
Abstract
Objectives:
Relatively little is known about how health-care utilization differs among individuals with psychological distress compared to those with major depressive disorder (MDD).
Methods:
Ontario participants of the Canadian Community Health Survey Cycle 1.2 (2002) were linked to health administrative data to follow their health-care utilization patterns for up to 15 years. Based on their survey responses, we classified individuals hierarchically into Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, criteria MDD, psychological distress (Kessler-6: 8 to 24), or an unexposed group with neither condition. We compared the rates of outpatient and acute care mental and nonmental health-related visits across the 3 groups over time using Poisson regression.
Results:
Among the 430 individuals with MDD, 668 with psychological distress, and 9,089 in the unexposed group, individuals with MDD and psychological distress had higher rates of health-care utilization than the unexposed overall and across time. The rates of psychiatrist visits for the MDD group were significantly higher than the other groups initially but declined over the follow-up. Conversely, the rates of psychiatrist visits among the psychological distress group increased over time and converged with that of the MDD group by the end of follow-up (rate ratioMDD vs. psychological distress at 1 year: 4.20 [1.97 to 11.40]; at 15 years: 1.53 [0.54 to 4.08]). Acute care visits were similar between the MDD and psychological distress groups at all time points.
Conclusions:
Individuals with psychological distress required mental health care rivalling that of individuals with MDD over time, suggesting that even a cross-sectional assessment of significant psychological distress is a serious clinical concern.
Introduction
Psychological distress is a nonspecific condition characterized by symptoms of depression and anxiety that does not meet criteria for a mental disorder, usually because the number or severity of symptoms does meet a certain threshold, or at times because a stressor is thought to be causing symptoms and it is expected that symptoms will resolve without significant intervention over time. It is common, affecting between up to 27% of the general population worldwide at any point in time. 1 –3 It is more prevalent than its more severe counterpart, major depressive disorder (MDD)—in Canada, about 20% of the population reported having high psychological distress compared to about 5% of adults with depression in the past year. 1,4 Major depressive disorder has been widely studied and has been associated with a reduced quality of life, increased health service utilization, and high economic burden. 5 –9 However, previous work by our team found that despite the perception that psychological distress is a less serious problem, the per capita direct health-care costs incurred by someone with psychological distress were similar to that of an individual with MDD over time, 10 as was the mortality rate. 11,12
One area that has received relatively less attention is the longitudinal pattern of health service use for an individual with psychological distress over time. There is some evidence that compared to the general population, individuals with psychological distress have more office visits, emergency department visits, and hospitalizations and are also more likely to consult different types of health-care professionals, including specialists. 13 –17 Most past studies only focused on either the ambulatory care or the acute care sector, relied on participant self-report for information on health-care utilization and did not differentiate between mental health and nonmental health-care visits. A better understanding of the trajectory of health service utilization for individuals with psychological distress over time might shed light on how and when to intervene in this population.
This study aimed to examine the longitudinal patterns of health service utilization among individuals with psychological distress at a cross sectional point in time and make comparisons between them and their counterparts with MDD or neither MDD nor psychological distress at the same point in time.
Methods
Data Sources and Study Population
The study population comprised of the Ontario component of the Canadian Community Health Survey (CCHS) Cycle 1.2 administered by Statistics Canada between May and December 2002. This survey focused specifically on mental health and included the Diagnostic and Statistical Manual of Mental Disorders criteria for depression using the World Health Organization World Mental Health Composite International Diagnostic Interview (WHO WMH-CIDI) and utilized a validated Kessler 6 (K6) scale to determine psychological distress. Details of the CCHS methodology have been described elsewhere. 18 Briefly, the survey was administered in a representative sample of households across Canada and included modules on health status, mental well-being, mental illness, determinants of mental health, health-care utilization, demographics, and other related variables. 18 Participants were aged 15 years and older living in private dwellings in Canada’s 10 provinces covering approximately 98% of Canada’s population. The respondents were randomly selected using a stratified, multistage, clustered area sampling strategy with an overall survey response rate of 77%. 18 Survey data from respondents residing in the province of Ontario were linked at ICES to health administrative databases available through Ontario’s single-payer health-care system enabling longitudinal measurement of health-care service utilization. ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. Multiple ICES databases, linked together using unique encoded identifiers, were used for the project: Outpatient care data were obtained from the Ontario Health Insurance Plan (OHIP) database, emergency department visit data were obtained from the National Ambulatory Care Reporting System database, and information about hospitalizations were obtained from the Canadian Institute for Health Information Discharge Abstract Database and the Ontario Mental Health Reporting System. For covariate measurement, we also accessed the Ontario Registered Persons Database (RPDB) (e.g., area-level income, death, and OHIP eligibility), the Ontario Cancer Registry, and validated population-based chronic disease cohorts based on combined ICES data sources (e.g., respiratory, cardiovascular disease, hypertension, and diabetes). 19 –23 The study sample was followed until the end of OHIP eligibility, death, or administrative censoring on March 31, 2017.
