
Abstract
Objectives:
Chronic pain and generalized anxiety disorder (GAD) are co-occurring, and both conditions are independently associated with substance misuse. However, limited research has examined the impact of comorbid GAD and chronic pain on substance misuse. The aim of this article was to examine the associations between comorbid GAD and chronic pain conditions compared to GAD only with nonmedical opioid use, drug abuse/dependence, and alcohol abuse/dependence in a Canadian, population-based sample.
Methods:
Data came from the 2012 Canadian Community Health Survey–Mental Health (N = 25,113). Multiple logistic regressions assessed the associations between comorbid GAD and chronic pain conditions (migraine, back pain, and arthritis) on substance misuse.
Results:
Comorbid GAD + back pain and GAD + migraine were associated with increased odds of nonmedical opioid use compared to GAD only. However, the relationship was no longer significant after controlling for additional chronic pain conditions. No significant relationship was found between GAD + chronic pain conditions with drug or alcohol abuse/dependence.
Conclusions:
Comorbid GAD + back pain and GAD + migraine have a unique association with nonmedical opioid use in Canadians compared to GAD only, and chronic pain multimorbidity may be driving this relationship. Results emphasize the need for screening for substance misuse and prescription access in the context of GAD and comorbid chronic pain.
Every year, approximately 100 million Americans and 7.5 million Canadians experience chronic pain. 1,2 Chronic pain is a complex phenomenon 3 and is associated with negative health sequelae such as emotional distress, decreased functioning, and suicide. 4 Chronic pain is often comorbid with a number of psychiatric conditions, 5 –7 with many individuals misusing substances, 8 –10 with growing recognition given the current opioid epidemic. 11,12
The association between chronic pain and psychiatric disorders is associated with greater pain symptom severity and poorer overall well-being. 7,13 –15 Much of this research has focused on the relationship between chronic pain and depression. 7 However, chronic pain and anxiety are also highly comorbid, 5,6,16 with rates of anxiety disorders as high as 60% in chronic pain samples. 17 –19 It has also been found that anxiety is more predictive of incident pain than depression. 20 Chronic pain and anxiety disorders share a number of cognitive features, including attentional biases and catastrophizing, 21,22 which is consistent with the shared vulnerability framework used to understand the comorbidity. 5,6
Particular attention has been paid to the comorbidity of chronic pain with phobias and trauma-related conditions; 5,6,23 however, research also suggests the importance of generalized anxiety disorder (GAD) in the experience of chronic pain. 16 GAD is characterized by pervasive worry over a number of events and activities including work, relationships, and health. 24 GAD is prevalent in North America, with estimates of 5.7% in the United States 25 and 2.6% in Canada. 13 GAD shares features with chronic pain including muscle tension, fatigue, and attentional biases. 26 However, there have been limited examinations of the relationship between GAD and chronic pain, and correlates of this comorbidity. Two recent studies by our group examined the negative health correlates associated with comorbid GAD and chronic pain. 13,27 We found that GAD in the context of chronic pain was associated with increased pain severity and disability compared to the pain condition alone 13 and that comorbidity was associated with increased suicidality compared to GAD only. 27
Research indicates that both individuals with GAD and chronic pain have elevated rates of substance misuse, which has been hypothesized as a maladaptive coping strategy. 9,10,28 Opioids are a common treatment approach for chronic pain; 29 however, research suggests that individuals with chronic pain may turn to nonmedical opioids (i.e., opioids without a prescription or misuse of prescription opioids 4 ) and other substances such as illicit drugs (e.g., cocaine, heroin) and alcohol. 8,10 Compared to other anxiety disorders, GAD has been associated with self-medicating alcohol and drug behaviour 30,31 as well as with nonmedical opioids. 32 Previous work has identified that comorbid anxiety symptomatology and chronic pain increase the risk of opioid misuse in American samples; 33,34 however, the impact of comorbid GAD and chronic pain on the risk of nonmedical opioid, alcohol, and illicit drug use is not fully understood in a Canadian population-based context. Little is known about the differences in negative correlates of comorbidity, including substance misuse, according to type of chronic pain condition, and differential relationships have been observed in other outcome research across conditions. 34 Given the increased access of prescription opioids in chronic pain, 29 that prescribing practices of opioids may differ across conditions, and the self-medicating behaviours observed in GAD, 30,31 it is important to understand the impact of having an opioid prescription on the risk of opioid misuse.
