
Abstract
Objective:
We aimed to investigate whether individuals with first-episode psychosis (FEP) receiving extended early intervention (EI) were less likely to experience suicidal ideation and behaviors than those transferred to regular care after 2 years of EI. Another objective was to examine the 5-year course of suicidality in FEP.
Methods:
We conducted a secondary analysis of a randomized controlled trial where 220 patients were randomized after 2 years of EI to receive extended EI or regular care for the subsequent 3 years. Suicidality was rated using the Brief Psychiatric Rating Scale. Linear mixed model analysis was used to study time and group effects on suicidality.
Results:
Extended EI and regular care groups did not differ on suicidality. There was a small decrease in suicidality over time, F(7, 1038) = 1.84, P = 0.077, with an immediate sharp decline within a month of treatment, followed by stability over the remaining 5 years. Patients who endorsed suicidality at entry (46.6%) had higher baseline positive, negative, and depressive symptoms. The 5-year course fell in 3 groups: never endorsed suicidality (33.9%), endorsed suicidality at low-risk levels (43.1%), and endorsed high-risk levels (23.0%). The high-risk group had a higher proportion of affective versus nonaffective psychosis diagnosis; higher baseline positive and depressive symptoms; higher 5-year mean depression scores, and fewer weeks of positive symptom remission over the 5-year course.
Conclusions:
The first month of treatment is a critical period for suicide risk in FEP. Although early reductions in suicidality are often maintained, our findings make the case for sustained monitoring for suicide risk management.
A meta-analysis of 50 longitudinal studies highlighted psychosis as a risk factor for suicidal ideation, attempts, and death with weighted mean odds ratios of 1.70, 1.36, and 1.40, respectively. 1 The onset of psychosis is a period of elevated vulnerability. A United Kingdom study that followed first-episode psychosis (FEP) individuals for an average of 11.5 years found suicide to be almost 12 times more frequent than in the general population, with the rate being highest in the first year. 2 A large Danish register study found suicide risk to be about 60% higher in the first year after hospitalization than later and to be largest in the younger age groups. 3
An estimated 26% to 46% of FEP 4 -6 individuals report suicidal ideation, which has been found to be predictive of suicidal plans and attempts at 1 and 2 years of follow-up 7 and of suicidal behavior. 7,8
It has been argued that early intervention (EI) services reduce the high risk of suicide but this is not unequivocally backed by trials comparing EI or EI extensions with regular care. The Hong Kong group found that compared to regular care, receiving EI in the initial 2 years was associated with suicide rate reduction over a 12-year period. 9 However, in their extended EI study, patients receiving a third year of EI made no fewer suicidal attempts than those who received EI for 2 years followed by a year’s regular care. 10 In Denmark’s OPUS-I trial, suicidal thoughts, plans, and attempts after 1 and 2 years of follow-up were not different between integrated versus standard treatment groups. 7 OPUS II, which evaluated 5 years of EI versus 2 years of EI followed by 3 years of standard treatment, also found suicidal ideation to not be different between the groups. 11 The U.S.’ Recovery After an Initial Schizophrenia Episode (RAISE) project found early treatment to not have an independent effect on suicidal ideation. 5
Few studies have investigated the trajectories of suicidality in FEP. In a Danish cohort study, suicidal ideation over a 10-year period fell into low-decreasing (61%), frequent-stable (33%), and frequent-increasing (6%) trajectories. Persistent suicidal ideation and suicide attempts were higher in the frequent-stable and frequent-increasing groups, but the groups’ 5- and 10-year suicide rates did not differ. 12
In Canada, there have been only 3 published investigations of suicidality in FEP. In 2004, Addington et al. reported that 15.1% of FEP patients had attempted suicide prior to receiving EI. In the first year after entry, 2.9% attempted suicide and 0.4% died by suicide. The authors attributed these rates that were lower than had been previously reported to the effectiveness of EI. 13 Using administrative data, Anderson et al. 14 in 2018 found mortality rates in the 2 years after admission to be 4 times lower among FEP persons who had received EI than those who had not received EI. However, the groups did not differ on self-harm and suicide rates. A recent study reported a 1.7% rate of suicide deaths within an average of 4.3 years after a first schizophrenia-spectrum diagnosis (N = 75,989). Suicide death was predicted by male sex, suicide attempts, later age at diagnosis, psychiatric hospitalizations before diagnosis, and mood or drug use disorders. 15
Our study aimed to investigate whether individuals receiving extended EI for 5 years were less likely to experience suicidal ideation and behavior compared to those receiving 2 years of EI followed by 3 years of regular care. Although the trial did not include a hypothesis on suicidality, addressing this aim seemed worthwhile given the seriousness of suicidal ideation and behaviors, the controversy around the superior performance of EI in this regard, and its limited investigation in Canada.
Our second aim was to examine the prevalence and longitudinal course of suicidality in FEP over a 5-year period. Based on previous research, 16 we expected a high number of individuals to endorse suicidality at baseline. We investigated whether suicidality significantly decreased over the 5-year course and compared those who endorsed high-risk levels of suicidality, low-risk levels, and no suicidality.
