
Abstract
Objective:
This article explores the life and career of Sebastian K. Littmann. He was a foundational figure of the University of Calgary’s Department of Psychiatry in his role as its second chair and, before this, as an influential administrator at Toronto’s Queen Street Mental Health Centre and Clarke Institute during a transitional period in the 1970s-1980s. According to McGill University’s Heinz Lehmann, this transitional period was when the field of psychiatry underwent an identity crisis that threatened to dissolve the discipline and see its functions increasingly filled by counsellors, neurologists, and primary physicians. Littmann’s professional background and training in Edinburgh was followed by periods of community work in New York, which—by the time he immigrated to Canada—predisposed him to favour a humane and community-based approach to psychiatric work; this approach encompassed the cultural variations that were increasingly characterizing North America’s urban social landscape. His compassionate and progressive approach to treatment was remarkable in light of his troubled and deprived upbringing in Nazi-era Germany.
Conclusions:
The present sketch of Littmann’s personal and professional biography serves to highlight the ways that major historical events and large-scale migration movements, which affected Central Europe, impacted the development of Canadian psychiatry and, by extension, individual Canadians in the twentieth century.
Introduction
It has been over 3 decades since Sebastian “Seb” Klaus Littmann (1931–1986) passed away, and the intervening span of an entire generation provides a fitting standpoint from which to reflect on his fascinating life and contributions to the field of psychiatry in a North American context.
During a period of youthful aimlessness in the ruins of postwar-Germany, his future trajectory first became tangentially linked with Canada owing to a chance meeting with John W. Thompson (1906-1965), a Canadian psychiatrist who was providing expertise in the Nuremburg Trials and taking part in projects by The United Nations Educational, Scientific and Cultural Organization (UNESCO) that sought to re-educate Germany’s shattered society after the war. 1 It was this encounter that would bring Littmann first to the United States and ultimately to his new homeland where he became an advocate of change and a promoter of community and family approaches to treatment within the Canadian psychiatric system. His work with patients represented a type of philanthropy in the original sense of the term and Sebastian Littmann had a colourfully diverse but unfortunately brief career; cut short by illness during his first term (1982-1986) as chairman of the University of Calgary’s newly established Department of Psychiatry. 2 This article intends to provide a summary of Littmann’s journey from a European to North American setting, beginning with a brief overview of his traumatic early experiences during his adolescence, his transition to academic training and clinical practice, his immigration to Canada, and finally his substantial influence on the University of Calgary’s Department of Psychiatry in its early years.
The mass immigration of psychiatrists and neurologists to North America and Britain from Central Europe as a consequence of Nazi policies and World War II is well documented, often being viewed as the definitive example of a “brain drain” process. 3 The authors here have taken part in publications or research projects investigating this large-scale migration of scientific researchers from German-speaking countries to North American settings, as well as the lasting consequences. 4 What we encounter is an extraordinarily complex historical phenomenon in which the individual experience of the émigrés could vary considerably, even though all were exiled or impelled in one sense or another to leave their homeland. There are figures who had already established careers in neurology and psychiatry in their homeland that were more or less violently ejected from Germany or Austria after the rise of National Socialism; one example is Kurt Goldstein (1878-1965). 5 Similarly traumatic was the forced exile of William G. Niederland (1904–1993) following implementation of the anti-Semitic “Law for the Re-establishment for a Professional Civil Service” on April 7, 1933; he later resettled in the USA, where he contributed significantly to the current understanding of post-traumatic stress disorder. 6 Some managed to persist in their positions before emigrating; Karl T. Neubuerger (1890-1972), a German-born neuropathologist, was released from his role as a scientific member of the Kaiser Wilhelm Society (KWG) and adjunct professor of pathology at the University of Munich during the Nazi Era. He fled to the USA in 1938 where he flourished, assisting in the creation of the American Association of Neuropathologists. 7 There were those like Franz J. Kallmann (1897-1965) who, despite being marginalized in their academic and laboratory roles on the basis of their Jewish background, lobbied incessantly to remain in the German research framework of their homeland before ultimately uprooting to North American settings. 8 At the tail end of this migration phenomenon, we come across individuals like Gerald M. Edelman (1929-2014), whose families made the decision to leave Europe during their school years or preliminary professional training so that their talents ultimately developed in North American research settings. 9 Littman’s emigration, while not forced by a malign state’s hostility toward him because of his political affiliations or ethnic background, can also be seen in the wake of this wider brain-drain trend. Talented clinicians continued to be drawn from a troubled Central Europe to the perceived peace and stability of British and North American societies, 10 contributing their expertise and novel perspectives to emerging or established research programs and departments.
