
Abstract
Objective:
Individuals with severe mental illness (SMI) are disproportionally affected by medical comorbidities, resulting in poor physical health and premature death. Despite this, care for chronic medical conditions is suboptimal, and there is limited research that explores this phenomenon from the patient’s perspective. The aim of this study was to identify barriers and facilitators of engagement with a physical health service experienced by individuals with SMI.
Methods:
Adults with SMI were recruited from a large psychiatric hospital and offered referral to a physical health service focused on the prevention and treatment of obesity and diabetes. Interviews were conducted at referral, 3, and 6 months. Data from 56 interviews of 24 participants were analyzed using the framework method to identify factors influencing engagement.
Results:
Barriers to engagement were identified at individual, medical program, and health system levels. Factors influencing the individual experience included difficulty in care coordination, affective symptomatology, and ability to bond with providers. Factors at the program level included difficulty adjusting to the clinic environment and the inability to achieve treatment goals. Factors at the system level included challenges in attending multiple appointments in a fragmented health system, lack of social support, and financial constraints.
Conclusions:
This qualitative study suggests that traditional models of medical care for chronic conditions pose challenges for many individuals with SMI and contribute to health disparities. Adaptation of medical care to populations with SMI and close collaboration between medical and mental health services are necessary to improve medical care and, subsequently, health outcomes.
Introduction
Individuals with schizophrenia and other forms of severe mental illness (SMI) have poorer physical health relative to the general population, resulting in disproportionately high rates of mortality from medical comorbidities. 1 The high burden of medical morbidity and mortality is associated with a 15- to 20-year shorter life expectancy 2 and excess health-care costs. 3 While this population is at risk of a myriad of medical illnesses, cardiovascular disease (CVD) is the leading cause of death, accounting for as much as 50% of all cases. 4 Advances in the screening, identification, and management of CVD and its risk factors have successfully decreased its lethality in the general population, which raises concerns as to why patients with SMI have not equally benefited from these advances. 5
Multiple factors contribute to excess medical morbidity in this population; the symptoms of a mental illness may interfere with receiving medical care, cognitive deficits compromise effective communication of medical symptoms, 6,7 and low health literacy contributes to unhealthy lifestyles such as tobacco smoking, low levels of physical activity, and poor diets. 8 Iatrogenic factors are also an issue, as atypical antipsychotics used in the treatment of SMI have been implicated in metabolic abnormalities such as weight gain, diabetes, hyperlipidemia, and hypertension, all of which are precursors of CVD. 9
Another obstacle to health care in this population is the fragmentation of care between primary and mental health-care services which can lead to uncertainty regarding which provider carries the responsibility for the physical health issues of those with SMI. Mental health providers may lack the skills to identify and manage medical comorbidities, and physical health-care providers may be unfamiliar with the management of mental illness. 10 Even with access to physical health services, the quality of care delivered to persons with SMI often is suboptimal relative to that seen in the general population. 11 For example, at the time of patient enrollment into the Clinical Antipsychotic Trials of Intervention Effectiveness schizophrenia trial, no-treatment rates of medical comorbidities were 30% for diabetes, 62% for hypertension, and 88% for dyslipidemia. 12
A call for action was issued by professional psychiatric organizations urging mental health services to address common medical comorbidities either by integration of basic physical health care into mental health services or by collaboration with primary and specialist care. 13,14 Designing, or redesigning, health-care processes from the patient’s perspective has been a key concept in contemporary medical improvement efforts 15 and essential for creating successful and sustainable medical services for individuals with SMI. Some qualitative studies have detailed the difficulties patients with SMI face when accessing medical care in acute care settings such as stigma and communication difficulties. 16,17 However, little is known about the experiences this population encounters when seeking continued specialist care for chronic medical conditions.
