
Abstract
Objective:
This study investigates the association between impulsiveness and six dimensions of recovery among homeless people with mental illness.
Method:
The sample was composed of 418 participants of a randomized controlled trial of Housing First, a recovery-oriented program that provides immediate access to permanent housing. The reliable change index method was used to provide an estimate of the statistical and clinical significance of the change from baseline to 24 months (i.e., clinically meaningful improvement), on outcomes that pertain to recovery dimensions: psychiatric symptoms (clinical), physical health and substance use problems (physical), residential stability (functional), arrests (criminological), community integration (social), and hope and personal confidence (existential). We tested for the effect of impulsiveness, assessed with the Barratt Impulsiveness Scale–11, on clinically meaningful improvement on each specific outcome, adjusting for age, gender and intervention assignment, as both intervention arms were included in the analysis.
Results:
For every increase in total impulsiveness score by one standard deviation, the odds of experiencing clinically meaningful improvement decreased by 29% (OR = 0.71, 95% CI, 0.55 to 0.91) on the clinical dimension and by 53% (OR = 0.47, 95% CI, 0.32 to 0.68) on the existential dimension. However, changes in outcomes pertaining to physical, functional, criminological, and social dimensions were not significantly influenced by impulsiveness.
Conclusions:
Findings highlight the importance of addressing impulsiveness in the context of recovery-oriented interventions for homeless people with mental illness. Further research may be required to improve interventions that are responsive to unique needs of impulsive individuals to support clinical and existential recovery.
The concept of recovery, understood as a continual, nonlinear, dynamic process by which individuals with mental illness gain or regain a sense of empowerment over their own lives, 1,2 is at the center of mental health services and interventions. 3,4 It has been suggested that research on recovery and program evaluation adapt by changing the metrics used to define success 5,6 —with holistic, dimensional measures being best aligned with service users’ experience of recovery. 7
Building on existing definitions of recovery as a dimensional construct, 8,9 Whitley and Drake 1 proposed a framework of five broad superordinate dimensions of recovery in which specific components or existing models can be operationalized: clinical, physical, functional, social, and existential. In addition to being holistic, the strength of this framework is its flexibility: It promotes a person-centered, consumer-defined approach to recovery in clinical settings, and it assists in the conceptualization of recovery for multiple subpopulations in the context of research. While this framework has been used primarily to structure qualitative findings, 10,11 it is also promising for structuring quantitative investigations and identifying more focused, measurable recovery components.
Such a flexible framework is useful when investigating recovery among people who experience both mental illness and homelessness, as they face unique barriers to recovery. 12 –19 In addition to residential instability, this group of persons experiences disproportionate justice involvement. 20,21 A scoping review of the literature on the experience of recovery among justice-involved individuals with mental illness 22 has argued that criminological recovery should be included in Whitley and Drake’s framework 1 when studying marginalized populations. Both this review and the qualitative findings of the At Home/Chez Soi (AHCS) demonstration project 23 generated important insights on which measurable components of recovery may best capture the six dimensions of recovery among homeless individuals with mental illness. 24 –26 Accessing and maintaining housing (functional), breaking social isolation and finding a sense of community belonging (social), rebuilding self-esteem and regaining hope (existential), improving one’s physical health (physical), and gaining a sense of control over substance use problems (physical) and mental illness symptoms (clinical) were highlighted by participants as significant aspects in their pathways towards recovery. 24 –26 Some justice-involved participants also underscored that multiple interactions with the justice system (criminological) contributed to their impression of feeling “stuck” on their pathway to recovery. 24
Narratives from people experiencing homelessness draw attention to the potentially disruptive impact of impulsive behaviors. 24,27 Impulsiveness—understood as a propensity to act in a sudden and unplanned manner with little consideration of consequences 28 —makes it difficult to inhibit certain behaviors to which immediate gratification is associated, impeding one’s ability to successfully pursue long-term goals. 29,30 Systematic or narrative reviews of the literature have shown that impulsiveness is overrepresented among people with several mental illnesses 28,31 and that it may be a risk factor for substance abuse, 32 as well as violence and aggression. 33,34 There is also some evidence that impulsiveness is associated to greater health-related disability among people with major depression 35 and higher social dysfunction among people with substance use disorder. 36,37 Among people in recovery of substance abuse, resistance to impulses also promotes hope: It increases the ability to envision long-term goals and to develop a plan to reach those goals. 38 Finally, although there is very little research on the role of impulsiveness on residential stability, several of these outcomes are associated with homelessness.
