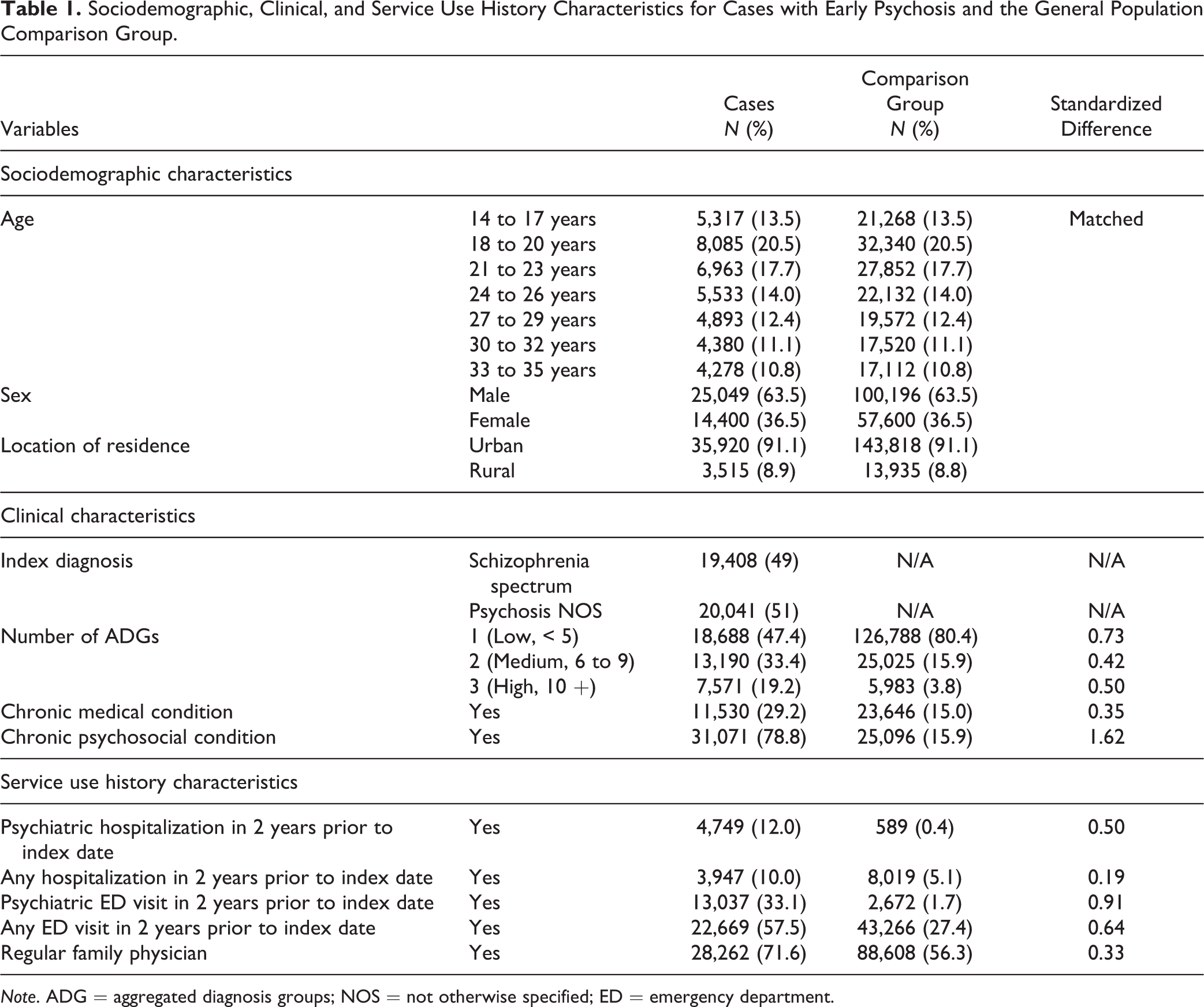
Note. ADG = aggregated diagnosis groups; NOS = not otherwise specified; ED = emergency department.
Statistical Analyses
Analyses were conducted using SAS (Version 9.4) and R (Version 3.3.0). We used frequencies and proportions, as well as medians and interquartile ranges (IQR), to describe the sample and the number of primary care contacts for each group. Standardized differences were computed to examine differences between case and comparison groups 33 —standardized differences greater than 0.10 were considered significant. 34
To compare the number of primary care contacts in the 6 years prior to the index date, we used a negative binomial regression model with robust variance estimators to account for the matched design. Among people with early psychosis, we examined the timing of changes in the frequency of primary care contacts using change-point analysis. Change-point analysis models the process of a sequence of observations undergoing sudden change at unknown times and to determine the point at which a change occurred. 35 We used change-point analysis to identify time points where changes occurred in the average number of contacts with primary care per person bimonthly prior to index date. We used the R changepoint package for analysis, and the cpt.meanvar function with binary segmentation (BinSeg) method was used to detect at least 1 change in the mean and/or variance of the data. 36 The time points in the sequence of observations where a change was detected and percentage of mean difference in change were calculated.