Our objective was to examine the associations between comorbid GAD and chronic pain with nonmedical opioid use, drug abuse/dependence, and alcohol abuse/dependence compared to GAD only (i.e., GAD without the chronic pain of interest). We used GAD only as our reference group as this article focused on substance use categories more broadly, and it is well established that GAD has high comorbidity with substance misuse, 9,10,30,31 but it is unclear whether comorbidity with chronic pain impacts rates of substance misuse compared to GAD only. We hypothesized there would be elevated rates of substance misuse for comorbid GAD and chronic pain across nonmedical opioid use, drug abuse/dependence, and alcohol abuse/dependence given that both GAD and chronic pain have been independently shown to be associated with increased risk. We anticipated that having both GAD and chronic pain would be associated with higher odds of substance misuse, compared to GAD only even after controlling for sociodemographics and comorbid psychiatric disorders. Finally, we hypothesized that additional chronic pain conditions (i.e., chronic pain multimorbidity) would impact the association of substance misuse among those with GAD and chronic pain compared to GAD only.
Methods
Sample
Data were drawn from the nationally representative 2012 Canadian Community Health Survey–Mental Health (CCHS-MH; N = 25,113; response rate = 68.9%). The sample is comprised of persons 15 years or older and living in one of the 10 Canadian provinces. Exclusion criteria included those living on Indigenous reserves, institutionalized, full-time members of the Canadian forces, or those without a home (due to the household sampling method used). Individuals who participated completed a comprehensive questionnaire administered by a trained lay-interviewer covering a range of topics including demographics, mental health, physical health, and overall well-being. Additional information about the CCHS-MH methodology can be found elsewhere. 35
Primary Variables
Sociodemographic characteristics
We assessed six sociodemographic characteristics: age (continuous), sex (male, female), race/ethnicity (White, Other), marital status (married/cohabitating, widowed/separated, single), education (high school or less, some postsecondary or higher), and income (less than $60,000, $60,000+). Categorizations were based on prior research; 13 however, ethnicity was collapsed into a dichotomous variable to have sufficient power for analyses.
Psychiatric conditions
Past-year psychiatric diagnoses were established using the World Health Organization Mental Health Composite International Diagnostic Interview, which is a reliable and valid tool to assess psychiatric conditions in population-based samples. 36 These conditions included GAD, mood disorders (depression, bipolar, and hypomania), and substance abuse/dependence that are based on Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) criteria. 24 We used three substance misuse conditions: drug abuse/dependence (i.e., sedatives/tranquilizers, stimulants, marijuana, cocaine, club drugs, hallucinogens, heroin, inhalants, other [e.g., opioids]), alcohol abuse/dependence, and nonmedical opioid use (excluding individuals who endorsed drug abuse/dependence). Participants self-reported whether they used opioids nonmedically (i.e., without the recommendation of a health professional, in greater amounts than a health professional prescribed, or for any other reason other than how a health professional prescribed) in the past year. Based on skip-out patterns in the survey, participants arrived at this question (i.e., assessing past-year nonmedical opioid use) if they (a) responded “yes, more than once” when asked about lifetime nonmedical opioid use” or (b) responded either “no” or “yes, just once” when asked about lifetime nonmedical opioid use AND “yes” when asked whether they ever used a prescribed pain killer AND “yes” when asked whether their opioid prescription use was so regular that they felt they could not stop using it. Participants who responded “no” to either of the prescription-related questions were not asked about past-year nonmedical opioid use. We observed that 24.3% of those in our nonmedical opioid use dependent variable (DV) followed the second path described. Based on the pattern of questioning, not all participants were asked questions about opioid prescription use/misuse. Subsequently, we were unable to clarify whether all individuals who endorsed nonmedical opioid use used a prescription or felt like they were unable to stop using prescribed pain killers.
Chronic pain conditions
Participants self-reported chronic pain conditions and were subsequently asked whether a health professional diagnosed them with the condition that lasted (or was expected to last) at least 6 months. These conditions included arthritis (excluding fibromyalgia), back pain (excluding fibromyalgia and arthritis), and migraine headaches. To assess chronic pain multimorbidity, we computed aggregate variables by summing the chronic pain conditions assessed and combined these variables with GAD, labeled “GAD + 1 chronic pain condition” and “GAD + 2-3 chronic pain conditions.”