Early Life
Dr. Littmann (see Figure 1) was not afforded the most advantageous start in life. Born as Klaus Littmann in Stettin, Pomerania (modern day Szczecin, Poland) during the last years of the volatile Weimar Republic, his childhood was shaped by the National Socialist era, which began only 2 years after his birth. At the age of 10, his sister died of a violent illness, and soon afterward, his father perished as a casualty of the German Wehrmacht’s invasion of the Soviet Union; his own remaining nuclear family members suffered mental health problems subsequently. 11 Due to his demonstrations of intelligence and maturity among his class peers, Klaus was inducted into a prestigious boarding school (“Nationalsozialistische Politische Erziehungsanstalt” – NaPolA) in Putbus, Island of Ruegen, at the age of 11. The school was based on the traditional model of Prussian cadet schools to train future officers, but he felt he was incompatible with the ideology and military drill that was typical of such institutions. In the economic difficulties of post-war Germany, following its surrender, he drifted into something of an itinerant lifestyle, dreaming of becoming a musician, frequently staying with relatives on a temporary basis, and even experiencing a period of homelessness in a street gang with other orphaned or abandoned children. 1,11
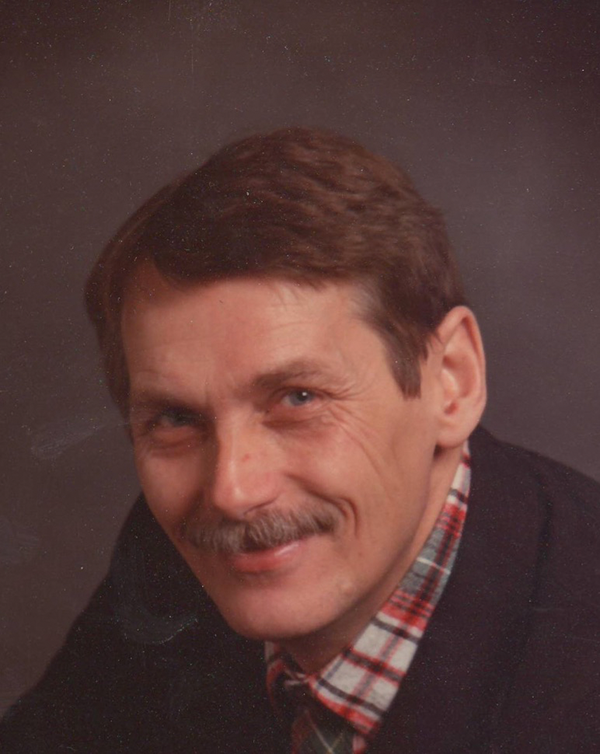
Portrait photograph of Dr. Sebastian Littmann (ca. 1975) - Courtesy of the Littmann Family, Calgary, Alberta, Canada.