Methods
Design and Sample
This is an open-label single-blind randomized controlled trial (RCT) conducted at 3 similar catchment-area based McGill University-affiliated EI programs, including the Prevention and Early Intervention Program for Psychosis (PEPP). These programs admit patients aged 14 to 35 years who have a nonaffective or affective psychotic disorder, have received antipsychotic medication for less than 1 month, and have an IQ above 70. Case management, medication, and various psychosocial interventions are offered during the first 2 years. 17 While no intervention specifically targets suicidality, clinicians assess the presence of suicidal ideation and address it with needed interventions (e.g., therapy, hospitalization, teaching coping strategies, etc.).
At the end of their initial 2-year follow-up (±3 months), 366 patients were assessed for eligibility for the RCT. A total of 220 patients (178 from PEPP; 42 from the other 2 EI sites) satisfied inclusion criteria and consented to the RCT whereby they either received an extension of the EI service or were transferred to regular care for the next 3 years. Inclusion criteria were the same as for entering the EI services except for restricting the trial to individuals ≥18 years. The randomization and study protocols and characteristics of care are detailed in previous publications. 18,19
In extended EI, case management focused on relapse prevention, treatment adherence, crisis and substance abuse management, and functional recovery was the primary intervention. Psychoeducation, multiple family group therapy, and peer support were offered to families. Cognitive-behavior therapy and individual placement and support were provided when necessary. Regular care comprised primary care (family physicians and/or community health and social service centers) or secondary care (hospital-attached outpatient services where psychiatrists provide care with allied staff). Where patients randomized to regular care would be transferred was decided before randomization based on needs, with complex cases assigned to secondary care.
This report is based on 2 samples: All patients who participated in the RCT (N = 220) to enable a comparison of suicidality between individuals who received EI for 5 years and those who received regular care for 3 years following 2 years of EI. Only PEPP patients who received either extended EI or regular care following EI (N = 178). Of these, baseline “suicidality” item data were missing for 4 individuals, leaving a final sample of 174 for analysis of 5-year suicidality trajectories. The 42 patients from the other sites were excluded because data on their suicidality for the first 2 years of EI were not collected. Of the 178 individuals, 1 individual, who was randomized to regular care, died due to a physical health issue. No other deaths were recorded.
Assessments
Demographic and clinical characteristics were prospectively collected. The Structured Clinical Interview for DSM-IV-TR Axis I disorders 20 was used for diagnosis. Duration of untreated psychosis (DUP) was estimated using the Circumstances of Onset and Relapse Schedule. 21
For the RCT sample (N = 220), suicidality and positive, negative, and depressive symptoms were assessed at randomization at the end of 2 years of EI and at 3-month intervals over the 3-year trial duration (i.e., 13 times). For the PEPP sample (N = 174), these had also been assessed at entry for initial treatment into EI (baseline) and Months 1, 2, 3, 6, 9, 12, 18, and 24 (i.e., 9 times) in the first 2 years prerandomization.
Main outcomes
Suicidal ideation and behavior were rated using the “suicidality” item of the Brief Psychiatric Rating Scale (BPRS), 22 rated on a 1 to 7 scale. Individuals endorsing some level of suicidality are rated “3 Mild” (described as “occasional suicidal thoughts”) or higher. Ratings of “4 Moderate” identify patients who frequently consider suicide but without intent or plan. Ratings of “5 Moderately Severe” describe individuals with a plan or those who make an attempt with low lethality. Ratings of “6 Severe” and “7 Extremely Severe” identify patients who clearly want to kill themselves or who make a potentially highly lethal suicide attempt. Ratings of “1 Not Present” and “2 Very Mild” (described as “occasional feelings of being tired of living”) are given when suicidal ideation or behaviors are absent. For our main analyses examining group and time effects, we used the entire range of scores on this BPRS item. For additional analyses (e.g., comparing those who did and did not endorse suicidality at baseline), we considered scoring ≥3 as endorsing some level of suicidality.
Positive, negative, and depressive symptoms
The Scale for the Assessment of Positive Symptoms (SAPS) 23 total global score (sum of global scores for the hallucinations, delusions, bizarre behavior, and formal thought disorder subscales) and the Scale for the Assessment of Negative Symptoms (SANS) 24 total global score (sum of global scores for the affective flattening/blunting, alogia, apathy, and asociality subscales) were calculated. Positive and negative symptom remission were defined as ratings of ≤2 (mild) on each SAPS and SANS global subscale, respectively. We used the definition of remission that has been the established standard in psychosis research since it was arrived at by consensus by an expert group in 2005. 25
Depression was rated using the BPRS’s “depression” item. 22 For the first 2 years, depression was also rated using the Calgary Depression Scale for Schizophrenia (CDSS) after eliminating the suicidality item. 26 The CDSS was administered in the first 2 years but not in the subsequent 3 years. We therefore could not use the CDSS suicidality item.
Analysis
All statistical tests were 2-tailed, and all analyses were performed using SPSS (version 23) and SAS (version 9.4). A P value of ≤0.05 was considered significant. Descriptive statistics are presented as means, standard deviations (SDs), ranges, and percentages.
