
Abstract
Introduction:
The recommended objective for mental health plans and policies is the adoption of recovery approaches to mental healthcare. Mental health recovery is no longer defined by symptom resolution but as a journey towards a meaningful life from the consumer’s own perspective. Recovery approaches focus on consumers’ strengths, feelings of well-being and the achievement of personal goals. Designing recovery-oriented interventions is crucial for supporting people in their personal recovery journey.
Aim:
This study sought to evaluate how attending a recovery-oriented intervention impacts the recovery of attending people living with serious mental illness.
Methods:
A quasi-experimental approach was utilised to examine changes in self-reported recovery progress in a purposive sample of consumers living with enduring mental illness (N = 105). Recovery progress was evaluated via the Recovery Assessment Scale – Domains and Stages (RAS-DS). Data were collected at entry and exit to a therapeutic recreation programme grounded in principles of recovery-oriented care and social contact theory. Pre-post scores were analysed via a repeated-measures multivariate analysis of variance (RM-MANOVA) per the four RAS-DS recovery domains.
Results:
After attending the therapeutic recreation programme, consumer recovery scores significantly increased in the functional, personal, and social recovery RAS-DS domains as measured by ‘Doing Things I Value’, ‘Looking Forward’, and ‘Connecting and Belonging’ (respectively). No changes were observed to consumers’ clinical recovery progress, as assessed via the recovery domain ‘Mastering my Illness’.
Conclusion:
The results of this study demonstrate that therapeutic recreation camps can provide a recovery-based approach to mental healthcare, with positive effects on the three areas of: a purposeful life; connection and belonging; and optimism and hope. Recovery Camp has been previously identified by the Productivity Commission as having potential person-centred recovery benefits for mental health consumers. The results of this study now establish these benefits as evidence based and can be used to guide mental health practice and policy for the implementation of therapeutic recreation camps for mental health recovery.
Introduction
Mental health recovery benefits individuals and communities. With approximately 970 million people globally (World Health Organization [WHO], 2022), including 44% of the Australian population (Australian Bureau of Statistics, 2022) living with mental illness, the impact on individuals and communities is immense. For communities, increasing healthcare costs, and the economic consequences of productivity loss related to mental illness is recognised (WHO, 2024). For individuals, living with mental illness can have significant psychosocial effects that impact their quality of life. Mental health recovery serves as the aspiration and journey to counteract the multifaceted impacts of mental illness.
Background
Mental health recovery
In the context of healthcare, the concept of recovery means different things in different settings. The term is commonly used in healthcare and can be linked to a medically based understanding, where it means that someone has no symptoms of illness (Slade et al., 2014). Definitions of mental health recovery, however, emphasise recovery as a personal journey which encompasses personal experiences not linked to symptom resolution (Whitley et al., 2015). Recovery in mental health comprises the notion that people living with serious mental illness can live a meaningful life. It is an approach that looks beyond a person’s mental health problems, recognises their strengths, and supports people to achieve their goals (Jacob, 2015).
While recovery is unique to each person, central to all recovery paradigms are hope, self-determination, self-management, empowerment, and advocacy (Australian Health Ministers’ Advisory Council, 2013). A systematic review synthesising definitions of mental health recovery (Ellison et al., 2016), found there are critical aspects of recovery, including that it must be individualised/person-centred, and connect individuals to experiences of empowerment, purpose, and hope. Critical too for recovery is the support the individual receives, including that from appropriate health and recovery-oriented interventions (WHO, 2021).
Support for the Recovery Assessment Scale (RAS) was established in a status report issued by the Australian Institute of Health and Welfare (AIHW, 2015), stipulating the RAS as one of four recovery suitable assessment tools to measure individual recovery for people living with mental illness. A systematic review identifying and scrutinising tools to measure personal recovery, has found the RAS to be the most robust and consistent tool, with most psychometric support (Sklar et al., 2013).