Statistical Analyses
Data were analyzed at the Research Data Centre in Winnipeg, Manitoba, Canada, using Stata 14 statistical software. 37 We conducted multiple logistic regression models to examine the contribution of comorbid GAD and chronic pain conditions on nonmedical opioid use, drug abuse/dependence, and alcohol abuse/dependence (as separate DVs). We used each of the three comorbid GAD and chronic pain conditions as separate independent variables (i.e., GAD + arthritis, GAD + migraine, and GAD + back pain) with GAD without the specific chronic pain condition of interest (i.e., GAD only) as the reference group. We ran four models. We ran an unadjusted model, a model adjusting for sociodemographic characteristics (age, sex, race/ethnicity, marital status, education, and income), and a model adjusting for sociodemographic characteristics and other psychiatric conditions (depression, bipolar, hypomania, and drug and alcohol abuse/dependence). In the regression with nonmedical opioid use as the DV, this included controlling for sociodemographic variables, mood disorders, and alcohol abuse/dependence. We did not include drug abuse/dependence as a covariate as the opioid misuse questions were used as part of a diagnosis for drug abuse/dependence. In the regression with drug abuse/dependence as the DV, this included sociodemographic variables, mood disorders, and alcohol abuse/dependence. In the regression with alcohol abuse/dependence as the DV, this included sociodemographic variables, mood disorders, and drug abuse/dependence. The final model adjusted for sociodemographic characteristics, other psychiatric conditions, and other chronic pain conditions, which allowed us to assess and control for the influence of chronic pain multimorbidity on substance misuse among those with GAD and chronic pain compared to GAD only. We obtained weighted sample size estimates and prevalence rates (%), derived odds ratios (ORs) using 95% confidence intervals (CI), and used p values to evaluate significance. Bootstrapping methods were used for variance estimation.
