
Abstract
Introduction:
Over the last 30 years, early intervention services (EIS) for first-episode psychosis (FEP) were gradually implemented in the province of Quebec. Such implementation occurred without provincial standards/guidelines and policy commitment to EIS until 2017. Although the literature highlights essential elements for EIS, studies conducted elsewhere reveal that important EIS components are often missing. No thorough review of Quebec EIS practices has ever been conducted, a gap we sought to address.
Methods:
Adopting a cross-sectional descriptive study design, an online survey was distributed to 18 EIS that existed in Quebec in 2016 to collect data on clinical, administrative, training, and research variables. Survey responses were compared with existing EIS service delivery recommendations.
Results:
Half of Quebec’s population had access to EIS, with some regions having no programs. Most programs adhered to essential components of EIS. However, divergence from expert recommendations occurred with respect to variables such as open referral processes and patient–clinician ratio. Nonurban EIS encountered additional challenges related to their geography and lower population densities, which impacted their team size/composition and intensity of follow-up.
Conclusions:
Most Quebec EIS offer adequate services but lack resources and organizational support to adhere to some core components. Recently, the provincial government has created EIS guidelines, invested in the development of new programs and offered implementation support from the National Centre of Excellence in Mental Health. These changes, along with continued mentoring and networking of clinicians and researchers, can help all Quebec EIS to attain and maintain recommended quality standards.
Introduction
Multiple studies reveal that the implementation of essential components of EIS remains heterogeneous. 1 –3 A 2016 Canadian survey of 11 academic EIS found that while they generally followed existing standards and guidelines, there was significant variance in the extent to which essential care components were offered. 4 The availability of guidelines alone may not be sufficient, and specific funding, mentoring, and auditing of fidelity to standards may be required to ensure consistency in the quality of programs. 1,4 –6
In Quebec, over a 30-year period, clinicians developed EIS without provincial standards/guidelines or policy commitments which only emerged in 2017. A provincial association of EI programs, the Association québécoise des programmes pour premiers épisodes psychotiques (AQPPEP), formed in 2004, has supported EIS through continuing education, training, and networking around the use of clinical guidelines. No thorough review of Quebec EIS practices has ever been conducted.
The Quebec government’s latest 5-year mental health plan 7 envisaged the development of EIS in all regions by 2020. In 2017, the ministry of health and social services committed funding to develop 15 new EIS 8 , appointed an advisor at the Centre national d’excellence en santé mentale (CNESM) to support program implementation and published provincial EIS standards. 9,10 Our aim was to investigate the extent to which Quebec EIS established before 2016 (i.e., before these policy changes occurred) adhered to internationally recognized standards and thereby establish a baseline against which Quebec EIS can be measured in the future.
Methods
Adopting a cross-sectional descriptive study design, an online survey assessing clinical and administrative variables was distributed to 18 Quebec EIS that existed in 2016. All programs consented to their data being published as reported here. Responses were reviewed in relation to existing EIS recommendations, which are summarized in previous work. 4
These recommendations were extracted from national and international guidelines on EIS for psychosis or articles on essential components of EIS. Clinical guidelines from the United Kingdom, 11 –14 Australia, 15 New Zealand, 16 Italy, 17 and from four Canadian provinces (British Columbia, 3 Ontario, 18,19 New Brunswick, 20 and Nova Scotia 21,22 ) identified through PubMed, PsycINFO, and Google Scholar search were studied.
Half the surveyed EIS were in small cities (<150,000 inhabitants), semirural or rural areas, and the rest were attached to urban academic programs. These two sets of EIS were compared to elucidate additional challenges that smaller rural services may face and their impacts on service functioning.
Results
Seventeen of the 18 EIS responded to the survey. Two were excluded from the analysis of specific survey sections for which they had provided incomplete data. Table 1 presents the results of the survey regarding the implementation of the recommended core components of EIS.
Expert Recommendations Regarding Core Elements of EIS for FEP, Their Rationale, and Survey Results Describing Actual Practices around Those Core Elements for Quebec Programs.