Recovery-oriented interventions
An individual’s engagement with recovery-supportive services can be an integral influence of their recovery journeys (Jacob et al., 2017; Happell, 2008). Happell’s (2008) study, which explored consumer perspectives in relation to the factors that promote and impact recovery, found that services play a crucial role in enhancing recovery. In particular, support from both staff and peers emerged as significant and influential factors (Happell, 2008). The development of community-based interventions that are recovery-oriented is crucial for supporting people in their personal recovery journey (WHO, 2021). Recovery-oriented community-based services should encompass the principles of providing a safe place, hope, finding balance, developing self-wisdom, enhancing enjoyment, building confidence and promoting self-determination, to support recovery (Ariss et al., 2019). However, there often still exists a reliance on diagnosis, medication and symptom reduction (WHO, 2021); approaches that do not privilege the personal experiences of mental health recovery.
Measuring recovery
Considering the unique and personal nature of mental health recovery, attempting to capture or measure recovery remains a complex task (AIHW, 2015). Compounding this, a lack of consensus around definitions and constructs for recovery lead to conflicting ideas on how to measure personal recovery in the mental health setting (Vogel et al., 2020).
Aim
This study sought to evaluate how attending a recovery-oriented intervention impacts the recovery of attending people living with serious mental illness.
Methods
Design
A quasi-experimental design was utilised to assess a purposive sample of consumers attending a therapeutic-recreation programme based on their eligibility and informed voluntary consent. Power analyses conducted via G*Power software (v.3.1.9.6) indicated a minimum sample size of 74 participants would yield 95% statistical power for detecting moderately-sized effects when using a repeated measures multivariate analysis of variance (f = 0.25, No. of groups = 2, No. of measures = 4, 1 − β = 0.95; Faul et al., 2009). The threshold for statistical significance was set at α = .05.
Ethical approval
Ethical approval was granted by the University of Wollongong Human Research Ethics Committee (approval number 2019/ETH03767). Consumers were briefed on the aims of the project and apprised of the voluntary nature of their participation. Informed written consent was obtained at both pre- and post-time-points prior to their involvement in the study.
Participants
Consumers (N = 105) attending the therapeutic-recreation programme between August 2018 and January 2020 volunteered to participate in the present study. The mean age of participants was 41.4 years (SD = 13.5, min. = 18, max = 70). Eligibility criteria included being over 18 years of age, living with a diagnosed mental illness (e.g. schizophrenia, PTSD and bipolar disorders) and living in the community at the time of the programme (i.e. not seeking acute care services).
Setting
The setting was the recovery-oriented programme, Recovery Camp. Recovery Camp combines therapeutic recreation activities to promote mental health, social connection, and physical activity in a natural Australian setting, for personal recovery. Recovery Camp includes a combination of structured activities (e.g. physically challenging, problem solving, and team building) that incorporate elements of cognitive, affective and psychomotor learning (Bloom, 1956). Integral to the activity, is the facilitated in-depth debriefing to enable participants to engage in reflexivity.
Recovery Camp is a 5-day community therapeutic intervention programme that positively impacts self and perceived choice for consumers (Taylor et al., 2017), enhances social relationships (Picton et al., 2018), and facilitates goal setting and attainment for people living with mental illness (Patterson et al., 2024). While these measured outcomes highlight aspects of the personal recovery journey, there is a need to evaluate the impact of the intervention specifically on the individual recovery process.
Consumers participated in instructor-facilitated recreation activities (e.g. giant swing, high ropes and bush dancing) alongside peers, mental health specialised nurses and student nurses completing a pre-registration mental health clinical placement.
Measure
The Recovery Assessment Scale-Domains and Stages (RAS-DS) is a self-report, 38-item instrument developed for use in Australian settings. It is widely used in non-government Australian mental health services to assess consumer mental health recovery (Hancock et al., 2016). The AIHW (2015), detailed its support for RAS as one of four recovery suitable assessment tools to measure individual recovery for people living with mental illness. A systematic review identifying and scrutinising tools to measure personal recovery, has found the RAS to be the most robust and consistent tool, with most psychometric support (Sklar et al., 2013).