This study addresses this gap and details the experiences of patients with SMI who were referred by their mental health providers to a community medical program to receive evidence-based care for the prevention and treatment of obesity and diabetes, two common chronic medical conditions found in SMI populations. 8 The objective of this qualitative study was to examine participants’ experience of engagement with a physical health service for chronic medical conditions that necessitate longitudinal care. We used these experiences to propose adaptations to care delivery that are patient-driven. The findings are valuable for health-care providers and administrators across primary, specialist, and mental health-care systems who wish to design a medical service that will engage and retain persons with SMI in care for their chronic medical conditions, thereby minimizing inequalities in health outcomes that shorten life span in this vulnerable group.
Methods
Design, Setting, and Recruitment
We used the theory of social construction to understand the experiences described by the participants of the study. This approach posits that an individual’s reality is shaped through their experiences and interactions with others. Social construction assumes that an individual’s perceptions and knowledge are dynamic and can change according to historical, geographical, social, and cultural contexts and thus may challenge the notion that a single reality is a direct representation of the “real world” exists. 18 In this study, we are not focusing on the disease (the biological condition). Instead, we seek to understand the social meaning of the condition from the perspective of the study participants. This research was informed by Goffman’s work on stigmatized illnesses. 19 Stigma is a social phenomenon that causes an individual to be classified by others as undesirable and thus discredited and rejected by society. Individuals with a stigmatized illness are perceived by society as having a “spoiled” identity. 19 Society attributes more stigmatizing stereotypes toward disorders such as schizophrenia, which have more visible symptoms than other mental disorders such as depression. 20 Therefore, individuals with a stigmatized illness are much more difficult to treat and manage because they are less likely to seek help for fear of being mistreated by clinicians. 21 Our study population—individuals with SMI who are also at risk of obesity and diabetes—could be considered a stigmatized group, given the negative attributes associated with their illness.
Participants with SMI were recruited from the Centre for Addiction and Mental Health (CAMH), a large urban academic psychiatric hospital, when they responded to a query regarding participation from their treating clinician in one of three CAMH services—the Partial Hospitalization Program, which cares for individuals recovering from an acute illness episode, the Downtown East Clinic, an assertive community treatment program, and the Mental Health and Metabolism Clinic, a medical consultation service for metabolic dysregulation. The three different services were chosen to ensure diversity in participants’ age, illness duration, and severity. To participate, individuals had to be ≥18 years of age, be able to converse in English, provide informed consent, and be diagnosed with a psychotic illness or bipolar disorder as identified by the referring clinician. They also had to be taking an antipsychotic for ≥4 weeks or be overweight or obese (body mass index ≥ 25 kg/m2). Individuals with significant suicidal ideation as documented by the referring clinician and those with a history of neurological impairment were excluded. Recruitment continued until no new themes or patterns (data saturation) were achieved to allow a rich representation of participants’ experiences. 22
Potential participants were provided with information about the study, and written consent was obtained. After consenting, participants who expressed interest in a referral were sent to Wharton Medical Clinic (WMC), a publicly funded interdisciplinary community program that delivers evidence-based care for prevention and treatment of obesity and diabetes. 23 Those who declined the medical referral were invited to participate to understand what influenced their decision not to seek treatment. Those who accepted the referral were followed over time. Once a participant’s medical referral was sent from CAMH, staff at WMC contacted the participant and booked an initial appointment as per the standard clinical care pathway. The treatment protocol at WMC involved an initial two-hour medical assessment to allow for anthropometric measurements, a 20-min educational session on nutrition delivered by a trained nutritionist, and a physician consultation for the management of obesity and diabetes. In subsequent visits (once to twice monthly), weight is monitored; the nutritionist delivered a 20-min session regarding weight management and provided individualized strategies for weight loss. This is coupled with ongoing physician management of both medical conditions. As both obesity and diabetes are chronic medical conditions, there is no defined program length. Approval was granted by the Research Ethics Board (REB) at the CAMH in Toronto, Ontario, Canada, in October 2016 (REB#1258).