Results
Table 1 displays the sample characteristics. Among the entire sample, 721,668 (2.6%) had a past-year diagnosis of GAD. Among these individuals, 205,239 (28.6%) had arthritis, 198,588 (27.5%) had migraines, and 311,425 (43.2%) had back pain.
Sample Characteristics of Adults with Past-Year GAD.
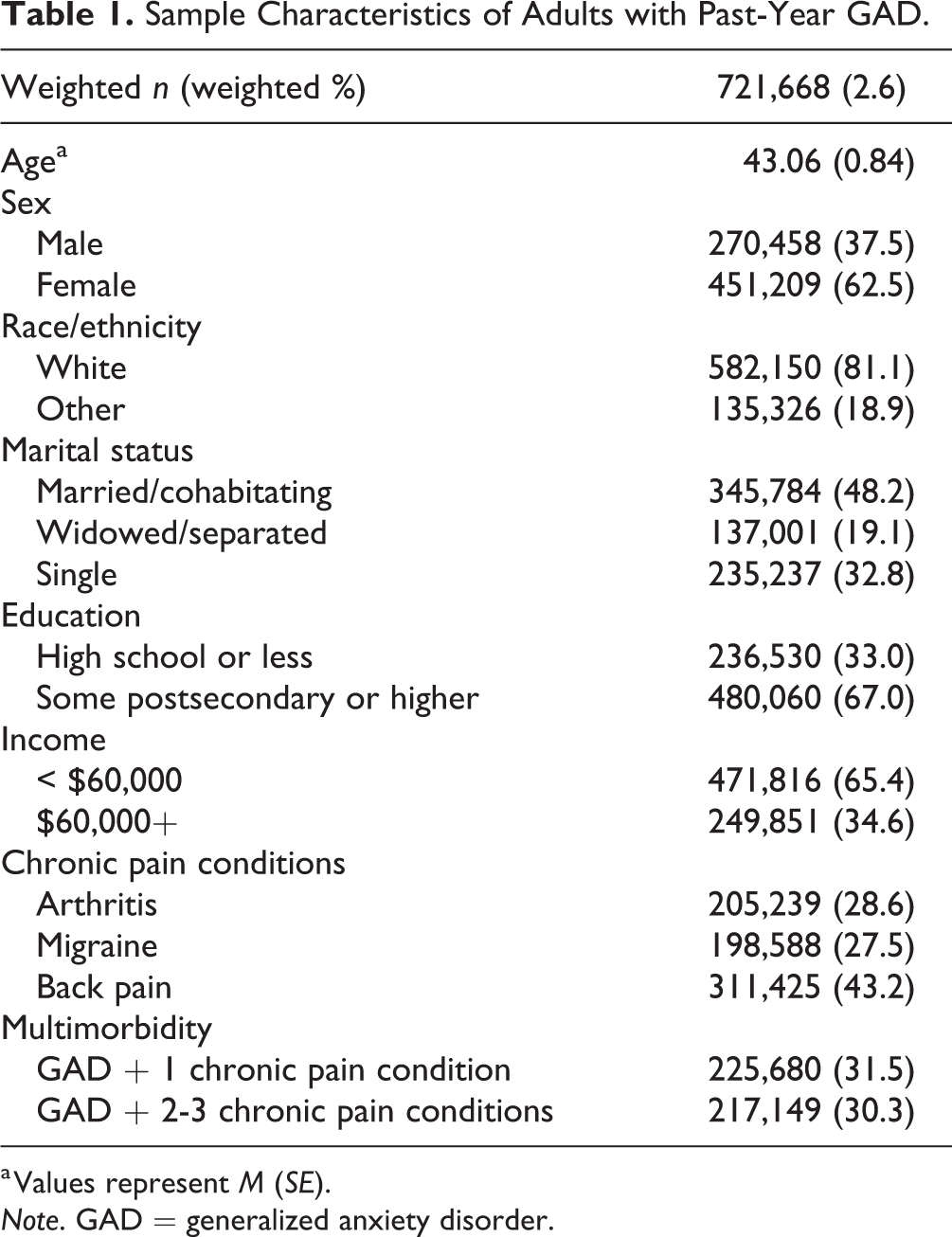
a Values represent M (SE).
Note. GAD = generalized anxiety disorder.
Table 2 displays the results from the logistic regression models. After controlling for sociodemographic characteristics and other psychiatric conditions, those with GAD + migraine (adjusted odds ratio [AOR1]: 2.38; 95% CI, 1.01 to 5.64; p < 0.05) and GAD + back pain (AOR1: 2.22; 95% CI, 1.01, 4.88; p < 0.05) had increased odds of nonmedical opioid use compared to GAD only. There were no associations found for any comorbid GAD and chronic pain condition on the odds of drug abuse/dependence or alcohol abuse/dependence compared to GAD only (AOR1 range: 0.37 to 1.28; 95% CI, 0.09 to 2.50; p > 0.05). In our most stringent model that additionally controlled for other chronic pain conditions (e.g., in the context of arthritis, we controlled for back pain and migraine), we no longer observed significant results for either GAD + migraine (AOR2: 2.22; 95% CI, 0.93 to 5.29; p > 0.05) or GAD + back pain (AOR2: 2.10; 95% CI, 0.92 to 4.80; p > 0.05) compared to GAD only.
Associations between GAD and Chronic Pain Conditions with Substance Misuse, Abuse, and Dependence.
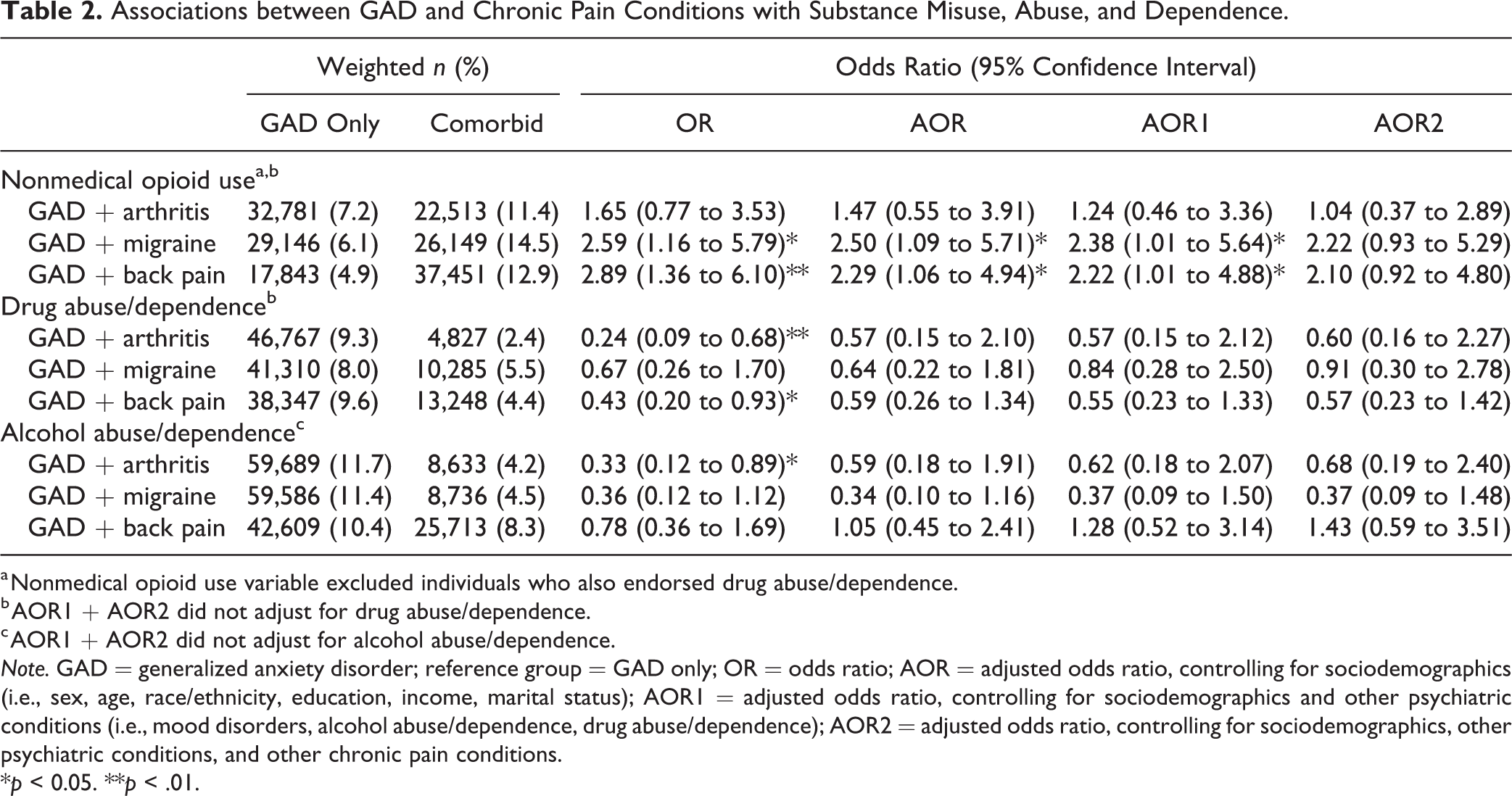