The scale exhibits acceptable internal validity (mean squares of ⩽1.5; Wright & Linacre, 1994) and excellent reliability indices (Cronbach’s α = .96; Hancock et al., 2014). The RAS-DS measures four distinct recovery domains, including functional recovery (‘Doing things I value’: Items 1 to 6, e.g. ‘I continue to have new interests’); personal aspects of recovery (‘Looking forward’: Items 7 to 24, e.g. ‘I can handle it if I get unwell again’); clinical recovery (‘Mastering my Illness’: Items 25 to 31, e.g. ‘My symptoms interfere less and less with my life’); and social recovery (‘Connecting and Belonging’: Items 32 to 38, e.g. ‘Even when I don’t believe in myself, other people do’). Responses are given on a 4-point Likert scale ranging from 1 = UNTRUE, 2 = A Bit TRUE, 3 = Mostly TRUE, to 4 = Completely TRUE. Higher scores are indicative of more advanced recovery (Hancock et al., 2016). No items are reverse-scored.
Procedure
At entry to the programme, consumers were informed of the research project and invited to participate. Those who volunteered provided their written consent and completed a paper version of the RAS-DS, at two time points, upon entry to Recovery Camp and upon completion of Recovery Camp. Approximate time to complete the survey averaged 15 minutes. Though the RAS-DS has been designed with as user-friendly language as possible, support was provided (as required) from the mental health specialised nurses. This commonly included reading various instrument items and assisting with indicating consumer-provided responses. The supported nature of completing the RAS-DS has been identified as a strength of the instrument as it cultivates conversations about the recovery progress, increased reflection, and ‘deeper personal and shared understandings’ of the recovery journey (Hancock et al., 2016, p. 9). A second paper version of the instrument was completed on the final day of the programme; 94.2% of the initial sample of consumers also completed the measure at time two (n = 99).
Data processing and statistical analysis
Responses were collated, de-identified, and digitised using Excel (Microsoft Corporation, 2023). Scores at time one and time two were summed within each recovery domain per the relevant instrument items as described above. The resulting data were imported into the open-source statistical software package Jamovi (v2.3.21.0, 2023) for subsequent statistical analysis. Descriptive statistics (mean, standard deviations) were calculated for the scores in each of the four recovery domains, as well as for the demographic data of age. A 2 (Time: Pre, Post) x 4 (Recovery Domain: DTV, LF, MMI, CB) RM-MANOVA was conducted on the scores to test for any changes in recovery in association with attending the recovery-oriented programme. Significance levels for all post-hoc analyses were adjusted using the Bonferroni correction.
Results