Data Collection
In-person semistructured interviews were conducted by a trained researcher (I.F.) to provide insight regarding participants’ engagement with the medical program. The interview guide included demographic information and a set of questions to explore barriers and facilitators to engagement (Table 1). Individual interviews lasted between 20 and 45 min and were conducted using open-ended questions to explore what was most important from the participant’s perspective. At the end of each interview, the interviewer reviewed the collected responses with the participant to allow for corrections and elicit additional clarifications. Data collection occurred between October 2016 and March 2018.
Interview Questions.a
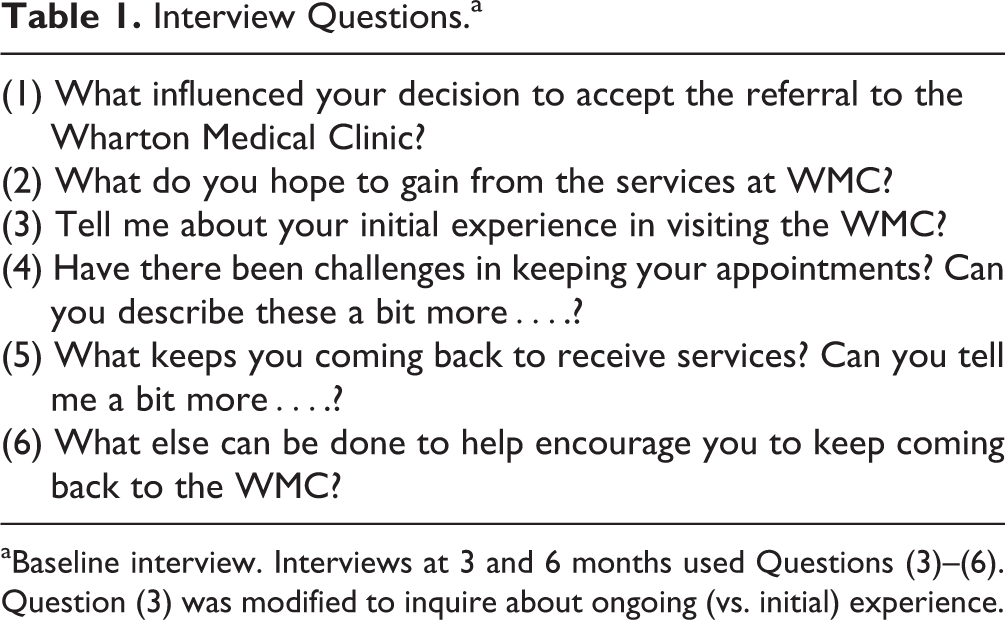
aBaseline interview. Interviews at 3 and 6 months used Questions (3)–(6). Question (3) was modified to inquire about ongoing (vs. initial) experience.
Data Analysis
All data were audio-recorded, unless otherwise requested by the participant, transcribed verbatim, anonymized, then analyzed using the framework analysis method described by Ritchie and Spencer. 24 The framework method uses distinct stages of data analysis: familiarization with data, theme identification, applying the thematic framework to entire data set, charting the data under the established thematic framework, and lastly, interpretation of the perceptions, accounts, and experiences appearing in the thematic framework. 25 All transcribed data were coded in a deductive manner into themes using Microsoft Excel. Under each theme, subthemes were identified in an inductive/open-coding manner. The lead author (O.C.M.) participated in coding at all stages of the analysis and facilitated the discussion with members of the research team. To ensure rigor in analysis, our team