The few studies examining the role of impulsiveness on change in outcome value among people with mental illness suggest that impulsiveness could impede recovery. 37,39,40 Impulsiveness has been shown to increase active psychiatric symptomatology through poor medication adherence among people with bipolar disorder. 40 It also leads to high dropout rates in addictions treatment and increased rates of relapse after program completion. 39 Impulsiveness also predicts poorer improvement in social quality of life in a sample of people in methamphetamine treatment. 37 Impulsiveness may thus influence many components of recovery relevant to homeless people with mental illness.
Purpose of the Study
The objective of this article is to test whether impulsiveness predicts clinically meaningful improvement on seven outcomes that pertain to six dimensions of recovery among homeless people with mental illness: psychiatric symptomatology (clinical), physical health and substance use problems (physical), residential stability (functional), arrests (criminological), community integration (social), and hope and personal confidence (existential). Based on the literature, we expect impulsiveness to be associated with lower odds of clinically meaningful improvement for all outcomes.
Methods
Study Design and Participants
This study examined a sample of participants recruited for the Montréal site of the AHCS study, a randomized trial of Housing First, 23 a recovery-oriented program that provides immediate access to permanent housing. The Montréal site was the only site of five to include a measure of impulsiveness.
To be eligible, participants had to be 18 years or older, absolutely homeless or precariously housed with recent episodes of homelessness, and have a diagnosis of serious mental disorder (psychotic disorder, mood disorder with psychotic features, major depressive episode, manic/hypomanic episode, panic disorder, or post-traumatic stress disorder) as determined by Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) criteria on the Mini-International Neuropsychiatric Interview. 41 The registered protocol provides details on the eligibility criteria and procedures. 23 The appropriate institutional research ethics approvals were obtained, and all participants provided written informed consent to participate in the study.
Of the 469 participants interviewed at baseline, 441 completed the Barratt Impulsiveness Scale–11 30 (BIS-11; participants who answered fewer than 10 items were excluded), and among whom 418 participants completed the final interview (at 21 or 24 months). The main characteristics of the sample are presented in Table 1. Participants included in the present analyses were similar to those who were not (see Table S1 in the Online Supplement).
