
Abstract
Objective:
It has been shown that men with a longstanding psychotic disorder have worse clinical and functional outcomes than women. Our objectives were to examine whether these sex differences are also present among patients treated in an early intervention service (EIS) for psychosis and to determine if these differences are related to risk factors other than sex.
Method:
Patients (N = 569) were assessed for demographic/clinical characteristics at entry and for symptoms/functioning over 2 years of treatment. Clinical outcomes included remission of positive, negative, and total symptoms. Functional outcomes included good functioning and functional remission. Logistic regression models examined the relationship between sex and outcomes after 1 and 2 years of treatment while controlling for the influence of other risk factors.
Results:
Men reported to be less educated and have a longer duration of untreated psychosis, poorer childhood and early adolescent premorbid functioning, higher rates of substance abuse/dependence disorders, greater severity of baseline negative symptoms, and poorer baseline social/occupational functioning than women. Women were more likely to achieve symptom remission than men after 2 years of treatment (negative odds ratio [OR], 1.69; 95% confidence interval [CI], 1.02 to 2.78; total OR, 1.79; 95% CI, 1.08 to 2.98). Women were also more likely than men to exhibit good functioning (OR, 1.61; 95% CI, 1.04 to 2.49) after 1 but not after 2 years of treatment. These results did not persist after controlling for other risk factors that could confound these associations (i.e., childhood premorbid functioning and age at onset of psychosis).
Conclusions:
Sex differences seen in outcomes among patients treated in an EIS for psychosis may be largely influenced by the disparity of other risk factors that exist between the 2 sexes.
It is generally accepted that men with a longstanding psychotic disorder have worse clinical and functional outcomes than women. 1 –3 Men often demonstrate poorer negative symptom outcomes than women, 4,5 which typically contributes to experiencing poor functional outcomes. 6,7 The worse outcomes seen in men may be attributed to sex-related differences in biology 8,9 as well as behavioural and social risk factors that predominate among men. Indeed, men generally exhibit an earlier age at onset of psychosis, 10 poorer premorbid functioning, 11 lower global functioning, 12 higher substance abuse rates, 13 and poorer cognition, 8 all known risk factors for poor outcomes. Furthermore, men show lower treatment response rates 2 and higher disengagement rates with psychiatric services. 14
Like those with a longstanding psychotic disorder, past reports suggest that men are less likely to achieve good outcomes than women in early intervention services (EIS) for psychosis. 4,5,15,16 However, these past findings may be limited for several reasons. First, most of these studies examined symptom severity as a measure of clinical outcomes rather than symptom remission. 4,5,15,16 The latter is often more desirable because of its stronger relationship with functional recovery. 7 Second, most of these reports examined functional outcomes as level of functioning, 4,5,15,16 which is less clinically meaningful than identifying those who are exhibiting good functioning 17 or are in functional remission. 18,19 Third, none of these studies controlled for important risk factors that have the potential to confound their results (e.g., age at onset of psychosis). 4,5,15,16,20 Finally, the generalizability of some of these findings is low given that some of these samples were derived from randomized controlled trials 5 (RCTs) and had experienced lengthy treatment delays (i.e., long durations of untreated psychosis [DUPs]). 4,5,20
In this report, we examine whether there are any sex differences in clinical and functional outcomes in a catchment area-based sample of patients treated in an EIS for psychosis. We also explore whether any of the observed sex differences in outcomes would persist after controlling for risk factors that could potentially confound our results. We hypothesize that any sex difference seen in outcomes will be largely affected by the disparity of other risk factors between the 2 sexes.
Methods
Participants and Settings
Data on patients receiving treatment in an EIS for psychosis (Prevention and Early Intervention Program [PEPP-Montreal]) between 2003 and 2016 and who had consented to participate in research were used in this study. PEPP-Montreal serves a French/English-speaking population of 300,000 inhabitants in southwest Montreal, Canada. The inclusion criteria for these services are age 14 to 35 years, diagnosis of nonaffective or affective psychosis, prior treatment with antipsychotics not >30 days, and an IQ ≥70 based on the short-form Wechsler Adult Intelligence Scale. 21 The exclusion criteria are major medical disorders that can explain the psychosis (e.g., traumatic brain injury) or substance-induced psychosis. Patients with concurrent substance abuse/dependence disorders are included.
The EIS offers lowest effective dose pharmacotherapy, assertive case management (ratio 20:1), family intervention, psychological therapies, psychosocial programs, crisis interventions, and interventions to reduce treatment delays. 22,23 At baseline, patients are approached to participate in a research protocol where trained research staff assesses demographic, clinical, and functional measures. Assessment of clinical and functional measures is repeated throughout the 2 years of treatment. Men and women who had completed at least 1 year of treatment and had functional measures data at baseline and at 1 year of treatment were selected for this study.