Cohort Creation
We considered all Ontario CCHS 1.2 respondents who consented to linkage of their data to ICES (86%). We excluded individuals with a history of more severe mental illness, such as a hospitalization record of schizophrenia/schizoaffective disorder (International Classification of Diseases [ICD] 9: 295; ICD-10: F20, F25) or bipolar disorder (ICD-9: 2960, 2961, 2964, 2965, 2966, 2667, 2668; ICD-10: F30, F31) in the 5 years preceding the date of the survey. We also excluded self-reported lifetime psychosis, past-year mania, or eating disorders at baseline. Respondents who lost OHIP eligibility a year prior to the interview date or had data inconsistencies (e.g., dead prior to interview date and missing data on main exposure; Supplementary Figure 1) were excluded as well.
Exposure
The WHO WMH-CIDI was administered by trained interviewers to determine depression diagnoses of CCHS 1.2 respondents. 18 It was developed by the World Health Organization (WHO) to take into account the Diagnostic and Statistical Manual, Fourth Edition (DSM-IV) definitions and the WHO ICD-10 and assesses for mood, anxiety, substance abuse, and impulse control disorders. 24 Respondents were classified as having MDD if they had a major depressive episode in the 12 months prior to the interview, as per DSM-IV criteria. 25 Among respondents who were not classified into the MDD group, those with scores of 8 to 24 inclusive on the K6 scale were classified as having psychological distress at the time of the interview. 26 The K6 is a measurement of nonspecific psychological distress found to be an accurate and valid measure within surveys and primary care settings. 27 It is a 6-item questionnaire based on a 5-point scale ranging from 0 = “none of the time” to 4 = “all of the time” resulting in response ranges from 0 to 24. 27 The remaining respondents who did not meet the criteria for MDD nor for psychological distress were considered the unexposed group.
Outcomes
We defined mental health-related ambulatory care visits as outpatient visits to a psychiatrist or a nonpsychiatrist (i.e., primary care outpatient visits to family physician [FP], general practitioner [GP], or pediatrician). Primary care outpatient mental health visits were based on the validated Steele algorithm 28 modified to include outpatient visits with a mental health diagnostic code, excluding some diagnostic and therapeutic procedures (i.e., G fee-codes). Mental health-related acute care visits were emergency department visits (coded with a primary diagnosis of ICD–10 F06–F99, X60–X84, Y10–Y19, Y28 or X60–X84, Y10–Y19, and Y28 as a secondary diagnosis with no F06–F99 as a primary diagnosis) or hospitalizations (defined as 1) inpatient admissions with a primary diagnosis of ICD–10 F06–F99 or any diagnosis of X60–X84, Y10–Y19, and Y28 as a secondary diagnosis with no F06–F99 as a primary diagnosis; or (2) an admission in the Ontario Mental Health Reporting System. An ED visit that led to a hospital admission was considered a single acute care visit. The remaining outpatient and acute care visits were grouped into nonmental health-related (1) primary care outpatient visits and (2) acute care visits. For descriptive purposes, we also recorded 6 to 7 of the most common mental health-related diagnoses during visits to primary care outpatient mental health visits and visits to psychiatrists during the follow-up period.
Study Variables
Baseline characteristics derived from the CCHS survey were age, sex, rural or urban residence, ethnicity, immigrant status, and marital status as well as individual income and employment status and lifestyle factors, such as physical inactivity (i.e., energy expenditure <1.5 kcal/kg/day), body mass index, alcohol consumption, and current smoking status. The CCHS WMH-CIDI was used to determine the presence or absence of anxiety disorder. Residential postal code from the RPDB was used to derive area-level income. We used the linked administrative databases and validated registries to examine baseline prevalent medical comorbidities, such as respiratory (i.e., asthma and chronic obstructive pulmonary disease), cardiovascular disease (i.e., acute myocardial infarction and congestive heart failure), hypertension, diabetes, and cancer.
Statistical Analysis
Sampling weights provided by Statistics Canada were applied in all analyses to account for the multistage survey sampling design and to ensure that estimates were generalizable to the Ontario population. Baseline characteristics of the 3 exposure groups were compared against the unexposed using weighted means and unweighted standard deviations for continuous variables and unweighted frequencies and weighted percentages for categorical variables. T-tests were used to compare differences in means, and chi-square tests were used to compare differences in proportions. Statistical significance was indicated by a 2-tailed P value <0.05. The association between exposure groups and health-care utilization was assessed using Poisson regression with log person-years as an offset. Yearly incidence rates were plotted by the exposure group, and P values for trends were calculated over time within each exposure group using the nonparametric Kendall Tau-b test for repeated summary statistics. We calculated rate ratios (RR) by comparing the rates of those with MDD to the unexposed, rates of those with psychological distress to the unexposed, and rates of those with MDD to those with psychological distress. Bootstrap methods using 500 bootstrap weights 16 were used to estimate 95% confidence intervals for incidence rates and RRs. All analyses were performed with SAS version 9.4 (SAS Institute Inc, Cary, North Carolina).
Ethics Approval
The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a Research Ethics Board.
Results
Study Sample
A total of 10,662 respondents completed the CCHS 1.2 Mental Health Survey in Ontario, of which 475 were excluded due to serious mental illness, loss of OHIP eligibility, or data inconsistencies, resulting in a study population of 430 with MDD, 668 with psychological distress, and 9,089 in the unexposed group (Supplementary Figure 1). Those with psychological distress and MDD were younger than the unexposed, were less likely to be married, and significantly more likely to be physically inactive, current smokers, and have an anxiety disorder. Compared to the unexposed, those with MDD were more likely to be female and a greater proportion had respiratory conditions. A greater proportion of the psychological distress group were unemployed and had lower income than the unexposed (Table 1).
