
Abstract

Keywords
Background
The rate of use of long-acting injectable antipsychotics (LAIAs) was reported to be as low as 6.3% in Canada in 2006 1 compared to rates above 15% reported in 9 other countries. 2 Recommendations of experts from Quebec published in 2011, 3 updated in 2019, 4 and Canadian ones published in 2013 5 called for more proactive use of LAIAs. However, we are unaware of any data on possible changes in LAIA since 2006, 1 and it is thus impossible to determine the impact of the introduction of new second-generation LAIAs (SG-LAIAs) or the publication of experts’ recommendations on the rates of use of LAIAs. Hence, the goal of this article is to examine the evolution of LAIA use in Québec from 2003 until 2017.
Methods
We obtained the total number of antipsychotic prescriptions reimbursed for each month from January 2003 to December 2017 from the IQVIA database, which includes all antipsychotic medication prescriptions covered by the provincial public insurance system that provides drug coverage to more than 90% of people suffering from a psychotic disorder. 6 As this data set does not include any information on the individuals included, we could not compute the rates of use in psychotic disorders per se. Hence, we computed their rate of use per 100,000 people, using demographic numbers from the government of Quebec’s Statistics Institute (http://www.stat.gouv.qc.ca).
Given the period covered by the database, data were available for first-generation (FG) LAIA, Risperdal Consta (introduced in Canada in 2005), Invega Sustenna (2011), and Abilify Maintena (2014) but not Invega Trinza (2016). We did not assess the proportion of all antipsychotics prescribed that are LAIAs since this proportion would be very sensitive to changes in off-label use of oral antipsychotics.
Results
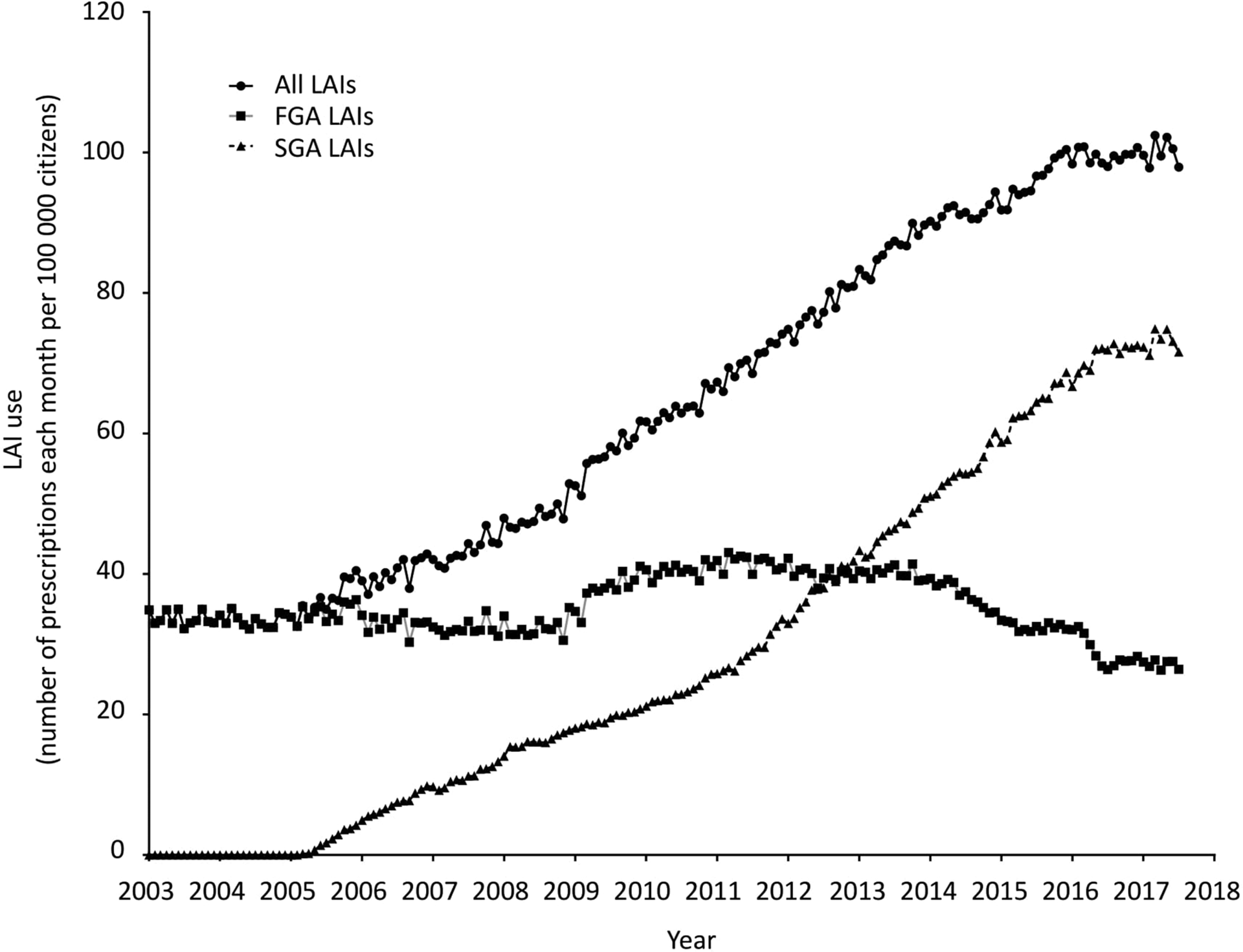
Figure 1 shows that over the studied period, the rate of use of LAIAs was multiplied by 3.07 going from 32.4/100,000 in 2003 to 99.6/100,000 in 2017. The use of FG-LAIAs decreased from 33.6/100,000 in 2003 to 24.5/100,000 in 2017. The use of SG-LAIAs, first introduced in 2003, reached 75.1/100,000 in 2017. Figure 1 shows that changes in rates started in 2004, a few months after the introduction of the first SG-LAIA, and increased in a linear pattern over the period of the study, without any significant inflection point.
Discussion
LAIA use in Québec has increased steadily since 2004, which coincides with the introduction of the first SG-LAIA. This supports the hypothesis that the previously reported modest rates of use of LAIAs might have resulted from the fact that only FGAs were available in the LAIA form while SGAs had become the mainstay in treating psychotic disorders. We did not observe further increases co-occurring with the publication of expert recommendations, although such an effect cannot be ruled out since they coincided with novel LAIA introduction. A study looking at the French public health insurance database also reported an increase in LAI use over a similar period of time, doubling from 2007 to 2014 7 which also resulted from increased use of SG-LAIAs as FG-LAIAs used remained stable during that period. The fact that comparable data were not available in provinces other than Québec precluded comparisons across Canada.
