
Abstract
Objective:
To examine the association between usual place of primary care and mental health consultation among those with self-reported mood or anxiety disorders. We also describe access to mental health services among people who are recent immigrants, longer-term immigrants, and nonimmigrants and determine whether the association with place of primary care differs by immigration group.
Methods:
We used data from the Canadian Community Health Survey (2015 to 2016) to identify a representative sample of individuals with self-reported mood or anxiety disorders. We used logistic regression, with models stratified by immigration group (recent, longer-term, nonimmigrant), to examine the association between usual place of primary care and receiving a mental health consultation in the previous 12 months.
Results:
Higher percentages of recent and longer-term immigrants see a doctor in solo practice, and a higher percentage of recent immigrants use walk-in clinics as a usual place of care. Compared with people whose usual place of care was a community health center or interdisciplinary team, adjusted odds of a mental health consultation were significantly lower for people whose usual place of care was a solo practice doctor’s office (AOR = 0.71; 95% CI, 0.62 to 0.82), a walk-in clinic (AOR = 0.75; 95% CI, 0.66 to 0.85), outpatient clinic/other place (AOR = 0.72 95% CI, 0.59 to 0.88), and lowest among people reporting no usual place other than the emergency room (AOR = 0.59; 95% CI, 0.51 to 0.67). Differences in access to mental health consultations by usual place of primary care were greatest among immigrants, especially recent immigrants.
Conclusions:
People with mood or anxiety disorders who have access to team-based primary care are more likely to report mental health consultations, and this is especially true for immigrants. Expanded access to team-based primary health care may help reduce barriers to mental health services, especially among immigrants.
Introduction
Mood and anxiety disorders affect 1 in 10 Canadians aged 18 years and older and can have a major impact on basic activities and ability to work. 1 Almost one quarter of Canadians with mood or anxiety disorders report that they did not access mental health services within the previous 12 months. 2 Immigrants to Canada and members of racialized communities may be even less likely to access mental health services 3 –8 and may experience barriers including cost, language, culturally inappropriate services, lack of awareness of services, and transportation issues. 9 –16
In Canada, most people with anxiety and depression access services through primary care, 17,18 and primary care plays a gatekeeping role in accessing specialized mental health services. 19,20 A strong, accessible system of primary care may improve access to mental health services, especially for recent immigrants, while gaps in primary care may further exacerbate challenges in accessing mental health services. Evidence suggests that patterns of primary care service use differ between immigrants and nonimmigrants in Canada. 4,7,21,22 Immigrants report unmet care needs and may underuse health care services due to not knowing where to access health care services, the perception that they would receive inadequate care, transportation barriers, and language barriers. 23 Immigrants are also less likely to have a regular doctor 24 and more likely to visit urgent care or walk-in clinics or emergency departments for care. 25 Furthermore, emergency departments may be viewed as a more convenient place of care, 26 and immigrant children appear more likely to receive mental health care for the first time in the emergency department. 21 Team-based primary care models, including community health centers (CHCs), may offer better access to mental health services through co-location of specialized mental health providers, greater capacity for referral and coordination of care, and better supports for primary care providers to manage common mental disorders. 22,25,27
The primary objective of this study is to explore the association between usual place of primary care and mental health consultation among those with self-reported mood or anxiety disorders. Secondary objectives are to describe access to mental health services among recent immigrants, longer-term immigrants, and nonimmigrants and determine whether the association with usual place of primary care differs among immigration groups. As primary care services are often the first point of contact for users of specialized mental health care, 17 –20 we hypothesized that primary care would impact access to mental health consultations and that this relationship would differ by immigration group.
Methods
Data Source: Canadian Community Health Survey (CCHS)
We use data from the 2015 and 2016 CCHS. Statistics Canada conducts this survey annually to gather health-related data about the Canadian population over the age of 12 in all provinces and territories. It is a representative sample of 98% of the Canadian population living in private dwellings, excluding people living on reserves and in other Aboriginal settlements, full-time members of the Canadian Forces, and institutionalized populations. To remove language as a barrier to conducting interviews, Statistics Canada recruited interviewers with a wide range of language competencies. When necessary, cases were transferred to an interviewer with the language competency needed to complete an interview. The complete description of the CCHS methodology including weighting can be found elsewhere. 28 All data in this analysis used CCHS data and which were accessed through the 2015 to 2016 Public Use Microdata File.
