
Abstract
Internet-delivered cognitive behaviour therapy (ICBT) has existed for 20 years and there are now several controlled trials for a range of problems. In this paper, we focused on recent meta-analytic reviews of the literature and found moderate to large effects reported for panic disorder, social anxiety disorder, generalized anxiety disorder, posttraumatic stress disorder, and major depression. In total, we reviewed 9 recent meta-analytic reviews out of a total of 618 meta-analytic reviews identified using our search terms. In these selected reviews, 166 studies were included, including overlap in reviews on similar conditions. We also covered a recent review on transdiagnostic treatments and 2 reviews on face-to-face v. internet treatment. The growing number of meta-analytic reviews of studies now suggests that ICBT works and can be as effective as face-to-face therapy.
Introduction
Internet-delivered interventions were developed and initially tested during the mid-1990s, and have subsequently generated a large number of publications, 1 including randomized controlled trials for various conditions; 2 narrative reviews; 3 systematic reviews and meta-analyses; 4 studies on cost-effectiveness; 5 effectiveness in clinical settings; 6 long-term outcomes; 7 implementation; 8 mechanisms of change; 9 negative effects; 10 qualitative studies; 11 aspects of treatment delivery, including the role of therapist factors; 12 therapists’ experiences of conducting therapy online vis-à-vis face-to-face; 13 and patient experiences. 11 The most common form of internet intervention is based on cognitive behaviour therapy, often abbreviated as ICBT.
How is ICBT conducted?
Most forms of ICBT are delivered using a secure platform that resembles online education, with security features resembling online banking. 14 Some systems can be responsive to delivery mode and, for example, adjust the screen when the system is accessed via a smartphone, tablet, or computer. 14 Treatment content is delivered via the platform with support provided from a clinician (mainly via text). There are contemporary programs involving no or minimal therapist support. 15 Previously, these were found to be less effective than therapist-supported interventions, 16 but there are exceptions; for example, in providing support when needed. 17
Various treatment manuals have been either transferred or inspired by previous self-help texts or developed with no previous self-help material. Further, modules in ICBT can be influenced by previous face-to-face work, including manuals, depending on the target condition. The programs also vary in terms of duration. For example, a typical ICBT depression program may have a duration of 8 to 10 weeks. Homework is included in most forms of ICBT 14 and, in many settings, the actual treatment is preceded by a clinical interview over the phone or in person.
Over the years, the conditions for which ICBT has been tested have expanded and there are now programs and controlled studies for many common psychiatric and somatic problems for which regular face-to-face psychological treatment is effective. Finally, therapist-supported ICBT appears to be as effective as face-to-face CBT but there are few direct comparative trials. 18 Recently, the possibility that ICBT can lead to harmful effects has been investigated and, even if uncommon, it is possible, and therefore should be monitored and documented. 10
Aim
The aim of this paper was to conduct a narrative umbrella review of the literature on ICBT for common anxiety and mood disorders in adults. We searched the literature for recent systematic reviews and report the findings as presented in the selected meta-analyses. We also rated the quality of the reviews and conclude with a discussion on future developments of the field.
Literature Search
We searched the literature (MEDLINE, PsycINFO, Scopus, CINAHL, Web of Science, Google Scholar, and contents in established journals in the field; e.g., JMIR, Internet Interventions) for systematic reviews and meta-analyses published between January 2014 and September 2018. Keywords for internet interventions, computerised treatments, online interventions, and web-based treatments were combined with search terms for anxiety and mood disorders (panic disorder, generalized anxiety disorder, social anxiety disorder, specific phobia, posttraumatic stress disorder [PTSD], obsessive compulsive disorder [OCD], major depression) and publications (meta-analysis, systematic review). We excluded reviews on computerised treatments unless meta-analytic statistics were presented for ICBT separately, and excluded blended treatments for which much of the intervention was delivered in person. Citations and reference lists of relevant reviews were also hand-searched (e.g., see Rogers et al. 2017 19 ). Targeted searches were used to identify additional reviews by first author names. When several reviews were available, we used the most recent one, and in cases of uncertainty, we used the one with the highest quality. The review protocol was registered at PROSPERO (CRD42018106156). In total, our search resulted in 9 meta-analyses. A summary of the included reviews is provided in Table 1, including an overall rating of the quality using AMSTAR-2. 20 Instead of giving a score, we followed the recommendation and provided a global rating (e.g., high, moderate, low, critically low). We identified several (N = 618) meta-analyses using different search terms, but excluded duplicates, reviews with a broader scope (e.g., guided self-help and computerised interventions overall) or the wrong scope (e.g., addictions), and reviews that did not focus on the disorders as a separate condition (with the exception of transdiagnostic target groups and face-to-face v. internet interventions). We did not include separate reviews on the treatment of adolescents and children 21 but, instead, focused on adults.