a Nonmedical opioid use variable excluded individuals who also endorsed drug abuse/dependence.
b AOR1 + AOR2 did not adjust for drug abuse/dependence.
c AOR1 + AOR2 did not adjust for alcohol abuse/dependence.
Note. GAD = generalized anxiety disorder; reference group = GAD only; OR = odds ratio; AOR = adjusted odds ratio, controlling for sociodemographics (i.e., sex, age, race/ethnicity, education, income, marital status); AOR1 = adjusted odds ratio, controlling for sociodemographics and other psychiatric conditions (i.e., mood disorders, alcohol abuse/dependence, drug abuse/dependence); AOR2 = adjusted odds ratio, controlling for sociodemographics, other psychiatric conditions, and other chronic pain conditions.
*p < 0.05. **p < .01.
We conducted a post hoc analysis among the conditions significantly associated with nonmedical opioid use in the model adjusting for sociodemographic characteristics and other psychiatric conditions (i.e., migraine and back pain) to assess the proportions of individuals who had access to opioid prescriptions but did not misuse them among those with comorbid GAD + chronic pain compared to chronic pain only. This analysis was assessed among a subset of the sample who were asked about opioid prescription access. We changed the reference group to chronic pain only thinking that those with pain conditions are more likely to have prescription access, and the addition of GAD could result in misuse. We found that those with chronic pain only were more likely to have a prescription for and access to opioids but not misuse their prescription compared to comorbid GAD + chronic pain. Specifically, the prevalence of not misusing prescription opioids was 94.8%, and 93.5% among those with migraine and back pain only, respectively, compared to 81.5%, and 84.0% among those with GAD + migraine and GAD + back pain, respectively.