Description of the Sample.
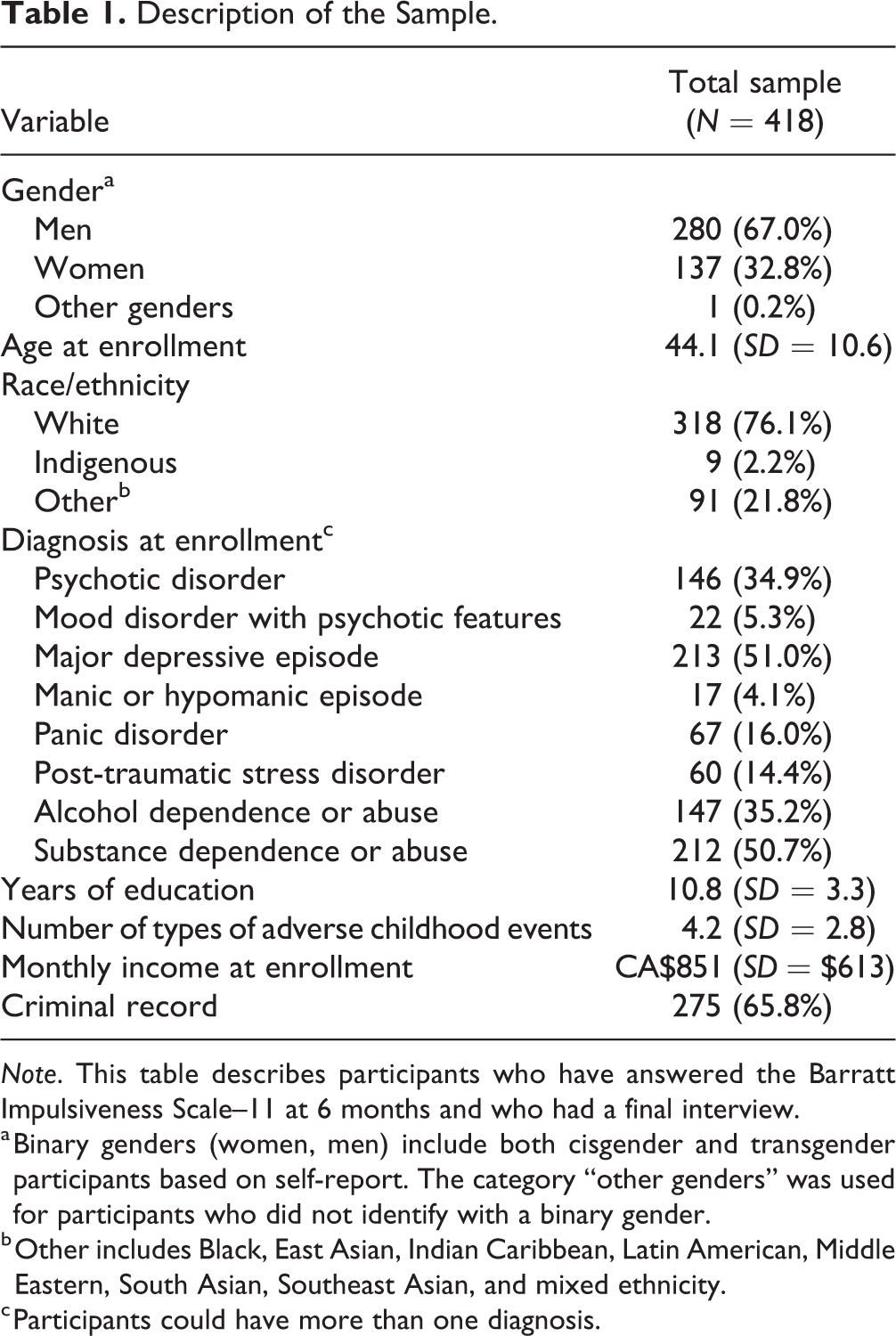
Note. This table describes participants who have answered the Barratt Impulsiveness Scale–11 at 6 months and who had a final interview.
a Binary genders (women, men) include both cisgender and transgender participants based on self-report. The category “other genders” was used for participants who did not identify with a binary gender.
b Other includes Black, East Asian, Indian Caribbean, Latin American, Middle Eastern, South Asian, Southeast Asian, and mixed ethnicity.
c Participants could have more than one diagnosis.
Measures
Impulsiveness
The BIS-11 30 is a 30-item self-report measure (possible range: 30 to 120, higher score indicating greater impulsiveness) that measures attention, cognitive instability, motor impulsiveness, perseverance, self-control, and cognitive complexity. It was administered at the 6 month interview. To deal with missing items, we prorated the total item score. We standardized the variable to ease interpretation (i.e., centered on the mean, one unit change represents one standard deviation). The mean total score on the BIS-11 was 68.1 (SD = 10.8). We elected to use only the total score, as opposed to scores pertaining to the subscales, as past research has found the factor structure to be unstable. 42 –48 The internal consistency was fair (α = 0.76), which is comparable to other psychometric studies of the BIS-11. 42
Recovery
Since recovery is a deeply personal experience 49 for which empowerment is a central pillar, we privileged self-reported outcomes. Each outcome was operationalized using a dichotomized measure of clinically meaningful improvement, 50,51 which was obtained through two steps. First, we computed a reliable change index, 50 using the Cronbach’s α of the scale or an intraclass correlation coefficient as reliability measurement. 51 When the absolute value is larger than 1.96, the change is said to be reliable at an alpha of 0.05. Second, we identified a cutoff score that distinguished “cases” (Note 1) from “non-cases,” from the literature, theoretical grounds, or formulas recommended by Jacobson and Truax. 50 Participants were considered to have improved in a clinically meaningful manner if they had both improved in a statistically reliable manner and were classified as a non-case at the end of follow-up. We included only participants who were considered cases at baseline on that specific outcome. Table 2 summarizes the outcomes, the scales or measures used, details pertaining to the reliability coefficients used, and the cutoff scores.
Variables Selected for the Six Dimensions of Recovery along with the Associated Scales or Measures as well as their Reliability and Clinical Cutoff Scores.