Baseline Characteristics of Those with Psychological Distress, Major Depression, and the Referent Group (Unweighted vs and Weighted Means and Proportions).a
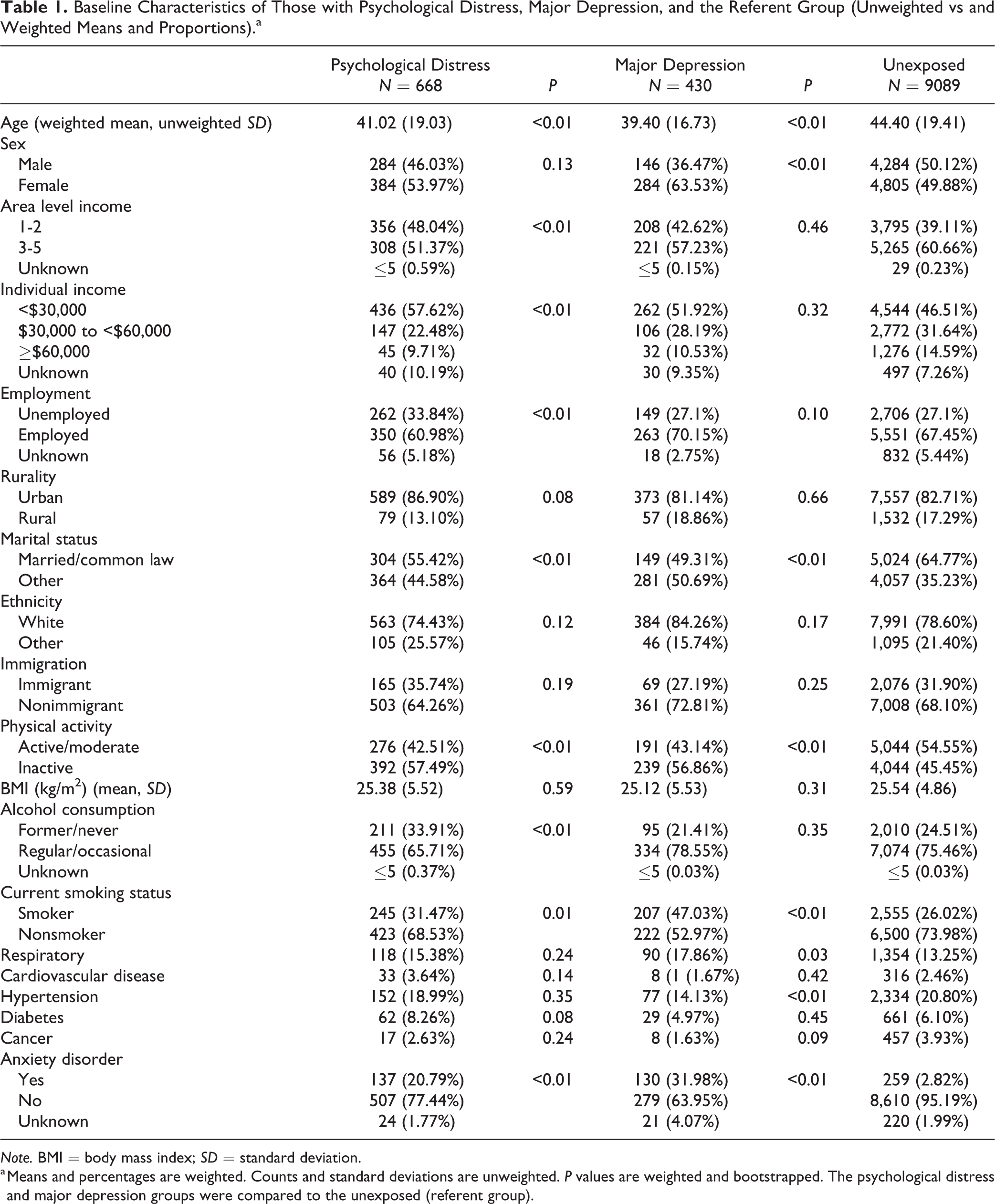
Note. BMI = body mass index; SD = standard deviation.
a Means and percentages are weighted. Counts and standard deviations are unweighted. P values are weighted and bootstrapped. The psychological distress and major depression groups were compared to the unexposed (referent group).
Outcomes
Over the 15-year follow-up period, there were 18,917 outpatient mental health visits to psychiatrists, 48,019 to primary care, and 1,819 acute care mental health-related visits in the whole cohort.
Psychiatrist and primary care outpatient mental health visits
From interview date to end of follow-up, the percentage of individuals with at least 1 nonpsychiatrist primary care mental health-related outpatient visit was 77.8%, 68.8%, and 52.3% for the MDD, psychological distress, and unexposed groups, respectively. The percentage of individuals with at least 1 outpatient psychiatrist visit was 36.9%, 24.8%, and 10.5% for the MDD, psychological distress, and unexposed groups, respectively.