Aim 1
To test the effect of time and the difference in suicidality between the experimental (extended EI) and control (regular care) groups, random-intercept multivariable linear mixed model 27 was used. An autoregressive first-order covariance structure was used to account for within-subject correlations of repeated suicidality scores. The mixed model approach allowed the use of all available data (participants with incomplete data were not excluded). This was an intention-to-treat analysis and missing data were not imputed. McNemar test was used to check whether individuals who endorsed suicidality during follow-up were likelier to have endorsed it at randomization.
Aim 2
As above, to accommodate for missing values and within-subject correlations of repeated suicidality scores, linear mixed-model analysis was used to investigate the 5-year longitudinal course of suicidality, that is, to study whether there was a significant decline from PEPP baseline/entry to Year 5.
One-way analysis of variance (ANOVA), Student t-test, and χ2 test were used for group comparisons as necessary. Specifically, we compared individuals who did and did not endorse suicidality at baseline on positive, negative, and depressive symptoms, given that symptoms, particularly positive and depressive, are well-known predictors of suicidality in psychosis. 5,16 We also compared the groups on age of onset, sex, education, DUP, diagnosis, and substance use.
We calculated the number of individuals endorsing “high suicide risk” at some point during their follow-up; those who endorsed suicidality at low-risk levels; and those who never endorsed suicidality. Using Fedyszyn et al.’s 28 recommendation, a score of ≥5 was considered “high suicide risk.” Scores of 3 and 4 were considered low-risk levels (ideation but no plan or attempt) and scores of 1 and 2 “absent” as per the scale’s anchors. These 3 groups were compared on positive and depressive symptoms, guided by previous literature 5,7,16,29 using one-way ANOVAs with Games-Howell post hoc test. We also compared these groups on their length of positive and negative symptom remission, which are well-known outcomes 30 and were the RCTs’ key outcomes, 18 using one-way ANOVAs. Partial eta squared (ηp2) was used to measure effect size where a value of 0.01 was considered small, 0.09 medium, and 0.25 large.
Results
Table 1 lists the RCT sample’s demographic and clinical characteristics. There were no significant differences between the extended EI (n = 110) and regular care (n = 110) samples at the time of randomization. As shown in our primary outcomes paper, 18 fewer individuals dropped out before the 36-month mark in the EI than in the regular care group. The number of observations on the primary outcome measure (the BPRS suicidality item) at each time point is provided in the Supplementary Table 1.
Demographic and Clinical Characteristics at Randomization for the RCT Sample.
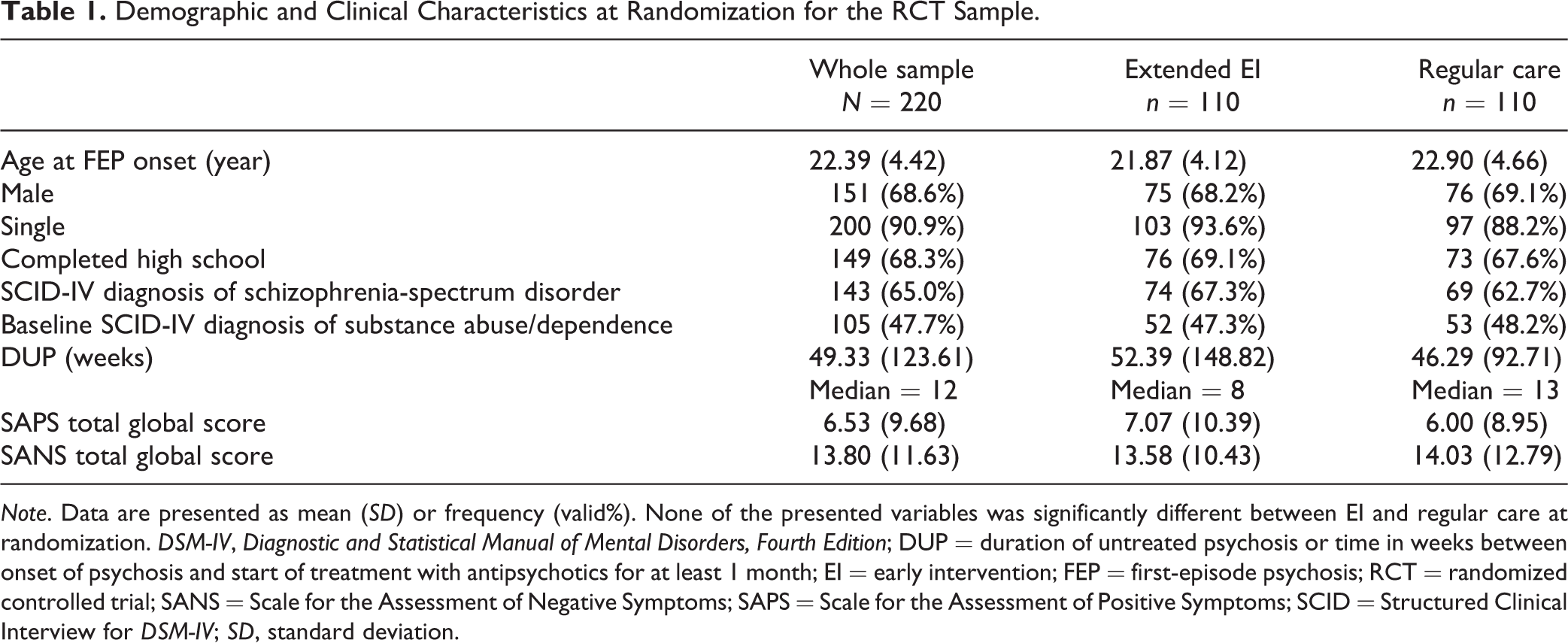
Note. Data are presented as mean (SD) or frequency (valid%). None of the presented variables was significantly different between EI and regular care at randomization. DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; DUP = duration of untreated psychosis or time in weeks between onset of psychosis and start of treatment with antipsychotics for at least 1 month; EI = early intervention; FEP = first-episode psychosis; RCT = randomized controlled trial; SANS = Scale for the Assessment of Negative Symptoms; SAPS = Scale for the Assessment of Positive Symptoms; SCID = Structured Clinical Interview for DSM-IV; SD, standard deviation.