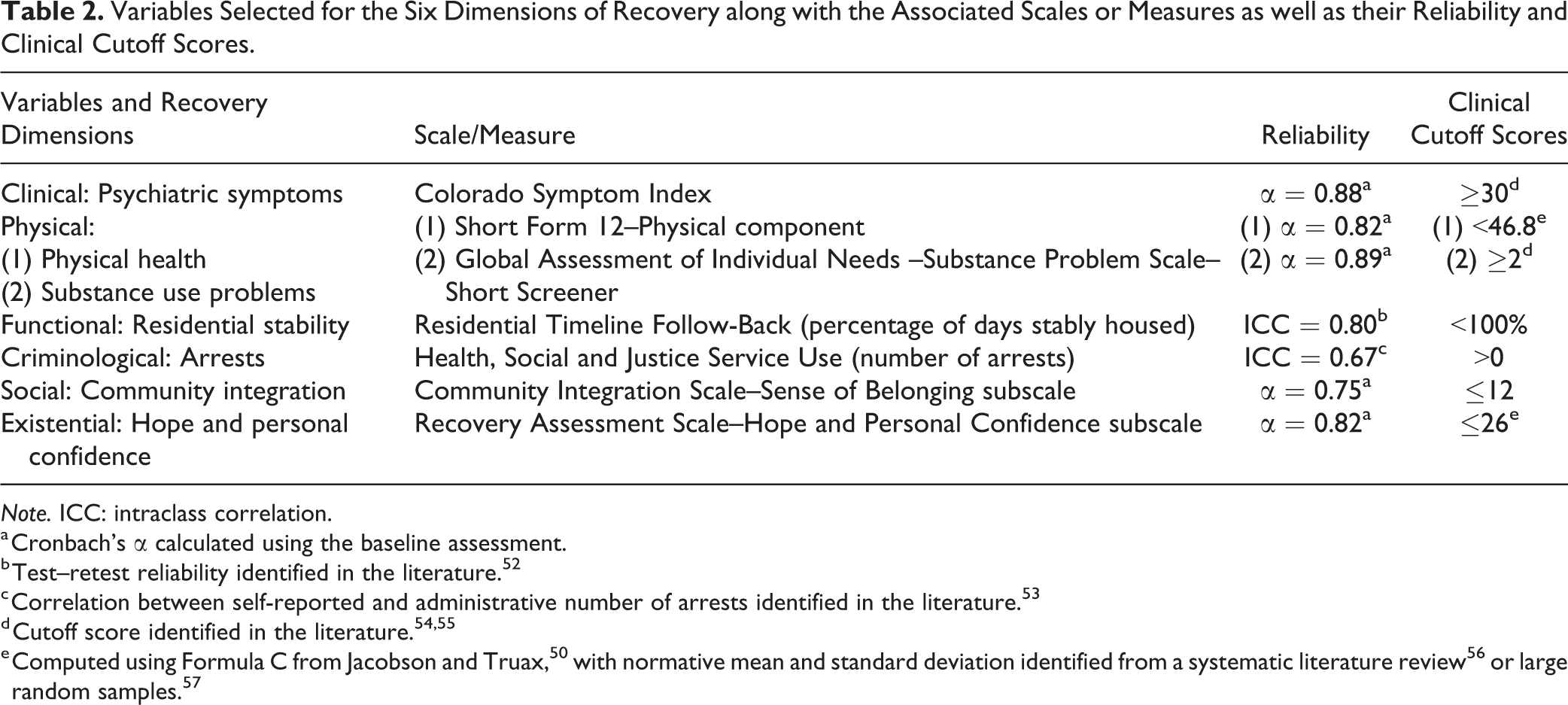
Note. ICC: intraclass correlation.
a Cronbach’s α calculated using the baseline assessment.
b Test–retest reliability identified in the literature. 52
c Correlation between self-reported and administrative number of arrests identified in the literature. 53
Clinical: Psychiatric symptomatology
The Colorado Symptom Index measures the presence and frequency of psychiatric symptoms 58,59 in the past month through 14 items (possible range: 14 to 70, higher scores indicate greater symptomatology). A cutoff score of 30 was selected based on the literature (sensitivity = 0.76, specificity = 0.68). 54
Physical: Physical health and substance use problems
We used the physical component summary of the Short Form 12 survey (possible range: 0 to 100, higher scores indicate better health status) to assess physical functioning and bodily pain in the past month. 60 A cutoff score of 46.8 was calculated 50 using norms (M = 47.4, SD = 9.53) identified from the literature. 57
Because over half of the sample has a substance use disorder, we included a second outcome to the physical dimension, using the Global Assessment of Individual Needs (GAIN)–Substance Problem Scale–Short Screener, 61 which assesses the number of problems related to drug and alcohol use in the past month through 5 items (possible range: 0 to 5). A cutoff score of 2 was selected based on the literature (sensitivity = 0.91, specificity = 0.96). 61
Functional: Residential stability
The percentage of days stably housed was assessed using the Residential Timeline Follow-Back questionnaire for the 3 month period prior to the interview. 52 Stable housing was defined as living in one’s own room, apartment, or with one’s family, and expecting to remain in this residence for at least 6 months or having tenancy rights. Because service providers continue working with clients until they are stably housed, we defined cases as those who did not spend 100% of days in stable housing. In several instances, participants were considered fully stably housed even though they had spent a number of days in institutions (e.g., hospitals) if they had continued to have a permanent stable residence.
Criminological: arrests
We assessed the number of self-reported arrests in the prior 6 months 23 and defined cases as those with any arrests.