Assessment of Variables
Positive and negative symptoms were assessed using the Scale for Assessment of Positive Symptoms (SAPS) 24 and Scale for Assessment of Negative Symptoms (SANS). 25 Depression and anxiety were measured with the Calgary Depression Scale for Schizophrenia (CDSS) 26 and the Hamilton Anxiety Rating Scale (HARS). 27
Functioning was assessed using the Social and Occupational Functioning Assessment Scale (SOFAS) 28 and the Strauss Carpenter Scale (SC). 29,30 The SOFAS provides a global rating of social/occupational functioning in the past year, while the SC examines the degree of social contact (i.e., frequency of seeing friends/family) and education/vocation (i.e., amount of time spent in school or at work) of patients in the past year.
Age at onset of psychosis and DUP were determined from the Circumstance of Onset and Relapse Schedule 30 (CORS). CORS is a semistructured interview that is supplemented with information from families and educational/medical records. Age at onset of psychosis was defined as the age when the patient first exhibited a threshold level of psychotic symptoms. DUP was defined as the time (weeks) between the onset of threshold-level psychotic symptoms and the start of 30 days of continuous antipsychotic medication, consistent with previous reccomendations. 31 Premorbid functioning was assessed with the Premorbid Adjustment Scale (PAS), 32 which provides scores for social and academic functioning during childhood, adolescence, and adulthood. Given that the age at onset of psychosis often overlaps with late adolescence and early adulthood, 33 we considered only the PAS scores for childhood and early adolescence.
Antipsychotic medication adherence rates were calculated from assessments conducted 3, 6, 9, 12, 18, and 24 months into treatment with the use of a validated method that included information obtained from patients and their families, case managers, and clinical notes. 34 Patients taking 75% to 100% of their antipsychotic medication at each assessment were considered adherent, while those taking 0% to 74% at any point during treatment were considered nonadherent. Diagnoses for the psychotic disorder and concurrent substance abuse/dependence disorders were determined with the Structured Clinical Interview for DSM-IV. 35 Diagnoses for psychotic disorders were clustered as nonaffective (schizophrenia, schizophreniform disorder, schizoaffective disorder, psychosis not otherwise specified [NOS]) and affective psychosis (bipolar or depressive disorders with psychotic symptoms). Additional variables analyzed for this study (e.g., relationship status) were self-reported by patients at baseline.
Definitions for Clinical and Functional Outcomes
Clinical outcomes
Remission of symptoms was examined after 1 and 2 years of treatment. We defined patients to be in remission of symptoms if they had a symptom severity of mild or less at each assessment in the past 6 months, consistent with the recommendations from the Remission in Schizophrenia Working Group. 36 Patients scoring ≤2 on all global items on the SAPS at each assessment in the past 6 months were in remission for positive symptoms, while those scoring ≤2 on all global items on the SANS at each assessment in the past 6 months were in remission for negative symptoms. Those who achieved remission of positive and negative symptoms concurrently at each assessment in the past 6 months were in remission for total symptoms.
Functional outcomes
Functional outcomes were examined after 1 and 2 years of treatment. Scoring >60 on SOFAS was considered exhibiting good functioning. 17 Those displaying good functioning and in school/working full- or part-time in the past year (SC educational/vocational subscale score ≥2) were in functional remission. 18,19
Data Analysis
We examined sex differences in variables at baseline as well as after 1 and 2 years of treatment for clinical and functional outcomes. Independent t tests were used to explore for differences in continuous variables, while chi-square tests were conducted to examine for differences in binary variables. Continuous variables were described as unadjusted means with standard deviations, and binary variables were reported as percentages.
Bivariate logistic regression models were used to examine associations between sex and outcomes after 1 and 2 years of treatment. For significant bivariate models, we then adjusted for variables that may potentially confound the relationship between sex and outcomes. To identify potential confounds, we first examined the literature for previous reports that have linked variables independently to both sex and outcomes, respectively. We then examined whether any of these theoretical confounds from the literature may mediate the association between sex and the outcome via PROCESS 37 in SPSS (SPSS, Inc., an IBM Company, Chicago, IL). Each mediation model conducted 1000 bootstrapped samples. The theoretical confound was identified to be a significant mediator if the indirect effect of sex predicting the outcome did not contain 0 between its upper and lower bootstrapped confidence interval. For the theoretical confounds that were not found to mediate the association between sex and the outcome, we then adjusted for them in our multivariate models. All statistical tests in this study were conducted in SPSS version 23.0, and significance was set at α < 0.05.
Ethical and Consent Considerations
We assert that all procedures contributing to this work comply with ethical standards of the Douglas Institute Research Ethics Board and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the Douglas Institute Research Ethics Board. Written informed consent was obtained from all patients.