We compared reasons for primary care contacts between cases and comparisons using diagnostic codes associated with primary care contacts. We used unadjusted log-linked binomial models with robust variance estimators, stratified by sex, to estimate the relative risk (RR) and associated 95% confidence intervals (CI) of contacting primary care within each diagnostic category in the 6 years prior to the index date for people with early psychosis, relative to the matched comparison group. For models comparing the frequency and reasons for primary care contacts between cases and controls, we used unadjusted models because cases and their comparisons were matched on age at index date, sex, and location of residence and also because other clinical and service use covariates will impact the frequency of primary care service use, and including these variables in analyses may adjust away any effect.
Finally, we used latent class growth modeling (LCGM) to identify distinct service utilization trajectories among people with early psychosis in the 6 years preceding diagnosis. LCGM is used to identify distinct subgroups of people following a similar pattern of change over time on a given variable. 37 First, a linear trajectory was modeled for one subgroup, then additional subgroups were added until the adjusted model fit worsened. With the number of subgroups determined, the optimal trajectory shape (i.e., linear, quadratic, cubic) for each group was tested until the adjusted model fit worsened and nonsignificant polynomial terms were removed, resulting in the final model. 38 A detailed description of the model selection process and the statistical parameters of the model is available in Online Appendix C. Variables entered in the LCGM included the number of primary care contacts per year for each of the 6 years of observation. The number of primary care contacts was categorized into deciles based on the sample distribution (0, 1, 2 to 4, 5 to 7, 8 to 10, 11 to 14, 15 to 18, 19 to 25, 26 to 37, 38+ contacts). We again chose not to include additional covariates in the LCGM, so that our ability to meaningfully observe primary care service use in this population was not obstructed. Once the service use trajectories were identified, we used log-linked binomial models to examine sociodemographic, clinical, and service use factors associated with the high-use trajectory. These variables were chosen based on established evidence of their relationship with primary care service utilization, and there was no indication of multicollinearity.
Results
We identified 39,449 incident cases of nonaffective psychosis over the 10-year period, matched to 157,796 comparisons (Table 1). Of the identified cases, 59.5% (n = 23,469) made help-seeking attempts for mental health reasons in primary care prior to first diagnosis, whereas the remainder were diagnosed in secondary or tertiary care with no prior mental health contacts in primary care. Significant differences between people with early psychosis and the comparison group were found for clinical and service use indicators (Table 1).
Over the 6-year period leading up to first diagnosis, 97.3% (n = 38,379) of people with early psychosis had any primary care contact (for both mental health and nonmental health related visits), compared to 76.4% (n = 120,600) of the comparison group. The median number of contacts over this period was 19 (IQR = 10,36) for people with early psychosis and 8 (IQR = 1,18) for the comparison group (standardized difference = 0.82). People with early psychosis contacted primary care over twice as frequently in the 6 years leading up to first diagnosis, relative to the comparison group (RR = 2.22; 95% CI, 2.19 to 2.25). The median number of primary care contacts per year begins to increase approximately 2 years before diagnosis for people with early psychosis, with no change for the comparison group over the 6-year observation period (Online Appendix D).
Five change points were detected in the mean number of primary care contacts per person with early psychosis, specifically at 56, 46, 30, 20, and 10 months prior to first diagnosis (Figure 1). The percentage mean difference between change points increases slightly at each time point from 105% at the first to second change point to 113% at the third to fourth time point although these differences are small and unlikely to be of clinical significance. However, there is a large increase in the percentage mean difference (140%) from the fourth to fifth change point, which occurs at 10 months before first diagnosis.