It was at this point in a life seemingly bereft of opportunities that Klaus Littmann was to experience a remarkable turn of events. Dr. John W. Thompson (1906-1965), an influential Canadian psychiatrist and neurophysiologist based at the University of Edinburgh, had participated in a UNESCO mission to re-educate and rehabilitate German children in the immediate post-war years. This prolonged appointment led the established psychiatrist and the young drifter to cross paths and begin a continued conversation and exchange. Upon becoming acquainted with Littmann’s mother, Thompson suggested that he adopt the teenage Klaus and his brother, Wolfgang, to rescue them from the widespread poverty and dangerous life on the streets of post-war Europe and to avoid wasting the potential Thompson felt he showed. 1 After the adoption, Thompson subsequently also inspired Littmann’s religious transition to Catholicism, Klaus choosing “Sebastian”—based on the legend of St. Sebastian’s conversion—as his new baptismal name to symbolize his new start in life. 11
Thompson did not waste any time in seeing Sebastian pursue the same sort of excellent formal education he himself had received. Despite some initial uncertainty about his goals, Littmann gradually began to flourish. In 1950, he was enrolled in the distinguished boarding school École des Roches located in France’s region of Normandy. He passed his baccalaureate—the high school qualification required for progression to university level education in France—in 1952, despite having only a limited grasp of the French language and little formal education previously. 1
With Thompson’s belief that the study of the human mind and behaviour could reveal the motivations behind the atrocities that had been committed in World War II, he encouraged Littmann to dedicate himself to psychology. 11 It was at this point that Littmann relocated to Oxford University in England, a move undoubtedly eased by Thompson’s influence and financial support for his tuition and boarding fees. Here, at Wadham College, he completed his undergraduate degree between 1953 and 1956, receiving an Honours BA in Psychology, Physiology, and Philosophy. Littmann then moved into postgraduate education in medicine. He earned his MB, ChB in 1963 at the University of Edinburgh Medical School and was awarded the prize in Anatomy along with 3 distinctions in Chemistry, Psychiatry, and Social Medicine. He also engaged in a circle of socially and politically engaged artists, writers, and curators, including Richard Domenico, in the Scottish capital. The local psychiatrist and head of the Medical Research Council, G. Morris Carstairs (1916–1991), who was exploring different approaches to possible drug therapies, had a profound influence on Littmann while he was continuing to study at the postgraduate level earning his diploma in Psychological Medicine (i.e., Psychiatry) in 1966. He remained at Edinburgh until 1969, winning the Gaskell Prize of the Royal College of London, the United Kingdom’s highest honour for psychiatric training. 2
During his final years of training, Littmann met Milton Rosenbaum (1910–2003), an eminent clinician and researcher and close associate of the recently deceased John W. Thompson, who had arrived in Edinburgh on sabbatical leave—another fortuitous meeting that influenced his decision to move to North America. After forming a close relationship with Littmann, Rosenbaum invited him to New York where a faculty position in social psychiatry was created for him. The Littmann family resided in New York until 1971 where he practiced out of a small clinic in a strip-mall of a predominantly Puerto Rican neighbourhood; this was all in keeping with the community and family psychiatry movement which was in its ascendancy in several leading New York-based institutions and universities in the 1960s and 1970s. 11
Eventually, the USA’s intensifying involvement in the Vietnam War was so distasteful to Littman that he desired to leave the country, which seemed to be perpetually at war. However, his wife, Marie-Odette Littman, had become fond of living in North America and, as a compromise, Littmann began to look for positions in Canada. 11 It was ultimately on his arrival here that Sebastian Littmann was to apply his unique experiences and characteristic approach to psychiatry (see Figure 2), often in institutions that needed serious reform or novel ideas. 12

Living with schizophrenia (1981). Public Domain.