Results
Study Population and Sample
Of the 747 patients accepted for treatment in this EIS from 2003 to 2016, 569 consented to research (i.e., the study population) while 178 of these did not (Figure 1). Since these 178 patients did not consent to research, we cannot compare them with our study population as we were unable to collect any relevant data on them. Based on our selection criteria, 452 patients from our study population were eligible for analysis (79% of the study population). Those who were eligible had a significantly lower childhood total PAS score than those who were not eligible (0.21 ± 0.14 vs. 0.26 ± 0.15, P = 0.04) (Suppl. Table S1).
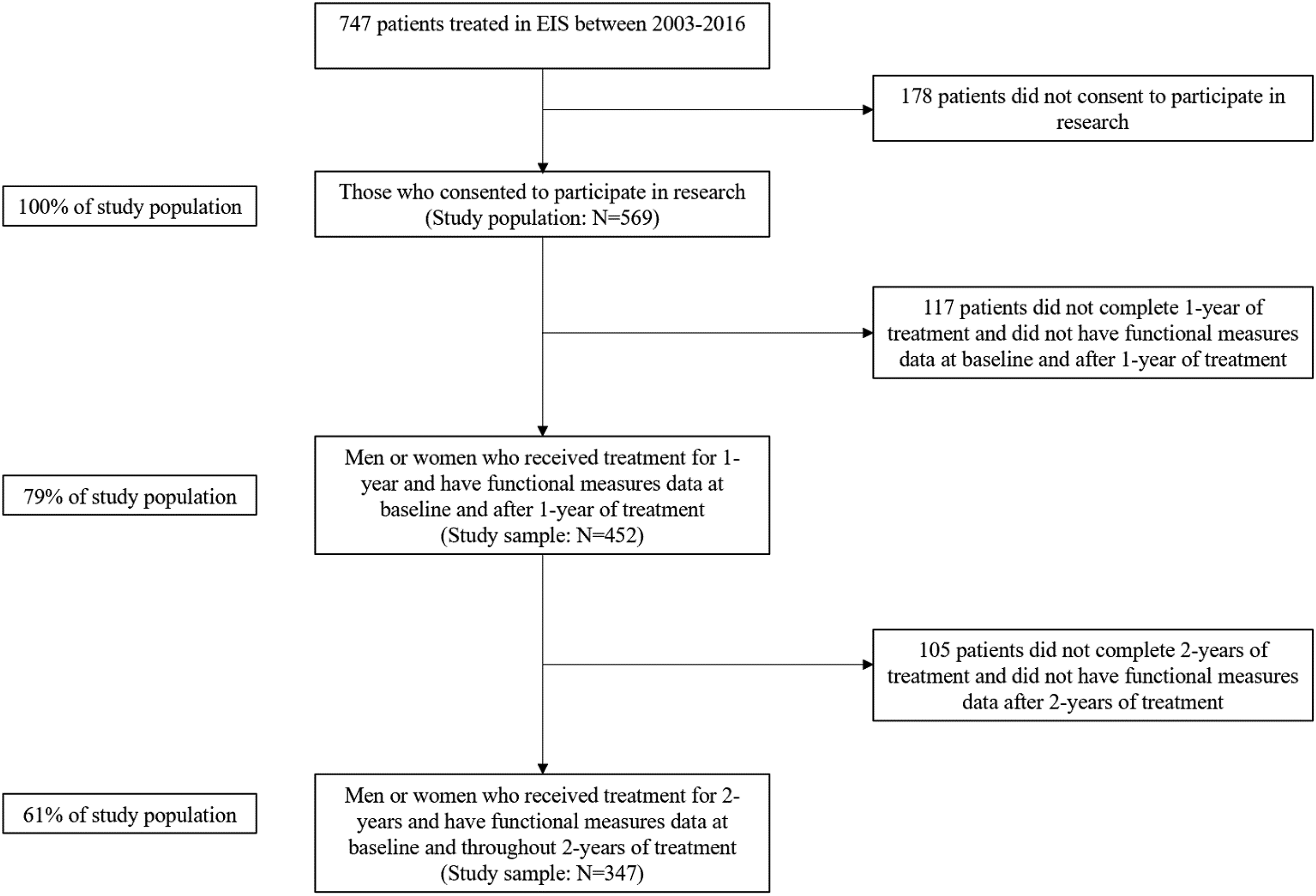
Flowchart of study population and sample. EIS, early intervention service for psychotic disorders.
Among our study sample (N = 452), 347 of these completed 2 years of treatment and had functional measures data throughout 2 years of treatment (61% of the total study population) (Figure 1). Women reported a significantly higher attrition rate than men (30% vs. 20%, P = 0.03). Those who completed 2 years of treatment (N = 347) were more adherent to antipsychotic medications during the first year of treatment than those who only completed 1 year of treatment (N = 105) (64% vs. 45%, P < 0.01). No other variable significantly differed between these 2 groups (Suppl. Table S2).