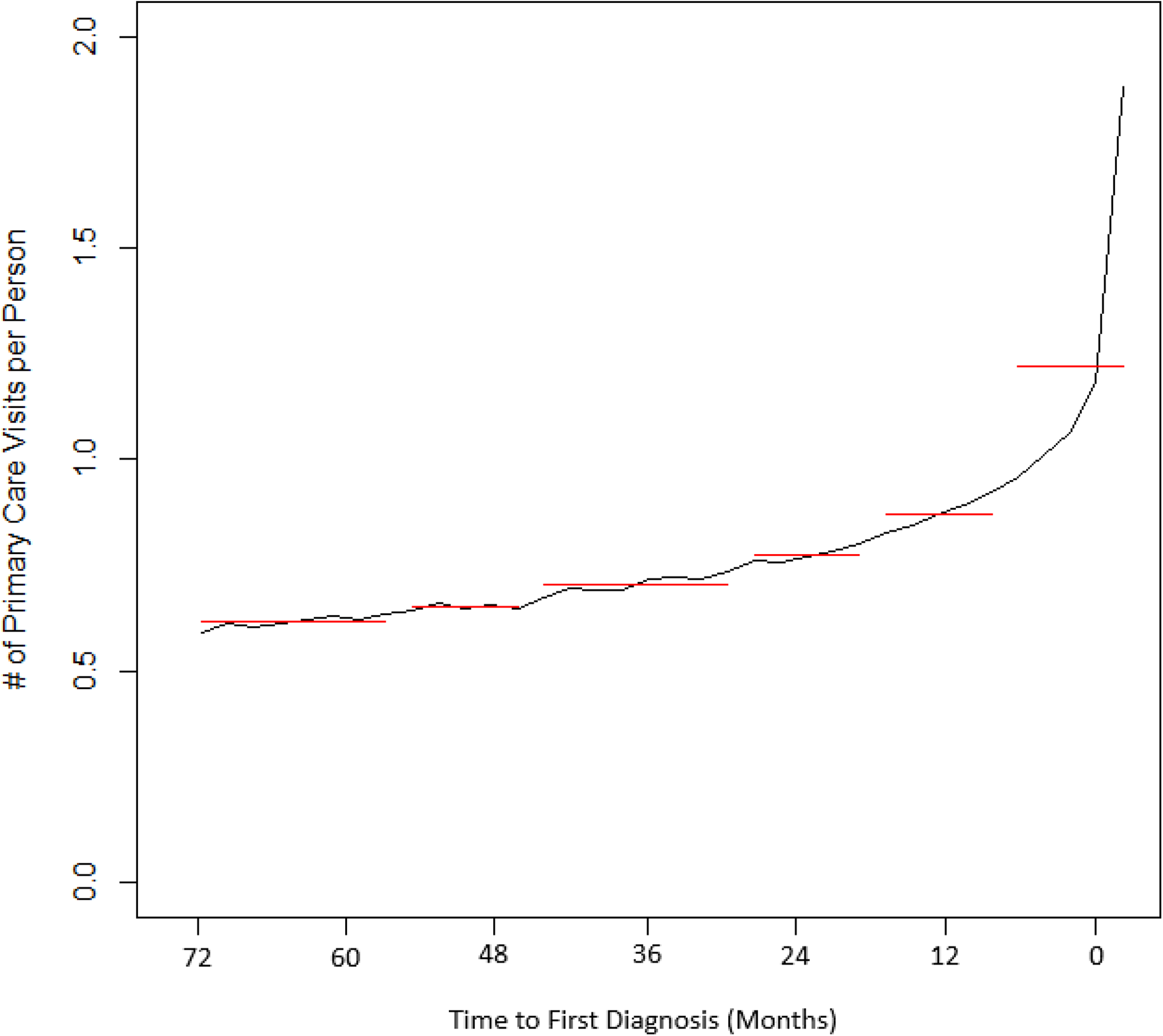
Mean number of primary care contacts per case with early psychosis, counted bimonthly over the 6 years leading up to first diagnosis (black line) and change point locations detected (red lines). Significant change points detected at 56, 46, 30, 20, and 10 months prior to first diagnosis.
Diagnostic Codes Associated with Primary Care Use
Both males and females with early psychosis have a higher prevalence of primary care contacts across nearly all diagnostic code categories, including mental health, physical health, and preventive health, compared to their matched comparisons (Table 2).
Proportions and RR for Diagnostic Code Categories associated with Primary Care Contacts for Male and Female Cases with Early Psychosis and the General Population Comparison Group, Who Contacted Primary Care At Least Once in the 6 Years Leading up to First Diagnosis, for Each Diagnostic Category.