Community and Family Psychiatry in Toronto
In the early 1900s, Canada, like many other western countries, practiced the concept of “warehousing:” the holding of patients with severe psychiatric illnesses, typically against their will, away from public view. Degradation and abuse were frequent, as the prevailing view of mental illness had regressed from curable to incurable and the eugenics movement had taken hold in Canada in the mid-to-late 19th century. 13 Protests from patients emanated in different forms and were common. Attempts to escape, verbal requests to leave, and assaults on staff were all indicative of the conditions that the patients were experiencing. The Toronto Asylum for the Insane was unfortunately one such “warehouse”. 14
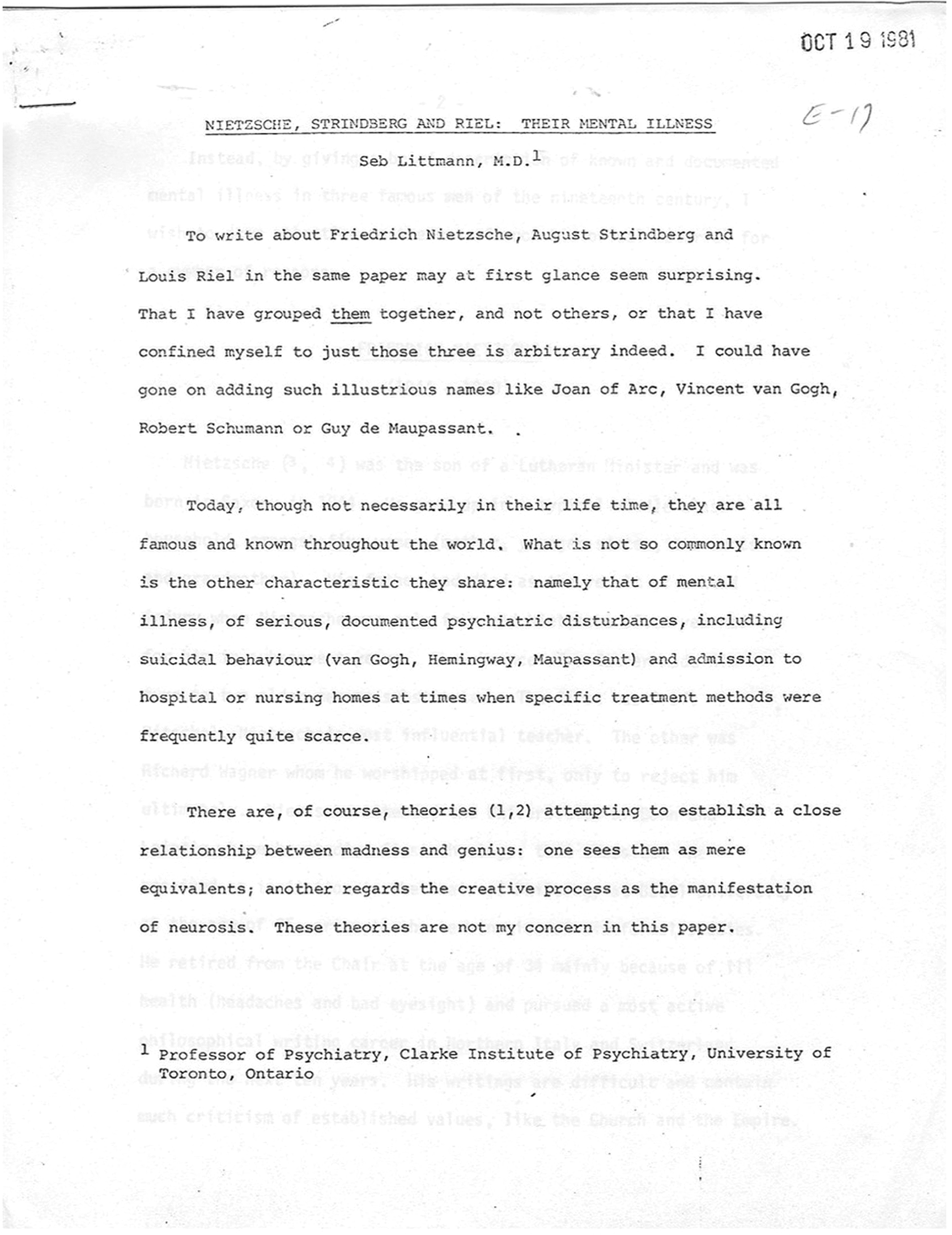
When Littmann arrived in 1972 as Service Chief and Education Director at the recently renamed Queen Street Mental Health Centre (see Figure 4), it seemed that vestiges of an earlier period had persisted. His wife, Marie-Odette, recalls Littmann’s being concerned by the relatively primitive conditions of Queen Street compared with what he had observed in the UK. 11 Patients were routinely locked in rooms and dozens of them shared a single bathroom. 2 The new chief of service was tasked with developing innovative treatment services, a day hospital, as well as outpatient programs, among others. It was during his time in Toronto that Littmann began to provide art therapies to patients. Judging from his teaching slides, which are still kept at the University of Calgary, and from Marie-Odette’s recollections, he became quite interested in historical cases of mental illness.