Is there a benefit of extending EI for suicidal ideation and behavior?
The average suicidality score at randomization baseline was 1.32 (SD = 0.84), that is, between “Not Present” and “Very Mild.” At any point between end of Year 2 (randomization baseline) and Year 5, 39.1% (n = 86/220) of patients reported suicidality. The mean suicidality score over the entire period was 1.84 (SD = 0.66). In the mixed model approach, no time, F(12, 1211) = 0.60, P = 0.840; group, F(1, 1211) = 0.43, P = 0.511; or group by time effects, F(12, 1211) = 0.84, P = 0.612, were detected (Figure 1). Suicidality remained stable and generally low over the 3-year period in both arms. Nonetheless, suicidality status at randomization was significantly associated with presence or absence of suicidality during the subsequent 3 years (McNemar test, P < 0.001).
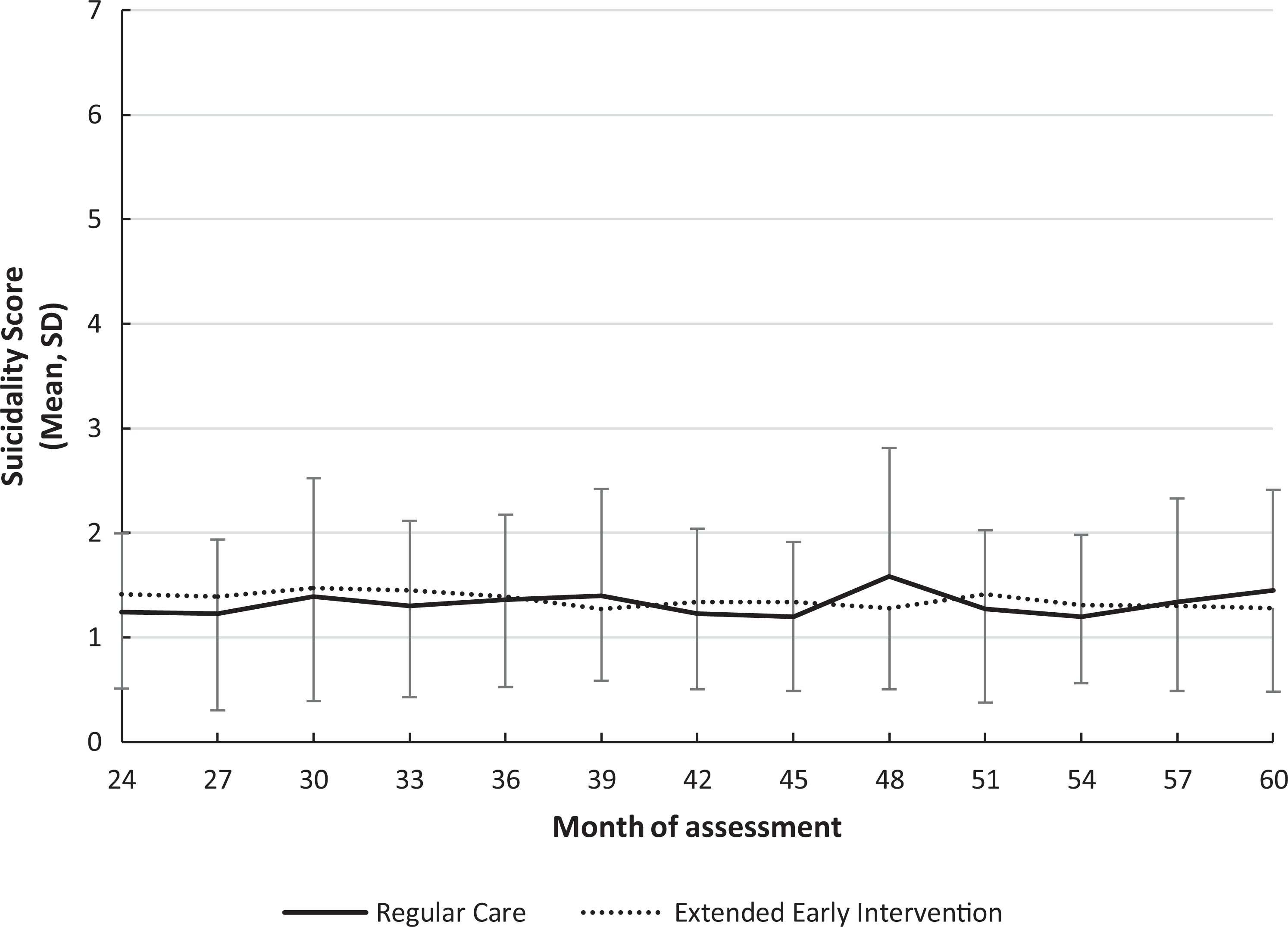
Course of suicidality over 3 years from randomization baseline (Month 24 ± 3 postadmission to early intervention) to Month 60 for the regular care and the extended early intervention groups. Data are based on the suicidality item of the Brief Psychiatric Rating Scale.