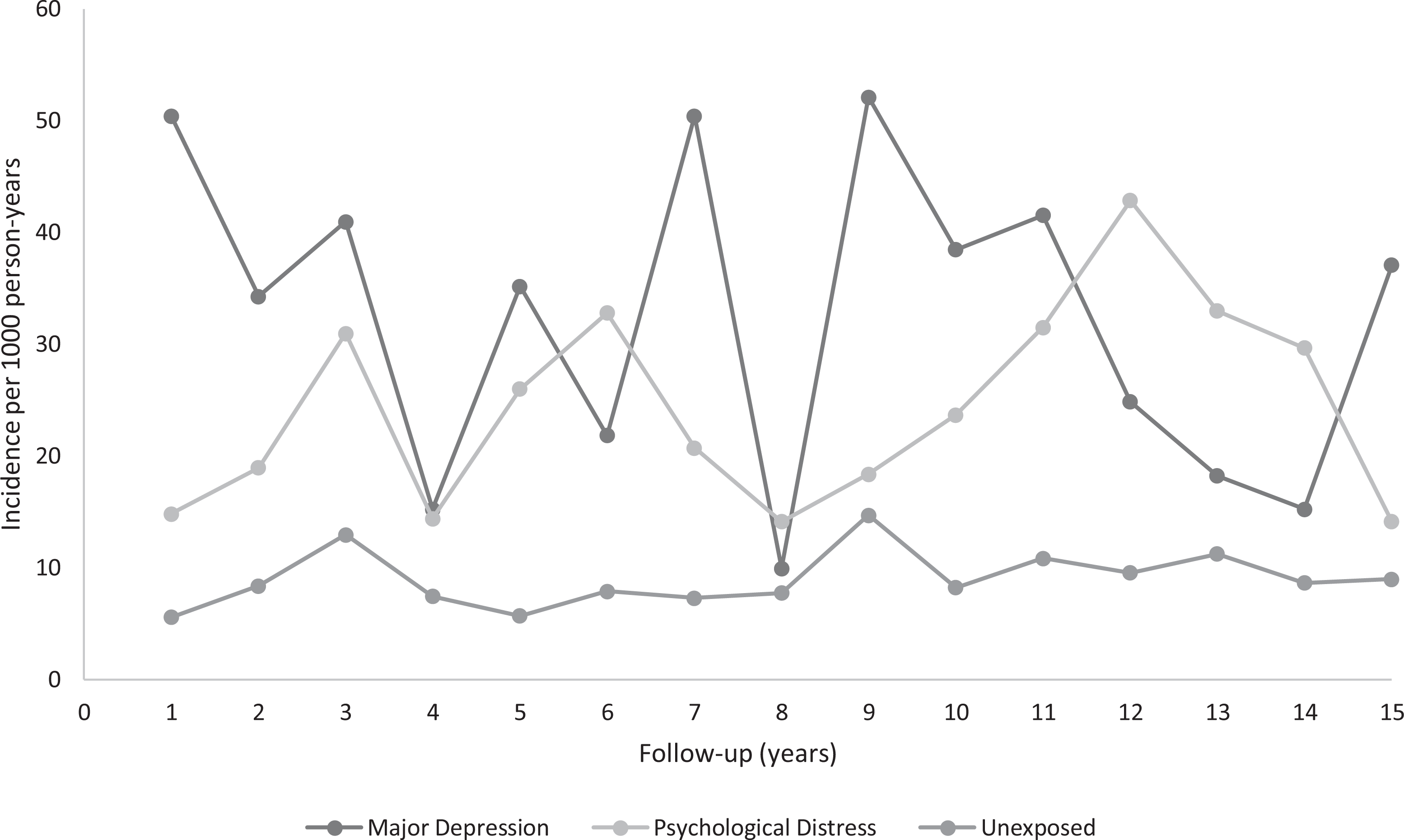
Overall, the rates of outpatient visits to a psychiatrist among those with MDD and psychological distress were significantly higher compared to the unexposed group. Compared to the unexposed group, individuals with MDD had higher rates of psychiatrist use in the initial years and these rates eventually declined and stabilized over time (RRMDD vs. unexposed at 1 year: 18.04 [8.91 to 33.18]; at 9 years: 3.19 [1.90 to 5.46]; at 15 years: 4.23 [1.90 to 7.41]). An interesting trend emerged when MDD was compared to psychological distress; in that the rates of psychiatrist visits were initially lower for psychological distress but these rates converged with the MDD group in later years of follow-up (RRMDD vs. psychological distress at 1 year: 4.20 [1.97 to 11.40]; at 5 years: 2.45 [1.09 to 6.33]; at 13 years: 1.18 [0.42 to 3.77]; at 15 years: 1.53 [0.54 to 4.08]; Figure 1 and Table 2).