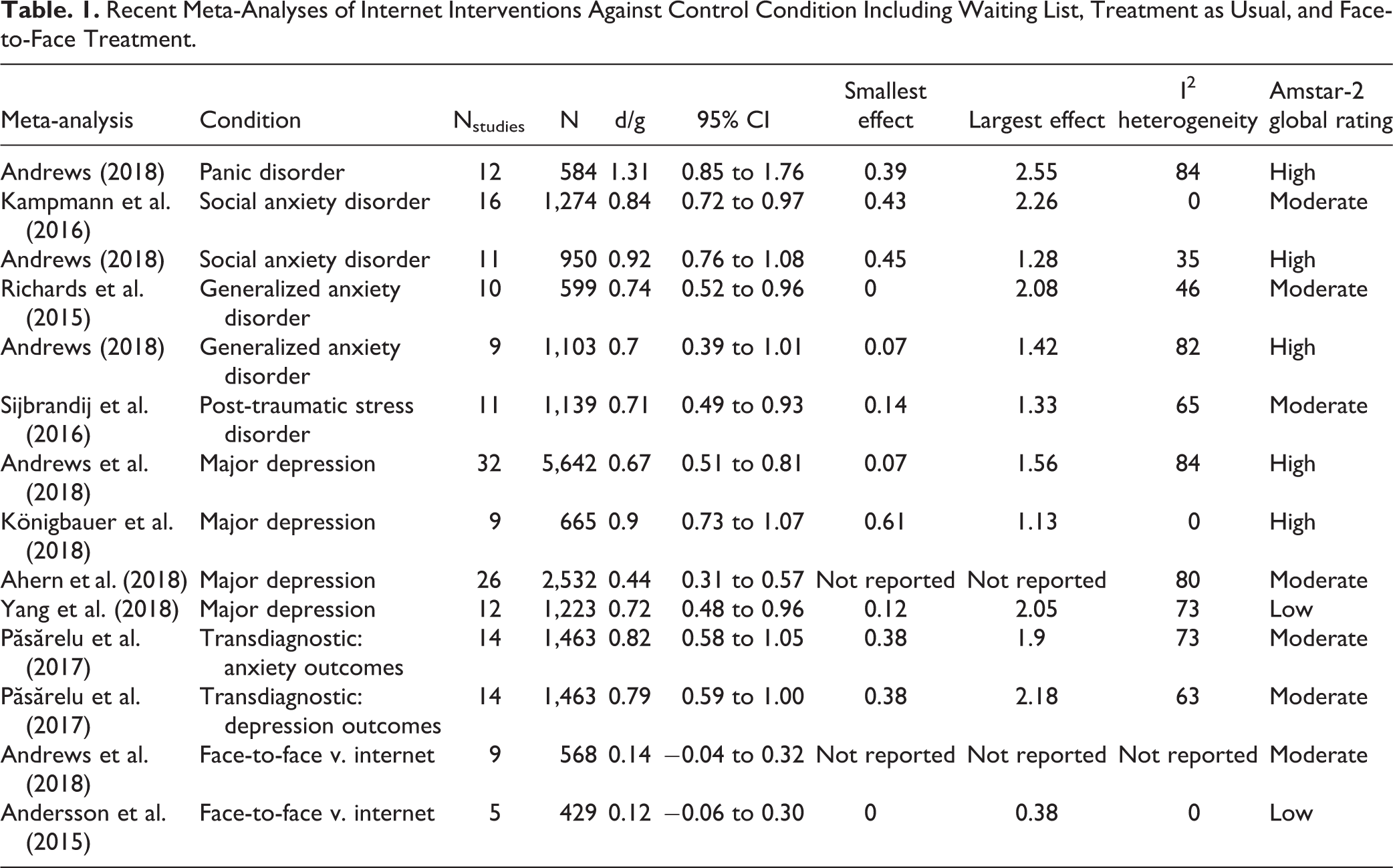
Recent Meta-Analyses of Internet Interventions Against Control Condition Including Waiting List, Treatment as Usual, and Face-to-Face Treatment.