These conclusions must consider that the lack of diagnostic information prevents assessing the extent to which the increased use observed might apply to people suffering from a psychotic disorder versus variations in off-label use, such as maintenance treatment of bipolar disorder, although informal discussions with psychiatrists across Québec suggest that off-label LAIA use remained relatively rare in our population over the observation period. To address such a possibility, we examined an alternative, that is, that off-label use did not occur at the beginning of the period and that it raised up to 30% of LAIAs received at the end. We had to rely on such as an arbitrary value since there is available evidence for both an increase 8 and a decrease 9 in the proportion of antipsychotics that are prescribed off-label and because we could not find any data of LAIA. Hence, this proportion of 30% was chosen to represent a fairly extreme scenario thereby providing a very conservative estimate of the rate of increase in LAIA use in psychotic disorder. Under this stringent scenario, the use of LAIAs would have increased from 32.4/100,000 up to 69.7/100,00%, still representing a 2.15-fold increase. Hence, variations in off-label use of LAIA cannot fully account for the observed increased use of LAIA. Also, since the lack of any demographic information prevents assessing the extent to which the same people received LAIAs over successive months, it is not possible to assess the exact number of people using LAIAs in a given year. However, this latter limitation is an unlikely explanation for the increased LAIA use observed since there is no reason to believe that this phenomenon varied significantly over the study period.
The contrasts across countries in rates of LAIAs use and differences in the evolution of these rates further underline that several factors may influence this use. A better understanding of these factors may guide their optimal use, and this report shows that pharmacoepidemiological studies using large data sets may shed light on some of these factors.
Footnotes
Acknowledgments
The author thanks Mr. Antoine Lampron, PhD, for his assistance with this work.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Roy has received honoraria, grants, or research contracts from Janssen-Ortho, Mylan and Otsuka-Lundbeck.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Janssen-Ortho paid the access to the IQVIA database.