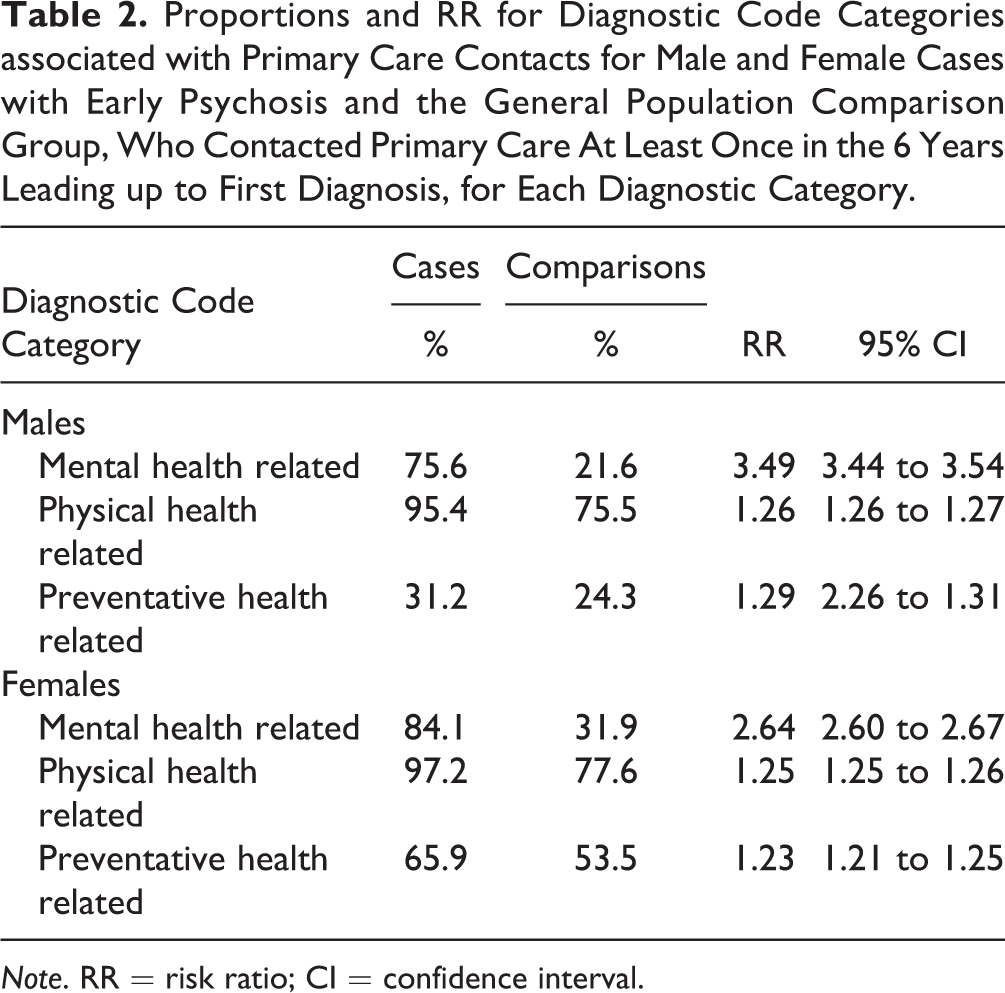
Note. RR = risk ratio; CI = confidence interval.
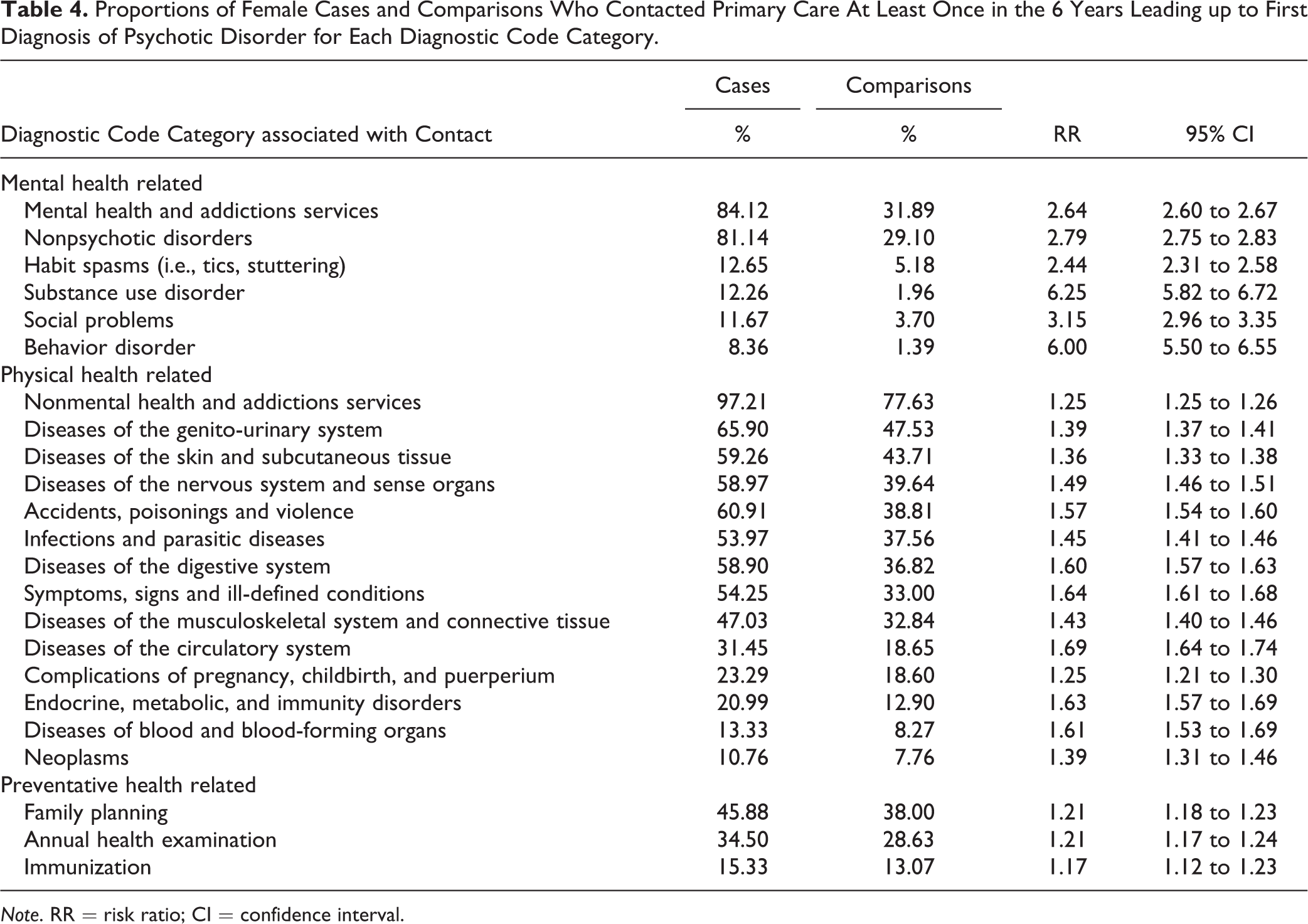
The complete list of the contact prevalence and RR for all diagnostic code categories (where prevalence >5%) is presented in Tables 3 and 4, stratified by sex. Notably, both males and females with early psychosis were over 6 times more likely to contact with a diagnostic code related to substance-use disorder (males: RR = 6.11; 95% CI, 5.84 to 6.40; females: RR = 6.25; 95% CI, 