Discussion
To our knowledge, this is the first study to demonstrate that, compared to GAD only, comorbid GAD + migraine and GAD + back pain are associated with greater odds of nonmedical opioid use in a Canadian populated-based sample. Increased odds of nonmedical opioid use was maintained even after controlling for sociodemographic characteristics and other psychiatric conditions. However, after controlling for additional chronic pain conditions, the relationship between GAD + chronic pain and nonmedical opioid use lost significance, suggesting the relevance of chronic pain multimorbidity for the risk of nonmedical opioid use. Post hoc analyses among a subset of individuals who endorsed nonmedical opioid use and access to prescription revealed that those with migraine or back pain only were more likely to not misuse their prescription opioid compared to those with comorbid GAD and migraine or back pain who were receiving a prescription. Finally, in our adjusted models, the comorbidity between GAD and the assessed chronic pain conditions was not associated with elevated odds of illicit drug or alcohol abuse/dependence when compared to GAD only.
The increased proportion of nonmedical opioid use in comorbid GAD + back pain and/or migraine compared to GAD only may suggest that anxious individuals suffering from chronic back pain and migraines may be more likely to turn to nonmedical opioids or misuse their prescriptions to cope with their conditions. Opioids are a common treatment strategy for chronic pain, particularly for back pain. 38,39 Yet, the evidence of the effectiveness of opioids for back pain is not convincing, 11,38 and recently, there has been growing attention on the opioid crisis in Canada. 12 For example, research has suggested the use of opioids for migraines may actually result in more emergency room visits, as compared to nonopioid treatments. 40,41 Moreover, 60% to 70% of users who started with prescription opioids for pain treatment go on to abuse opioids for nonmedical reasons and report greater physical and mental health problems compared to those who do not abuse opioids. 42 A Canadian population-based study revealed that 58% of drug-related deaths in a 2-year period were attributed to the presence of opioids, 43 placing a huge burden on the public and health-care system. However, the CCHS-MH survey was conducted in 2012, and changes in prescription practices have occurred more recently. Indeed, the 2017 Canadian Guideline on Opioid use suggests, for example, that opioids should only be introduced after unsuccessful nonopioid treatment, and opioids should not be used for individuals with prior history of substance use disorders, 44 which would likely impact the current analyses had they been conducted since the release of these guidelines. In light of the high prevalence of migraine and back pain in the context of GAD and the association with nonmedical opioid use, it is necessary to replicate the current analyses with contemporary data in light of the new opioid practice guidelines.
Interestingly, the largest discrepancy in proportion between nonmedical opioid use was between GAD + migraine and migraine alone. This finding supports our previous work that identified comorbid GAD + migraine, compared to chronic pain only, was associated with the worst profile of pain severity and disability, 13 and, compared to GAD only, greater suicide ideation and plans. 27 It is possible that the presentation of GAD, which can include muscle tension, irritability, and worried thoughts, 26 is similar to the presentation of migraines. It has been suggested that migraines can be an indicator of the presence of GAD. 45,46 Consistent with the shared vulnerability model, it is possible that the overlapping symptomatology between GAD and migraines may make an individual more vulnerable to experience a range of negative sequelae such as nonmedical opioid use, self-medicating behaviour, and disability through symptom exacerbation. 5,6
There was no observed effect for comorbid GAD + arthritis on odds of nonmedical opioid use compared to those with GAD only. Compared to chronic back pain and migraines, arthritis has been conceptualized to have a relatively homogeneous presentation of symptoms. 47 There is a large body of literature that has been dedicated to the treatment of arthritis. Specifically, validated treatments, such as biologics used to target inflammation, have been considered a first-line treatment for patients with arthritis. 48 It is possible that biologics may be used as a treatment strategy prior to the use of opioids for individuals with arthritis resulting in lowered susceptibility of abuse in the context of GAD. It would be interesting for future research to examine the differences in opioid access across physical health conditions to better understand why migraine and back pain seem to exacerbate GAD more so than arthritis.
