
Abstract
Objective:
Understand the relationship between criminal accusations, victimization, and mental disorders at a population level using administrative data from Manitoba, Canada.
Method:
Residents aged 18 to 64 between April 1, 2007, and March 31, 2012 (N = 793,024) with hospital- and physician-diagnosed mental disorders were compared to those without. Overall and per-person rates of criminal accusations and reported victimization in the 2011/2012 fiscal year were examined. Relative risks were calculated, adjusting for age, sex, income, and presence of a substance use disorder. The overlap between diagnosed mental disorders, accusations, and victimization with a χ2 test of independence was studied.
Results:
Twenty-four percent (n = 188,693) of the population had a mental disorder over the 5-year time frame. Four to fifteen percent of those with a mental disorder had a criminal accusation, compared to 2.4% of the referent group. Individuals with mental disorders, especially psychotic or personality disorders, were often living in low-income, urban neighborhoods. The adjusted relative risk of accusations and victimization remained 2 to 5 times higher in those with mental disorders compared to the referent group. Criminal accusations and victimization were most prevalent among individuals with a history of attempted suicide (15.2% had an accusation and 8.1% were victims). The risk of victimization in the same year as a criminal accusation was significantly increased among those with mental disorders compared to those without (χ2 = 211.8, P < 0.001).
Conclusions:
Individuals with mental disorders are at elevated risk of both criminal involvement and victimization. The identification of these multiply-stigmatized individuals may lead to better intervention and support.
Introduction
The proportion of persons with mental illness involved in criminal justice has increased over time 1,2 and their burden of illness is enormous. 3 –6 Deinstitutionalization in North America, with a corresponding shift in mental health services from hospitals to community settings, has been criticized as providing inadequate support for the complex needs of those with mental disorders 7,8 and leading to their increased contact with the justice system. 9 –11 European research indicates conflicting support for this relationship, 12,13 while an association has been found in 6 countries throughout South America followed longitudinally. 14 Individuals who interact with the law may do so as either an accused person, as a victim of crime, or both.
Little population-based literature has explored criminal victimization among people with mental disorders. In a cohort study in Denmark, 15 new onset mental disorder, especially substance use disorder and personality disorder, conferred victimization risk of both general and violent crime. Other research has been limited by including narrowly defined populations such as hospital inpatients, 16 outpatients with a diagnosis of schizophrenia, 16,17 or the homeless, 18 using interview study designs with a focus on violence. 16,17,19 These studies have highlighted the increased risk of victimization among those with mental disorders, urging for further exploration of this complex intersection. In considering perpetrators of crime, research has demonstrated that prisoners have a greater prevalence of mental disorders such as depression, psychosis, antisocial personality disorder, and substance use disorders compared with the general population, 20,21 with the onset of illness usually occurring prior to incarceration. 22 Despite their presence, mental health needs are unmet in both men and women inmates. 22,23 Upon release, prisoners with mental disorders have elevated disability and mortality risk independent of sociodemographic, criminological, and familial factors. 24,25 They often lack housing, struggle with substance use issues, 26 –29 and become trapped in a revolving door of recidivism, 30 –32 especially when less serious or technical violations are considered. 33 –35 Incarceration is endured for a defined period of time, but mental health needs exist before, during, and after custody. 36
The heavy emphasis on prison data in examining justice system involvement among the mentally ill 20–21 is rife with problems, as numerous individuals who never come into custody are excluded. Crime and incarceration rates do not consistently rise and fall in synchrony with each other; in the United States, the two became uncoupled over a 20-year time frame. 37 The use of prison alternatives, such as restorative justice, community service orders, and electronic monitoring, has decreased the rate of detention in many countries worldwide. 38 The implementation of specialized problem-solving courts (e.g., for mental disorder or substance use) often diverts the mentally ill away from prisons. 39 In addition, individuals found not criminally responsible or unfit to stand trial due to their mental state are typically brought to forensic hospitals for treatment, leading to their exclusion in studies of prisoners.
Several factors can keep individuals trapped at the nexus of mental health and criminal justice systems. Stigma by society (including potential employers) 40 as well as self-stigma, where the individual believes the negative perceptions of society, are linked to reduced medication adherence, increased arrests, increased psychiatric symptom severity, interference with rehabilitation, and homelessness 41 –43 which put individuals at risk of being caught at the intersection of these two systems. While programs for offenders with mental illness including forensic assertive community treatment and intensive case management exist, it has been argued that there is too much emphasis on treating mental illness instead of other causes of criminal behavior, such as antisocial cognitions and lack of prosocial skills. 44
In order to truly support those who are vulnerable, it is imperative to understand the relationship between mental disorders and justice involvement using a broader lens. Our study used population-level administrative data from Manitoba, Canada, to examine the relationship between criminal accusations and victimization among a representative sample of people with mental disorders. Administrative data are advantageous because they provide clinician-based diagnoses, whereas interview assessments may misclassify mental disorder in 10% to 15% of individuals. 45 We determined the 1-year relative risk of accusations and victimization among individuals with a diagnosed mental disorder compared to a referent group with no mental disorder and specifically examined the rates of intersecting vulnerability.