Anxiety Disorders and Obsessive-Compulsive Disorder
Panic Disorder
The latest meta-analyses on panic disorders were by Apolinário-Hagen, 22 Adeleman-Hagen et al. 23 and Andrews et al. 24 A Cochrane review from 2016 was also considered. 25 We selected Andrews et al. 24 as it included the most studies and more than the Cochrane review. Apolinário-Hagen 22 did not present summary statistics clear enough for coding, whereas Adeleman et al. 23 did not present effect size summaries separately for panic disorder. An earlier review also did not include separate summary statistics for panic disorder. 26 The results from the selected review are presented in Table 1.
Social Anxiety Disorder
We focused on 3 recent meta-analytic reviews for social anxiety disorder. Kampmann et al. 27 included separate statistics for ICBT, as did Andrews et al. 24 More studies were included in the earlier review, and we present both in Table 1. Fewer studies were included in previous reviews, for example, the review by Arnberg et al. 28 and the Cochrane review, 25 but overall findings were consistent with the later reviews.
Generalized Anxiety Disorder (GAD)
For GAD, we included 2 reviews, as the previous Cochrane review 25 only included 5 trials, and another review only 4 trials. 28 The most recent review by Andrews et al. 24 included 9 trials and an earlier review by Richards et al. 29 included 11 trials. Richards et al. 29 reported different outcomes with the main outcome for GAD being present in 10 trials. Andrews et al. 24 included a large trial on unguided ICBT that was not included in the review by Richards et al. 29 The latter, however, included non-CBT studies and transdiagnostic target groups; the average effects are strikingly similar (see Table 1).
Specific Phobia
We could not locate any meta-analyses on ICBT for specific phobia: the Cochrane review 25 included 2 trials and Arnberg et al. 28 only one trial. Both trials in the Cochrane review were against live one-session exposure therapy and were included in a meta-analysis on face-to-face v. internet treatment, 30 which we will comment on later.
Posttraumatic Stress Disorder
Reviews on the effects of ICBT for PTSD were also identified. Whereas Arnberg et al. 28 and the Cochrane review 25 included only 2 studies each, we found 2 meta-analyses directly focusing on PTSD and published the same year. A third meta-analysis, also published in the same year, had a broader focus and explored other interventions. 31 Sijbrandij et al. 32 included 12 trials and Kuester et al. 31 included 20 trials. Because Kuester et al. 31 included studies on cancer that did not focus solely on PTSD symptoms, we excluded that review. The results from Sijbrandij et al. 32 are presented in Table 1.
Obsessive-Compulsive Disorder
With regards to ICBT for obsessive-compulsive disorder, we located one review in a conference report 33 and one systematic review on remote treatments including ICBT. 34 But as only 2 controlled trials were included in that review for the between-group contrast against no treatment or attention, we excluded this review. The within-group effect size for 7 trials was g = 1.21 (95% CI, 0.93 to 1.50). Because there are more recent controlled studies, a new meta-analysis should be conducted.