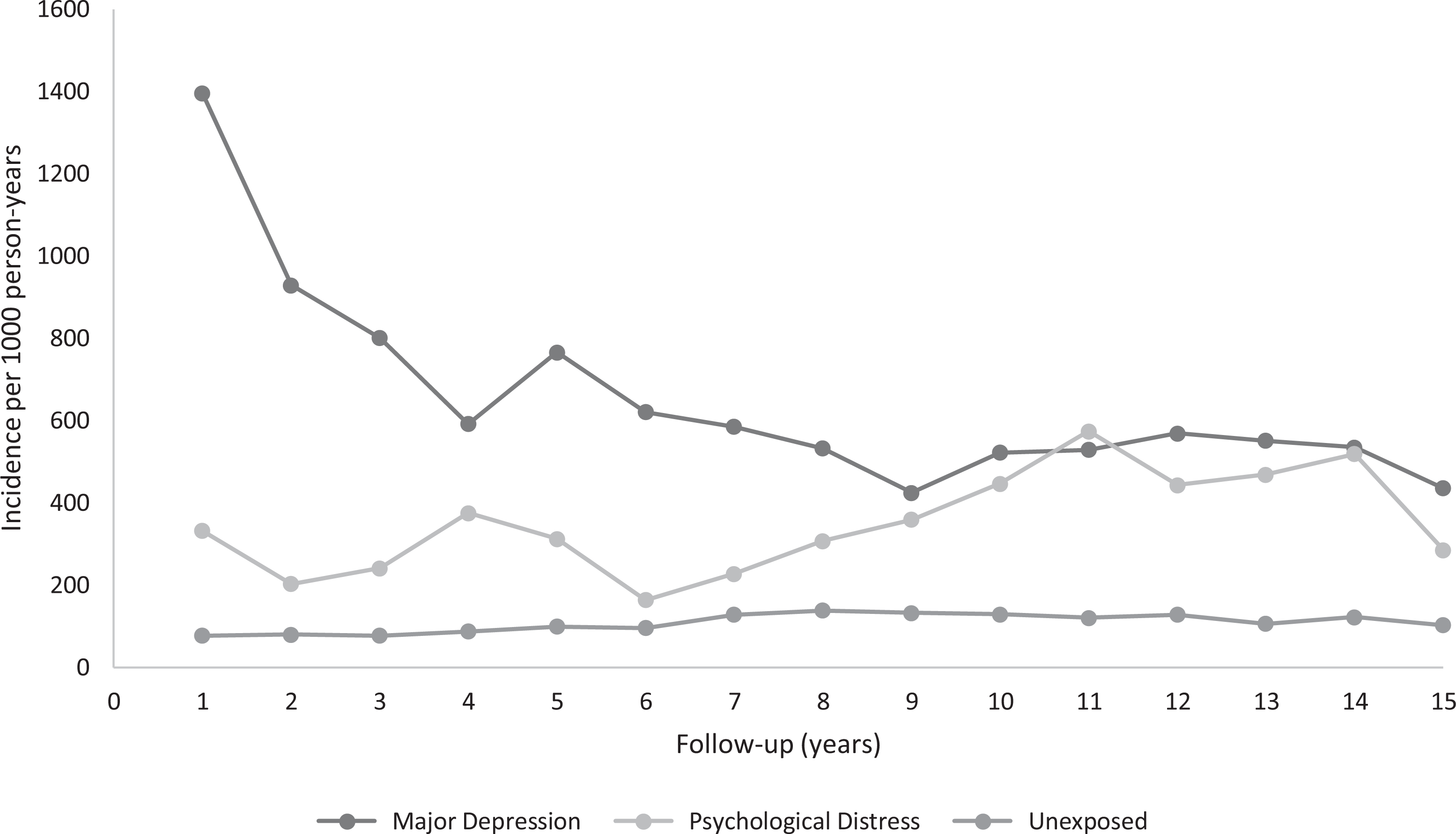
Rates of psychiatrist claims by exposure groups. P trend MDD = 0.0006; P trend psychological distress = 0.03; P trend unexposed = 0.03. MDD = major depressive disorder.
Rates and Rate Ratios of Psychiatrist and Primary Care Outpatient Mental Health Visits by Exposure Group Over Time.a
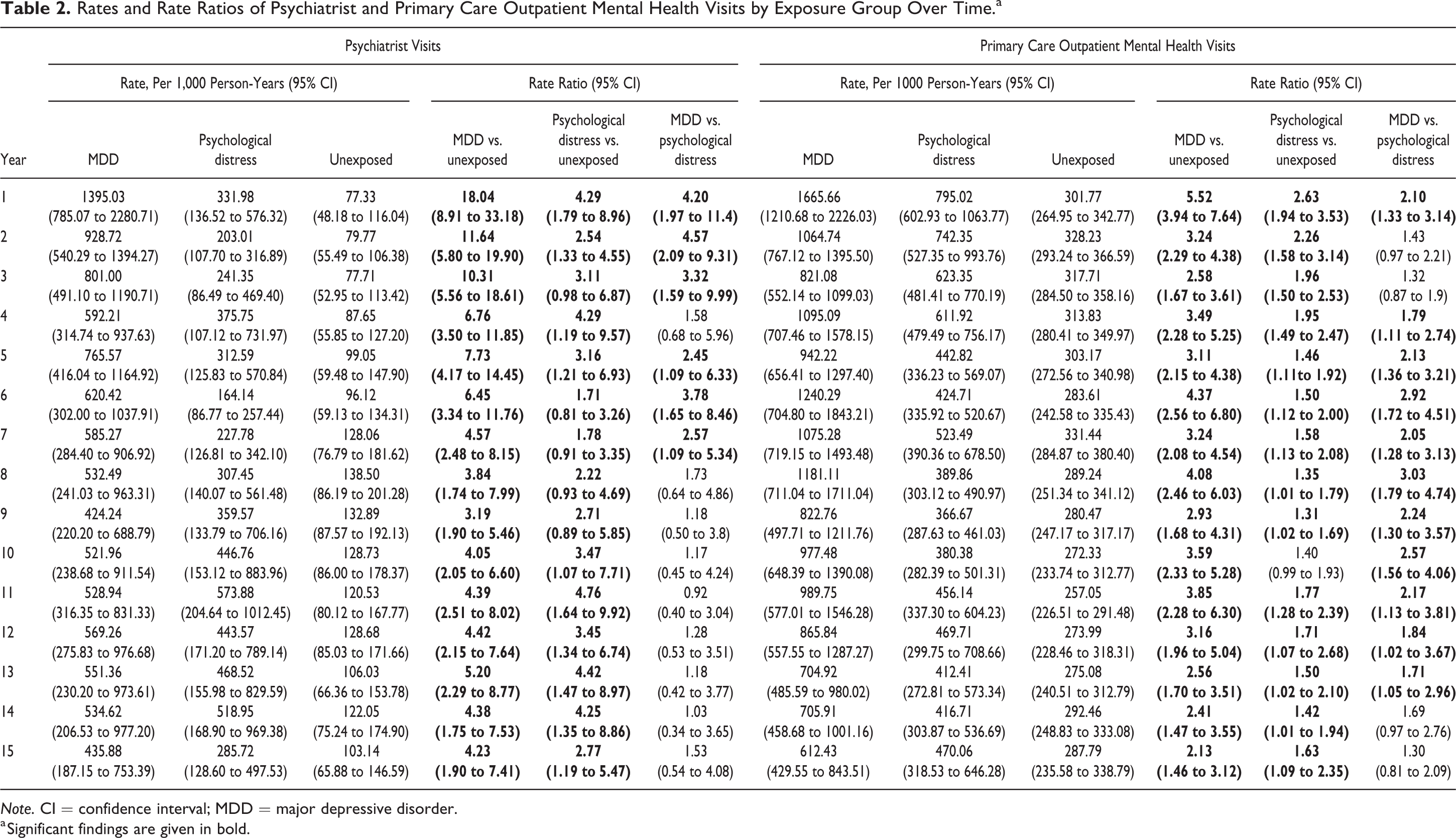
Note. CI = confidence interval; MDD = major depressive disorder.
a Significant findings are given in bold.
In general, the rates of primary care outpatient mental health visits were highest among the MDD group followed by the psychological distress group and the unexposed group. Compared to the unexposed group, both the MDD and psychological distress groups had higher rates of visits in the initial years of follow-up and service use declined over time (RRMDD vs. unexposed at 1 year: 5.52 [3.94 to 7.64]; at 7 years: 3.24 [2.08 to 4.54]; at 15 years: 2.13 [1.46 to 3.12]; RRpsychological distress vs. unexposed at 1 year: 2.63 [1.94 to 3.53]; at 7 years: 1.58 [1.13 to 2.08]; at 15 years: 1.63 [1.09 to 2.35]). The rates of primary care mental health visits declined over time to a greater extent in the MDD group such that the rates of use among MDD and psychological distress were no longer statistically different after 13 years of follow-up (RRMDD vs psychological distress at 1 year: 2.10 [1.33 to 3.14]; at 7 years: 2.05 [1.28 to 3.13]; at 15 years: 1.30 [0.81 to 2.09]; Figure 2 and Table 2).
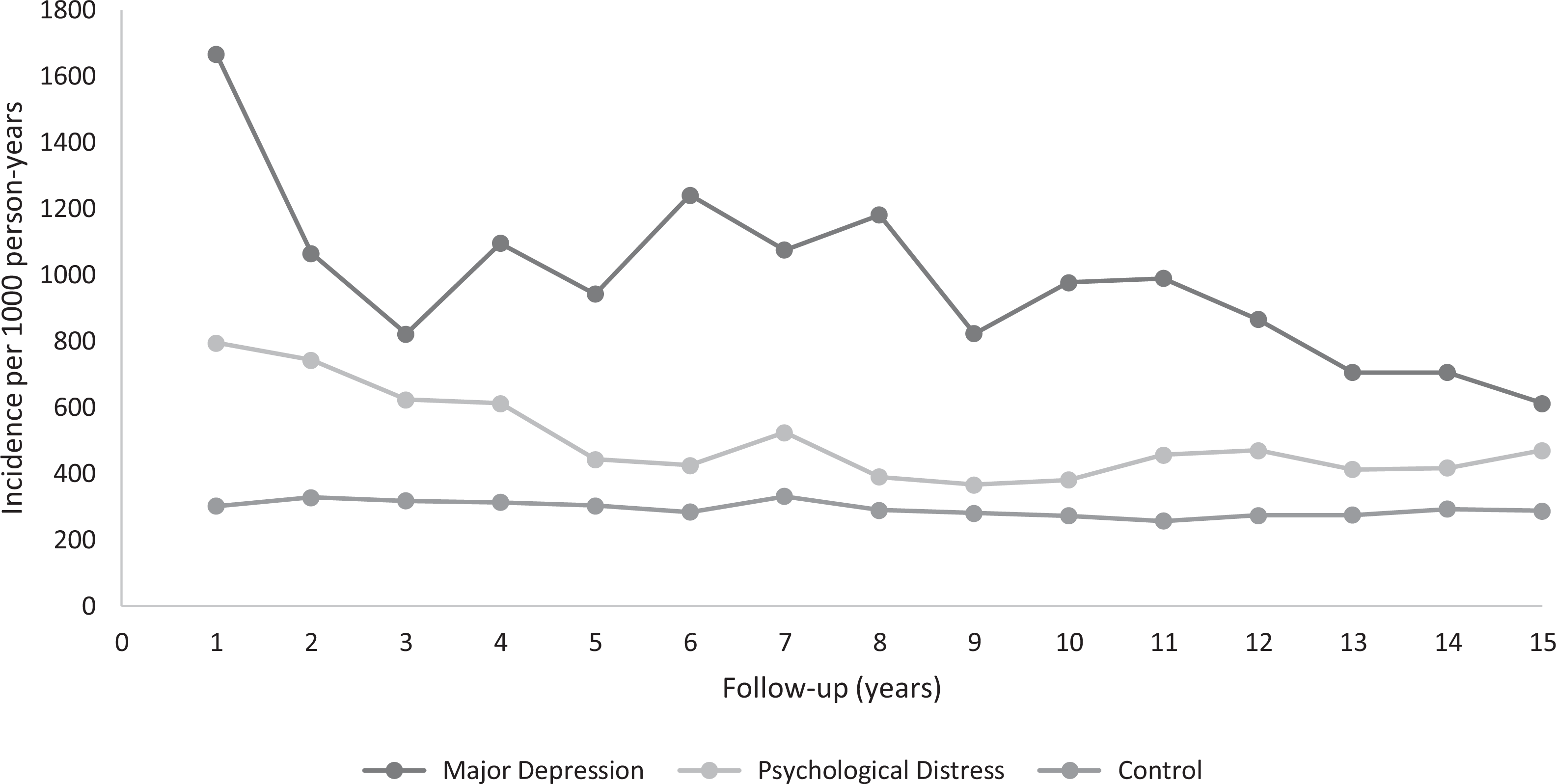