Method
Participants and Data Sources
Our sample included residents from Manitoba, Canada, aged 18 to 64 between April 1, 2007, and March 31, 2012. Data were retrieved from the Manitoba Population Research Data Repository at the Manitoba Centre for Health Policy (MCHP). 46 The MCHP holds a wide range of population-level data sets linkable at the individual level using a unique encrypted personal health information number. The repository contains data for more than 99% of the province’s residents, 47 with data linkage accuracy over 95%. 48 We used data from the Manitoba health insurance registry (age and sex), the Manitoba Justice Prosecution Information and Scheduling Management (PRISM) registry (criminal accusations and victimization), hospital records and physician billing (diagnoses), and the Canada Census (area-level income). This study was approved by the University of Manitoba research ethics board and the Health Information Privacy Committee of Manitoba Health.
Mental Disorder Diagnosis
Based on diagnoses recorded in their inpatient and outpatient health care data, individuals were coded as having a mental disorder or not between April 1, 2007, and March 31, 2012. Inpatient diagnoses were based on the International Classification of Diseases, 10th Edition, Canada (ICD-10-CA) system, while outpatient diagnoses utilized the International Classification of Diseases, ninth Revision, Clinical Modification (ICD-9-CM) classification system. Nonmutually exclusive groupings of mood or anxiety disorders, psychotic disorders, substance use disorders, and personality disorders were created based on definitions used in previous studies (see Supplemental Table A1). 49 Hospitalized suicide attempts were also included in the mental disorder cohort. A referent no mental disorder group was created by removing all individuals in the cohort with any ICD-10-CA or ICD-9-CM diagnosis of a mental or behavioral disorder or hospitalization for attempted suicide (see Figure 1).
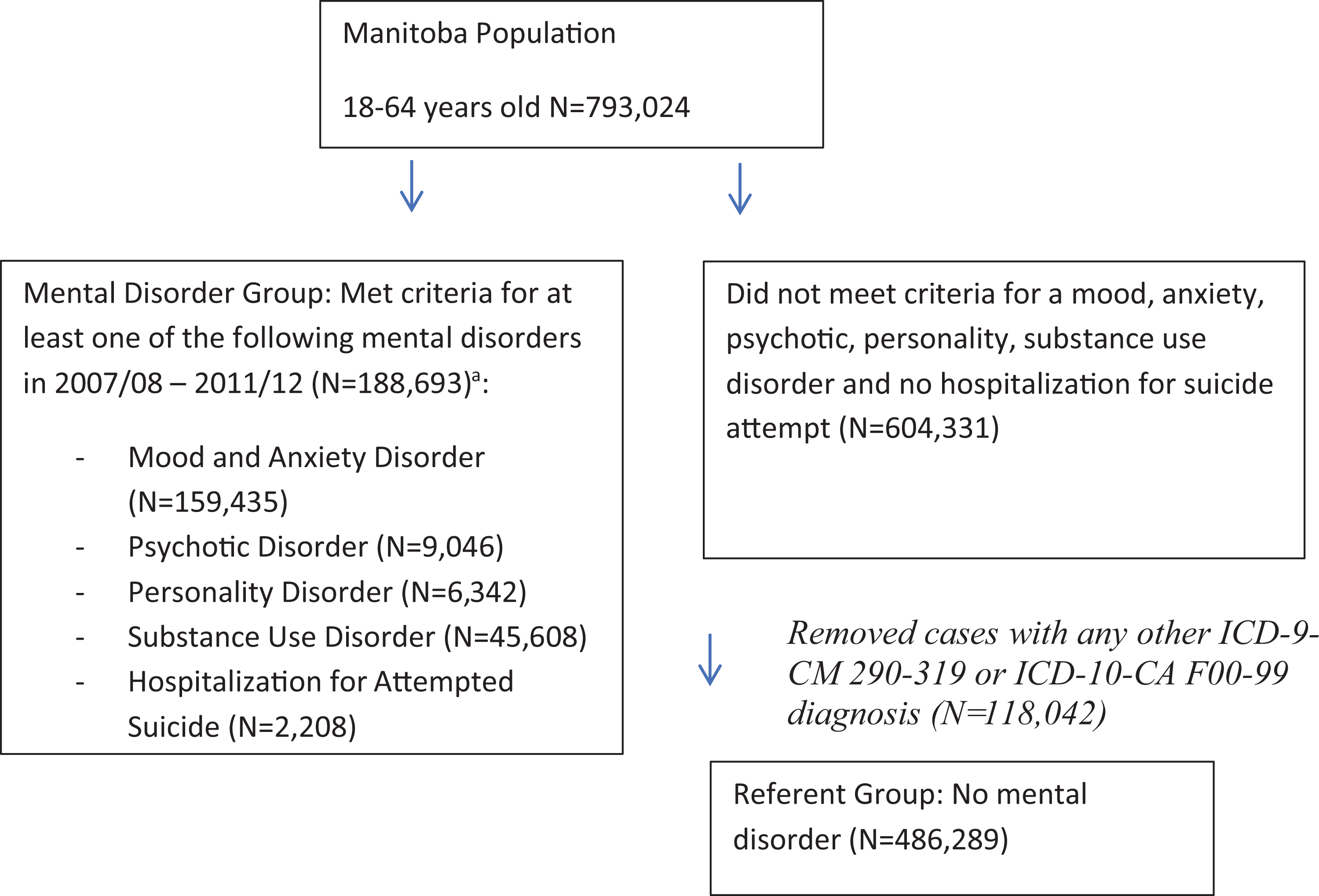
Creation of the study sample. ICD-9-CM = International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10-CA = International Classification of Diseases, 10th Edition, Canada. aDisorders are not mutually exclusive.