Ethics Approval and Declaration of Consent
This study used publicly available CCHS data and did not require institutional ethics review. 29
Sample Population
All analyses were completed using the pooled CCHS 2015 and 2016 survey cycles that generated a total of 109,659 respondents. We restricted the sample to 14,378 respondents who reported having been previously diagnosed with a mood or anxiety disorder. Respondents were identified as having a previous diagnosis for a mood or anxiety disorder if they said “yes” to either or both of the following questions: “Do you have a mood disorder such as depression, bipolar disorder, mania, or dysthymia?” 30 or “Do you have an anxiety disorder such as a phobia, obsessive-compulsive disorder, or a panic disorder?” 30
Outcome
Our primary response variable, having a mental health consultation, was assessed based on a dichotomous survey question. Respondents were classified as having consulted with a mental health professional if they answered “yes” to the question: “In the past 12 months, that is, from (date 1 year ago) to yesterday, have you seen or talked to a health professional about your emotional or mental health?” 30
We also describe total number of consultations received over the 12-month period and the type of health care provider seen based on the numbered value respondents provided to the question: “How many times in the past 12 months (have you seen or talked to a health professional about your emotional or mental health)?” and the follow-up question: “Whom did you see or talk to?” We describe mental health services (number of mental health consultations and type of providers seen for mental health consultations) by place of primary care, and immigration group, but these are not included in regression analyses.
Exposure
Access to primary care was measured based on self-reported usual place of care. We grouped respondents into those whose usual place of care was a CHC or interdisciplinary team of health care providers, a doctor’s office with solo practice, a doctor’s office with several doctors working independently, a walk-in clinic, a hospital outpatient clinic or some other place, and respondents who had no usual place other than the emergency room (ER). Some other place was defined as any other place that was used to seek care but was not included in the aforementioned list. We combined hospital outpatient clinic and some other place because of the small numbers for each.
Covariates
We identified factors that may shape both use of primary care and mental health services based on previous literature. In addition to place of primary care and immigration group, we included gender, age, racialized status, marital status, socioeconomic status, education, and self-rated mental health in all models.
The CCHS asks whether respondents are male or female. Based on the question’s design, it is not possible to distinguish between sex assigned at birth and gender identity, though we believe that gender identity and expression more plausibly shape access to mental health services. 31 We describe this variable as gender. The CCHS Public Use Microdata File excludes data on Aboriginal identity and categorizes race as White and other racial origin. 32 Racialized communities may experience race-related structural challenges such as discrimination and racism when accessing health services. 33 –35 We describe this variable as racialized status. We also included variables measuring age, total household income from all sources, education, social support, and self-reported mental health.
Immigration is classified into 3 groups based on length of time since arriving in Canada: “recent immigrant’” describes those who became a landed immigrant or permanent resident 0 to 9 years ago, “longer-term immigrant” describes those who became a landed immigrant or permanent resident 10 or more years ago, and “nonimmigrant” describes those who were born in Canada.” 30
Statistical Analysis
We calculated frequencies (unweighted) and percentages (weighted using sample weights provided by Statistics Canada) of all variables, stratified by immigration group. We performed univariable logistic regression to measure the magnitude of the unadjusted association between mental health consultations and all covariates. We then performed multivariable logistic regression to determine whether differences in mental health consultations between recent immigrants, longer-term immigrants, and nonimmigrants persist, adjusting for covariates. Finally, we determine whether the relationship between access to primary care and mental health service use differs by immigration group by running stratified multivariable models. We report odds ratios (ORs) and associated 95% confidence intervals (95% CIs). All statistical analyses were completed using SAS 9.4.
Results
Only 14,378 respondents with mood or anxiety disorders were included in the analysis (Table 1). Of these, 17.19% reported their usual place of primary care was a CHC or an office with interdisciplinary team, 13.75% a doctor’s office with solo practice, 23.83% an office with multiple doctors working independently, 23.81% a walk-in clinic, 4.80% outpatient clinic or some other place, and 16.61% reported no usual place other than ER. The percentage of recent immigrants whose usual place of care was a CHC or an interdisciplinary team was 11.52% compared with 16.47% among longer-term immigrants and 17.46% nonimmigrants. Higher percentages of immigrants reported a doctor’s office with solo practice was their usual place of care (20.31% recent and 21.21% longer-term compared with 12.56% nonimmigrant), and almost a third of recent immigrants (30.17%) reported their usual place of care was a walk-in clinic. A higher percentage of respondents reporting male gender reported they had no usual place other than ER (44.82%). Respondents who identify walk-in clinics as their usual place of care tended to be younger (23.78%, age 12 to 24; 40.22% age 25 to 44). The percentage of people who are racialized in Canada was higher among people who report a doctor’s office with solo practice (18.60%) and walk-in clinic (15.28%) as their usual place of care. The percentages of respondents with household income less than $40k and less than secondary education were highest for outpatient clinic or some other place (42.39%, 30.20%) and no usual place other than ER (40.03%, 27.05%). Higher percentages of respondents with poor or fair self-rated mental health had no usual place of care other than ER (35.39%).