included researchers with varied professional backgrounds: psychiatry (V.H.T., M.K.H.), family medicine (O.C.M.), psychology (I.F.), social science (S.S.), and health service administration (K.W.L.). The findings from the interviews were discussed in an iterative process during data analysis. All research team members were affiliated with CAMH. One member was a psychiatrist (M.K.H.) who referred patients to the Wharton Medical Clinic. This manuscript was written in accordance with the Standards for Reporting Qualitative Research guidelines. 26
Results
Participants and Interviews
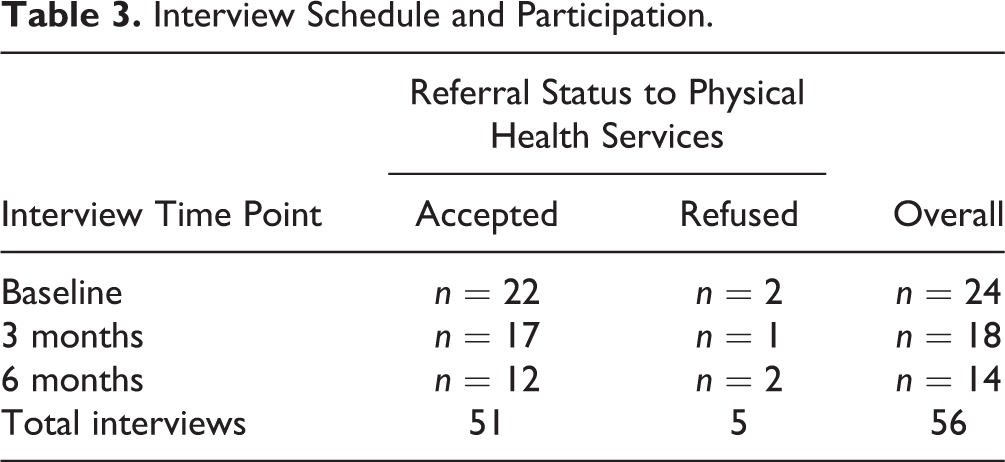
Thirty-eight participants were referred to the study and of that, 24 participants initially provided informed consent (mean age 37.1, SD 10.8; 13 women). Of those, 22 participants accepted the referral to the medical clinic, while 2 declined the referral but consented to participate in the study. Due to loss of follow-up, 18 participants remained in the study at 3 months and 14 were available at the 6-month mark, whereas one participant withdrew during the study. The cohort presented with a mix of mental health diagnoses including schizophrenia (n = 14), bipolar disorder (n = 3), and psychotic depression (n = 2). They endorsed illness durations that ranged from 1 to 5 years (n = 9), 6 to 10 years (n = 5), and >10 years (n = 10). One participant was not able to provide this information. Participant characteristics and interviewing schedules are summarized in Tables 2 and 3, respectively.
Demographic and Socioeconomic Characteristics of Participants.
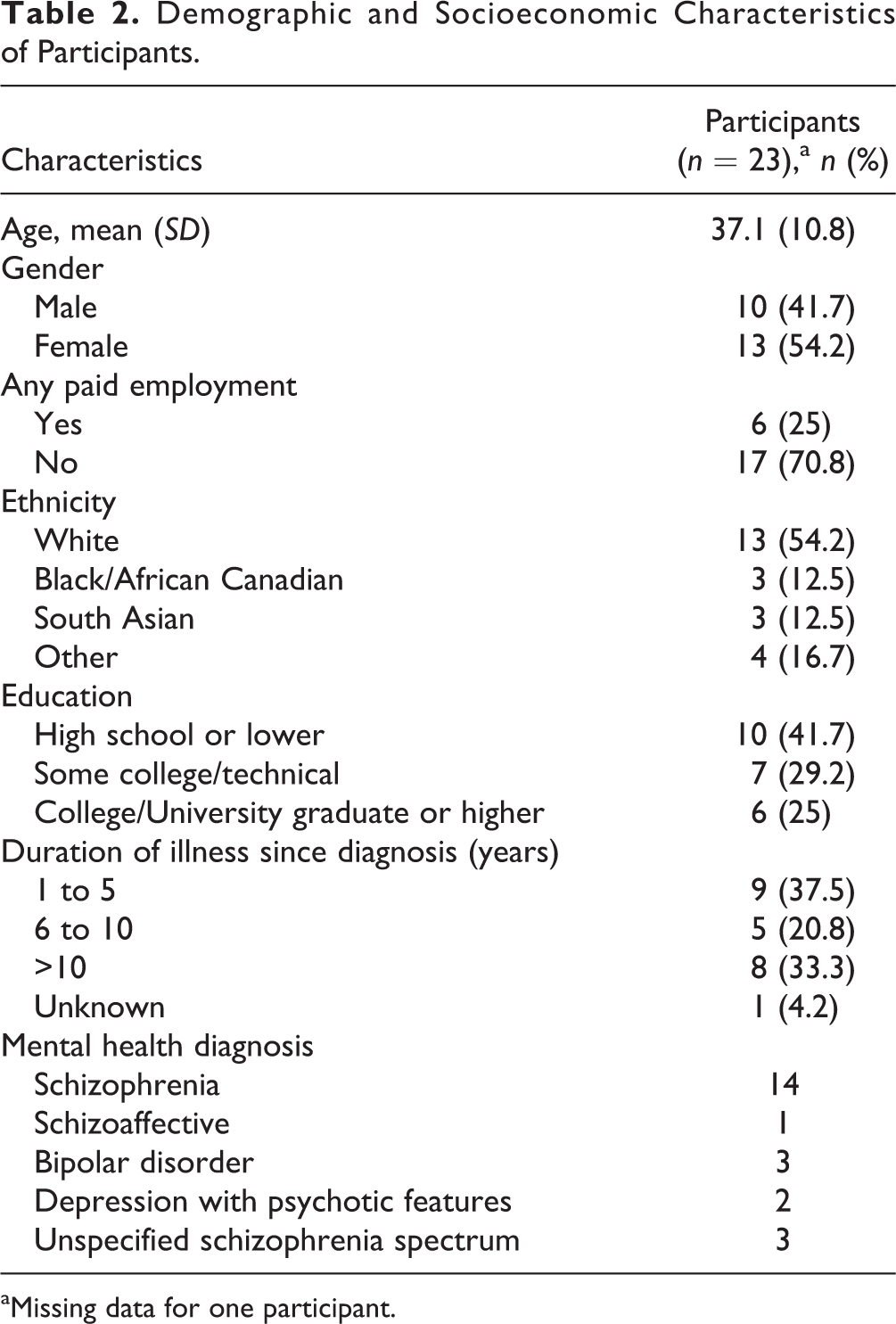
aMissing data for one participant.
Interview Schedule and Participation.
Overview of Themes