What is the 5-year course of suicidality?
Supplementary Table 2 presents the PEPP-only sample’s (N = 174) demographic and clinical characteristics. Suicidality data were available for all individuals at baseline and an average of 71% of individuals at the remaining time points of the 5-year course (range: 46% to 97%), Supplementary Table 1.
The average suicidality score at PEPP entry was 2.40 (SD = 1.58), that is, between “Very Mild” and “Mild,” median = 2 and range = 1 to 7. Linear mixed-model analysis indicated a small decrease in suicidality scores over time; F(7, 1038) = 1.84, P = 0.077 (Figure 2). Means and SDs show important changes in the beginning: an immediate sharp decline within the first month upon treatment being initiated, followed by stability over the remaining 5-year course.
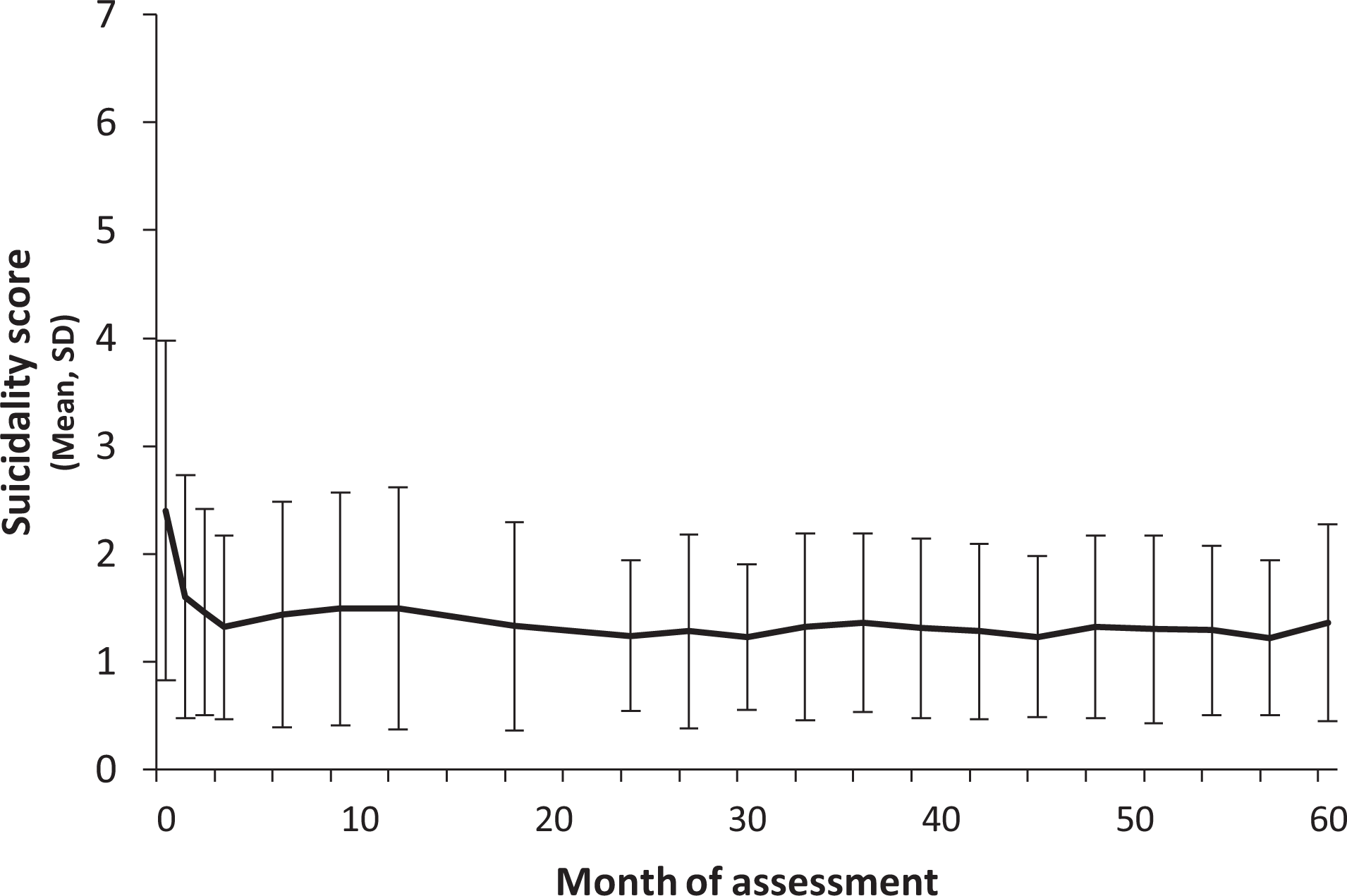
Suicidality over a 5-year period after entry in a sample of first-episode psychosis patients treated in a catchment-based early intervention service (n = 174). Data are based on the suicidality item of the Brief Psychiatric Rating Scale.