He also took some inspiration from Philippe Pinel (1745–1826) in the history of psychiatry (see also Figure 3), the French physician whose humanitarian treatment of the mentally ill was a ground-breaking departure from the methods employed by his contemporaries. 8 Littmann encouraged the patients of Queen Street to meet and undertake formal artistic projects with the guidance of a professional art teacher. 11 Indeed, the director at Queen Street is still remembered by former colleagues as a compassionate and attentive clinician, who endeavoured to understand the complete picture behind each patient. 15 For Littmann, a dispassionate list of signs and symptoms of the patients’ illnesses was not enough. He required the individual’s situation be placed in a social and historical context, with the patient’s family dynamics and level of support detailed, for example, as he considered this a crucial factor contributing to successful treatment. 11 It was this focus on family and community support that would characterize Sebastian Littmann’s contributions to psychiatry in Canada and make a lasting impression on his associates.
Nietzsche, Strindberg and Riel: Their Mental Illness (Ms. 1971) - Courtesy of the University of Calgary’s History of Medicine and Health Care Program.
Dr. Littmann in his office at the Clarke Institute, Toronto (ca. 1980) - Courtesy of the Littmann Family, Calgary, Alberta, Canada.
Littmann strongly emphasized the role of family and the wider community in contributing to the psychiatric well-being of the individual. During his time working and living in Toronto, Littmann made annual visits to Sioux Lookout in north-western Ontario, which formed part of a structural program link with the University of Toronto. 15 The indigenous community of Sioux Lookout were psychiatrically neglected, and Littman, with his proclivity for community and humanitarianism, provided the residents with typical psychiatric care but also something out of the ordinary: Littmann facilitated the building of a hockey rink in Sioux Lookout with the intention of providing the community with a positive outlet—a gesture not typically performed by the average clinician. 16 Littmann’s outlook on psychiatric practices, namely, emphasizing the role of the community in matters of mental health, was clearly shaped by his time at Queen Street and was demonstrated by his outreach work with the different ethnic groups within Toronto. In that regard, Littmann was concerned less with the labels and categories offered by the “Diagnostics and Statistical Manual of Mental Disorders” (DSM) and more with the wider context—the community, family, and life experiences—of the patient. Other psychiatrists in Canada, like Charles A. Roberts (1918-1996), a founding member of the Canadian Psychiatric Association and its president in 1965, had already been early proponents of these types of approaches since the 1940s. Nevertheless, Littmann’s approach might seem forward-thinking for its time, more akin to today’s widely expounded biopsychosocial model of mental health. Whereas social and hermeneutic approaches had a high time in the 1930s and 1940s, it was the introduction of shock therapy and the availability of new synthetic anti-psychotic drugs in the 1940s and 1950s that subsequently led to a relative decrease in the social psychiatric approaches in psychiatry, before they resurged with Littmann and others again—almost as a direct reflex to the biological treatment options of the two decades before. 17 Though Littmann undoubtedly improved the conditions at Queen Street, the institution had been tainted by its past association with neglect and abuse. It ultimately disappeared from Toronto’s cityscape in 1976 with its closing and demolition. The destruction of the building seemed to serve as a testament to the need and desire to blot out a dark stain on the history of Canadian psychiatry. 18