Criminal Justice Involvement
We coded all criminal accusations and victimization reports between April 1, 2011, and March 31, 2012. Criminal accusations were defined as charges laid down by police and tracked by Manitoba Justice’s Prosecution Information and Scheduling Management database, including administrative crimes, drug-related crimes, crimes against person or property, assaults, sexual and violent crimes, that may or may not lead to conviction. Victimization included incidents where a formal report was filed with law enforcement by or on behalf of a victim across the same range of charges as those captured for criminal accusations. Criminal accusations and victimization reports were tracked in the PRISM prosecutions database. We also coded whether or not the accusation was violent, inclusive of assault, sexual, and other violent crimes (see Supplemental Table B1).
Statistical Analysis
We descriptively analyzed age, sex, area-level income, and presence of a substance use disorder in all mental disorder groups and the referent no mental disorder group. For each mental disorder group, variables were compared to the referent group with independent t tests or χ2 tests of independence, as applicable. We examined the proportion and per-person rates of criminal justice involvement (both criminal accusation and victimization separately) in the 2011/2012 fiscal year across mental disorder diagnostic groups, each compared to the no mental disorder reference group with crude relative risks. We examined the total number of accusations and reports of victimization per individual. We also calculated relative risks adjusted for age, sex, income, and presence of a comorbid substance use disorder, given the known associations between these factors and criminal activity. 50 –52 We created a Venn diagram of criminal accusations, victimization, and mental disorder to examine the overlap between these variables. We then compared the presence or absence of both victimization and mental disorder among those with a criminal accusation with a χ2 test of independence. This illustrated an additional vulnerability for criminal justice involvement in the presence of both a mental disorder and victimization.