Sex Differences over 2 Years of Treatment
In our study population (N = 569), men (n 1 = 391) and women (n 2 = 177) differ significantly in their education status, DUP, total PAS score and academic PAS subscore during both childhood and early adolescence, substance abuse/dependence disorder rates, and SANS, CDSS, and SOFAS scores (Table 1). The sex difference in the age at onset of psychosis was borderline significant (Table 1). There were no significant sex differences in antipsychotic medication adherence rates during the first year of treatment (N = 452; 60% vs. 62%, P = 0.80) or throughout 2 years of treatment (N = 347; 52% vs. 61%, P = 0.21).
Differences in Demographics and Clinical Variables between Men and Women at Baseline from Study Population (N = 569).
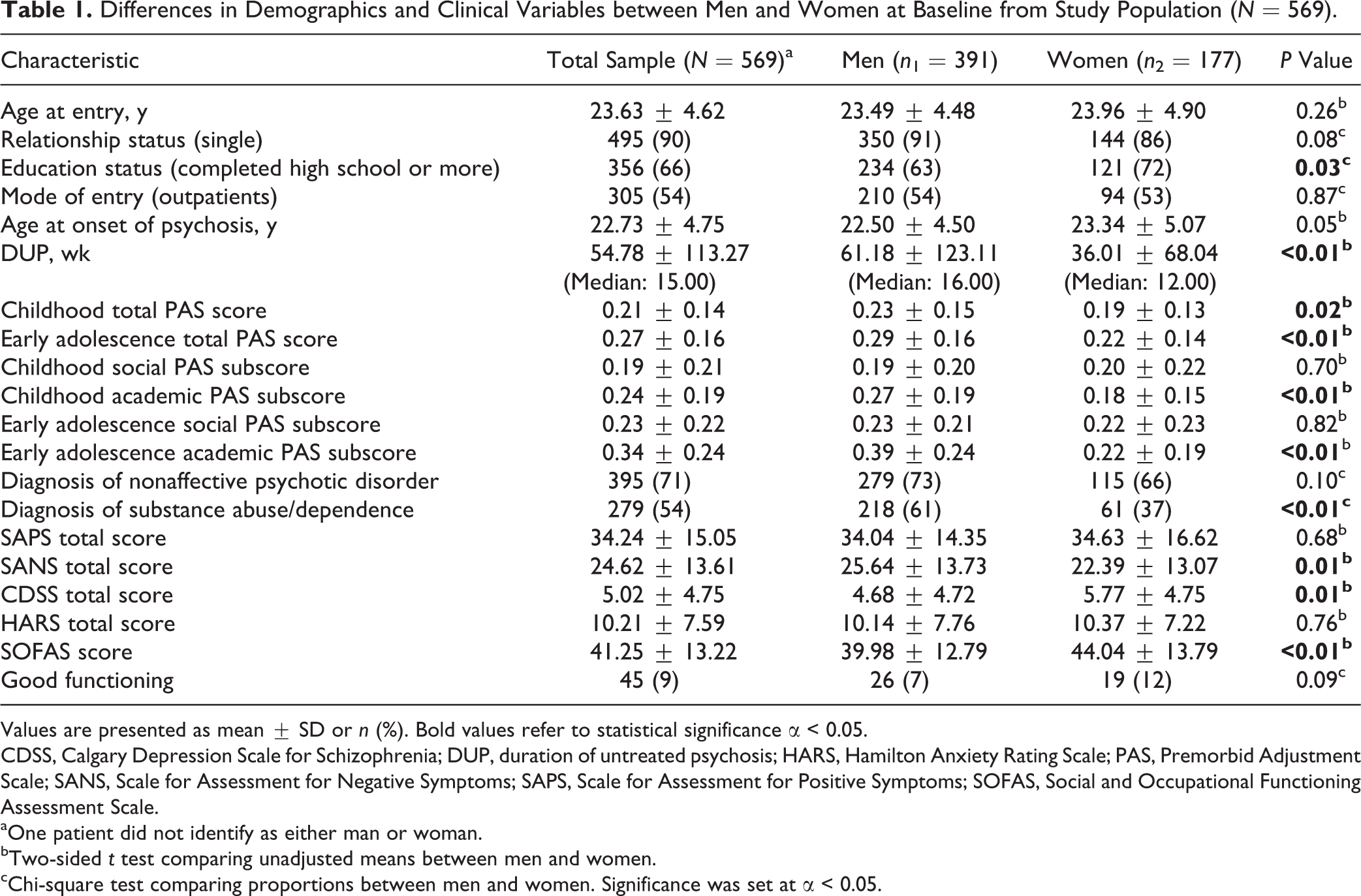
Values are presented as mean ± SD or n (%). Bold values refer to statistical significance α < 0.05.
CDSS, Calgary Depression Scale for Schizophrenia; DUP, duration of untreated psychosis; HARS, Hamilton Anxiety Rating Scale; PAS, Premorbid Adjustment Scale; SANS, Scale for Assessment for Negative Symptoms; SAPS, Scale for Assessment for Positive Symptoms; SOFAS, Social and Occupational Functioning Assessment Scale.
aOne patient did not identify as either man or woman.
bTwo-sided t test comparing unadjusted means between men and women.
cChi-square test comparing proportions between men and women. Significance was set at α < 0.05.