Descriptive Characteristics and Health Service Use Patterns (Unweighted Counts and Weighted Percentages) of the Analytic Sample: Respondents with Self-reported Mood or Anxiety Disorders, Stratified by Usual Place of Care, CCHS 2015/2016.
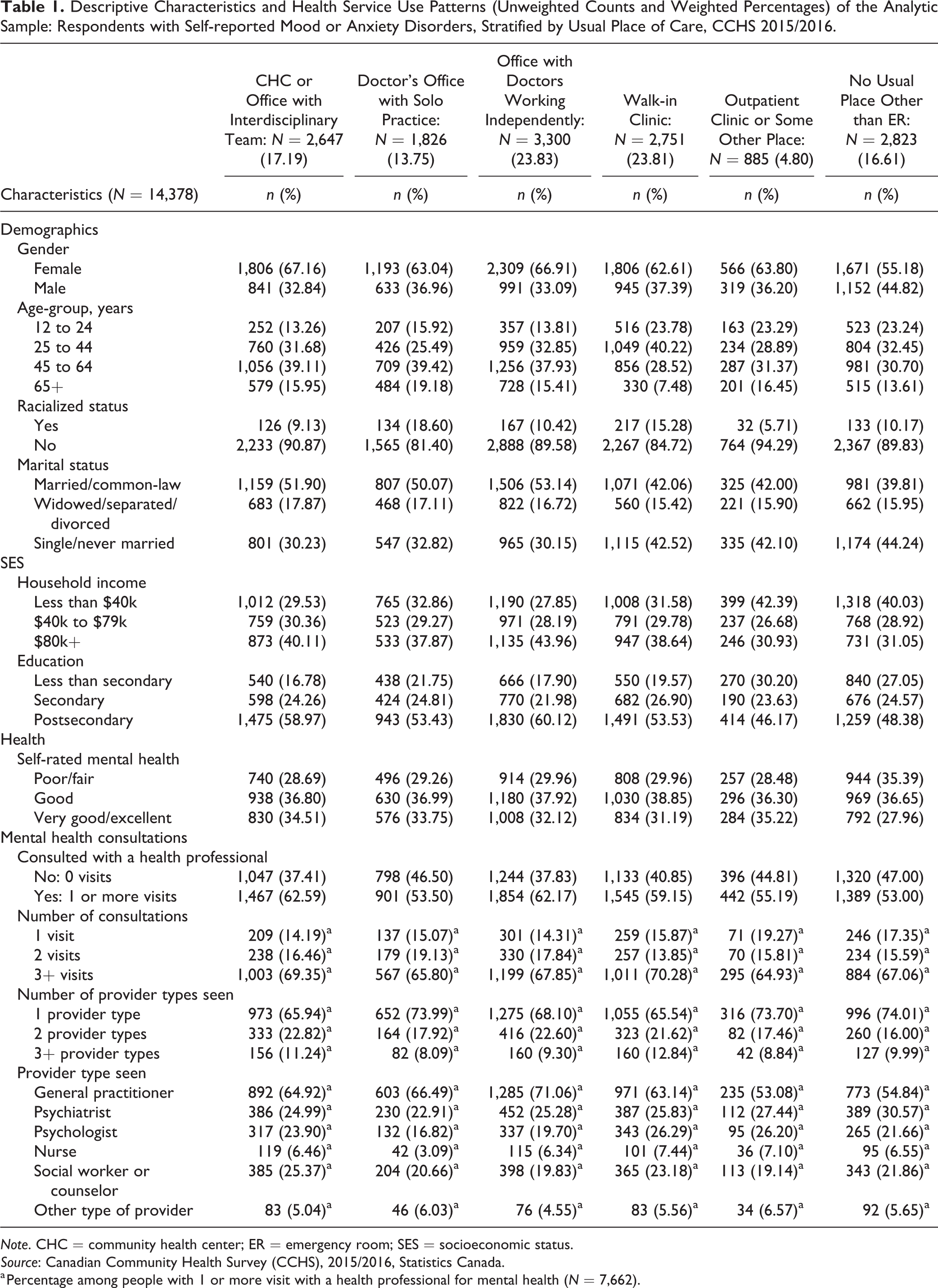
Note. CHC = community health center; ER = emergency room; SES = socioeconomic status.