Through the lens of social construction and Goffman’s work on stigmatized illnesses, we focused on the experiential dimensions of illness. 19 Thus, we organized our findings into three different levels of analysis: the micro level which examined the factors that influenced an individual’s experience with the program, the meso level which examined how services were provided, and the macro level which considered the role of societal or systemic issues that impact medical care. Although many themes overlapped, which is common in qualitative research, we arranged the themes to highlight the personal, the programmatic, and the systemic factors that influenced our participants’ experiences of engaging with a physical health service. Quotes are provided in italics and followed by the source and time point of the interviews at baseline, 3, and 6 months after referral (B/3 m/6 m).
Micro level—Factors influencing an individual’s experience
Many participants accepted the referral to the medical program because they saw a clear benefit in receiving treatment at a specialty clinic, in this case an obesity and diabetes clinic. Perceived benefits were gaining knowledge in obesity management (i.e., topics of physical activity, nutrition, and healthy eating habits), acquiring practical tools, and receiving motivational support for health behavior change. This was particularly important for participants who had gained weight due to antipsychotic use “…I just want to get my weight under control which is really hard to do with (antipsychotic) medications and stuff” (PP008/B). Beyond the need for medical support around weight, the fact that a trusted mental health-care provider offered it to the participants increased its acceptability: “Well, since Dr. X (psychiatrist) recommended it…it kind of made sense. She would know best since she also knows the impact of the medications on my weight” (PP001/B).