Clinical outcomes
There were no significant sex differences in symptom remission rates after 1 year of treatment (Tables 2 and 3). After 2 years of treatment, women were more likely than men to be in remission of negative (odds ratio [OR], 1.69; 95% confidence interval [CI], 1.02-2.78) and total symptoms (OR, 1.79; 95% CI, 1.08-2.98).
Differences in Outcomes between Men and Women following 1 and 2 Years of Treatment.
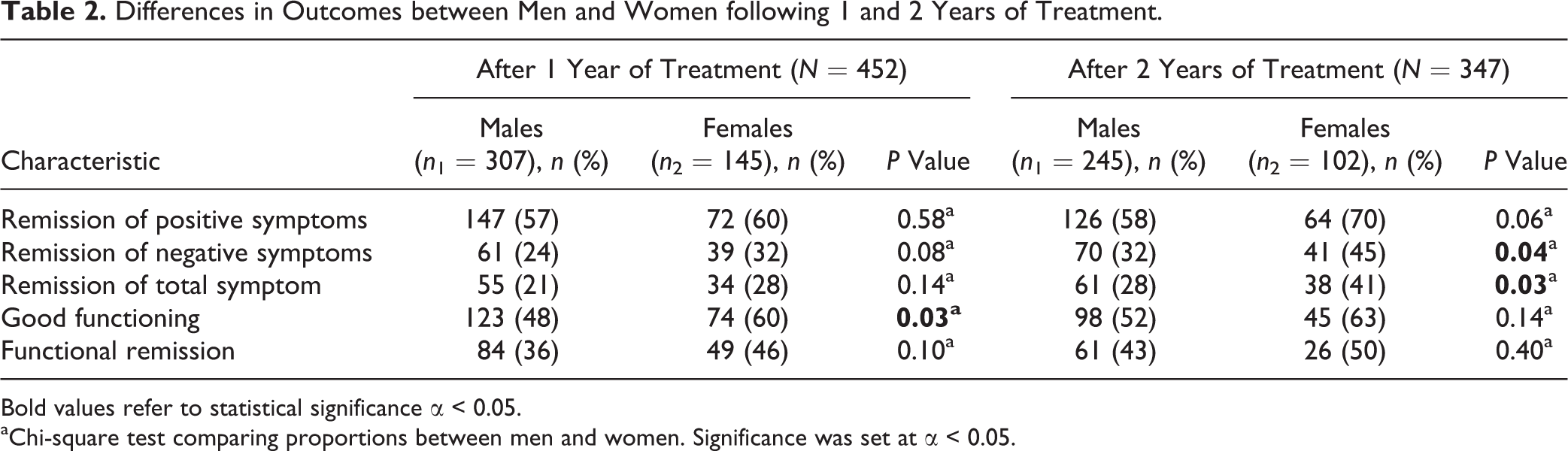
Bold values refer to statistical significance α < 0.05.
aChi-square test comparing proportions between men and women. Significance was set at α < 0.05.
Bivariate and Multivariate Analyses Comparing Sex Differences and Outcomes following 1 and 2 Years of Treatment.
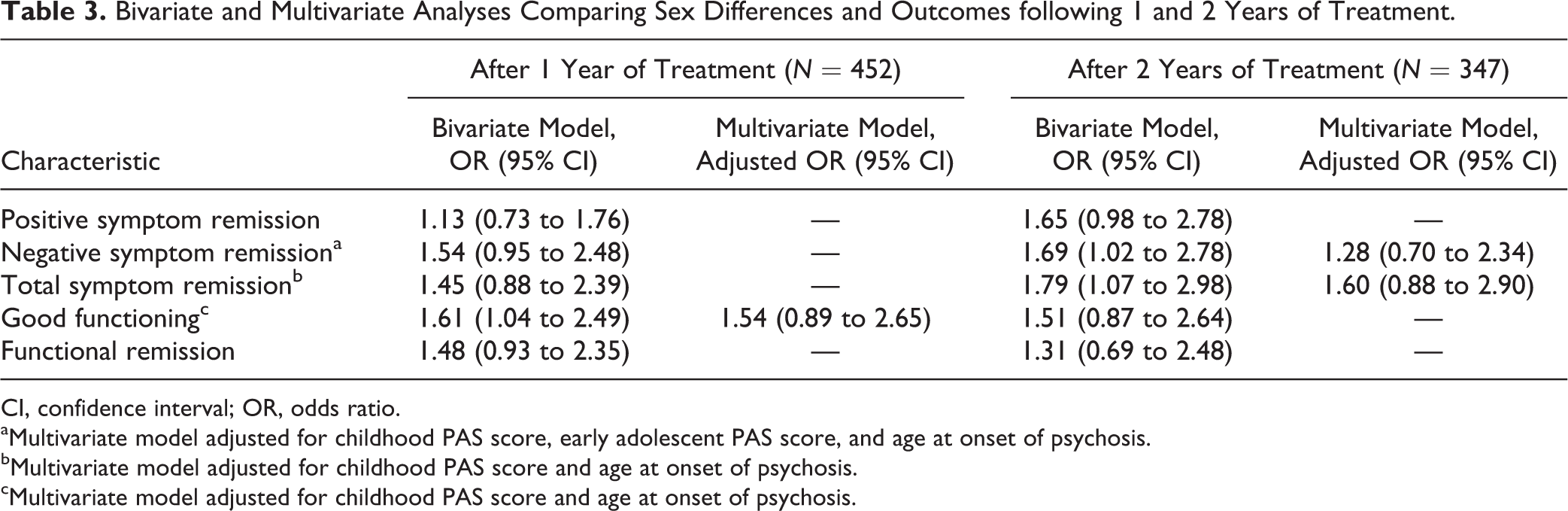
CI, confidence interval; OR, odds ratio.