5.82 to 6.72), and over 4 to 6 times more likely to contact with a diagnostic code related to a behavioral disorder (males: RR = 4.23; 95% CI, 4.02 to 4.45; females: RR = 6.00; 95% CI, 5.50 to 6.55), relative to the comparison group.
Proportions of Male Cases and Comparisons Who Contacted Primary Care At Least Once in the 6 Years Leading up to First Diagnosis of Psychotic Disorder for Each Diagnostic Code Category.
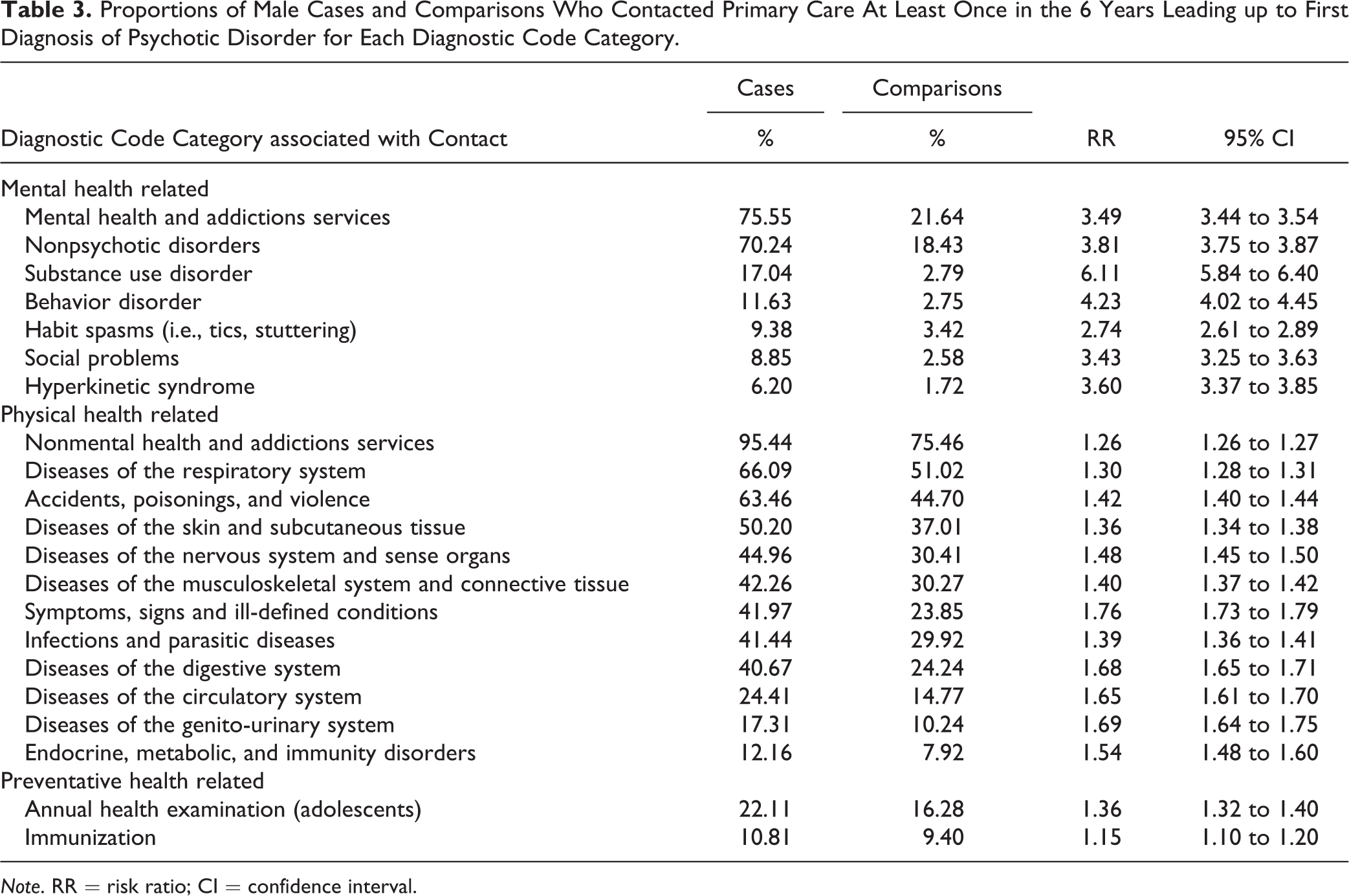
Note. RR = risk ratio; CI = confidence interval.