Upon entering PEPP, 46.6% of patients (n = 81/174) scored ≥3 on the suicidality item, that is, endorsed some level of suicidality. At baseline, compared to those not endorsing suicidality (n = 93), those who endorsed suicidality had significantly higher levels of positive symptoms, SAPS Total = 32.82 (13.19) versus 39.42 (15.18), respectively, t(172) = 3.070, P = 0.002); negative symptoms, SANS Total = 23.74 (14.77) versus 28.12 (11.95), respectively, t(171) = 2.162, P = 0.032; and depressive symptoms, CDSS Total = 2.61 (2.95) versus 7.00 (4.32), respectively, t(130) = 7.567, P < 0.001; and BPRS depression = 2.81 (1.50) versus 4.48 (1.33), respectively, t(172) = 7.740, P < 0.001. The groups were similar in terms of age of onset, sex, education, DUP, affective versus nonaffective psychosis, and presence of substance use disorder.
At some point along the 5-year period, excluding entry, 52.9% of patients (n = 92/174) reported suicidality. Of these 92 patients, 58 (63.0%) had also endorsed suicidality at entry. Notably, 19.5% of all patients (34/174) did not report suicidality at baseline but went on to endorse it during their follow-up.
Among those who reported suicidality, the average score was 3.71 (SD = 0.78; range: 3 to 6), that is, between “Mild” (occasional suicidal thoughts) and “Moderate” (frequent suicidal thoughts). In all, 23% of patients (40/174) could be considered “high suicide risk” (scoring ≥5) at some point during their follow-up. 28 Only 33.9% (n = 59/174) did not disclose any suicidality at entry or thereafter.
Subgroup analyses
Forty individuals (23.0%) met the “high suicide risk” criterion during their 5-year follow-up and 75 (43.1%) endorsed suicidality without reaching high-risk levels; 59 individuals (33.9%) never endorsed suicidality.
As indicated in Table 2 (see Supplementary Table 3 for post hoc results), the 3 groups differed significantly at baseline and over the course of their follow-up in terms of positive and depressive symptoms. The high-risk group had the highest level of baseline positive and depressive symptoms; and the never-suicidal group had the lowest levels of these symptoms, with the group that endorsed suicidality without reaching high-risk levels falling in between. The same pattern was observable with respect to average scores on depression (excluding baseline) over the 5-year follow-up, with the high-risk group reporting the highest average levels of depression, followed by the groups that endorsed suicidality at low risk and never endorsed suicidality, in that order. The never-suicidal group spent significantly more time in positive symptom remission than the other 2 groups.
Differences Between Groups Varying in Their Course of Suicidality Over a 5-Year Follow-up.
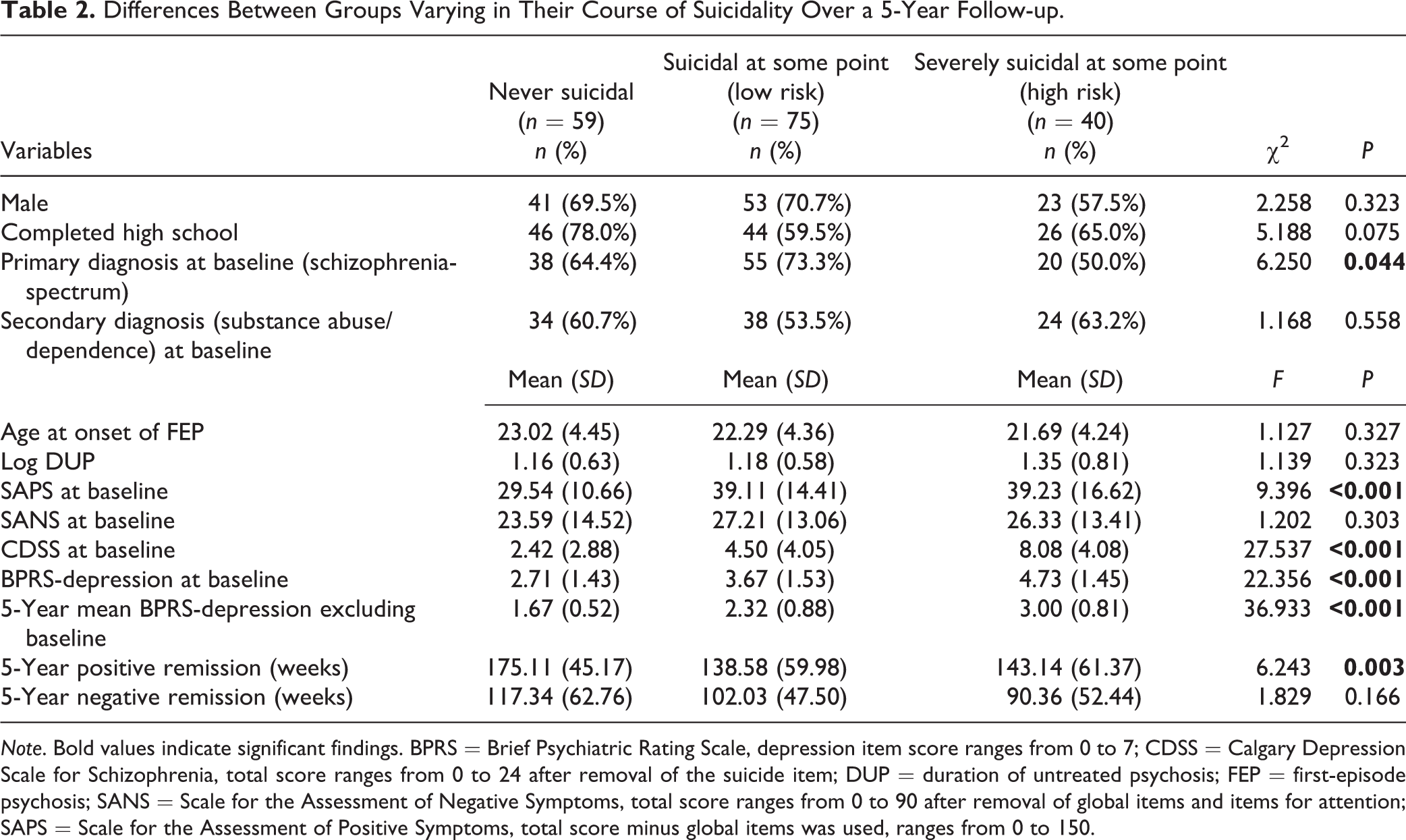
Note. Bold values indicate significant findings. BPRS = Brief Psychiatric Rating Scale, depression item score ranges from 0 to 7; CDSS = Calgary Depression Scale for Schizophrenia, total score ranges from 0 to 24 after removal of the suicide item; DUP = duration of untreated psychosis; FEP = first-episode psychosis; SANS = Scale for the Assessment of Negative Symptoms, total score ranges from 0 to 90 after removal of global items and items for attention; SAPS = Scale for the Assessment of Positive Symptoms, total score minus global items was used, ranges from 0 to 150.
A significantly higher proportion in the high-risk suicidal group had an affective psychosis diagnosis compared to the low-risk group, 50.0% versus 26.7%, respectively, χ2(1) = 6.261, P = 0.012. At baseline, the 3 groups were similar on age of onset, sex, education, DUP, negative symptoms, and presence of substance use diagnosis.