aMultivariate model adjusted for childhood PAS score, early adolescent PAS score, and age at onset of psychosis.
bMultivariate model adjusted for childhood PAS score and age at onset of psychosis.
cMultivariate model adjusted for childhood PAS score and age at onset of psychosis.
Our literature review suggested that childhood premorbid functioning, 11,38 –40 early adolescent premorbid functioning, 11,38 –40 age at onset of psychosis, 10,41 and global functioning prior to treatment 7,12,15,20,38 may have the potential to confound the observed associations between sex and symptom remission. Mediation models indicated that only baseline SOFAS score produced a significant indirect effect on sex predicting negative symptom remission after 2 years of treatment (β = 0.0959 [Boot SE = 0.0618]; Boot CI, 0.0040 to 0.2478) (Suppl. Figure S1). However, total childhood PAS score, total early adolescent PAS score, and age at onset of psychosis did not demonstrate such significant results (Suppl. Figures S2-S4). Total early adolescent PAS score (β = 0.1658 [Boot SE = 0.1011]; Boot CI, 0.0016 to 0.4041) and baseline SOFAS score (β = 0.1105 [Boot SE = 0.0628]; Boot CI, 0.0119 to 0.2578) each produced a significant indirect effect on sex predicting total symptom remission following 2 years of treatment (Suppl. Figures S5-S6). However, total childhood PAS score and age at onset of psychosis did not exhibit such significant findings (Suppl. Figures S7-S8).
After controlling for potential confounds (total childhood PAS score, early adolescent PAS score, and age at onset of psychosis), sex no longer significantly predicted negative symptom remission after 2 years of treatment (adjusted OR, 1.28; 95% CI, 0.70 to 2.34). Sex also no longer significantly predicted total symptom remission after 2 years of treatment (adjusted OR, 1.60; 95% CI, 0.88 to 2.90) following the adjustment of potential confounds (total childhood PAS score and age at onset of psychosis).
Functional outcomes
After 1 year of treatment, women were significantly more likely than men to exhibit good functioning (OR, 1.61; 95% CI, 1.04 to 2.49) (Table 3). There was no significant sex difference in achieving functional remission after 1 year of treatment (Tables 2 and 3). Also, there were no significant sex differences in either of the 2 functional outcomes after 2 years of treatment.
Past reports suggest that childhood premorbid functioning, 7,11,38,39 early adolescent premorbid functioning, 7,11,38,39 age at onset of psychosis, 10,41 and the severity of negative symptoms prior to treatment 5,7,16 may potentially confound relationships between sex and functional outcomes. Our mediation model demonstrated that total early adolescent PAS score (β = 0.2312 [Boot SE = 0.0965]; Boot CI, 0.0772 to 0.4588) and baseline SANS score (β = 0.1098 [Boot SE = 0.0596]; Boot CI, 0.0066 to 0.2386) each had a significant indirect effect on sex predicting good functioning after 1 year of treatment (Suppl. Figures S9-S10). However, total childhood PAS score and age at onset of psychosis did not produce such significant findings (Suppl. Figures S11-S12).
After adjusting for potential confounds (total childhood PAS score and age at onset of psychosis), sex no longer significantly predicted good functioning after 1 year of treatment (adjusted OR, 1.54; 95% CI, 0.89 to 2.65) (Table 3).
Discussion
In this large and well-characterized sample of patients from an EIS for psychosis, we examined whether there were any sex differences in clinical and functional outcomes. Our results from unadjusted models showed that women were more likely than men to be in good functioning following 1 year of treatment (Tables 2 and 3). After 2 years of treatment, while women were more likely to have better clinical outcomes, there were no sex differences in any of the functional outcomes (Tables 2 and 3). After controlling for risk factors that could potentially confound our results, the observed sex differences in clinical and functional outcomes did not persist (Table 3). Therefore, our findings support our hypothesis that the sex differences seen in outcomes from an EIS for psychosis may be largely affected by the disparity of other risk factors between the 2 sexes.