Proportions of Female Cases and Comparisons Who Contacted Primary Care At Least Once in the 6 Years Leading up to First Diagnosis of Psychotic Disorder for Each Diagnostic Code Category.
Note. RR = risk ratio; CI = confidence interval.
Service Use Profiles
Among people with early psychosis, the number of primary care contacts per year was best fit by a 3-group model with linear, quadratic, and cubic terms. Bayesian Information Criterion for model selection and estimates of trajectory parameters are provided in Online Appendix C, and Online Appendix E shows the trajectory of each group. The first trajectory (n = 23,380; 59% of cases) identified people with low and steady primary care usage (second decile or 1 contact per year) with an increase to almost the third decile (2–4 contacts per year) approximately 1 year before first diagnosis. The second trajectory (n = 13,468; 34% of cases) identified people with medium and steady primary care usage (third decile or 2–4 contacts per year) with an increase to the fourth decile (5–7 contacts per year) approximately 1 year before first diagnosis. The third trajectory (n = 2,601; 7% of cases) identified people with high and increasing primary care usage, beginning at the fifth decile (8–10 contacts per year) at approximately 6 years before first diagnosis and steadily increasing each year to the seventh decile (15–18 contacts per year) at approximately 1 year before first diagnosis. These patterns of low-, medium-, and high-usage were similar for the comparison group (Online Appendix E) although at a lower frequency and without the increase in the final year before the index date. Additionally, the trajectory for the high-use group was not increasing over time in the comparison group.
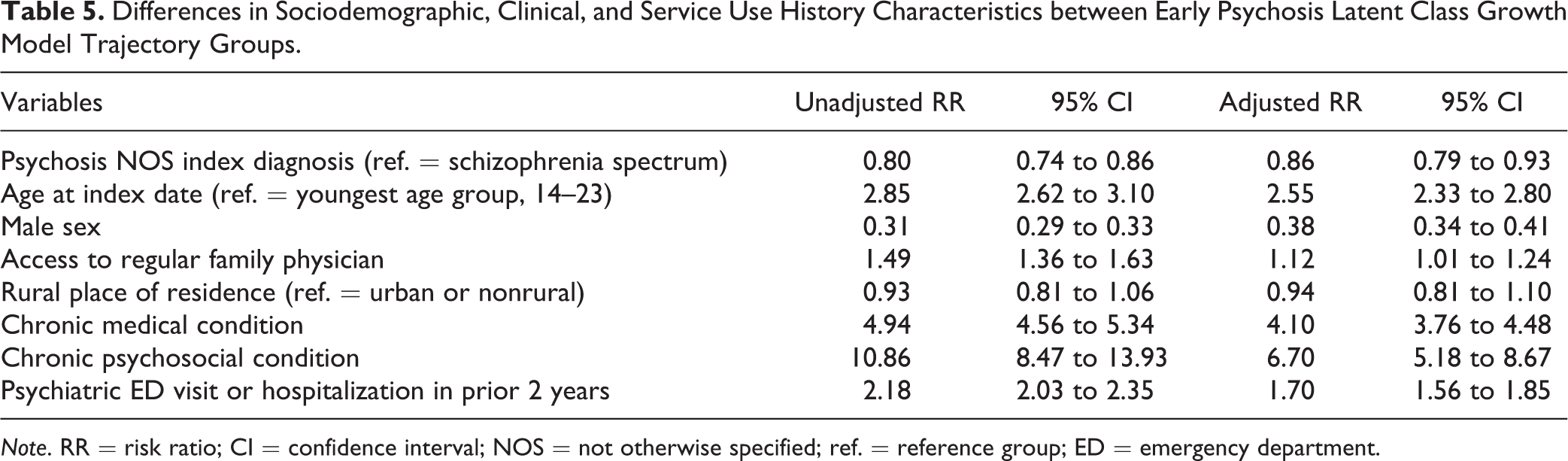
We compared sociodemographic, clinical, and service use history characteristics for the high-increasing trajectory, relative to the other 2 trajectories combined (Table 5). People with early psychosis were more likely to be in the high-increasing-usage trajectory versus the low- and medium-usage trajectories, if they were older (aged 24+; RR = 2.55; 95% CI, 2.33 to 2.80), had a regular family physician (RR = 1.12; 95% CI, 1.01 to 1.24), had a chronic medical condition (RR = 4.10; 95%CI, 3.76 to 4.48), had a chronic psychosocial condition (RR = 6.70; 95% CI, 5.18 to 8.67), or had contact with acute care services in the 2 years prior to diagnosis (RR = 1.70; 95%CI, 1.56 to 1.85). People with early psychosis were less likely to be in the high-increasing-usage trajectory if they were subsequently diagnosed with psychosis NOS (vs. schizophrenia spectrum disorder; RR = 0.86; 95% CI, 0.79 to 0.93) or were male (RR = 0.38; 95% CI, 0.34 to 0.41).