Despite holding positive attitudes toward the medical program, participants described challenges in engagement including difficulty in care coordination, affective symptomatology, and inability to bond with medical providers. For example, several participants were unable to arrange for their appointments: “There’s been a lot of back and forth with the clinic. They (clinic staff) didn’t follow up and just left me a message. I didn’t know I had to call back and I also have a lot on my plate…so it’s kind of hard to manage. I forget and then remember but something usually comes up” (PP005/B). Many participants wished for support from the hospital to help with scheduling “Maybe if the Partial Hospitalization Program (at CAMH) could help with the scheduling because right now it’s up to me and it’s hard to manage” (PP021/6 m).
Several participants described how affective symptomatology such as exhaustion and low motivation was a barrier to attending and feeling successful in this program. Having motivation was described as an overwhelming task, and while participants articulated a desire to do things, physically and psychologically they were unable to achieve the goals they set for themselves. As one participant articulated: “My weight hasn’t changed and it’s really demotivating. Like, I have a pretty good understanding of the recommendations they give, and I want to keep making my own effort but at every visit they keep telling me to exercise and thing is I don’t have any motivation. And it’s not because I don’t want to, but I can’t. Getting out of bed is hard enough” (PP015/3 m). For some participants, their affective symptoms completely prevented them from attending services. According to this study participant: “I stopped going to my appointments unfortunately. I’ve been really ill…I’ve been feeling tired and really exhausted so I can’t get out of bed to go anywhere” (PP012/6 m). Affective symptomatology interfered with attendance especially when appointments were booked in the morning, “…in the mornings it is very tough to get up and early morning appointments aren’t the best” (PP005/B). Conversely, having the medical program accommodate for these missed appointments enhanced motivation to attend “They’re really good about trying to rebook me so I do make the effort because of that” (PP012/3 m).
A few participants described a lack of motivation for ongoing engagement with medical services that require long-term commitments. As this participant points out: “I went for a little bit but then I stopped going. I lost motivation over time” (PP022/6 m).
The quality of the relationship participants held with health providers also influenced engagement: “I’ve been going like a prayer to my appointments and now the staff knows me really well. It’s been an overall positive interaction” (PP014/3 m). On the other hand, when participants perceived care as impersonal, it interfered with engagement: “The atmosphere was really like an assembly line. It wasn’t a place of compassion and the empathy or personal touch wasn’t there with the care” (PP001/B).
Meso level—Factors related to medical program
Initially, some participants described difficulty adjusting to the clinic environment that was unfamiliar, crowded, and busy. One participant commented, “It is a busy place…I feel by myself” (PP014/B) and another stated, “It can be overwhelming and that sort of made me not want to go again” (PP001/6 m). Fitting in with the multidisciplinary medical program was also a challenge for some participants who came in with little knowledge regarding the offered program: “I was unsure of what to expect. My psychiatrist didn’t really tell me very much other than that it was a weight and diabetes management clinic” (PP003/B) and another participant commented: “It was unexpected…I anticipated an onsite gym with staff” (PP017/B).
Program efficacy played a key role in engagement, in that those who were able to achieve weight loss and change to healthier habits held positive attitudes toward the service: “I really need the help with weight management. I just lost 10 pounds in the last few weeks which has been great. So that’s the main thing for me. Extra support” (PP014/3 m). In contrast, some participants found the cognitive aspects of the medical program too demanding, which decreased their motivation to continue: “I felt like I couldn’t keep up with the homework…They also asked me to count calories and fat and I don’t have a computer” (PP007/3 m). Others questioned the efficacy of a generic medical program that is not specific to SMI populations who take antipsychotics: “I also don’t think what they are offering like lifestyle or exercise modification is even useful because at the end of the day the medication makes you gain weight even without eating more than usual” (PP001/B), and some participants expressed frustration that the program did equip with personally relevant content such as how to eat healthy on a budget: “I get that I have to eat better but I also need to be able to afford what they’re recommending” (PP002/6 m).