Source: Canadian Community Health Survey (CCHS), 2015/2016, Statistics Canada.
a Percentage among people with 1 or more visit with a health professional for mental health (N = 7,662).
The percentage of people with mood and/or anxiety disorders who had not consulted with a health professional within the past 12 months was highest among those whose usual place of care was no usual place other than ER (47.00%) followed by doctor’s office with solo practice (46.50%) and outpatient clinic or some other place (44.81%; Table 1). Among people who had at least 1 mental health consultation, percentages of having 3+ visits were highest if their usual place of care was a walk-in clinic (70.28%) and CHC or an office with interdisciplinary team (69.35%). Similarly, people who reported walk-in clinics (12.84%) and CHC or office with interdisciplinary team (11.24%) as their usual place of care had higher percentages of seeing 3 or more types of health provider. Among those whose usual place of care was an office with doctors working independently, higher percentages saw a general practitioner (71.06%) followed by a psychiatrist (25.28%) and social worker or counselor (19.83%). People were less likely to see psychiatrists (22.91%), psychologists (16.82%), and nurses (3.09%) for mental health consultations if their usual place of care was doctor’s office with solo practice. Higher percentages of respondents reported seeing social workers or counselors if their usual place of care was a CHC or an office with interdisciplinary team (25.37%).
The percentage of respondents reporting female gender was similar across immigration groups (63.21% to 64.10%). Longer-term immigrants were older (28.67%; age 65+) than recent immigrants (6.12%; age 65+) and nonimmigrants (12.25%; age 65+; Table 2). Higher percentages of immigrants were non-White (55.43% to 59.70% vs. 4.40%). More than half of immigrants (53.97% recent, 54.80% longer-term) were married compared with 45.76% among nonimmigrants; 46.51% of recent immigrants had a household income less than $40k compared to 28.93% among longer-term immigrants and 32.56% among nonimmigrants. Almost two thirds of immigrants had postsecondary education (62.32% recent, 64.30% longer-term) compared with 53.17% among nonimmigrants. A lower percentage of recent immigrants reported poor or fair self-rated mental health (23.03%) compared with longer-term immigrants (33.23%) and nonimmigrants (30.27%).
Descriptive Characteristics and Health Service Use Patterns (Unweighted Counts and Weighted Percentages) of the Analytic Sample: Respondents with Self-reported Mood or Anxiety Disorders, Stratified by Immigration, CCHS 2015/2016.
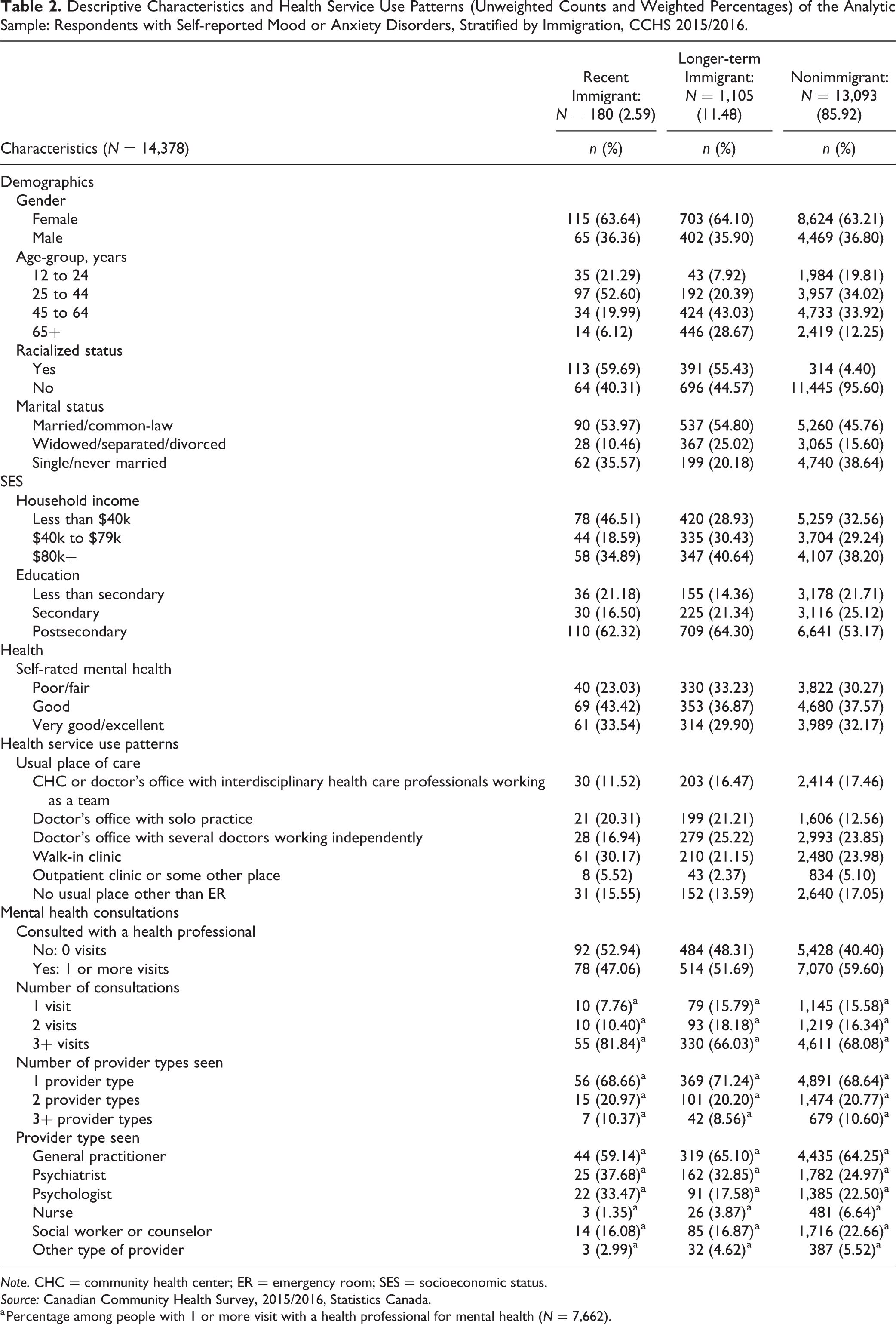