Results
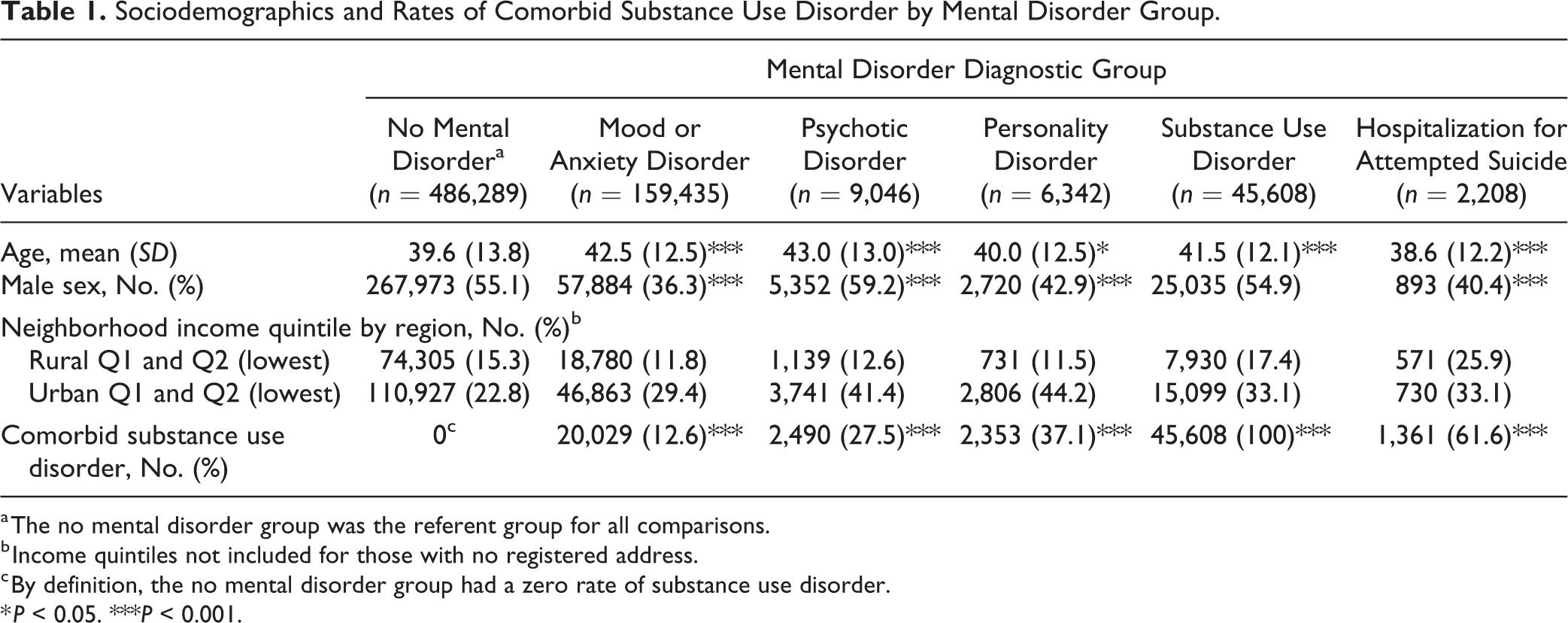
Over the 5-year time frame, 188,693 (23.8%) people had a diagnosed mental disorder, including mood and anxiety disorders (n = 159,435; 20.1%), psychotic disorders (n = 9,046; 1.1%), personality disorders (n = 6,342; 0.8%), and substance use disorders (n = 45,608; 5.8%; Table 1). Men had a greater proportion of psychotic disorders (59.2%) and substance use disorders (54.9%), whereas women had a greater proportion of mood or anxiety disorders (63.7%), personality disorders (57.1%), and hospitalizations for attempted suicide (59.6%). In our sample, the mean age of those with a mental disorder diagnosis (excluding attempted suicide) ranged from 40.0 to 42.5 years, while the mean age of those with no disorder was 39.6 years. Those with suicide attempts were on average the youngest subgroup with a mean age of 38.6 years. Those with a mental disorder, most notably, a psychotic or personality disorder, frequently lived in urban, low-income neighborhoods.
Sociodemographics and Rates of Comorbid Substance Use Disorder by Mental Disorder Group.
a The no mental disorder group was the referent group for all comparisons.
b Income quintiles not included for those with no registered address.
c By definition, the no mental disorder group had a zero rate of substance use disorder.
* P < 0.05. ***P < 0.001.
At the population level, there were between-group differences in age, gender, income distribution, and presence of a substance use disorder consistent with previous literature, 50 –52 justifying the inclusion of these variables as covariates in all analyses (see Table 1). Substance use disorder comorbidity ranged from 13% (mood and anxiety disorders) to 62% (individuals who had attempted suicide).
Risk of Criminal Accusations and Victimization
Between April 1, 2011, and March 31, 2012, 2.4% of those without a mental disorder had at least one criminal accusation (see Table 2). Rate of criminal accusations among individuals with mental disorders ranged from 4% to 15.2%. The total number of accusations per individual among those with at least one accusation was significantly higher in those with a diagnosed mental disorder. Depending on the diagnosis, and after adjusting for age, sex, income, and substance use disorder, those with a diagnosed mental disorder were 2.14 (mood and anxiety disorder) to 4.81 (hospitalized for attempted suicide) times more likely to be accused of a crime compared to those without any mental disorder. Among those accused at least once, those with a diagnosed mental disorder had 15% to 38% higher per-person rates of accusations than those without. Those individuals who had attempted suicide had the highest proportion of criminal accusations (15.2%) over the 1-year time frame.
Crude Rate, Relative Risk, and Adjusted Relative Risk for Accusations of Crime and Victimization across Mental Disorder Groups.