Social: Community integration
The Community Integration Scale–Psychological Integration and Sense of Belonging subscale was specifically developed for the AHCS study. 23 It includes 4 items rated on a 5-point scale (e.g., “I interact with the people who live near me”), and higher scores indicate greater social integration (possible range: 4 to 20). Norms or a validated cutoff being unavailable, we used an arbitrary score of ≤12, applying the following reasoning: for each item, a score of ≤2 indicates a disagreement with the statement, a score of 3 indicates neutrality, while a score of ≥4 indicates an agreement. This cutoff score thus allows to identify individuals who would generally disagree or feel neutral. This strategy has been used in other studies among homeless people and is supported by qualitative findings. 62
Existential: Hope and personal confidence
We used the Hope and Personal Confidence subscale of the Recovery Assessment Scale, 63 which is constituted of questions related to self-efficacy, self-esteem, and hope. Higher scores indicate greater hope and personal confidence (possible range: 7 to 35). A cutoff score of 26 was calculated 50 using norms (M = 26.5, SD = 1.3) identified from a systematic review. 56
Exploratory analyses
Based on the findings, we sought to understand what could explain the association between impulsiveness and lower odds of improvement on the clinical dimension. We hypothesized that impulsiveness would reduce access to healthcare, measured using the Health Services Access questionnaire 23 at the 6 month interview.
Analytic Approach
To measure the association of impulsiveness with clinically meaningful improvement on each specific outcome, we used logistic regressions, adjusting for age, male gender (Note 2) and intervention assignment (as both intervention arms were included in the analysis [Note 3]) using Stata 15.1. We selected covariates based on whether they could theoretically confound the association between impulsiveness and recovery. More specifically, they had to be associated to impulsiveness but could not be an effect of impulsiveness. 66 All sensitivity analyses are detailed in the Online Supplement.
Results
For each outcome, Table 3 describes the number of participants who were classified as cases based on the clinical cutoff at baseline, along with the proportion of cases who experienced a clinically meaningful improvement. Impulsiveness was associated with a lower likelihood of clinically meaningful improvement in clinical and existential dimensions, but no association was observed with the physical, functional, criminological, and social dimensions (see Table 4). On average, for every increase in impulsiveness by one standard deviation, the odds of experiencing clinically meaningful improvement decreased by 29% (OR = 0.71, 95% CI, 0.55 to 0.91) for the clinical dimension of recovery and by 53% (OR = 0.47, 95% CI, 0.32 to 0.68) for the existential dimension.
Description of the Six Recovery Dimensions at Baseline and at the Final Interview along with the Proportion of Baseline Cases having Experienced Clinically Meaningful Improvement.
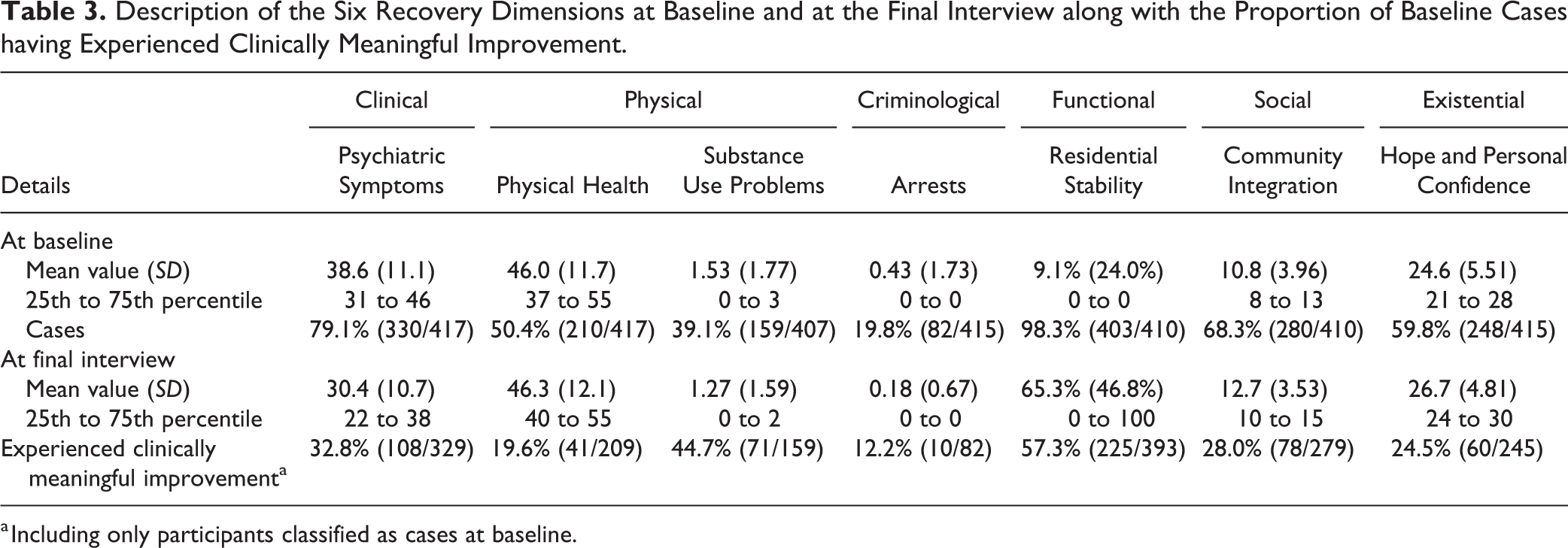
a Including only participants classified as cases at baseline.