Note. CHC = community health center; ER = emergency room; SES = socioeconomic status.
Source: Canadian Community Health Survey, 2015/2016, Statistics Canada.
a Percentage among people with 1 or more visit with a health professional for mental health (N = 7,662).
The percentage of people with mood and/or anxiety disorders who had not consulted with a health professional within the past 12 months was highest among recent immigrants (52.94%) followed by longer-term immigrants (48.31%) and then nonimmigrants (40.40%; Table 2). Among people who had at least 1 mental health consultation, a higher percentage of recent immigrants (81.84%) had 3+ visits compared to longer-term immigrants (66.03%) and nonimmigrants (68.08%). The percentages of people who saw 1, 2, or 3+ types of health providers for at least 1 mental health consultation were similar across all immigration groups. Slightly lower percentages of recent immigrants received mental health consultations from general practitioners (59.14% recent) compared with longer-term immigrants (65.10%) and nonimmigrants (64.25%). Slightly higher percentages of immigrants saw psychiatrists (37.68% recent, 32.85% longer-term) compared with nonimmigrants (24.97%).
Odds of a mental health consultation were lower among recent and longer-term immigrants compared to nonimmigrants in both unadjusted and adjusted models (AOR = 0.64, 95% CI, 0.50 to 0.83 recent; AOR = 0.86, 95% CI, 0.74 to 1.00 longer-term; Table 3). Compared with people whose usual place of care was a CHC or an interdisciplinary team, adjusted odds of a mental health consultation were significantly lower for people whose usual place of care was a solo practice doctor’s office (AOR = 0.71, 95% CI, 0.62 to 0.82), doctors office walk-in clinic (AOR = 0.75, 95% CI, 0.66 to 0.85), outpatient clinic or some other place (AOR = 0.72, 95% CI, 0.59 to 0.88), and lowest among people reporting no usual place other than ER (AOR = 0.59, 95% CI, 0.51 to 0.67). Odds were higher among females (AOR = 1.53, 95% CI, 1.41 to 1.66) and lower among older age groups (45 to 64 years old AOR = 0.63, 95% CI, 0.57 to 0.70 and 65+ year old AOR = 0.28, 95% CI, 0.24 to 0.32), racialized people (AOR = 0.73, 95% CI, 0.63 to 0.85), people in lower-income groups (AOR = 0.83, 95% CI, 0.75 to 0.91), and people without postsecondary education (AOR = 0.84, 95% CI, 0.76 to 0.92). Odds of consultation corresponded to self-rated mental health, with people reporting poor or fair self-rated mental having highest odds of mental health consultation (AOR = 5.53, 95% CI, 4.97 to 6.15).
Unadjusted and Adjusted Odds (Weighted) of Seeing a Health Professional for a Mental Health Consultation.