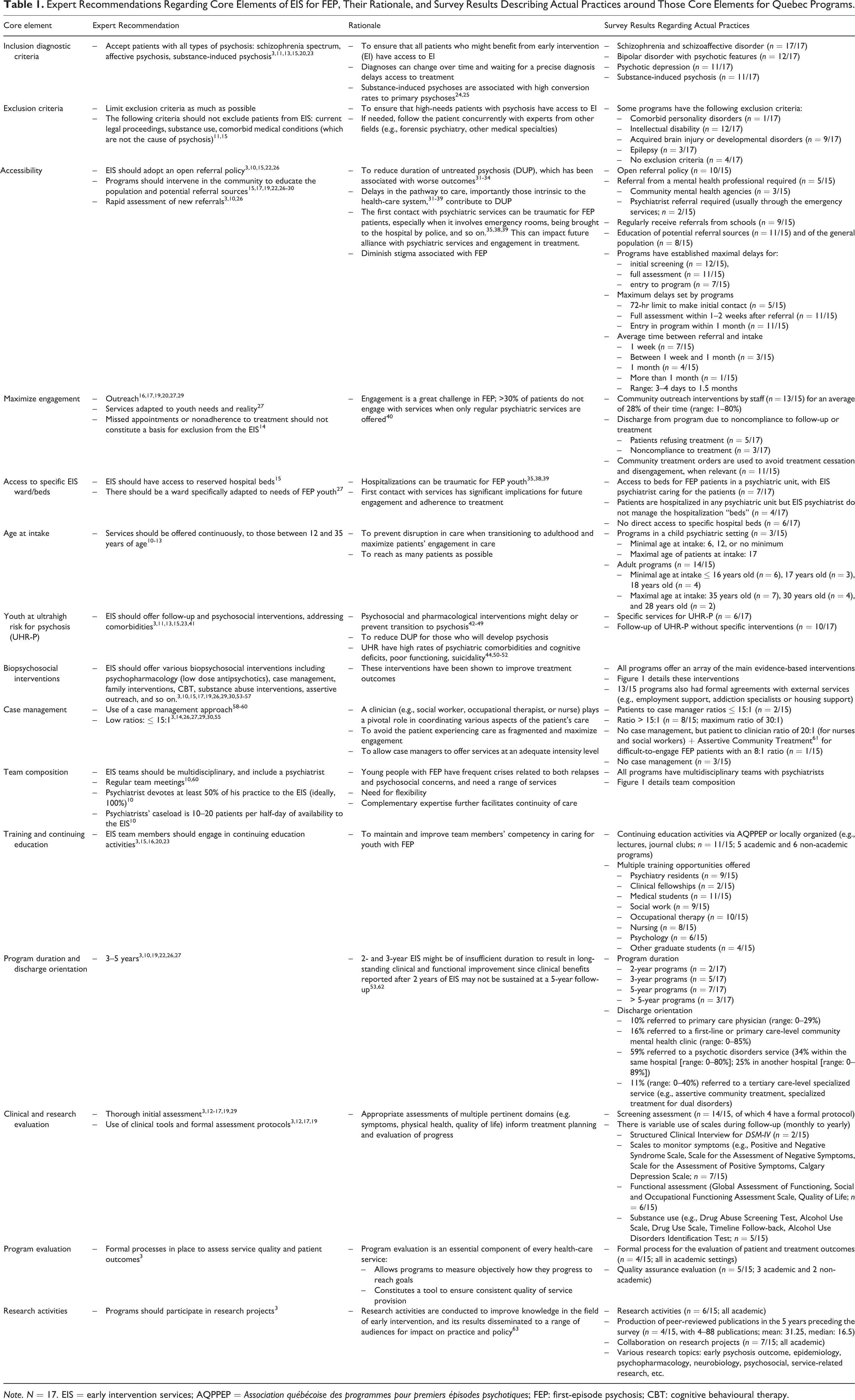
Note. N = 17. EIS = early intervention services; AQPPEP = Association québécoise des programmes pour premiers épisodes psychotiques; FEP: first-episode psychosis; CBT: cognitive behavioural therapy.
Detailed program and patient characteristics are reported in Table 2. Figure 1 shows the differences in access to mental health professionals in surveyed EIS and the variety of psychosocial interventions they offered.
Characteristics of the Surveyed EIS for FEP in Quebec, as of 2016.
