
Abstract
Objectives:
Compelling animal data exists examining the impact of the gut microbiome on the brain, but work is required to translate these findings in a clinical population. We sought to do this by exploring the effects of antidepressant medications on the gut microbiota, and establishing a baseline Major Depressive Disorder (MDD) gut phenotype.
Methods:
Participants with a primary diagnosis of MDD (n = 15) who were nonmedicated were recruited and followed over 6 months. Stool samples were collected prior to treatment initiation and 3 and 6 months following treatment. 16S rRNA sequencing was employed in order to analyze the gut microbial community profile. Symptom severity was measured by the Beck Depression Inventory. Alpha diversity metrics revealed no significant difference in the community diversity across any of the time-points.
Results:
Comparison of within-group versus between-group distances revealed a lack of clustering of samples based on time-point, suggesting no significant change in the microbiota across treatment duration. When analyzed based on treatment response, however, patients in the responder group exhibited greater phylogenetic diversity than non-responders (Mann-Whitney U = 5, p = 0.026). At 3-months, 35 Operational Taxonomic Units (OTUs) were significantly different between groups and at 6-months, 42 OTUs were significantly different between responders and non-responders.
Conclusions:
These observations indicate that antidepressant medications alter the gut microbiota of patients with MDD, with disparate effects in responders versus non responders. This supports the concept of a microbiota phenotype associate with treatment response in MDD.
Recent interest has focused on interactions between the microbiota and the central nervous system (microbiota–gut–brain axis) and its influence on mental illness, 1 –3 highlighting the important role of bacteria in bidirectional communication with the brain. This area of investigation may provide new insights into the cause and treatment of mental illness.
We therefore proposed to conduct the first longitudinal investigation of a possible link between major depressive disorder (MDD) and the gut microbiome by examining microbial patterns prior to the initiation of antidepressant pharmacotherapy and over 6 months of therapy. No other work has examined the microbiota in a population free of antidepressant use.
Methods
Participants were between 18 and 60 years of age with MDD as confirmed by the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID) and moderate depression as indicated by a Montgomery–Åsberg Depression Rating Scale (MADRS) score of >19. Exclusion criteria included psychiatric medication use (other than sedatives for sleep and benzodiazepines) at minimum 1 week prior to visit 1, medical conditions or current use of medications or natural health products known to impact the microbiota, and current substance abuse. After the screening visit, participants were given a 3-day food diary that was returned prior to the baseline visit and repeated at 3- and 6-month assessments. Anthropomorphic measurements (height, weight, and waist circumference) were also completed, and the MADRS administered, at the same time points. Participants then initiated therapy with Citalopram or Escitalopram.
Participants were given stool collection kits and provided samples at baseline and 3- and 6-month assessments. Specimens were stored at −80°C. Bacterial community profiling using 16S rRNA gene sequencing was carried out using a modified bar-coded Illumina sequencing method. 4 Using data rarefied in QIIME at the lowest sequencing depth, phylogenetic diversity was analyzed. For beta diversity, Jackknife resampling was used to generate Bray–Curtis distances. To identify differentially abundant operational taxonomic units (OTUs), OTUs not observed in 75% of samples were eliminated, and the data set was analyzed using DESeq2 and Benjamini–Hochberg.
Results
Fifteen participants (mean age = 36.9, SD = 12.9; 12 women) were studied. The average baseline MADRS score was 22.53 (SD = 6.63). At 6 months, 11 participants were classified as remitters (MADRS
Remitters exhibited greater diversity at baseline than nonremitters (Figure 1; Mann–Whitney U = 5, P = 0.026). Bray–Curtis distances revealed no differences in variability (Mann–Whitney U = 138, P = 0.517) and a lack of community clustering based upon eventual treatment response (PERMANOVA; F = 0.720, P = 0.824). At baseline, 22 OTUs were differentially abundant between the remitter and nonremitter groups.