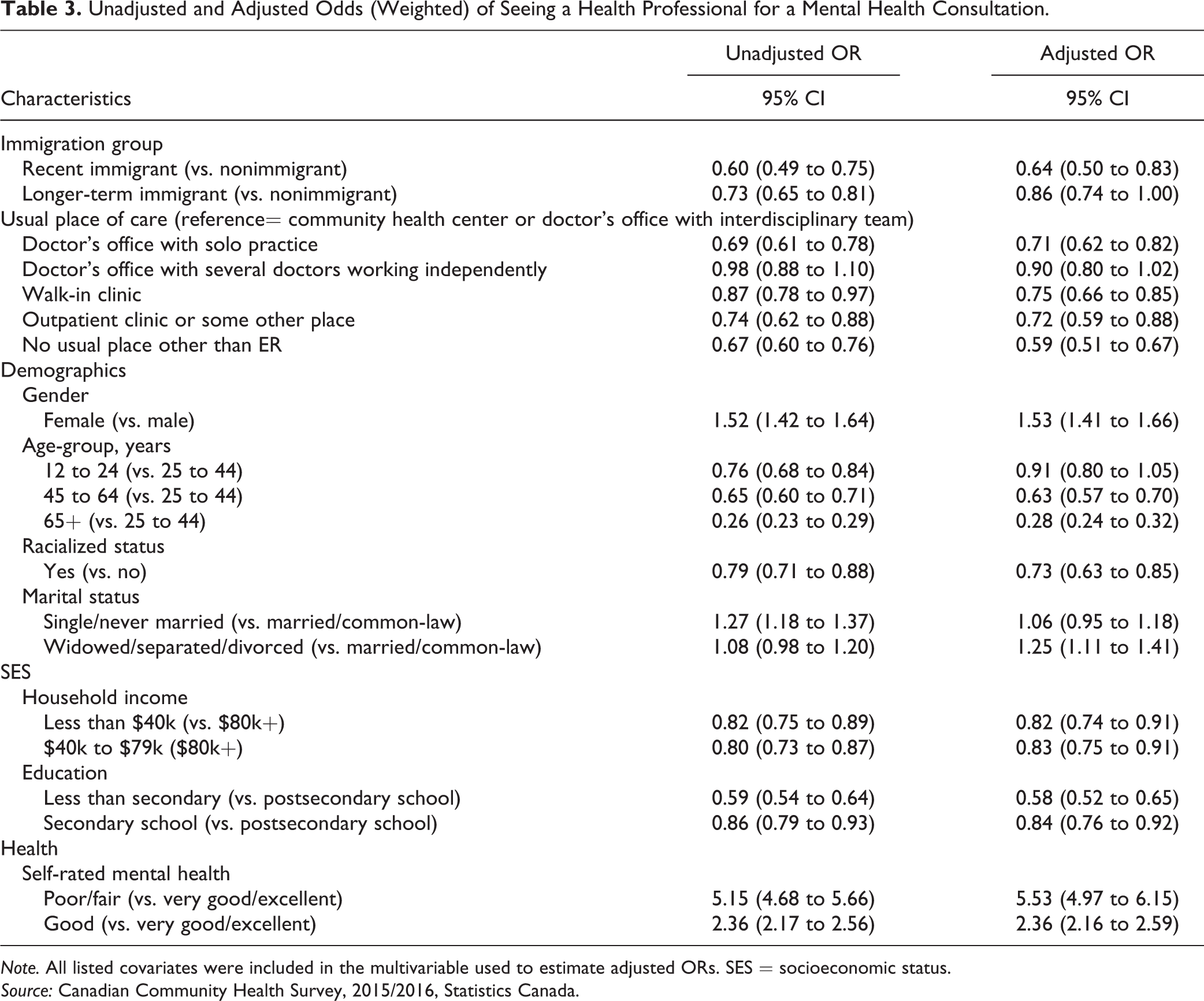
Note. All listed covariates were included in the multivariable used to estimate adjusted ORs. SES = socioeconomic status.
Source: Canadian Community Health Survey, 2015/2016, Statistics Canada.
Models stratified by immigration groups (Table 4) reveal that magnitude of the association with usual place of care differs by immigration groups. People whose usual place of care was a doctor’s office with solo practice had lower odds of a mental health consultations relative to CHCs/interdisciplinary team overall, but the magnitude of this association was greatest for recent immigrants (AOR = 0.25, 95% CI, 0.08 to 0.74) followed by longer-term immigrants (AOR = 0.55, 95% CI, 0.37 to 0.82) and then nonimmigrants (AOR = 0.79, 95% CI, 0.67 to 0.92). Similarly, among people with no usual place other than an ER, the AOR was 0.13 (95% CI, 0.04 to 0.45) among recent immigrants, followed by 0.33 (95% CI, 0.21 to 0.53) among longer-term immigrants, and 0.64 (95% CI, 0.55 to 0.75) among nonimmigrants.