The observed sex differences in functional outcomes were rather nuanced. Despite more women significantly exhibiting good functioning after 1 year of treatment, this sex difference was not present following 2 years of treatment (Table 2). Moreover, there were no significant sex differences in functional remission rates throughout 2 years of treatment. These findings suggest that EIS may require more than 1 year to effectively improve the overall functioning of men. This may be partially related to men in our sample presenting with poorer early adolescent premorbid functioning than women as we report that this variable was a significant mediator in the relationship between sex and good functioning after 1 year of treatment (Suppl. Figure S9). In addition, it is possible that the greater severity of negative symptoms seen among men may have limited their ability to engage with the psychosocial interventions aimed at improving their functional outcomes (e.g., employment/educational supported programs) during their first year of treatment. 42 Indeed, this is supported by the observed mediation of baseline negative symptoms on sex predicting good functioning after 1 year of treatment (Suppl. Figure S10). Therefore, reducing negative symptoms during the first year of treatment may be critical in improving functional outcomes. Patients may benefit from more frequent and intensive psychological therapies during their first year in EIS as multiple meta-analyses have suggested that these interventions are effective in reducing negative symptoms. 43,44 Furthermore, 1 meta-analysis has suggested that pharmacological options such as antidepressants or glutamatergic agents may also be helpful in reducing negative symptoms. 43
After 2 years of treatment, more women significantly reported to be in remission of negative and total symptoms (Table 2). These findings are consistent with previous studies suggesting that women may experience better clinical outcomes than men after 2 years of treatment in EIS. 4,5 Given our results and these past reports, some men may need more than 2 years of EIS to achieve good clinical outcomes. This is particularly important for negative symptoms as only one-third of men achieved negative symptom remission after 2 years of treatment (Table 2). Recent evidence has shown that patients receiving EIS care beyond 2 years may continue to experience further reductions in negative symptoms, specifically those related to expressivity (e.g., affect flattening or alogia). 45 Such improvements are likely related to patients continuing to receive psychological interventions in EIS care. 43,44 However, the study indicated that the severity of motivational-based negative symptoms (e.g., anhedonia or avolition) remained stable during the additional years of treatment in EIS. 45 Regardless, transferring men to regular care (i.e., primary care or non-EIS psychiatric clinics) after completing 2 years of EIS may increase their risk of experiencing poorer clinical outcomes given that they still exhibit severe negative symptoms (Table 2), and this may lead them to disengage with treatment 42 in regular care. In a recent RCT in which all patients who completed 2 years of EIS were randomized to receiving a 3-year extension of EIS (EEIS) or 3 years of regular care, patients receiving EEIS remained in treatment longer and engaged in more interventions than those receiving regular care. 46 Furthermore, the EEIS produced longer lengths of positive, negative, and total symptom remission than regular care. 46 As previously reported, 46,47 patients in EEIS are more likely to continue to engage in treatment compared to regular care because the assertive case management model employed by EIS ensures that case managers regularly contact patients (at least twice a month) and actively support them in completing their treatment plans. Thus, the continuation of receiving assertive case management from EEIS may help men to continue to engage in treatment and subsequently yield better clinical outcomes.
While it may be expected that premorbid functioning may mediate the effects of sex on outcomes, our mediation models suggest that premorbid functioning during early adolescence (Suppl. Figures S5 and S9) and not during childhood (Suppl. Figures S2, S7, and S11) may act as a mediator in these associations. Although men may generally exhibit poorer premorbid functioning than women during childhood, 11,39 there is the possibility that some men may experience functional improvements once they reach early adolescence. Indeed, past evidence has shown that some patients display a positive trajectory in which premorbid functioning improves from childhood to early adolescence. 48 However, the poorer premorbid functioning generally found among men during early adolescence 11,39 is likely to be a mediator because their first episode of psychosis and the treatment for it in an EIS typically occur between late adolescence and early adulthood. 33 Given this implication, we removed early adolescent premorbid functioning from our multivariate model examining sex and negative symptom remission after 2 years of treatment and only adjusted for childhood premorbid functioning and age at onset of psychosis. The association remained nonsignificant (adjusted OR, 1.46; 95% CI, 0.82 to 2.60).
Age at onset of psychosis is also thought to mediate the effects of sex on outcomes as the earlier age of onset commonly found among men may lead them to experience poorer psychosocial development and therefore poorer outcomes. However, we did not identify age at onset of psychosis as a mediator in the associations between sex and outcomes (Suppl. Figures S4, S8, and S12). Despite bordering on statistical significance, the sex difference in the age at onset in our study is rather minor, with men developing psychosis nearly 1 year earlier than women (Table 1). Our findings are consistent with a recent meta-analysis demonstrating that men may generally develop psychosis approximately 1 year earlier than women. 10 Thus, age at onset of psychosis may only mediate these associations if men experience a far earlier onset that would substantially impair their psychosocial development.