Discussion
With respect to suicidality, we found no benefit to extending EI for 3 years. This is congruent with the other 2 RCTs of extending EI in FEP. 10,11 Post-EI regular care may fare as well as extended EI in reducing suicidal ideation or maintaining it at low levels. Suicidality risk is known to be highest during the first year after onset. 2,31,32 Receiving EI early on may rapidly reduce suicidality such that it remains low regardless of the subsequent model of care (regular or EI). In our study, the prevalence of suicidality reduced significantly within a month of treatment and remained relatively low throughout the 5-year course. An Australian FEP study similarly reported that suicidality was highest in the first month of EI and decreased rapidly over the next 6 months. 28 Similarly, in OPUS-I, the majority (61%) of patients experienced a decreasing trajectory. 12
Consistent with previous EI literature, 6,33 about half of our sample endorsed some level of suicidality upon entering EI. Suicidal ideation remained higher during follow-up among those who experienced it at the point of randomization; 63% of those who experienced suicidality during their 5-year follow-up also endorsed it at entry. This aligns with evidence for the strongest predictors for suicidal plans and attempts being prior suicidal ideation and attempts. 7 Individuals entering EI with suicidality may therefore need attention to mitigate their increased suicidality risk. However, about a fifth of patients endorsing suicidality during follow-up had not had it upon entry. Further, 23% of patients rated as high-risk at some point during their follow-up. 28 Our results thus underline the need for the sustained monitoring of suicidal ideation and behavior throughout treatment. Earlier, in 2010, Dutta et al. 2 advocated for continuous vigilance by highlighting that even 10 years after FEP, suicide risk remained about 4 times higher than the general population. In 2016, Madsen et al. concurred based on their OPUS-I findings that frequent suicidal ideation persisted in 33% of patients and increased in 6% during the first 3 years of treatment. 12
Consistent with previous literature, 16 our findings suggest that early in FEP, suicidality may be associated with acute psychotic symptoms and the attendant distress and depressive symptoms. Our results and previous studies suggest that treatment very effectively reduces this high early prevalence of suicidality. This early reduction may result from patients feeling supported upon treatment being initiated in hope-inducing EI services, often after long periods of distress and confusion. 34,35 The rapid positive symptom remission that ensues may also contribute to reduction in suicidality. In fact, Bornheimer et al. in 2019 found a dose–response relationship between the severity of hallucinations and delusions at treatment onset and the odds of further suicidal ideation. 5
Our findings highlight that affective symptoms like depression are associated with the presence and severity of suicidality, suggesting that suicide management must integrate tailored interventions targeting depression, self-esteem, and so on. 16 That our high-risk group was characterized by higher presence of depressive symptoms, and affective psychosis diagnosis is thematically consistent with a recent Canadian study highlighting mood disorders as a risk factor for suicide death. 15 It included only patients with schizophrenia-spectrum/nonaffective psychosis, unlike our study which permitted a comparison of patients with affective and nonaffective psychosis.