Adjusted Odds of Seeing a Health Professional for a Mental Health Consultation, Stratified by Immigration Group.
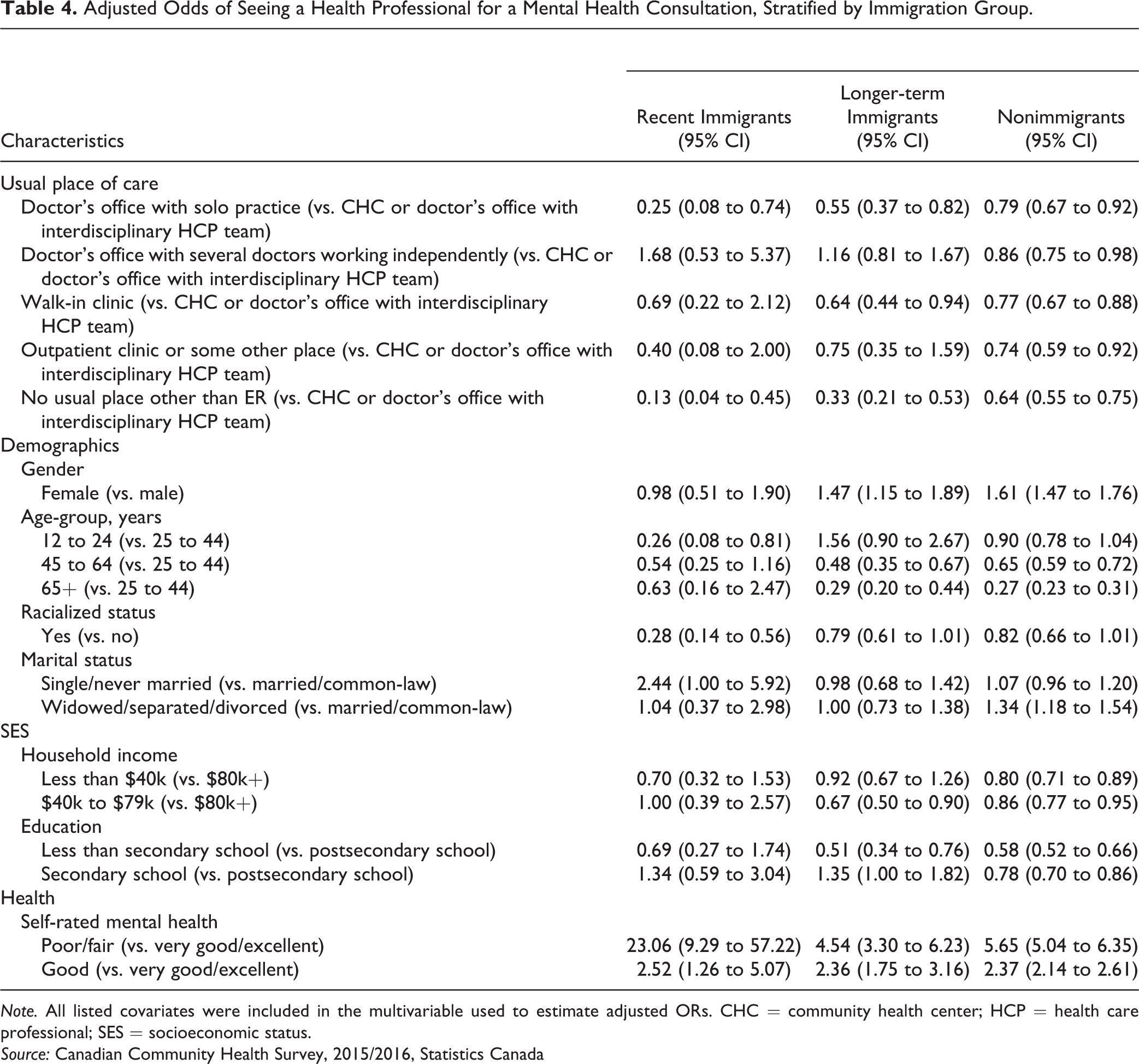
Note. All listed covariates were included in the multivariable used to estimate adjusted ORs. CHC = community health center; HCP = health care professional; SES = socioeconomic status.