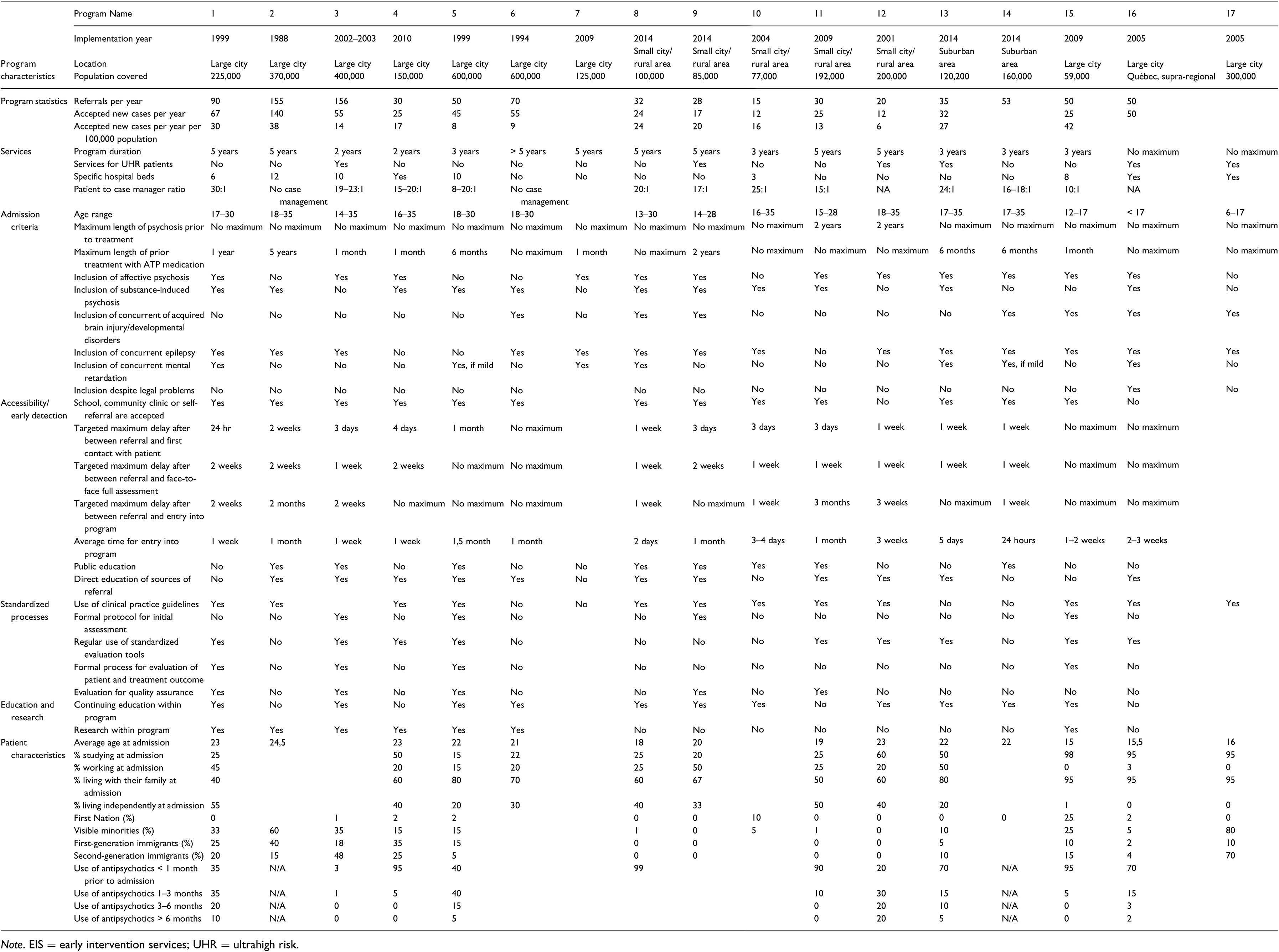
Note. EIS = early intervention services; UHR = ultrahigh risk.