Patients who expressed concerningly high levels of suicidality also spent less time in positive symptom remission during the 5-year follow-up. It may be that not attaining and sustaining symptom improvement contributes to suicidality, or that there is a patient subgroup characterized by both difficulties attaining positive symptom remission and higher levels of suicidality and depression. Future research should investigate temporal associations between suicidality and symptom remission given their treatment implications (e.g., targeting sustained positive symptom remission to reduce suicidality or offering intensive follow-up for those expressing suicidality for better symptom outcomes).
Although suicide risk is known to be high among persons with schizophrenia and related psychotic disorders, 36,37 there were no deaths by suicide in our sample over 5 years. Repeated assessment using a standardized tool may itself have contributed to the early identification and appropriate management of suicide risk. This resonates with prior research demonstrating that an intervention wherein postcards were sent regularly following discharge to individuals who had been hospitalized for self-poisoning reduced future self-poisoning events and psychiatric admissions. 38 The value of regular monitoring and measurement-based care for reducing suicidality merits further investigation. Our finding is also consistent with prior research showing that EI may protect against suicide while in treatment and for a limited period afterward. 39
Our study has limitations including a relatively small sample size with more individuals dropping out from the RCT’s regular care arm. Investigating suicidality was not our RCT’s primary objective. We therefore did not collect information on pretreatment suicide attempts. We also did not use a specific suicidality measure, relying instead on a BPRS item. Further, because the CDSS was only administered in the first 2 years, we could not take advantage of its suicidality item or use its “hopelessness” item for a richer interpretation of the results. Nonetheless, our study yielded valuable insights about suicidality in the early course of psychosis and raises questions (e.g., what explains the association between symptom remission and suicidality?) that can be better unpacked with larger sample sizes and mixed methods approaches.
Supplemental Material
3_Supplementary_Tables_minor_changes_22_Sep_2020 - Suicidality Over the First 5 Years of Psychosis: Does Extending Early Intervention Have Benefits? Suicidabilité dans les cinq premières années d’une psychose: Prolonger une intervention précoce a-t-il des avantages?
3_Supplementary_Tables_minor_changes_22_Sep_2020 for Suicidality Over the First 5 Years of Psychosis: Does Extending Early Intervention Have Benefits? Suicidabilité dans les cinq premières années d’une psychose: Prolonger une intervention précoce a-t-il des avantages? by Srividya N. Iyer, Sally S. Mustafa, Laura Moro, G. Eric Jarvis, Ridha Joober, Sherezad Abadi, Nicola Casacalenda, Howard C. Margolese, Amal Abdel-Baki, Martin Lepage and Ashok Malla in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Malla reports honoraria for lectures delivered at conferences sponsored by Otsuka and Lundbeck, Canada and Global; and consulting activities with Otsuka and Lundbeck. Dr Joober reports to be a speaker and/or consulting committee member for Pfizer, Janssen, BMS, Sunovian, Myelin, Otsuka, Lundbeck, Shire, and Perdue; and to have received grants from Janssen, BMS, Otsuka, Lundbeck, Astra Zeneca, and HLS’ and to have royalties from Henry Stewart talks. Dr Lepage reports grants from Otsuka Lundbeck Alliance and Janssen and personal fees from Otsuka Canada, Lundbeck Canada, Janssen, MedAvante-Prophase, and Amplexor. Dr Margolese reports to be a paid speaker and/or consulting committee member and/or to have received honoraria from HLS Therapeutics, Janssen, Lundbeck, Mylan, Otsuka, Pfizer, Shire, Sunovion; and research support from Acadia, Amgen, Lundbeck, Janssen, and SyneuRx. All mentioned conflicts of interest are unrelated to the present article. The authors Iyer, Mustafa, Moro, Jarvis, Abadi, Casacalenda, and Abdel-Baki have no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The RCT part of this study was supported by an operational grant from the Canadian Institutes of Health Research (CIHR) (grant MCT 94189; registration CCT-NAPN-18590). The data for the first 2 years were collected as part of a longitudinal project on outcomes in FEP. This longitudinal project was supported by a combination of grants from the National Institute of Mental Health (MH093303), CIHR, CIHR New Investigator Award (Iyer), Fonds de Recherche du Québec—Santé (FRQS) Clinician-Scientist Award (Iyer and Joober), FRQS Research Chair award (Lepage), and the Canada Research Chairs Program (Malla). The funding agencies had no role in the conduct and publication of the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.