Differences in Sociodemographic, Clinical, and Service Use History Characteristics between Early Psychosis Latent Class Growth Model Trajectory Groups.
Note. RR = risk ratio; CI = confidence interval; NOS = not otherwise specified; ref. = reference group; ED = emergency department.
Discussion
Our findings suggest that people with early psychosis contact primary care at a higher frequency and at an increasing rate, compared to the general population, during the 6 years preceding first diagnosis of a psychotic disorder. Our findings show repeated contacts with primary care prior to first diagnosis, which is consistent with other studies on first-episode psychosis. 24,25,39 It is important to note that this pattern may also be seen prior to first onset for other nonpsychiatric medical conditions. 40 –44
The trends we observed may reflect physician difficulty recognizing and responding to the emerging signs and symptoms of psychosis—including prodromal symptoms—possibly due to nonspecific or changing clinical presentation over time. 45 People with early psychosis use a range of mental health services for a wide array of psychiatric conditions prior to first diagnosis of psychosis, 5,16,46 and this generalized presentation often makes for a complex diagnostic process. 22,47 –50 Additionally, more than 1 consultation may be needed to gather sufficient information to make a diagnosis. 48 –50 Our findings may also suggest that the family physician may be conservative in assigning a diagnosis of psychotic disorder due to the gravity and consequences for the patient. 51 These patterns may also reflect an absence of partnership with early psychosis intervention programs and other mental health services, as family physicians may have difficulty connecting the person with specialized care. 22,47 –50 These findings highlight opportunities for early intervention in the primary care context.
We found that males and females with early psychosis have higher visit frequencies not only for mental health–related diagnostic codes but also for physical and preventive health–related reasons. Previous research suggests that people with early psychosis are often in contact with primary care for both mental health reasons 5,16,46 and somatic reasons 52 during the period before first diagnosis. The heterogeneity in diagnostic codes, including both mental health and physical health–related codes, are expected given the myriad of symptoms seen in prodromal psychosis, and are consistent with other studies using health administrative data to investigate prodromal help-seeking. 5,16 People with schizophrenia often have other physical comorbidities, 53 –59 and schizophrenia is associated with a range of preexisting somatic conditions, including infectious illness, autoimmune diseases, and head injury, 52,60 –65 which may account for the physical health–related contacts that we observed. The higher number of contacts for preventative health–related diagnostic codes may be a result of family physicians practicing opportunistic prevention, where each contact provides an opportunity for the prevention of illness and encouragement of healthy lifestyles, and may involve the provision of additional services beyond the original presenting issue. 66
This study reports 3 trajectories of service use over the 6-year observation period for people with early psychosis: low-, medium-, and high-increasing usage. There is a lack of literature on service use trajectories in psychotic disorders; however, it may be that the trajectories identified are not unique to psychotic disorders and instead may be expected prior to first diagnosis for any serious medical condition.
Limitations
This study is limited by the variables available in the ICES data holdings, and we are missing information on important confounding factors, such as the severity of symptoms, acuity of first presentation, and ethnicity. 67 –71 We are unable to identify primary care visits initiated by parents or other caregivers who play an important role in help-seeking for early psychosis, 72 and the patterns of primary care use may differ based on who initiates contact. The databases also do not have information on the timing of onset of psychotic symptoms, and thus, we cannot decipher between help-seeking for prodromal psychosis or active psychosis, which may confound the patterns observed. The ICES databases were not developed for research purposes, and the diagnostic codes assigned may not accurately represent the reason for contacting primary care, due to under- or overcoding of diagnoses and a lack of diagnostic standardization across professionals. 73,74 Unlike hospital data, physician billings are limited to 1 diagnostic code per contact; therefore, the diagnostic codes used may not provide an accurate description of the reason for the contact with primary care. Furthermore, when multiple contacts occurred on the same day, only the diagnostic code for the first contact was retained.