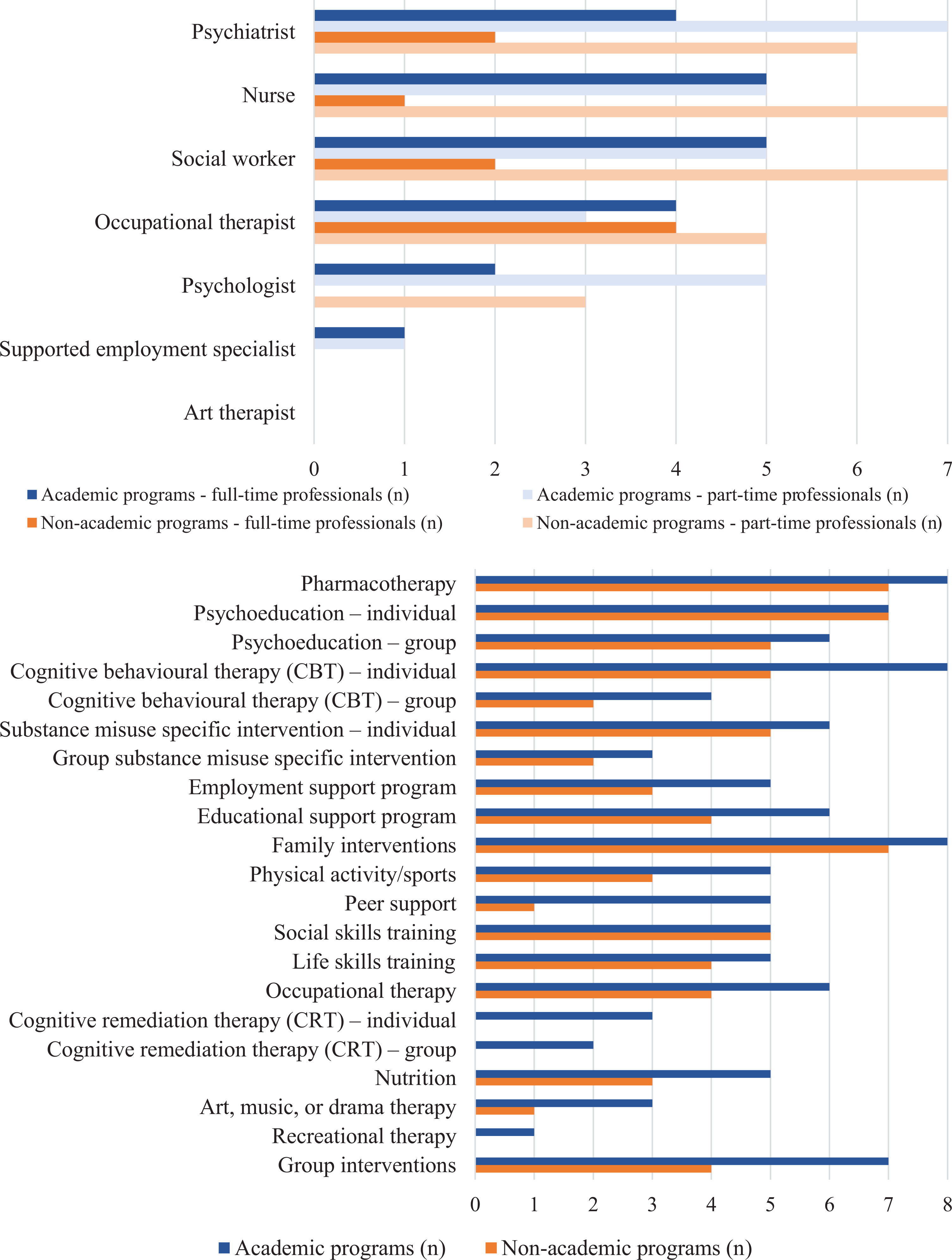
Team composition of Quebec early intervention services and offered psychosocial interventions.
Discussion
Access, Treatment Delay, and Care Continuity
At the time of the survey, about 3.75 million people (less than half of Quebec’s population) lived in catchment areas served by EIS. 64 To reduce the duration of untreated psychosis (DUP) and traumatic pathways to care, 10 programs had an open referral policy and most accepted self-referrals and referrals from schools, family, and friends. Several programs specified maximum acceptable delays between referral and initial screening, assessment and entry to program. The average time between referral and intake varied greatly (3–90 days). To promote early case identification (community capacity to recognize early signs of psychosis and refer without undue delay), 8 programs engaged in public education, and 11 offered education to potential referral sources (e.g., schools). The reasonable delays between referral, assessments, and the beginning of treatment reported by 11 programs could be attributed to service reorganizations that bypassed traditional pathways to care. Although these efforts sought to reduce DUP, most programs did not specifically estimate DUP. Our results are similar to those of an Ontarian EIS survey. 65
Some programs’ restrictive intake criteria may have excluded some patients who might have benefited from EI. To ensure continuity of care, EIS should serve people from adolescence past the age of majority (18 years in Quebec) instead of having hard age-based cut-offs. Several surveyed adult programs admitted patients under 18, but child and adolescent programs did not continue follow-up once patients turned 18.