Rates of primary care mental health-related claims by exposure group. P trend MDD = 0.009; P trend psychological distress = 0.03; P trend unexposed = 0.02. MDD = major depressive disorder.
In the outpatient setting, the most common diagnosis across all 3 exposure groups was anxiety neurosis, hysteria, neurasthenia, obsessive compulsive neurosis, and reaction depression followed by depressive or other nonpsychotic disorders. Combined, this resulted in approximately 75% of diagnoses among those with MDD, 85% among those with psychological distress, and 70% among unexposed for psychiatrist visits and approximately 75% to 80% of diagnoses across all 3 exposure groups for primary care outpatient mental health visits. Psychiatrists used the depressive or other nonpsychotic disorders more frequently for patients with psychological distress (29.7%) than for those with MDD (17.0%) or the unexposed group (13.6%; Supplementary Figure 3).
Acute care mental health-related visits
There were no observable differences in the rates of acute care mental health-related visits in those with MDD and psychological distress compared to the unexposed, neither overall nor across time. There were no statistically significant differences in the rates of acute care mental health visits in the MDD group compared to those with psychological distress groups except for in the first year of follow-up, where those with MDD had significantly higher rates (emergency department visits among those with MDD: 43 per 1,000 person-years vs. psychological distress: 16 per 1,000 person-years; hospital visits among those with MDD: 25 per 1,000 person-years vs. psychological distress: 0.93 per 1,000 person-years, P < 0.01; Figure 3, Supplementary Table 1).
Rates of acute care mental health-related visits by exposure group. P trend MDD = 0.35; P trend psychological distress = 0.35; P trend unexposed = 0.07. MDD = major depressive disorder.
There were no observable differences in the rates of nonmental health-related primary care outpatient visits and acute care visits among those with MDD and psychological distress compared to the unexposed, neither overall nor across time, nor were there any differences when comparing the MDD group to the psychological distress group (Supplementary Figure 2).
Discussion
In this large population-based study comparing longitudinal health-care utilization patterns across individuals with cross-sectional evidence of psychological distress, MDD or neither, we found greater health-care utilization among those in the exposed versus unexposed groups. We also found that mental health-care utilization in those with cross-sectional evidence of psychological distress but not MDD was associated with a pattern of utilization that was quite similar to that of the MDD group as time progressed. A large proportion of those with psychological distress were eventually diagnosed with anxiety and depressive disorders by physicians over the 15-year follow-up period.