Macro level—Factors related to the health system
The unmet need for physical health care propelled many participants to join the medical program; however, geographic distance, financial constraints, and schedule conflicts with other medical appointments were common barriers.
Some participants noted the scarcity of obesity treatment options for individuals with SMI, especially for individuals with cognitive deficits: “It is difficult for a person with psychiatric difficulties to access support (for weight management). It is difficult for me, I have no computer knowledge and I don’t know how to go about it. I don’t find my family doctor all that in depth or helpful” (PP011/B). This increased motivation to attend the offered medical services: “I was also desperate and thought I’d take any help possible” (PP001/B). However, since geographic locations of the medical program were too far, many stated that they found this an insurmountable challenge: “I was unable to go…It’s just too far for me to travel…I don’t drive…I can’t go by myself” (PP010/B). Some participants overcame this challenge with support from family members or personal support workers provided by the health system: “My support worker joins me and that’s really helpful” (PP011/3 m). Travel costs to medical appointments also posed a barrier for some: “Well, I can’t really afford (transit) tokens to get there. That is a problem” (PP012/B).
Fragmentation of health services into mental and physical health care creates a plethora of appointments which was cited as a barrier by some participants for attending the medical service: “I didn’t go because I ended up feeling very overwhelmed with other appointments in general” (PP019/B). This was a significant barrier especially for participants who reported full-time work/school commitments: “I volunteer and go to school so making time for these appointments is difficult” (PP08/3 m). This prompted the notions of integration of physical health services within mental health services: “I think there needs to be a (weight management) clinic at CAMH; it’s just easier with my other appointments” (PP022/3 m) or a remote care delivery using technology: “I wonder if they can have a service like Skype appointments or something” (PP010/3 m).
Discussion
Our findings suggest that participants with SMI have initial positive attitudes toward involvement in medical care targeting chronic medical conditions, but ongoing engagement with medical services is influenced by a multitude of factors at the individual, program, and health system levels.
To the best of our knowledge, this is the first qualitative study to examine the experience of engaging with a medical program for chronic medical conditions in the context of having a SMI. The findings provide insight into the challenges individuals with SMI face when they present for medical care. Since this population is disproportionally affected by chronic medical comorbidities, it is crucial to design medical services based on the service-user perspective.
Successful health-care delivery for chronic medical conditions necessitates long-term engagement to allow for uptake of new treatments and ongoing monitoring to ensure health maintenance over time. Our study employed a longitudinal design over the course of 6 months. We found that individual factors such as fluctuating levels of motivation and depression undermined long-term engagement with the medical program. 27 This barrier may be overcome by increasing contact time including longer visit duration and frequency of appointments as well as leniency toward missed appointments. 28 Establishing a therapeutic rapport between participants and medical staff was found to be contributing to engagement of participants, whereas failure to achieve rapport was a significant barrier. This issue is of importance as health-care providers who lack understanding of mental illness may deliver care that is perceived as noncaring, impersonal, and stigmatizing. 6,29 Factors related to the medical program were also found to influence participant engagement. Consistent with previous reports, certain environments such as noisy and crowded waiting rooms are a deterrent to some participants. 30 Most participants struggled to adjust to a multidisciplinary medical program, specifically as they had limited knowledge and prior experience with this type of health-care delivery model. However, having a trusted mental health-care provider endorse the service helped alleviate some concerns from the unfamiliar. Certain characteristics of the medical program also influenced engagement. For individuals with cognitive limitations, self-management tasks were perceived as overwhelming at times and could be addressed by peer-led programs that offer support for self-management of chronic medical conditions. 31 For others, disappointment with the lack of specific advice offered to individuals with a SMI led to the conclusion that there were few benefits from participation in the program. For instance, food insecurity, which disproportionally affects people with mental illness, prevented participants in our study from following a recommended diet plan. 32 This illustrates the importance of medical care providers having awareness to the socioeconomical vulnerabilities found in this population. Individuals with SMI are more likely to experience poverty and lack social support which must be accounted for in their health-care delivery. 10 Reimbursement for travel costs and allocating support workers to accompany individuals to appointments may improve engagement. Many participants noted that finding the time to attend medical appointments was challenging since they also have to attend a myriad of health appointments, reflecting the complexity of this population. Fragmentation between physical and mental health services adds to this challenge. Possible solutions include the integration of medical services within mental health services or care coordination between mental health and medical services. 33,34