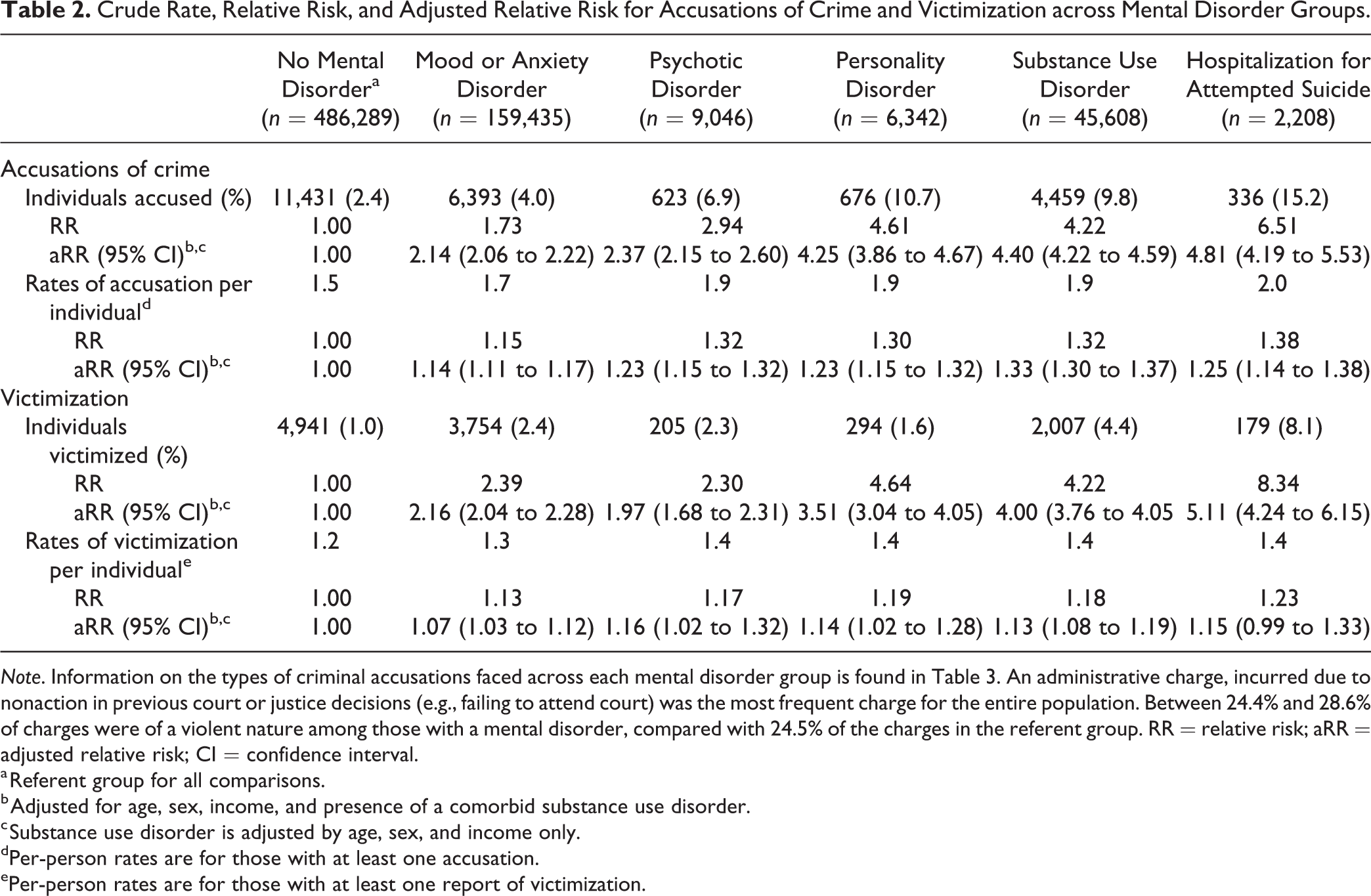
Note. Information on the types of criminal accusations faced across each mental disorder group is found in Table 3. An administrative charge, incurred due to nonaction in previous court or justice decisions (e.g., failing to attend court) was the most frequent charge for the entire population. Between 24.4% and 28.6% of charges were of a violent nature among those with a mental disorder, compared with 24.5% of the charges in the referent group. RR = relative risk; aRR = adjusted relative risk; CI = confidence interval.
a Referent group for all comparisons.
b Adjusted for age, sex, income, and presence of a comorbid substance use disorder.
c Substance use disorder is adjusted by age, sex, and income only.
dPer-person rates are for those with at least one accusation.
ePer-person rates are for those with at least one report of victimization.
Categories of Criminal Charges.