The algorithm used in this study was validated for chronic schizophrenia, 28 whereas the cases identified had a first onset of psychotic disorder; therefore, the algorithm performance may not be as stated in the original validation article. This study also defined the cohort using nonaffective psychosis, as we are unable to identify people with affective psychoses using health administrative data, and therefore, results do not generalize to all cases of first-episode psychosis. Our findings also cannot be extrapolated to older age groups who may have different patterns of help-seeking in primary care, 75 and our age restriction may have disproportionately excluded women with psychotic disorders who tend to have an older age at onset. 76 The data represent patterns of primary care use for cases of psychotic disorder diagnosed between 2005 and 2015, and ongoing changes to the mental health system in Ontario may have altered these patterns; therefore, updates to these analyses are warranted. Finally, the administrative data used in this study did not capture all contacts with primary care. The databases are missing information from nurse practitioners and salaried physicians (<6% of family physicians) who often provide primary care services in clinics for marginalized populations. Not all people in our sample had access to a regular family physician (72% for cases, 56% for comparison group), so we kept our definition of primary care broad to include walk-in clinics and other settings where family physicians may provide care. Nonetheless, some people may have been forced to turn to other service providers due to lack of access, meaning that help-seeking in primary care for early psychosis could be even higher if all young people had access to a regular family physician.
Conclusions
The patterns of primary care use we observed in this study support the notion that family physicians play an active role on the pathways to care for young people with early psychosis. We need to consider how we can better support family physicians in their role, perhaps through additional training and resource allocation to improve necessary collaborations between primary care and early psychosis intervention programs. Further research on this topic could incorporate information from electronic medical records and prescription databases to further delineate the practice patterns of family physicians treating people with early psychosis. Future research could also explore whether these patterns of service utilization in primary care could be used in risk prediction algorithms to distinguish nonaffective psychotic disorders from other mental health conditions. Increasing the detection of early psychosis in primary care could help reduce the duration of untreated psychosis and improve the social, educational, and professional outcomes in young people with first-episode psychosis.
Supplemental Material
Supplemental Material, FEP_Help-Seeking_in_Primary_Care_-_Appendices_Submission_#2 - Patterns of Primary Care Use Prior to a First Diagnosis of Nonaffective Psychotic Disorder in Ontario, Canada: Modèles d’utilisation des soins de première ligne avant un premier diagnostic de trouble psychotique non affectif en Ontario, Canada
Supplemental Material, FEP_Help-Seeking_in_Primary_Care_-_Appendices_Submission_#2 for Patterns of Primary Care Use Prior to a First Diagnosis of Nonaffective Psychotic Disorder in Ontario, Canada: Modèles d’utilisation des soins de première ligne avant un premier diagnostic de trouble psychotique non affectif en Ontario, Canada by Nicole Schoer, Rebecca Rodrigues, Jennifer Reid, Bridget L. Ryan, Daniel J. Lizotte, Richard Booth, Arlene G. MacDougall, Paul Kurdyak and Kelly K. Anderson in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
The project coinvestigators include Kelly K. Anderson (The University of Western Ontario); Suzanne Archie (McMaster University); Richard G. Booth (The University of Western Ontario); Elisa Candido (ICES); Chiachen Chang (Northern Ontario School of Medicine); Saadia Hameed (The University of Western Ontario); Liisa Jaakkimainen (ICES); Paul Kurdyak (Centre for Addiction and Mental Health); Daniel Lizotte (The University of Western Ontario); Arlene G. MacDougall (The University of Western Ontario); Ross Norman (The University of Western Ontario); Lena Palaniyappan (The University of Western Ontario); Rebecca Rodrigues (The University of Western Ontario); Bridget L. Ryan (The University of Western Ontario); Amanda L. Terry (The University of Western Ontario); Aristotle Voineskos (Centre for Addiction and Mental Health). Parts of this material are based on data and information compiled and provided by the Ontario Ministry of Health and Long-Term Care (MOHLTC), Cancer Care Ontario (CCO), and Canadian Institute for Health Information (CIHI). The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred. The data set from this study will be held securely in coded form at ICES and the ICES analyst will have full access to study data. While data sharing agreements prohibit ICES from making the data set publicly available, access can be granted to those who meet pre-specified criteria for confidential access, available at ![]() . The full dataset creation plan is available from the authors upon request.
. The full dataset creation plan is available from the authors upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The study was completed at the ICES Western site, where core funding is provided by the Academic Medical Organization of Southwestern Ontario, the Schulich School of Medicine and Dentistry, Western University, and the Lawson Health Research Institute. This study also received funding from a project grant from the Canadian Institutes of Health Research (PJT 153022).
Source of Data and Ethics Approval
In 2018, the institute formerly known as the Institute for Clinical Evaluative Sciences formally adopted the initialism ICES as its official name. ICES is a prescribed entity under section 45 of Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 is the provision that enables analysis and compilation of statistical information related to the management, evaluation and monitoring of, allocation of resources to, and planning for the health system. Section 45 authorizes health information custodians to disclose personal health information to a prescribed entity, like ICES, without consent for such purposes. The portions of this protocol that involve health administrative and electronic medical record data do not require review by a Research Ethics Board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.