High-Quality Interventions
Similar to the Ontario survey’s results, 65 most Quebec programs offered various evidence-based services, namely, pharmacotherapy, patient and family psychoeducation, cognitive-behavior therapy, and substance misuse interventions.
Four of the 15 programs did not offer intensive case management and one offered it only to patients considered difficult to engage. Furthermore, as in the Ontario study, 66 most programs did not adhere to recommended low patient-to-case manager ratios. This could lead to staff burnout 65,67 and impede the provision of services of appropriate intensity. Given that case management is a pillar of EI, 58,59 lack of selective and inadequately resourced case management is disconcerting.
High-Fidelity Implementation
Quebec’s EIS struggle with integrating administrative or organizational elements that could improve the implementation of standards and guidelines, likely due to their widely reported lack of adequate administrative, financial, and political support. Few programs had formal protocols for patient assessment, outcomes monitoring, and quality assurance. Such heterogeneity has been observed in implementing other high-intensity mental health programs on large scales. 68
To address the lack of continuing education opportunities especially in French, that most programs reported, AQPPEP organizes conferences and mentoring on-site and online. These are often the main or only continuing education opportunities available.
Contextual Influences
Unlike academic programs with dense urban catchment populations (range: 125,000–600,000; median: 370,000), non-academic programs face challenges attributable to the vastness (up to 10 times larger) and sparse populations of their catchments (range: 77,000–200,000; median: 120,000). Their smaller, less professionally diverse teams often dedicate part of their time to non-EIS activities and offer fewer types of psychosocial interventions. Some remote programs offer outreach services so that patients need not travel long distances to receive care. They combine several types of group interventions to serve more patients simultaneously and hold groups (e.g., family psychoeducation) in collaboration with local community organizations (often not restricted to first-episode psychosis [FEP] patients). The scarcity of employment support personnel and adapted employment options could result in patients in rural programs having poorer social and functional recovery. To enhance EI service provision and training/supervision opportunities for remote areas, alternative service models like flexible assertive community treatment, 69 specialist outreach 70 or hub-and-spoke, 70 and technological options should be considered. Training and supervising mental health-care providers, especially for interventions like cognitive behavioural therapy (CBT) for psychosis, remains challenging for all EIS. 70
It is known that fidelity to service models is attainable rapidly after implementation. 71,72 We found that how long programs had been in operation had little bearing on their fidelity to core EI components. British Columbia and Ontario, where provincial EIS standards exist, 3,19 have reported heterogeneous implementation and called for close and continuous monitoring. 65,73 Fidelity scales have been proposed and used in program audits to facilitate homogenization and adherence to standards among EIS. 29,60,74,75 Dedicated resources to support programs in continuous quality improvement (like the implementation advisor appointed by CNESM in 2017) may also help improve and evaluate fidelity.
Our findings also highlight the need to support EIS programs as they are being created in Quebec to ensure their alignment with standards and their collection of data on key performance indicators 71 from the outset.
Limitations
Data collected through a survey completed by program directors is subject to desirability bias. Although the data were 90% complete, two small programs did not complete most of the survey. EIS engaging in research activities may have been able to provide more accurate data-informed answers than non-academic programs. How programs were evaluated by patients and their families was not addressed.
Although most services reported offering many psychosocial interventions, the survey did not query what proportion of patients received them. We also did not enquire whether clinicians offering specialized interventions were properly trained and supervised.
Conclusion
Quebec EIS offer quality services to persons with FEP and adhere to several of the model’s essential components, despite lacking dedicated funding and policy support until recently. There is some heterogeneity in programs’ clinical and administrative components. Similar to studies of EI implementation, we found that smaller (rural) programs offered several essential components in adherence to standards, despite having a limited number of clinicians. 65 Some of the variance in services offered may be attributed to specific clinical or geographical realities. Most programs reported difficulties in implementing some essential components, even though clinical guidelines are widely available to clinicians and administrators.
Our survey represents an initial step in the monitoring of EIS implementation prior to the establishment of provincial guidelines and wider funding commitments. The survey allowed us to evaluate programs’ perceptions of their own performance. The next step would be to use scales to measure the quality of services and their fidelity to the EI model, as was recently done in Ontario 66 and in other countries. 76,77 Comparing the results of this survey with scale-based assessments in the future will help develop interventions to improve the quality of care and enhance programs’ and clinicians’ awareness of their strengths and weaknesses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.