In 1975, Sebastian Littmann moved to Toronto’s newly created Clarke Institute of Psychiatry, becoming clinical director of the institution just four years later. It was in this role that Littmann had an increasingly free hand to pursue his favoured psychiatric approaches. The new position involved a great deal of administrative tasks, but this did not entirely diminish Littmann’s characteristic approach. Former colleague, Dr. Badhri Rickhi, recalls that Littmann worked long hours in his management role but that he retained a discernible enthusiasm for interacting and speaking directly with his patients. 19 In line with to his trips to Sioux Lookout, Littmann continued to reflect a concern for the mental wellbeing of minority communities, including also the provision of basic internal medical therapy. It was during his time at the Clarke Institute that Littmann began to seek out groups that were underrepresented in psychiatric care, such as the Chinese and Sikh populations of Toronto, attempting to understand how these largely insular ethnic groups managed their own mental health issues. 8
Chairman of Psychiatry at the University of Calgary
In the 1980s, despite being in the wealthiest province in the country, 12 Calgary was noted as the worst city in Canada for accessing psychiatric services. 19 By the midpoint of the decade, the economic boom that had contributed to Alberta’s wealth started to wane. Strategies were implemented by the federal government to reduce spending in healthcare and education, which in turn resulted in provincial budget cuts and layoffs. Nursing historian Geertje Boschma has detailed the impact this economic decline had on nursing in Alberta during this period. 20 The wider university was reluctant to provide funding for graduate programs, and funding for nursing research required intensive lobbying by its proponents. This is indicative of the prevailing attitude in an era that risked marginalization of necessary health care services, including psychiatry. Though the economic downturn of the 1980s exacerbated the situation, there had already been moves in British Columbia and Alberta since the 1950s toward scaling down large mental health institutions and for the community care of patients. This “deinstitutionalization” process in mental health in the western Canadian provinces resulted in fewer available beds in the psychiatric institutions of Alberta, and the University of Calgary’s affiliated Foothills Hospital was no exception. 2, 21
Keith Pearce (1927–2013), the inaugural head of the Department of Psychiatry, which had been founded only in 1972, had to persuade the administration for additional funding. 22 As health care costs began to spiral, Pearce recognized the necessity to move toward outpatient care, and eventually care in the community. This approach would render the psychiatric unit more akin to a hospital outpatient department. Furthermore, the new form of mental healthcare would reduce the cost of the service to the psychiatric department but was also in keeping with Pearce’s views on the way psychiatry should be conducted. He felt that a patient should be viewed as an individual and that psychosocial factors had to be seen in the general context of the individual’s social and community milieu; a view of the treatment of mental illness 22 that was, of course, wholeheartedly shared by his successor. In addition to that, Calgary’s ongoing resistance to the creation of a separate psychiatric hospital had led to—by necessity—an integration of mental health care with general health care, a situation that would certainly fit with Littmann’s own community approach. This important cornerstone of psychiatry in Calgary has been discussed by the aforementioned Geertje Boschma in her seminal book Faculty of Nursing on the Move (2005), which details the history of specialized nursing at the University of Calgary. In fact, the resistance to create a separate psychiatric hospital was then paired with the creation of a community health-oriented approach that was strongly supported through the community mental health program in the University of Calgary’s Faculty of Nursing. 