It is possible that the results seen after 2 years of treatment may be affected by the higher attrition rate among women. To explore this, we compared baseline variables and 1-year outcomes between women who completed only 1 year of treatment with women who completed 2 years of treatment (Suppl. Table S3). There were no significant differences between these 2 groups for any variable. Hence, it is not likely that the higher attrition rate among women affected our results after 2 years of treatment. Women may have had a higher attrition rate because more of them exhibited good functioning than men after 1 year of treatment (Table 2). Hence, some women may have felt that they did not require more help after completing 1 year of treatment. In addition, the higher attrition rate among women may be related to their smaller sample size (31% of study population). Despite these limited data, we examined whether weight gain during the first year of treatment and severity of extrapyramidal symptoms 49 at the end of the first year of treatment may have contributed to the observed sex difference in attrition rates (Suppl. Table S4). We found no significant sex differences in these side effects.
Limitations
Unfortunately, our study does have some limitations. First, we were unable to examine the influence of factors that may vary during treatment (e.g., quantity and frequency of substance abuse). Second, our final study sample is 61% of our study population (Figure 1). This 39% attrition rate is a combination of patients dropping out of treatment and missing data on functional measures. The attrition rate seen in our study is comparable to other cohort studies consisting of patients being treated for 2 years in an EIS for psychosis (e.g., OPUS trial: 33% attrition rate). 5 Furthermore, we conducted a supplementary analysis comparing baseline variables between our final study sample (N = 347) and those that were not apart of it (N = 222) (Suppl. Table S5). The final study sample reported only a significantly shorter length of DUP than those who were not part of it. Third, we did not examine rates of antipsychotic-induced amenorrhea as this may have contributed to the higher attrition rate seen among women. Furthermore, it may have also affected our results after 2 years of treatment given that women developing amenorrhea would lose the beneficial effects that estrogen has in psychotic disorders. 50 Although all patients were treated with a low-dose second-generation antipsychotic and side effects were carefully monitored, if serious side effects had arisen (e.g., amenorrhea), medications would have been changed immediately. Regardless, future research examining sex differences in longitudinal outcomes in psychotic disorders should measure rates of antipsychotic-induced amenorrhea to examine if it affects attrition and any observed sex difference in outcomes. Last, we were unable to understand the role that gender identification may have had in our study. Gender may exist as a spectrum of different phenotypes (cis-man, cis-woman, trans-man, trans-woman, etc.), and classifying it as simply man or woman may not be valid. Only 1 patient in the study population did not identify as either a man or woman, and we excluded this person from our statistical analyses. Future studies examining the wide spectrum of gender and its role on outcomes in psychotic disorders are needed.
Conclusions
In summary, our findings suggest that it may take men more time than women to achieve good clinical and functional outcomes in EIS for psychosis. Furthermore, our results suggest that sex differences seen in outcomes may be largely driven by the disparity of other risk factors between the 2 sexes. Overall, it is it is hoped that this report will alert clinicians in developing treatment plans that might need to be adjusted for men given that they often present with several risk factors for poor clinical and functional outcomes.
Supplemental Material
Supplemental Material, 854069_Supplementary_Material - Sex Differences in Clinical and Functional Outcomes among Patients Treated in an Early Intervention Service for Psychotic Disorders: An Observational Study
Supplemental Material, 854069_Supplementary_Material for Sex Differences in Clinical and Functional Outcomes among Patients Treated in an Early Intervention Service for Psychotic Disorders: An Observational Study by Manish Dama, Franz Veru, Norbert Schmitz, Jai Shah, Srividya Iyer, Ridha Joober and Ashok Malla in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We thank the participants and their families as well as the PEPP-Montreal research staff.
Data Access
Please contact
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.D. has nothing to disclose. F.V. reports he is supported through a doctoral training award granted by the Fonds de recherche du Québec–Santé. N.S. has nothing to disclose. J.S. has nothing to disclose. S.I. reports she has received salary awards from Fonds de recherche du Québec–Santé and the Canadian Institutes of Health Research, as well as grants from the Canadian Institutes of Health Research. R.J. reports that he sits on the advisory board and speakers bureaus of Pfizer, Janssen Ortho, BMS, Sunovion, Otsuka, Lundbeck, Perdue, and Myelin. He has also received grant funding from them and from Astra Zeneca and HLS. He has also received honoraria from Janssen Canada, Shire, Lundbeck, Otsuka, Pfizer, and Perdue for CME presentations and royalties from a Henry Stewart talk. None of these are related to the study reported here. A.M. reports receiving research funding for an investigator-initiated project, unrelated to the present article, from BMS Canada and honoraria for lectures and consulting activities (e.g., advisory board participation) with Otsuka and Lundbeck, all unrelated to the present article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.