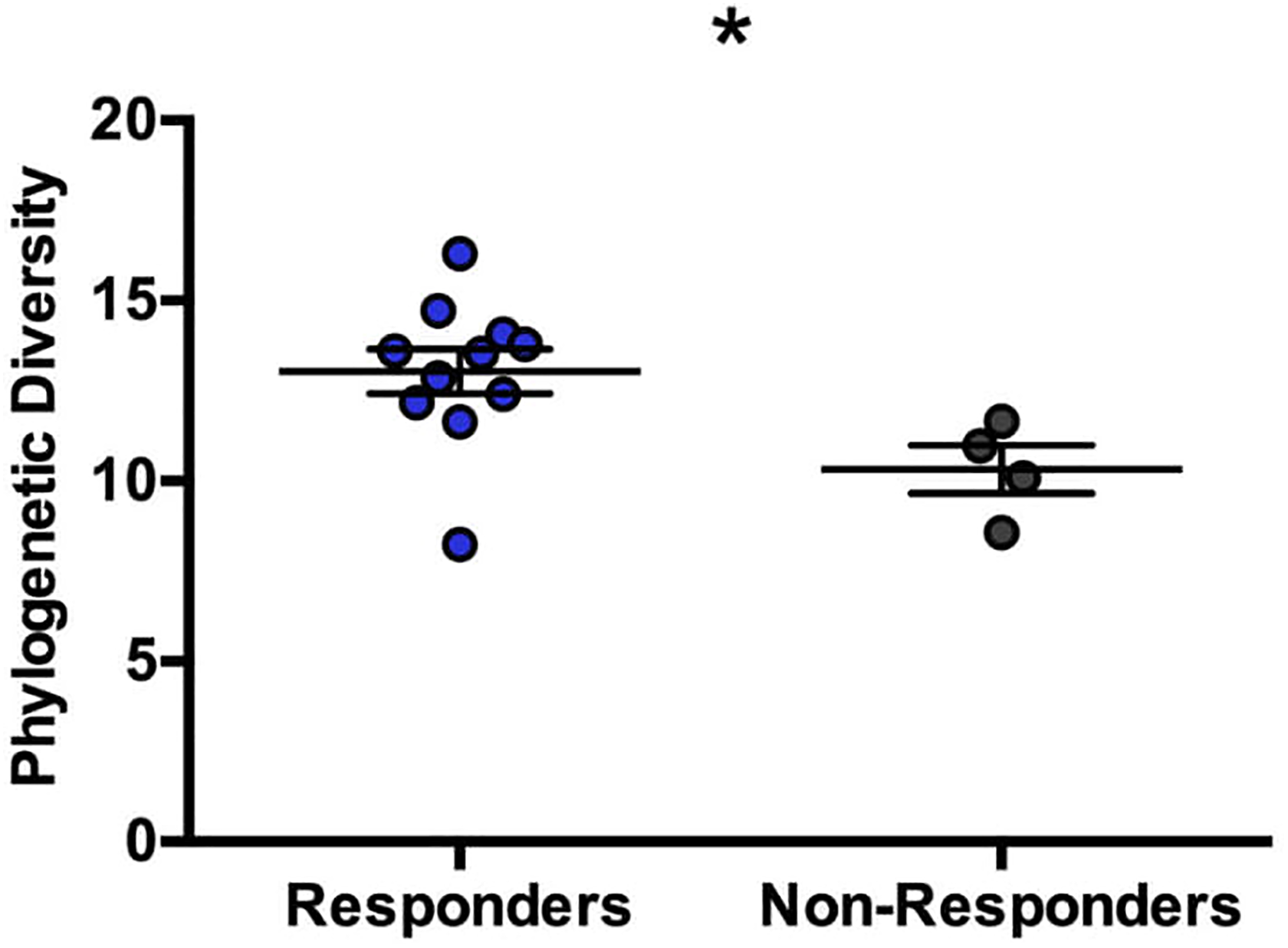
Baseline differences between eventual responders and nonresponders in alpha-diversity metrics. Source: Faith’s Phylogenetic Diversity: 3703 reads/sample.
Comparisons at 3- and 6-months following treatment showed no change in diversity in remitter or nonremitters. Differences in diversity between groups were no longer significant at 3 months but were again significant at 6 months (F 1, 13 = 4.773, P = 0.048, post hoc P < 0.05). Analysis of the composition in remitters showed no clustering by time point (PERMANOVA; F = 0.262, P = ∼1) and no changes in within-subject distances (Friedman statistic = 0.546, P = 0.844). Similarly, nonremitters showed no clustering of the community across treatment (PERMANOVA; F = 0.433, P = 0.951) or changes in within-subject distances (Friedman statistic = 3.50, P = 0.273).
Next, we examined whether specific OTUs were altered after treatment. In remitters, a single OTU was altered—a Clostridiales, elevated at 6 months. No OTUs were altered in nonremitters. At 3 months, 35 OTUs were significantly different between remitters and nonremitters but 16 were no longer different by the 6-month time point. At 6 months, 42 OTUs were different between groups: 23 were unique while the remaining 19 were also differentially abundant at 3 months. There was no impact of dietary composition as analyzed by Nutritionist Pro diet analysis software or antidepressant exposure.
Discussion
Our findings indicate that antidepressant treatment affects the microbiota of MDD patients at the OTU level, based on response to treatment. Assessment at 3 and 6 months following treatment revealed no changes to the diversity or profile of the community relative to baseline, which is consistent with previous work demonstrating the lack of effects of antidepressant medications on bacterial taxa. 5
It was therefore interesting that notable differences in the microbial community were observed in analyses based on treatment response. Despite similar baseline depression severity scores, nonremitters exhibited lower diversity prior to treatment initiation (Figure 1). Additionally, 22 microbial groups were differentially abundant between response groups. Our data provide compelling preliminary evidence that baseline differences in the microbiota may be correlated with antidepressant medication efficacy.
To further examine the impact of antidepressant medications, we compared changes in the microbiota in remitters and nonremitters across 6 months of treatment. There was no change in diversity or overall profile in either response group, paralleling our findings of limited community-wide changes. However, baseline differences between remitters and nonremitters were still evident after 6 months of treatment: Remitters continued to exhibit greater diversity. These observations further suggest a microbial community signature distinguishing treatment response groups.
Conclusion
Our data indicate antidepressant medications may alter the gut microbiota of patients with MDD and outline the disparate nature of their effects in remitters versus nonremitters. Limitations include the small sample size and the lack of a placebo control. Larger studies are needed to investigate whether the gut microbiome may serve as a potential biomarker to aid in guiding treatment.
Supplemental Material
Supplemental Material, 19040-a-CJP-2019-186-RL.R1-abstarct_for_translation - Gut Microbiome Patterns Associated With Treatment Response in Patients With Major Depressive Disorder
Supplemental Material, 19040-a-CJP-2019-186-RL.R1-abstarct_for_translation for Gut Microbiome Patterns Associated With Treatment Response in Patients With Major Depressive Disorder by Aadil Bharwani, Asem Bala, Michael Surette, John Bienenstock, Simone N. Vigod and Valerie H. Taylor in The Canadian Journal of Psychiatry
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VT and JB received support for this study from McMaster University and the University of Waterloo. AB gratefully acknowledges funding support from the Canadian Institutes of Health Research (GSD-148222) and an MD/PhD student award from The Research Institute of St. Joe’s Hamilton. MGS is supported by a Canada Research Chair.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.