12 This deliberate approach was also a very important part of the history of psychiatry in the new medical school in Calgary; since the late 1960s, it has boasted an interdisciplinary, non-departmental, and community care-based research set-up. 23
Before his arrival in Calgary, Sebastian Littmann had been looking to increase his ability to influence how psychiatry was being taught and practiced at an institutional level; hence, he was actively seeking a position as head of a psychiatry department. This opportunity came in 1982 with the offer to direct and restructure the University of Calgary’s newly founded Department of Psychiatry. Upon acceptance of the position, however, Littmann inherited the same bureaucratic difficulties with which his predecessor Keith Pearce had continually struggled, which included convincing his medical and surgical colleagues that psychiatry was a discipline worthy of greater institutional support, staffing, and funding. 11 Moreover, there were major transitions in the treatment of psychiatry at the time. The use of pharmaceuticals in psychiatry in the 1970s, when Littmann was accruing a good amount of professional experience with patients, was relatively limited. 14 However, the biological view of psychiatry—that serious mental illness is a brain disease, and that the so-called associated chemical imbalances can be rectified by the administration of a correct dosage of pharmaceuticals—had gradually gathered momentum. By the 1980s, it predominated, not least due to its time efficiency and cost effectiveness. Though psychiatry has often been criticized by the scientific community as myopic, this somewhat reductionist approach to treatment was gaining attraction with practitioners in Littmann’s time and continues to dominate modern-day psychiatry. 12,24
In the mid-1980s, psychiatry in Canada was very much at a crossroads. Not everyone was so willing to adopt the wholesale pharmaceutical approach, though motivations varied. Another German-Canadian émigré psychiatrist Heinz Lehmann (1911-1999) at McGill University lamented that, despite the progress in psychopharmacology having unquestionably and valuably brought about major therapeutic benefits for sufferers of mental illness, the effectiveness of such treatments could make psychiatry obsolete as a specialized discipline. 25 Although drug therapies grew in popularity, Littmann opposed their use to the complete exclusion of other more interpersonal approaches to psychiatric treatment. An example of this is remembered by Dr. Tomm, a former colleague of Littmann. He found that, throughout his career, he often clashed with department heads as he wished to focus on relationship dynamics and family therapy and not merely drug therapies alone. Fortunately, he found Littmann was of a similar outlook regarding a stronger focus on the community dimension, and Tomm’s holistic approach had the enthusiastic support of the chairman during Littmann’s tenure. 11 The Calgary Family Therapy Centre, still in operation today and headed by Tomm, bears witness to the fact that the community and family psychiatry approaches have been actively fostered in the city for an extensive period. As for how Littmann might have viewed the subsequent developments in the field, we can unfortunately only speculate.