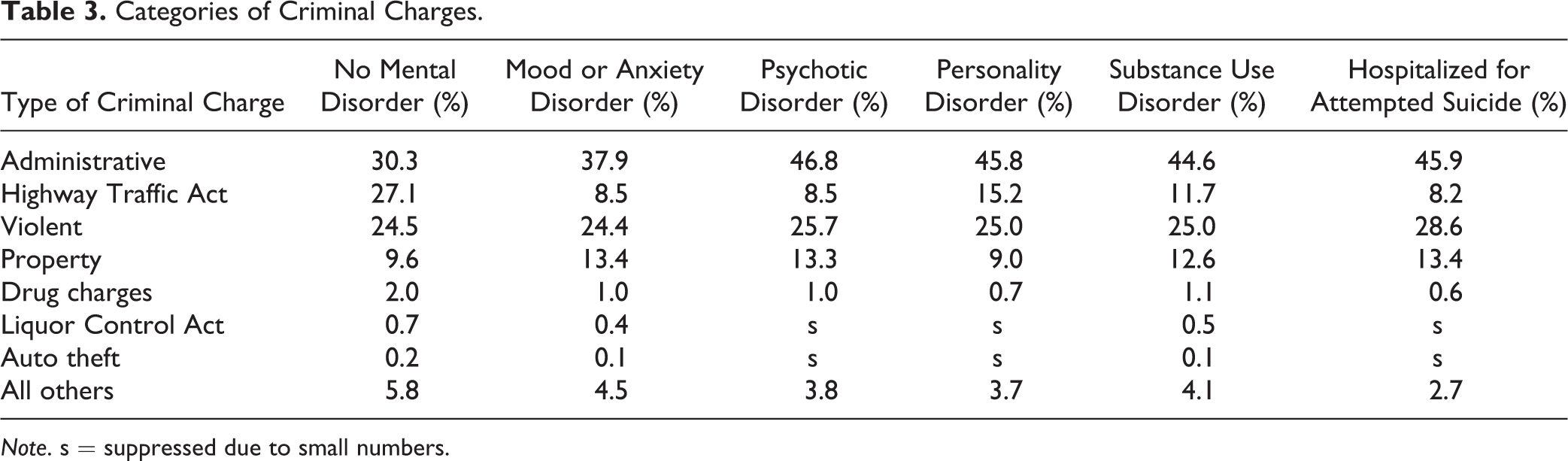
Note. s = suppressed due to small numbers.
A similar pattern of findings was observed for rates of victimization. Although only 1% of those without a mental disorder were victims of crime, up to 4.4% of those with a mental disorder filed a complaint of victimization with police services. The adjusted relative risk for any victimization varied from 1.97 (psychotic disorder) to 5.11 (history of attempted suicide). The per-person rates of victimization for those who were a victim of any crime were 13-23% higher compared to those with no mental disorder. Adults who had attempted suicide reported victimization more frequently (8.1%) compared to other mental disorder groups (1.6-4.4%).
Information on the types of criminal accusations faced across each mental disorder group is found in Table 3. An administrative charge, incurred due to non-action in previous court or justice decisions (eg. failing to attend court), was the most frequent charge for the entire population. Between 24.4-28.6% of charges were of a violent nature among those with a mental disorder, compared with 24.5% of the charges in the referent group.
Figure 2 is a Venn diagram of intersecting vulnerability between diagnosed mental disorder, criminal accusations, and victimization. The majority (93.6%) of individuals with a mental disorder did not have justice involvement of any kind. Among those with a criminal accusation and no mental disorder (n = 11,431), 738 (6.5%) experienced same-year victimization. Among those with a criminal accusation who did have a mental disorder (n = 8,575), 1,064 (12.4%) experienced same-year victimization. The presence of a mental disorder significantly increased the risk of experiencing criminal accusations and victimization concurrently.