Although no previous study has compared health service use between people with psychological distress and MDD, our finding that those with MDD have the highest primary care outpatient mental health visits compared to those with psychological distress and the unexposed group is consistent with previous research, which reported that among those with depression, over 90% reported only having ambulatory care contact for their mental health-care needs, and nearly 75% of these contacted an FP or GP. 29 Similarly, another study found that those with MDD visited an FP significantly more often than those without MDD. 16 Similar to our findings, research has also shown significantly higher use of office-based and outpatient visits as well as mental health visits to nonmental health professionals among those with psychological distress compared to those without. 16,30 –34
Our study showed that in later years of follow-up, the rate of psychiatrist visits among those with psychological distress increased and converged with the MDD group. There is some evidence in the literature suggesting a significant association between psychological distress and seeking specialist care. Research in the United States has shown that, in general, the prevalence of contact with mental health professionals has significantly increased from 29.1% in 1997 to 35.5% in 2002. 35 One such study showed that those with psychological distress were significantly more likely to consult a psychiatrist in the past 12 months compared to those without psychological distress (P = 0.004). 16 Similar conclusions have been drawn by another study showing that psychological distress was associated with 1.5-fold higher odds of a mental health specialist visit and was also a strong predictor of mental health visits to all types of professionals. 32
Our study provides further evidence that psychological distress, a much more prevalent condition than depression, is a nontrivial health issue that results in significant health service use—and may commonly progress to mental disorders such as MDD and anxiety disorders over time. A previously published economic analysis by members of our group found that people with psychological distress incur similar per capita costs and double the population-wide costs to the health-care system as those with MDD. 10 Psychological distress is also associated with a greater risk of poor physical health, chronic diseases, and mortality. 12,36 –39 In this study, we found decreasing general and specialist outpatient use in the MDD group over time but an increase in the psychological distress group. While the reasons for this are not necessarily discernible from these data, it is plausible that while those with MDD were receiving treatment and starting to recover, a good proportion of those with psychological distress were beginning to develop full blown psychiatric disorders.
The population-based nature of this study, the detailed characterization of the exposure groups based on self-report of participant mental health status taken by trained interviewers, and the 15 year follow-up are important study strengths. Depression status was ascertained using validated and widely used instruments for depression diagnoses, while health-care utilization was obtained from health administrative records allowing for a more objective measure of health-care utilization by reducing risk of recall bias. However, there are some limitations. Although the survey covered approximately 98% of the Canadian population and weighting and bootstrapping were conducted to make the sample more representative of the general population, 18 some populations were not sampled in this survey (e.g., persons living in Indigenous Reserves or Crown lands, individuals living in institutions, members of the Canadian Forces, and residents of some remote locations). Since MDD and psychological distress were ascertained only at baseline, the exact nature of an individual’s symptoms was not known over time (i.e., we only had physician-based diagnoses in the health-care data). Although we excluded individuals with past-year mania and those who were hospitalized for bipolar disorders in the past 5 years, we may not have excluded all individuals with history of manic or hypomanic episodes. In addition, some health service use may not have been captured in our study as there are services that are paid for privately when delivered outside of a hospital or family practice setting (e.g., non-MD psychological treatments), but the extent of this would not be expected to differ between groups. Another important limitation is that distress is a nonspecific indicator of mental illness, useful for assessing population mental health. Elevated scores of the K6 may represent a variety of mental disorders; this inherent nonspecificity of the K6 makes it difficult to assess the implications this might have on health services and interventions. This study was largely descriptive; further studies are needed to determine a specific response or course of action.
Conclusions
Individuals who present cross-sectionally with MDD and psychological distress have similarly high rates of mental health-related health-care utilization over time. The evidence that rates of outpatient mental health visits tend to increase among those with psychological distress while decreasing among those with MDD suggests that the prognostic importance of psychological distress presentations may be minimized in our health-care system, and that there is a missed opportunity to secondary prevention of the progression from symptoms of psychological distress to a mental disorder. As even a cross-sectional assessment of psychological distress seems to be a serious clinical concern, further efforts to understand the characteristics of psychological distress may prevent the escalation of symptoms from distress to depression and help to reduce health-care utilization over time.
Supplemental Material
Supplementary_material - Health Service Use among Individuals with Depression and Psychological Distress: A Population-Based Cohort Study in Ontario, Canada
Supplementary_material for Health Service Use among Individuals with Depression and Psychological Distress: A Population-Based Cohort Study in Ontario, Canada by Maria Chiu, Farah E. Saxena, Paul Kurdyak, Andrew S. Wilton and Simone N. Vigod in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
Maria Chiu was the principal investigator of this study and provided the conception and design for the study and provided study supervision. Andrew Wilton performed the statistical analyses. Maria Chiu, Simone Vigod and Farah Saxena drafted the manuscript. All authors interpreted the data, provided critical revisions for the manuscript, and final approval of the contents of the submitted manuscript. The data set from this study is held securely in coded form at ICES. While data sharing agreements prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at ![]() . The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Acknowledgments
The authors acknowledge that the data used in this publication are from Statistics Canada’s Canadian Community Health Survey on Mental Health and Well Being, cycle 1.2 (CCHS 1.2). We thank all the participants of this survey and the staff from Statistics Canada who assisted in the survey data collection and management. We would also like to thank Maria Eberg for her earlier contribution to the analytical work on this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: P. Kurdyak has received operational support by an Ontario Ministry of Health and Long-Term Care (MOHLTC) Health Services Research Fund Capacity Award to support this project. S. Vigod is supported by a New Investigator Award from the Canadian Institutes of Health Research. This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). The opinions, results, and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and information provided by Cancer Care Ontario (CCO). The opinions, results, views, and conclusions reported in this article are those of the authors and do not necessarily reflect those of CCO. No endorsement by CCO is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed in the material are those of the author(s) and not necessarily those of CIHI.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.