In 1986, the same year that Lehmann voiced his concerns over the future of psychiatry as a discipline, Littmann unfortunately passed away from brain cancer before the completion of his first term as chair (see also Figure 5).
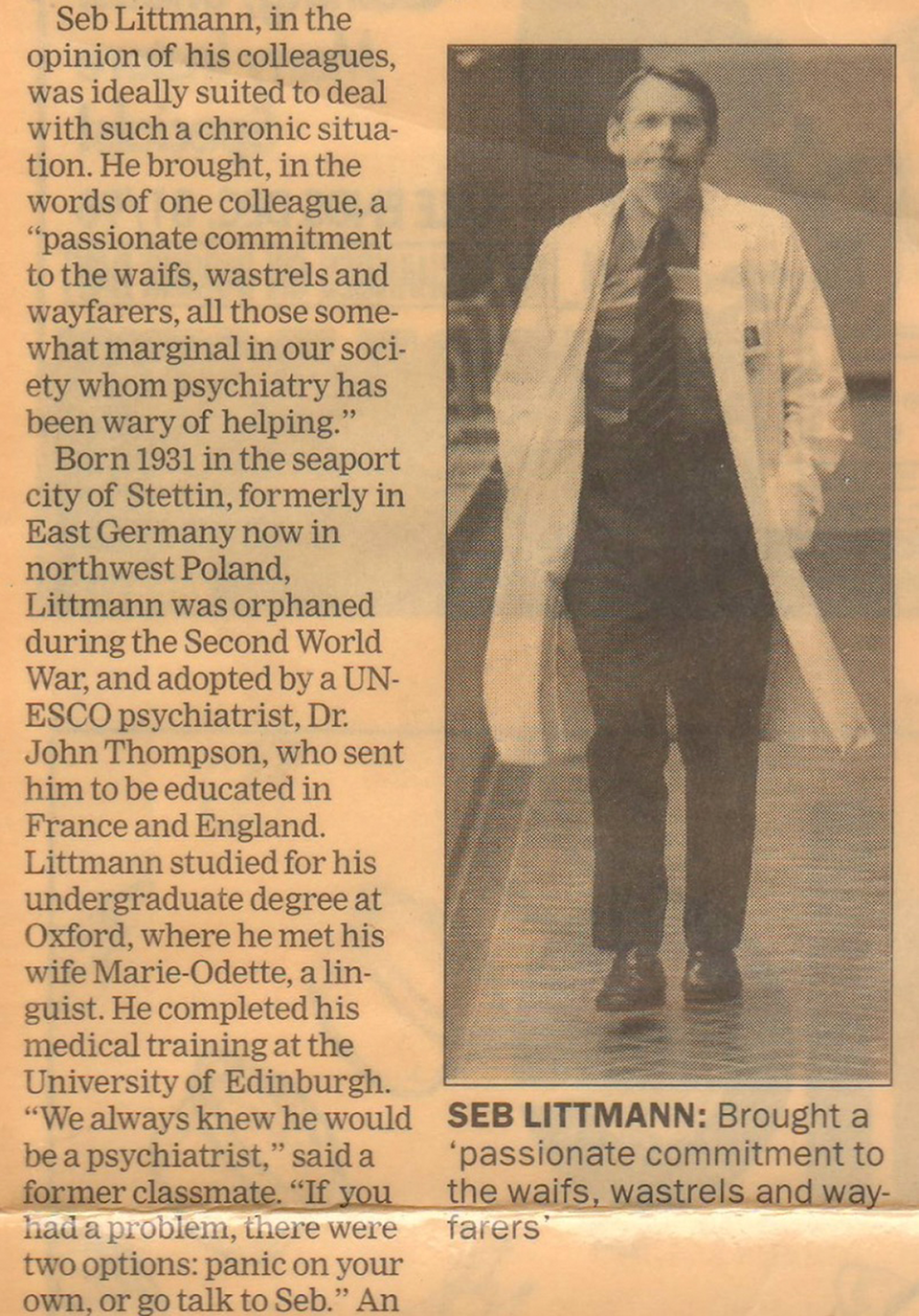
Obituary for Dr. Sebastian K. Littmann in the Calgary Herald (1986) - Courtesy of the Littmann Family, Calgary, Alberta, Canada.
Conclusions
Throughout his career in Canada, Sebastian Littmann’s work with mentally ill patients in both Ontario and Alberta appears to have sometimes gone beyond the typical routines of both a psychiatric practitioner and an administrator. The early death of such an ambitious and energetic physician came as a shock to his colleagues and family. Evidently, the abrupt curtailing of his career surprised Littmann as well: he had been saving a lot of writing on the history of psychiatry for his retirement, including extensive notes and many lecture manuscripts on the history of psychiatry topics from his courses for the Calgary medical students. Though not provided the time to do all he wanted, colleagues remember him fondly, wherever his career took him, as numerous oral history interviews have revealed from this research project. When asked, a long-term colleague John Parboosingh theorized that the adversity Littmann experienced in his early life is likely to have contributed to his humanitarian approach to the treatment of those with psychiatric illnesses during his later career. 11 Psychiatry of course did not lose its relevancy after the mid-1980s and it has come a long way in the generation in between. Littmann, were he here today, might be surprised by its progress. All the same, perhaps its practitioners today would do well to remember his example and those of his colleagues who recommended seeing the individual patient amidst the reductionism paradigm of modern medicine. Certainly, his own story of immigration from the German-speaking milieu to a North American setting, despite relating to prevailing historical trends of his time, is a rather exceptional and thus individual one. That Littmann and his legacy are commemorated annually at the Department of Psychiatry’s Research Day at the University of Calgary is proof that the individual personalities of physicians can create a profound and lasting impression on the community as a whole. 26
Footnotes
Acknowledgements
The authors wish to thank Professor Paul J. Weindling at Oxford Brookes University, England for inspiring this research project, as well as the Littmann family—Sebastian’s wife Marie-Odette and daughter Véronique Littmann—for their helpful information. We acknowledge Littmann’s former colleagues at the University of Calgary, Drs. David Miyauchi, John Parboosingh, Badri Rickhi, Henderikus J. Stam, and Karl Tomm. Members of the Department of Psychiatry are thanked for their support in previous presentations given at the “Sebastian K. Littmann Research Days” in 2014 and 2015 at the Cumming School of Medicine at the University of Calgary. For his kind support with the French-language abstract, we would like to thank Dr. Levente Seláf at Eötvös Loránd University, Budapest. We are grateful for support from the Mackie Family Collection in the History of Neuroscience and the Hotchkiss Brain Institute (all: Calgary, Alberta). We further acknowledge the receipt of information from the Clarke Institute at the University of Toronto, Ontario.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was partially provided for this research by a CIHR research grant (EOG-123690). [An Author Disclosure Form has been filled out and signed by each author.]