Odds Ratio Associated with Clinically Meaningful Improvement in the Six Dimensions along with 95% Confidence Intervals.
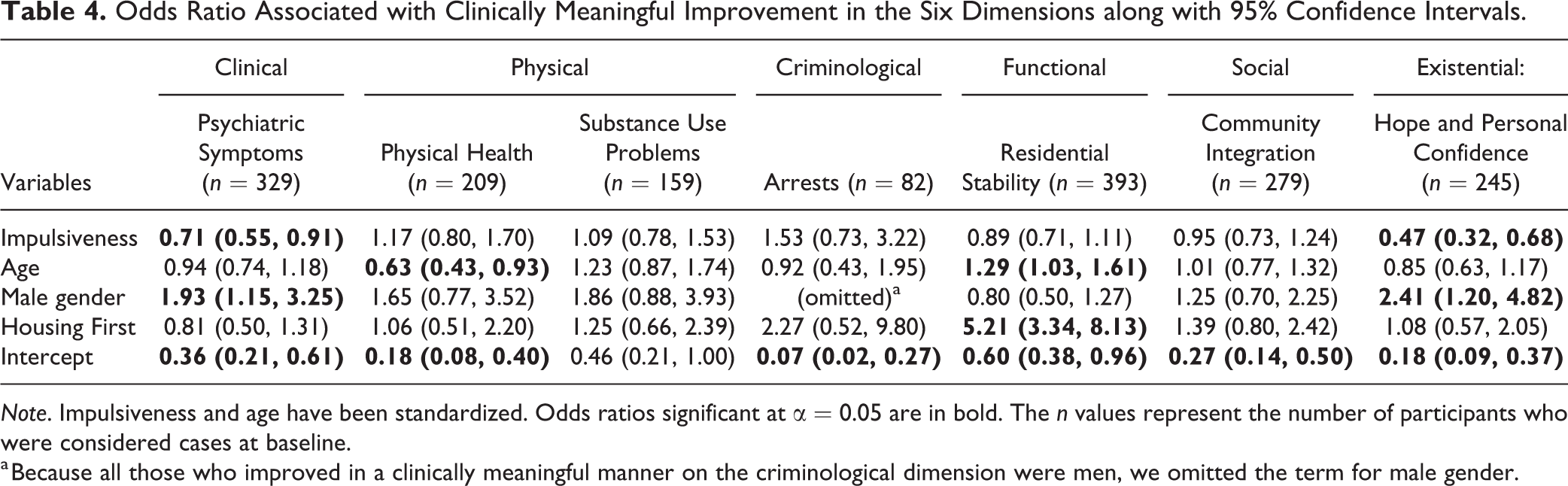
Note. Impulsiveness and age have been standardized. Odds ratios significant at α = 0.05 are in bold. The n values represent the number of participants who were considered cases at baseline.
a Because all those who improved in a clinically meaningful manner on the criminological dimension were men, we omitted the term for male gender.
Exploratory analyses
Impulsiveness was associated cross-sectionally with increased odds of not obtaining health care when the need arises (OR = 1.51, 95% CI, 1.22 to 1.88, adjusting for all covariates), which in turn predicted lower odds of clinically meaningful improvement on the clinical dimension (OR = 0.49, 95% CI, 0.30 to 0.83, adjusting also for impulsiveness).
Discussion
The objective of the study was to measure the association of impulsiveness with clinically meaningful improvement among homeless people with mental illness on six dimensions of recovery. 1,22 Our hypothesis was partly confirmed: Impulsiveness predicted lower odds of improving in a clinically meaningful manner for clinical and existential dimensions, but not for physical, functional, criminological, and social dimensions.