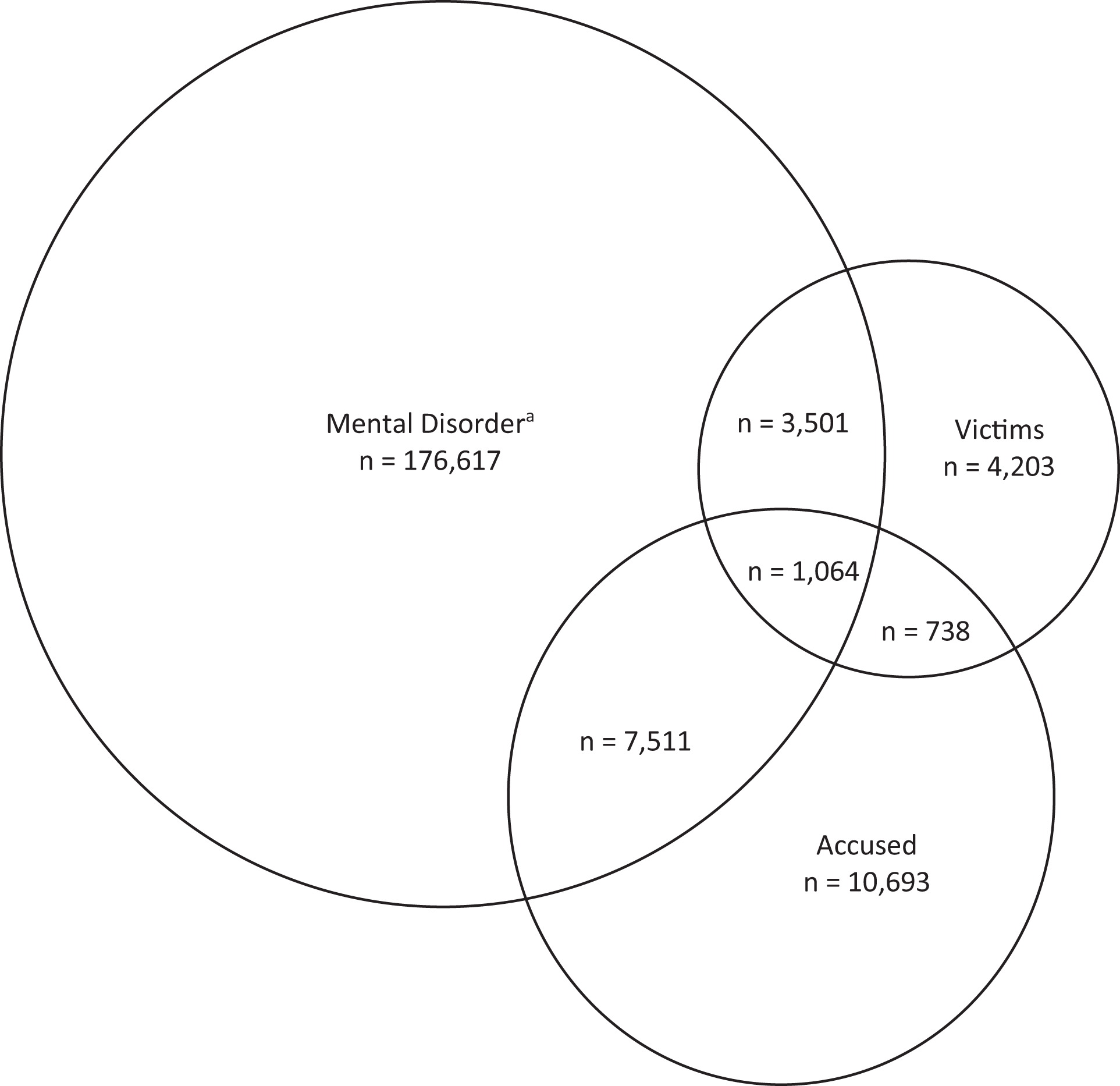
Intersection of diagnosed mental disorders, criminal accusation, and victimization. Total diagnosed mental disorder: 188,693. Total accused: 20,006. Total victims: 9,506. aMental disorder includes mood or anxiety disorder, psychotic disorder, substance use disorder, personality disorder, or history of suicide attempt diagnosed between April 1, 2007, and March 31, 2012. Accusations and victimization occurred between April 1, 2011, and March 31, 2012. The population excludes residents of Manitoba who had any other mental disorder not listed above (n = 118,042), regardless of whether those individuals were accused or victims. Schematic is proportionally representative but not 100% to scale.
Discussion
This large, population-level study is the first of its kind to use administrative data to examine both accusations of crime and victimization among a representative cohort of people with diagnosed mental disorders. Across the mental disorder diagnostic categories, the relative risk of either a criminal accusation or victimization in a 1-year time period, after adjusting for demographics and presence of a substance use disorder, remained 2 to 5 times higher than the general population without mental disorder. The proportion of accusations that were violent in nature was comparable across groups. There was an overlap between accusations and victimization, supporting the view of intersecting vulnerabilities. In all cases, those with diagnosed mental disorders had significantly more interaction with justice, either as an accused person or as a victim.