The current results highlight an important issue: chronic pain multimorbidity. While we did not directly assess chronic pain multimorbidity and the chronic pain conditions assessed in the CCHS-MH were limited, the associations between comorbid GAD + back pain and GAD + migraine on nonmedical opioid use compared to GAD only lost significance after controlling for additional pain conditions. This suggests the presence of multiple chronic pain conditions may be driving the significant relationship between migraine and back pain with comorbid GAD on nonmedical opioid use. Multimorbidity has been found to be associated with reduced quality of life and increased disability, 49,50 which could leave individuals more vulnerable to opioid misuse than if they had one chronic pain condition. However, it is also possible that the reverse directional relationship is true: multimorbidity may increase access to opioids and thus provide more opportunity to abuse or opioid misuse may perpetuate greater morbidity. 51 Given the cross-sectional nature of our design, we are unable to ascertain directionality. However, clinically, our results highlight the importance of screening for multiple chronic pain conditions and targeted, early intervention to attempt to improve overall health and well-being for those with comorbid GAD and chronic pain.
Surprisingly, we did not observe a significant relationship between comorbid GAD and chronic pain on the odds of drug or alcohol abuse/dependence compared to GAD only. This is of interest given existing substance use literature that suggests those with physical health or psychiatric conditions self-medicate. 8,10 GAD has been associated with the highest rate of self-medicating behaviour (35.6%) compared to any other anxiety disorder (21.9%). 52 Although we controlled for drug abuse/dependence, perhaps access to medication, like opioids, reduces the likelihood of other illicit drug or alcohol misuse. To illustrate, research has suggested that individuals with chronic pain are less likely to drink alcohol, especially if they are regular opioid users. 53 It is known that there are polypharmacy effects with mixing opioids and alcohol, and physicians advise against this practice. Further, it has been found that those with chronic migraines were more likely to use pain killers and less likely to turn to alcohol compared to those with tension headaches. 54 Future research is warranted to examine how the access to prescriptions influences self-medicating behaviour in individuals with GAD and comorbid GAD and chronic pain.
Despite these findings, it is important to consider limitations. First, the CCHS-MH is cross-sectional in nature; therefore, we cannot establish causality. Second, the chronic pain conditions were self-reported. It is possible that the reported prevalence rates are an over- or underestimation of the true prevalence of chronic pain. Future research should complete a more comprehensive assessment of chronic pain conditions including validation using medical charts, for example, to eliminate potential reporting bias. Similarly, although we controlled for other chronic pain conditions, we did not comprehensively examine multimorbidity such as including a Charlson comorbidity index. Given the obtained results and the importance of multimorbidity, future research should further examine the role of multimorbidity on the relationship between GAD, chronic pain, and nonmedical opioid use. Third, the CCHS-MH relied on DSM-IV-TR criteria rather than contemporary nomenclature. Although the criteria for GAD remained relatively consistent, the diagnostic criteria for substance use disorders changed. Research has suggested that there have been discrepant prevalence rates of substance use disorders from DSM-IV to DSM-5 criteria. 55 Fourth, the CCHS-MH did not comprehensively assess for opioid abuse/dependence directly, as it was included within “other drug abuse/dependence,” but the specific drug of interest could not be identified. Similarly, opioid prescription access could only be assessed for certain individuals based on their responses to other questions. Although we conducted preliminary analyses among a subset of participants, it would be important for future research to conduct a more fulsome analysis, given the initial, yet cautious findings discussed here. It would also be interesting to determine whether similar results are obtained using contemporary diagnostic criteria, with particular attention on opioid misuse and abuse/dependence. Fifth, a limited number of psychiatric disorders were used in the present study. It is possible that some of the unassessed conditions may have an impact on the results we observed. Finally, the exclusion criteria for the study may limit the generalizability of the current findings. Results may not capture the most severe presentations of conditions as a result of excluding those who are institutionalized.
Our study reveals that comorbid GAD and chronic pain conditions, specifically migraines and back pain, are associated with increased risk of nonmedical opioid use in a large, population-based Canadian sample compared to GAD only. The results suggest that chronic pain multimorbidity may be driving the relationship between comorbid GAD + migraine or back pain and nonmedical opioid use. Given the opioid epidemic in Canada, this work highlights the importance of screening for multiple chronic conditions, particularly as it relates to opioid misuse.
Footnotes
Acknowledgments
We would like to thank our patient partner, Janet Gunderson, from the Strategy for Patient-Oriented Research (SPOR) Chronic Pain Network.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. El-Gabalawy reports grants from CIHR (SPOR) Chronic Pain Network, during the conduct of the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Canadian Institutes of Health Research (SPOR) Chronic Pain Network operating grant (grant number: 320095 340100 2000) and University of Manitoba Start-Up Funding (El-Gabalawy).