The prospective association of impulsiveness with lower odds of improving in a clinically meaningful manner in terms of psychiatric symptomatology suggests that the role of impulsiveness in mental illness symptoms is more than an artefact of the presence of behavioral disinhibition among the diagnosis criteria for several mental disorders. 28 It may suggest that people who are highly impulsive may be less likely to adhere to psychotherapies or pharmacotherapies. Belzeaux et al. 40 found that impulsiveness reduced adherence to medication, and that this association was not mediated by substance use disorder. An exploratory analysis of our data reveals that access to health care may also be a concern, and that reasons for nonaccess should be further investigated. The literature also shows that individuals who experience emotional distress may shift their focus away from long-term goals towards the short-term goal of alleviating the sensation, resulting in lower impulse control. 67 For example, individuals with heightened impulsiveness use fewer adaptive emotional regulation strategies when exposed to trauma, resulting in greater depression symptoms. 68 The high prevalence of adverse childhood experiences 69 and victimization, 20 as well as the experience of other long-standing trauma 24 among homeless people with mental illness may thus constitute an additional challenge for resistance to impulsiveness and highlights the importance of trauma-informed care. 70
Our findings also suggest that impulsiveness is associated with lower odds of clinically meaningful improvement in one’s sense of hope, self-esteem, and self-efficacy. Although a similar finding had been found among adolescents, 71 personal confidence and self-efficacy have long been considered a stable personality trait among adults. 72,73 But in our sample, every increase in impulsiveness score by a standard deviation halved the odds of improving in a clinically meaningful manner on hope and personal confidence. Auerbach and Gardiner 71 had hypothesized that acting without forethought of consequences resulted in careless behaviors, which people may later regret or for which they later blamed themselves. Impulsive people have also been shown to engage in fewer adaptive counterfactual (“if-then”) thinking (i.e., where someone reflects on a negative event, proposing an alternative that could have led to a more positive outcome), 74 which allows to turn a failure into an opportunity for further goal pursuit 75 and enhances self-efficacy. 76 Some dimensions of impulsiveness are also associated with difficulties in inhibiting coping strategies that rely on self-blame and catastrophizing, 68 which could in turn negatively impact one’s self-efficacy and hope in the future.
While impulsiveness is a known risk factor for adverse outcomes on physical, functional, criminological, or social dimensions, our findings suggest that it may not interfere with the recovery process. We expected to find an association between impulsiveness and lower odds of clinically meaningful improvement on substance use problems. This was not the case. Given that we used a validated cutoff score 55 and that the odds ratio was close to the null effect, this finding is unlikely to be an artefact of the cutoff score or a lack of statistical power. One possible explanation for this nonassociation may relate to the motivational interviewing and harm reduction approaches used by AHCS case managers to address substance use. Improvements made in this context may not be as highly susceptible to the client’s impulsiveness as traditional addiction treatment programs. Furthermore, the GAIN amalgamates problems caused by all substances (alcohol, stimulants, opiates, etc.) into a single score. Impulsiveness and substance abuse may have a distinct causal relationship for different groups of substance, 32 which may not be reflected in our analysis. A more specific scale may be required for highly vulnerable study populations such as homeless people with mental illness.
Implications
These findings regarding clinical and existential recovery dimensions highlight the importance of taking impulsiveness into account in the context of recovery-oriented interventions for homeless people with mental illness. A first approach could directly target impulsiveness, under the assumption that impulsiveness is a dynamic individual risk factor and that interventions may enhance impulse control. A systematic review of experimental interventions found that episodic future thinking (i.e., thinking about an episode from one’s future in vivid terms) 77 reduced impulsive choice. 77 It could thus be integrated into cognitive or behavioral interventions for individuals with high impulsiveness, such as self-control training 78 or mindfulness approaches. 79,80 However, given that nearly three quarters of AHCS participants demonstrated cognitive impairments, 81 implementing these strategies could prove challenging.
A second approach could seek to adapt recovery-oriented services to address the needs of their impulsive clients, under the assumption that impulsiveness is a stable trait or unlikely to change meaningfully among adults. Our findings suggest that impulsive individuals experience difficulties in accessing care, highlighting the importance of organizing community mental health services in ways that favor outreach to homeless clients with mental illness. Interventions that address hope, personal confidence, and self-efficacy among vulnerable populations are promising areas which nevertheless require more research. A systematic review highlighted some self-management strategies to foster hope identified by mental health service users, which included cognitive reframing, fighting isolation, and education regarding their symptoms. 82 The authors suggested that future interventions for hope enhancement among people with mental illness should focus on fostering relationships, developing a peer support network, formulating and pursuing realistic goals, and addressing specifically self-esteem and self-efficacy. 82 Clients with high impulsiveness may especially benefit from the assistance of case managers in developing skills for goal achievement. Given that hope, personal confidence, and self-efficacy are not only desirable endpoints but important factors on the pathways to other dimensions of recovery, 83 implementing strategies to foster hope and personal confidence has the potential to have a large impact on the clients’ lives and well-being. Some compensatory strategies could also be considered to limit the impact of impulsive decisions, for which people may later blame themselves. For example, people with lived experience of homelessness highlighted that participating in a trust account (where the clients’ finances are managed by the team, with individualized support for budget planning and management) was helpful in avoiding impulsive spending. 27 This voluntary compensatory strategy could easily be implemented by Assertive Community Treatment and intensive case management teams.