The RM-MANOVA identified a main effect of time on recovery scores, F(4, 95) = 2.87, p = .027,
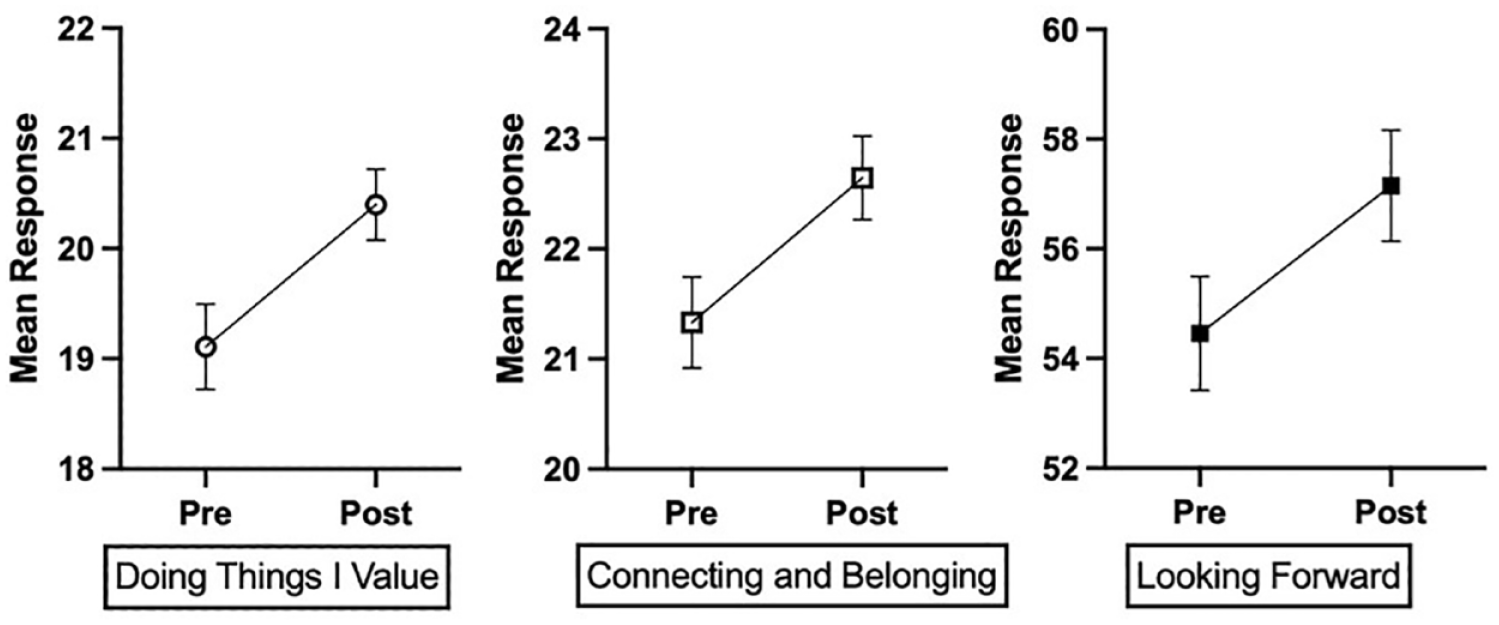
Self-reported consumer recovery scores increased after attending the recovery-oriented programme. Positive changes were observed in functional (left), social (middle) and personal (right) recovery domains. Higher scores indicate more advanced recovery progress. Error bars are the standard error of the means.
Discussion
Recovery as a concept reflects the shift in mental health care from a long held medical model towards a recognition of a person being an active agent in their own life (Picton et al., 2018). This psychosocial lens has at its heart, a more person centred, strengths based, and trauma informed approach. In this regard, tools such as the RAS-DS, as described above with its confluence of factors, contributes to understanding where a person feels they are on their recovery journey through four domains. The intersectionality of these domains assists with gaining insight into a person’s mental health recovery by capturing and valuing the person’s insider knowledge and priorities in relation to understanding what they value, what they look forward to, whether they feel they are ‘mastering’ their illness, and their sense of connection and belonging.
This research found positive changes in terms of ‘Doing things I value’. Within this domain the importance of having fun, pursing new interests, having healthy habits, doing things that are meaningful and give a feeling of pleasure, and doing things that are helpful to others, gives someone a purpose in life. Having a Purpose in Life (PIL) that orients one’s behaviour as well as providing a sense of direction is considered to be a key ingredient of a meaningful life and a central component of well-being (Crego et al., 2021; Kim et al., 2020). Fundamentally, PIL is important for health protection (Shiba et al., 2022). So much so, there is a growing body of research detailing that a higher sense of purpose is associated with improved health outcomes such as increased physical activity, preventive healthcare use, healthier sleep (Turner et al., 2017), reduced drug misuse (Kim et al., 2020), better biological functioning including reduced inflammation and allostatic load (Lewis & Hill, 2023), reduced risk of diseases (like cardiovascular disease), cognitive impairment, and better physical functioning (Kim et al., 2019; Willroth et al., 2021). As R. Cohen et al. (2016) found in their meta-analysis, a higher sense of purpose is also associated with reduced mortality. The participants in this current study were people living with mental illness and in that regard, evidence indicates that ‘positive psychological states such as having a sense of purpose, do not merely reflect the absence of poor mental health but that measures of psychological well-being independently predict less subsequent mental illness’ (VanderWeele et al., 2020, p.189).