A substantial contribution to the literature derived from this study is knowledge about the impact of mental disorder on crime while controlling for sociodemographic factors and substance use disorders, the latter of which has been suggested as the main cause for criminal activity among the mentally ill. 53 –55 We found that even after adjusting for these factors, the presence of a mental disorder remained significantly associated with criminal accusations, akin to a Swedish cohort study that exclusively examined prisoners. 56 Although individuals with mental disorders had more criminal accusations when viewed as a group, their per-person rates did not vary as widely when compared to those without mental disorder. Mental disorder is a risk factor, but there are still likely important individual-level factors that lead to repeat offending. For example, criminal justice system involvement can exacerbate social marginalization, along with disrupting treatment and linkage to service systems. 57,58 A highlight from this study includes the remarkably high proportion of accused individuals with a history of attempted suicide who had an accusation of violence; this supports previous literature describing aggression among people who attempt and die by suicide. 59 –61 More research is required to determine how addressing these challenges, particularly with the advent of newer mental health diversion programs, will impact judicial involvement.
We also found a significantly increased risk of victimization among those with a diagnosed mental disorder. Other studies have found similar associations between mental disorder and victimization, 17 –20 though they have not examined the additional impact of criminal accusations. Our rates of victimization were lower than those reported among samples of psychiatric inpatients or outpatients using interview methods, 17 likely owing to the general underreporting of crime to law enforcement. 62 –64 Consistent with other work, we did observe a significant overlap between criminal accusation, mental disorder, and victimization. 17 –20,65 Only a small subset of the population had criminal accusations, and people were more likely to have a mental disorder than criminal justice involvement.
Several limitations are noted in this study. Victimization required an individual to file a claim with law enforcement, which is subject to underreporting. 62 –64 Similarly, diagnoses were dependent on hospital or physician care, which would likely lead to an underestimation of some disorders. 66 Health care in Canada is universal; findings from this study may not be generalizable to other countries. This study examined a 1-year time frame for justice involvement; longer observation may reveal higher rates of overlap between those who move between mental health and legal systems. The administrative health database did not include data for individuals who were in federal custody. However, only a minority of accused are incarcerated and incarceration periods are generally short. For example, in 2015/2016, 60% of remanded accused in Canada were in custody for 1 month or less and among those sentenced, 60% left within 1 month. 67 This study did not determine cause and effect, and as such, it is important to caution any misled inferences suggesting that mental disorders lead to criminal behavior. Our study demonstrated that a greater proportion of individuals with mental disorder lived in poor, urban areas, which are factors linked in and of themselves to encounters with justice either as a victim or as a perpetrator of crime. 68 –74 The associations between victimization, criminality, substance misuse, and low socioeconomic status suggest a disadvantaged lifestyle in which a person with mental disorder faces many adversities. Future directions could include an identification of particularly vulnerable subgroups in the population and exploration of how the quality and utilization of healthcare and reintegration services impact future involvement in criminal justice.
Of particular note, we were not able to identify the ethnicity of participants, which may be a component of the relationship between justice involvement and mental disorder. Martin et al. 75 remarked on racial differences in access to treatment among Canadian prisoners. Although Indigenous people make up only 18% of Manitoba’s population, they represent 74% of adults in provincial correctional facilities. 76 Indigenous inmates have been found to have elevated rates and severity of mental health symptoms. 77 Given that the proportion of Indigenous inmates has risen in Canada, 23 the identification and treatment of mental disorder among justice-involved individuals is an important step in reducing inequalities between racial groups.
Conclusions
Much attention has been given in the media to the perception of violent crime being perpetuated by persons with mental disorder, 11,78 though it has been argued that victimization among the mentally ill is a greater societal concern. 24 Our study underscored the robust relationship between mental disorders and both criminal accusations and victimization. Correcting public misperceptions of a strong link between mental disorder and interpersonal violence is a key component of the strategy for ending discrimination toward those with mental disorder. 79 Stigma is associated with low treatment rates, discriminatory housing and employment practices, as well as public opposition to the expansion of mental health services. 11,80
There are important intersecting vulnerabilities among those who navigate between mental health and legal systems. Few studies have pulled all of these pieces together in a comprehensive examination of the intersection between mental disorders and justice involvement. The impact of the burden of illness among these multiply-stigmatized individuals behooves us as a society to identify and care for the some of the most marginalized of our citizens.
Supplemental Material
Supplemental_Material - The Intersection between Criminal Accusations, Victimization, and Mental Disorders: A Canadian Population-Based Study
Supplemental_Material for The Intersection between Criminal Accusations, Victimization, and Mental Disorders: A Canadian Population-Based Study by Hygiea Casiano, Jennifer M. Hensel, Mariette J. Chartier, Okechukwu Ekuma, Leonard MacWilliam, Natalie Mota, Chelsey McDougall and James M. Bolton in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
The data used in this study were obtained from linked datasets contained in the Population Health Research Data Repository held at the Manitoba Centre for Health Policy (MCHP) under HIPC Project Number 2015/2016-65. The results and conclusions are those of the authors, and no official endorsement by the MCHP, Manitoba Health, or other data providers is intended or should be inferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.