Limitations and Strengths
The results of this study were obtained in a population currently engaged in mental health care, who expressed interest to be referred to a medical service by their mental health program. Despite our intention, we were unable to recruit a sizable sample of individuals who refused the referral. Future research is needed on how to optimize medical care for those with low interest or motivation. This study targeted individuals referred to a specific program. It is possible that issues identified are unique to this setting. It is also important to highlight that research bias exists and a thematic analysis is influenced by researchers’ interpretation. To mitigate this, we included researchers from diverse backgrounds. To ensure the validity, rigor, and credibility of our study, we anchored our findings within a theoretical framework, met several times to discuss the results, and worked iteratively through consensus to analyze the findings. 35,36 A strength of this study is its longitudinal design that allowed us to assess the full extent of factors that moderate long-term engagement with care for chronic medical conditions. Although pursuing this design proved challenging for participants and researchers alike, it highlighted critical issues that were used to inform implications for practice.
Conclusions and Practice Implications
Populations with SMI are disproportionally affected by medical comorbidities, and CVD is the leading cause of premature death. This qualitative study provides insight to the well-documented phenomenon that SMI patients receive poorer quality of medical care relative to their healthy peers. Our study used the patients’ perspective to address knowledge gaps by describing many of the factors at the individual, medical program, and health system levels that interfere with medical care delivery. Based on our findings, we provide a series of recommendations to help improve the engagement of those affected by SMI in a medical setting.
Practice Implications
Individuals with severe mental illness (SMI) should be empowered by all health-care providers to pursue proper physical health care and given information about physical health services available to them. Trusted mental health providers can positively influence the acceptability of medical services among their patients and therefore need to be informed of their patients’ physical health status and needs. Simply endorsing connection with a different health-care provider regarding a health issue can impact behavior change.
Fragmentation of care between mental and physical health care for individuals with SMI, who often lack other social support and are cognitively challenged, was a barrier found by us and others. Care delivery that integrates physical and mental health care or at least provides care coordination for physical health services can overcome this barrier.
Physical health services, in particular those that address chronic medical conditions, should be aware of the social, medical, and cognitive challenges faced by individuals with SMI and attempt to provide care tailored to their unique circumstances. This includes providing a combination of written and verbal information, making tasks smaller and attainable, conceptual reiteration with one-on-one augmentation if needed, as well additional contact time and leverage of social support.
Physical health services should aim to have available if possible, access to a safe environment space (i.e., quiet, noncrowded room) and attempt to offer flexibility in appointment scheduling for patients with SMI. Introduction to the services can be done ahead of time via technology such as an orientation video, thus reducing anxiety from the unfamiliar.
Health-care providers both in mental and physical health care should be offered education to improve their knowledge and confidence around management of physical health in patients with SMI. Provider training is key to establishment of referral networks, effective collaboration, and increased capacity to address both physical and mental health needs.
Educational efforts should target health-care providers’ stigma against patients with SMI, as stigma has been consistently reported by this group as a barrier for receiving physical health care. Respectful encounters that offer warmth and optimism are paramount to building strong patient–provider relationships and facilitating engagement.
Footnotes
Acknowledgments
The authors wish to thank the participants for their contribution to this study and acknowledge the reviewers’ constructive feedback that has strengthened this manuscript.
Data Access
Data collected in this study are restricted in access for privacy reasons in accordance with the Research Ethics Board approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Medical Psychiatry Alliance at the Centre for Addiction and Mental Health.