The domain of ‘connecting and belonging’ was also seen to be positively affected in this study. According to Adler’s Individual Psychology theory, the inability to belong or to connect with others results in pathology (Watts, 2015). Long after Adler’s seminal theory, there is growing recognition that social inclusion, community participation and meaningful connections are essential to positive mental health and social recovery (Jay et al., 2023; Picton et al., 2020). According to Maslow’s Hierarchy of Needs, ‘love and belongingness’ refers to a human emotional need for interpersonal relationships, affiliating, connectedness and being part of a group (Maslow, 1943). This need recognises that human connection is a bond formed between people when they feel seen and when they feel valued and that during an authentic human connection, people exchange positive energy with one another and build trust (Jay et al., 2023). More recently the World Happiness Report in 2021 asserts that during COVID-19 physical separation may have curtailed the spread of the virus, but the practice of physical distancing and the reduction in the physical availability of social connections was concerning, as over a century of research has proven how crucial social connection is for well-being (Okabe-Miyamoto & Lyubomirsky, 2021). Preston and Rew’s (2022, p. 32) systematic review examining ‘what protective factors mitigate the effects of social isolation’, found that social connection was a protective factor for adolescent mental health.
‘Looking forward’, as a domain in the RAS-DS, included dimensions of hope and invited participants to respond to questions about being able to cope if becoming unwell, having the desire to succeed and having goals that one wants to reach. Moxham et al. (2017) assert that goal-setting within the sphere of mental health recovery is a means by which aspirations for the future can be explored and steps towards those aspirations can eventuate; speaking to notions of hope. Hayes et al. (2017) describe hope as the expectation or desire for positive events in the future. Hope is the route that underpins a personal recovery journey and is considered a core component of mental health recovery (Honey et al., 2023; Murphy et al., 2022). Laranjeira and Querido (2022) remind us that positive expectations for the future, (i.e. looking forward) commonly conceptualised as hope and optimism in the literature, can act as potential mechanisms towards achieving positive mental health, which ultimately is the aim of us all.
Limitations
This study is not without limitations. As a result of the questionnaire being administered at the completion of the intervention, it is not known whether the improvements were maintained after participants returned home. A 3-month follow-up study could be carried out to test the longevity of the effects of the Recovery Camp clinical experience.
Conclusion
This paper detailed how the RAS-DS was utilised to examine the impacts of an intervention camp on changes in recovery. Analysis of results from the purposive sample of consumers living with enduring mental illness revealed the importance of a purposeful life, connection and belonging, and optimism and hope. The paper demonstrated the efficacy of a strength based, trauma-informed therapeutic recreation camp as a recovery-oriented intervention. Recovery from mental illness is no longer defined by symptom resolution, but as a journey towards a meaningful life from the consumer’s own perspective. It is clear that looking outside the box of traditional approaches and more towards community based psychosocial interventions should be considered a serious strategy in a personal recovery journey. The authors therefore recommend this type of intervention as a recovery-based approach to mental healthcare and as a positive tool for working with people with mental illness to achieve their recovery outcomes.
Footnotes
Acknowledgements
The authors wish to thank the participants of the research for their time and effort in completing surveys.
Author contributions
Jay: Conceptualisation, Writing, Reviewing and Editing; Moxham: Supervision, Conceptualisation, Methodology, Writing, Reviewing and Editing; Roberts: Statistical Analysis, Writing, Reviewing and Editing; Yousiph: Software, Data Curation, Statistical Analysis, Writing, Reviewing and Editing; Robson: Software, Data Curation, Writing, Reviewing and Editing; Lewer: Writing, Reviewing and Editing; Patterson: Conceptualisation, Methodology, Writing, Reviewing and Editing.
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Recovery Camp is a research and social impact programme that has been supported by the University of Wollongong to explore its potential as a social enterprise. Authors C. Patterson and L. Moxham are directors of Recovery Camp Pty. Ltd.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from the relevant institutional ethical board (approval no: 2019/ETH03767).