Source: Canadian Community Health Survey, 2015/2016, Statistics Canada
Discussion
Our findings confirm that there is a gap in access to mental health services among immigrants with mood and/or anxiety disorders compared to nonimmigrants. Even in fully adjusted models, recent and longer-term immigrants were less likely to have a mental health consultation compared with nonimmigrants (Table 1). While multiple variables are associated with having reported a mental health consultation, people with access to team-based primary care are more likely to report mental health consultations, and this is especially true for immigrants. Unfortunately, immigrants, and especially recent immigrants, are more likely to receive primary care from a solo practice or walk-in clinic.
Our finding of a gap in health service use among immigrants with diagnosed mental health disorders is consistent with previous studies. 16,18 –21,23 –26 Gaps in health insurance coverage may impact access to services and influence future use and interactions with the Canadian health system. 36,37 Many provinces have a 3-month waiting period before new, landed immigrants are eligible for provincial health coverage 38 causing delays in seeking or accessing health services. 22,39 –41
Findings are likely shaped by what services are publicly covered, as family doctor and psychiatrist services are available free of charge for individuals with provincial insurance in all provinces, but services from clinical counsellors, psychologists, or social workers may be more accessible through team-based primary care. This may also explain our observation that among people who received consultations, the percentage of people who saw a psychiatrist was highest among recent immigrants. Models of integrated care teams often enhance access to health services through no or low-cost services and may have interpreters and bilingual staff, as well as longer consultation hours. 25,42 By training providers in culturally sensitive care and providing linguistically appropriate services, these care models can enhance the quality of care provided and, in doing so, positively affect patient health outcomes. 43 –46 Unfortunately, our finding that a lower percentage of recent immigrants report their usual place of care was a CHC or interdisciplinary team is consistent with an Ontario study that found immigrants were underrepresented in newer team-based models of primary care. 47 While findings highlight a clear role for primary care, system-level changes such as eliminating waiting periods for insurance, expanding coverage, and ensuring access to interpretation services are needed.
Limitations and Future Research
A limitation of this study is that it only includes landed immigrants and permanent residents, and we are unable to distinguish between immigrant admission classes. Temporary foreign workers, recent refugees, and people with precarious status are not captured by the CCHS and may experience extreme barriers to accessing health care. 48,49 Refugees and refugee claimants are temporarily covered through the Interim Federal Health program. However, changes and cuts to this program have created confusion among health providers and consumers alike regarding eligibility and coverage. 38 –40 The lack of data on severity of symptoms prevented us from accounting for this potential confounder. Additionally, the survey asks respondents whether they describe themselves as male or female. While it may be plausible that biological sex differences shape mental disorders, it is likely that gender identity and expression play a larger role in determining patterns of access to services. As the CCHS is a cross-sectional survey, we were unable to infer causal relationships between variables. The CCHS is also a voluntary survey and so is subject to all the limitations of any other survey data, including self-report of mood or anxiety disorders. Previous research has found discordance in diagnoses of mood and anxiety disorders between survey and administrative data. 50 However, administrative data in Canada are limited in capturing privately paid services and cannot identify people with mood or anxiety disorders who have not accessed care. Survey data are therefore well aligned with our objectives related to gaps in access. Another limitation is the small sample size within the recent immigrant group and correspondingly wide CIs in the stratified model. Future analysis can include additional cycles of CCHS data which may increase power to detect meaningful relationships.
It is important to remember that immigrant and refugee groups are heterogenous. A limitation of the study is the inability to analyze by racialized groups or by country of origin as these are unavailable in the public CCHS data files. Future research can use nonpublic use CCHS data files to further explore how racialization and country of origin impact access to needed health services. Furthermore, the migration journey is different for all migrants and the experiences and challenges faced before, during, or after migration can have various impacts on health, belonging, and acculturation. 51,52 Future research should also explore how additional factors such age of migration, and pre- and postmigration factors impact mental health and access to primary care and specialized mental health services. Additionally, future studies should explore differences in access to mental health services between and among provinces and territories, as planning and funding are managed at the provincial level. 53 Access to primary care differs by province and the role it plays in shaping access to mental health services may as well. 54 Finally, future work could test interventions aimed at reducing system barriers, including access to interpreters and training providers in cultural humility, so that no matter where people are from, and where they access care, they can build a trusting relationship which can lead to better mental health care.
Conclusion
Our finding confirms that there is a gap in access to mental health services for immigrants with mood and/or anxiety disorders. Primary health care appears to play an important role in shaping access to mental health consultations. People with access to team-based primary care are more likely to report mental health consultations, and this is especially true for immigrants. Unfortunately, immigrants, and especially recent immigrants, are more likely to see a doctor in solo practice or use walk-in clinics as a usual place of care. Policies are needed to expand access to team-based primary health care and address barriers to mental health services throughout the health care system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.