Implementing distress tolerance strategies as an adjunctive voluntary intervention could be an avenue of interest, both in terms of psychiatric symptoms and hope and personal confidence. 84 A study among psychiatric inpatients has shown that one’s perceived ability to tolerate distress has a greater impact on symptoms related to trauma than one’s actual ability—and that socioeconomically disadvantaged individuals were more likely to underestimate their distress tolerance. 85 Training case managers to promote the clients’ self-efficacy in terms of distress tolerance could alleviate the negative effect of impulsiveness and improve resilience when facing obstacles to their long-term goals.
Limitations
Each dimension of recovery encompasses a multitude of outcomes and recovery should be person-centered when addressed in the context of interventions. We selected the measurable outcomes that appear to best capture each recovery dimension among a sample of homeless people with mental illness and included in the AHCS protocol, though these are in no way exhaustive. Arguably, a multidimensional recovery scale could partly address this shortcoming, 86,87 but none had been developed at the time the study protocol was elaborated. Nevertheless, this is an early attempt to investigate recovery using an expanded version of a dimensional framework, and it demonstrates the importance of delineating various recovery dimensions. Second, validated or theoretically-grounded cutoff scores were unavailable for two outcomes. One should be careful in interpreting the size of the effect until findings are reproduced using validated cutoff scores. Finally, suicidality was not explicitly integrated into our model other than as an item on the Colorado Symptom Index. Given the high correlation between suicidality and impulsiveness (both in our data and in the literature) 88 , future studies should examine the potential interactions between impulsiveness, clinically meaningful improvements in terms of psychiatric symptoms as well as hope and personal confidence, and suicidality.
Conclusion
This is the first study to use clinically relevant reliable change indices to examine recovery across multiple dimensions among homeless people with mental illness. The findings show that impulsiveness has a clinically meaningful impact on two important dimensions of recovery among this population: clinical and existential. This points to the importance of taking the clients’ impulsiveness into account for service delivery and training Housing First staff to adopt various strategies to reduce the harms related to impulsiveness. 89 Clarifying the causal associations could be helpful to identify potential intervention targets that may be more liable to change than impulsiveness.
Supplemental Material
Supplemental Material, leclair_onlinesupp - Pathways to Recovery among Homeless People with Mental Illness: Is Impulsiveness Getting in the Way?
Supplemental Material, leclair_onlinesupp for Pathways to Recovery among Homeless People with Mental Illness: Is Impulsiveness Getting in the Way? by Marichelle C. Leclair, Ashley J. Lemieux, Laurence Roy, Michael S. Martin, Eric A. Latimer and Anne G. Crocker in The Canadian Journal of Psychiatry
Footnotes
Authors’ Note
The views expressed herein solely represent those of the authors.
Data Access
The data may be obtained from the first author upon request for the purpose of replication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Marichelle Leclair would like to acknowledge the financial support of Fonds de recherche Québec—Société et Culture (FRQ-SC) in the form of an MSc fellowship, and Équipe Vulnérabilité, intégration sociale et violence (VISEV) as a bursary. She was also partly funded through Dr. Anne Crocker’s William Dawson Award from McGill University in the first phases of the study. Dr. Ashley Lemieux was granted an FRQ-SC doctoral fellowship, a VISEV doctoral bursary, and a Graduate Excellence Fellowship in Mental Health Research from McGill University. Dr. Laurence Roy was supported by a postdoctoral fellowship grant from the Fonds de Recherche du Québec–Santé (FRQ-S). Dr. Michael Martin was supported in part by a Vanier Canada Graduate Scholarship. Dr. Crocker acknowledges the support of the Canadian Institutes of Health Research (CIHR) and the FRQ-S for consecutive salary awards while working on this study. We also thank Jayne Barker, PhD, Cameron Keller, and Catharine Hume, the Mental Health Commission of Canada, the At Home/Chez Soi national project leads, the late Paula Goering, PhD, national research lead, the national research team, the site coordinators, and the numerous service and housing providers, as well as persons with lived experience, who have contributed to this project. This research has been made possible through a financial contribution from Health Canada.
Notes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.