Major depression and symptoms of depression
There are numerous meta-analyses on internet interventions for major depression and symptoms of depression, including individual patient-level meta-analyses. 35 The latter can provide more exact estimates of effects but often suffer from a selection bias, as not all authors respond to data requests. We decided to focus on regular meta-analyses in this report. Some reviews focused on diagnosed major depression, whereas others had a broader focus. There were also separate reviews on, for example, sub-threshold depression, 36 people living in developing countries, 37 cost-effectiveness, 38 behavioural activation, 39 post-partum depressive symptoms, 40 design features, 41 and mobile phone and internet interventions within the same review. 42 Andrews et al. 24 included 32 trials with only 2 focusing on computerised CBT. We decided to include their estimates in Table 1, as the 2 non-ICBT trials were very similar to the rest in terms of effects. We also included the findings of Königbauer et al. 42 in Table 1. This review had fewer trials but a clear focus on diagnosed depression. The effects against waiting-list controls are presented. We included another meta-analysis in which the overall effects of ICBT against control conditions were presented: Ahern et al. 43 included 26 studies, but also reported effects against waiting list controls only (n = 8 trials). This yielded a larger effect (g = 0.79; 95% CI, 0.59 to 1.00). Finally, a fourth meta-analysis was included, which had 12 trials in their analysis 44 (see Table 1).
Transdiagnostic interventions for mixed anxiety and depression
Whereas there are several studies on specific disorders, there are also transdiagnostic and tailored intervention studies that target comorbid anxiety and depression. We selected one recent meta-analytic review. 45 The effects on depression and anxiety outcomes were presented separately, and both are displayed in Table 1.
ICBT versus face-to-face
The contrast between ICBT and face-to-face treatment has been reviewed in some previous meta-analyses. Carlbring et al. 30 included somatic disorders in the review and we thus selected Andrews et al., 24 who reported the contrast as part of their review (heterogeneity and separate effect sizes were not reported). As Andrews et al. 24 included 4 studies on depression and, in an earlier review, 5 studies, we chose to include the earlier review, which focused on depression. 46
Discussion
Research on internet interventions is a fast-growing field that is becoming impossible to cover within one review. 2 In this report, we endorsed an umbrella approach and focused on recent meta-analytic reviews in the field, with a special focus on anxiety and mood disorders in adults. Overall, evidence is now accumulating to suggest that therapist-supported internet interventions, particularly ICBT, can be effective. In this overview, we found meta-analytic support for panic disorder, social anxiety disorder, GAD, PTSD, and major depression, with moderate to large average effect sizes overall. We did not find separate reviews on OCD or specific phobia, which indicates that more research is needed for those conditions, including targeted meta-analyses. We also found support for the notion that transdiagnostic ICBT works and that ICBT can be as effective as face-to-face treatment, even if that is another area in which more work is needed.
This paper did not focus on implementation but, increasingly, internet interventions are being implemented across the world. 8 This is important, as there is a gap between access and need of treatment; for example, in Canada, there is an increased demand for treatment of depression, 47 even if incidence remains stable. Moreover, the role of blending services and using modern information technology as an adjunct to other services is gradually becoming more common. 48 This could be important for the many patients who receive psychological and pharmacological interventions in tandem. To date, the benefits of combining internet interventions and medications have been sparsely investigated, but one exception was a study on OCD, in which d-cycloserine was used in combination with ICBT. 49 Moderators and mediators of outcome is another topic under investigation in this field, including the role of genetics, 50 and brain functioning, 51 in addition to process variables. 52 With an increasing number of studies indicating the effects, it is important to obtain knowledge about what works for whom, but also the mechanisms of change behind intervention effects. Some research has been done on traditional topics, like therapeutic alliance, but it is possible that other mechanisms, more directly linked to the treatment format or skills practice, 53 may be more informative. For example, there is research on knowledge acquisition that shows some promise, 54 but this has not yet been studied as a mechanism of change.
There are several limitations with this review. First, we selected very recent reviews instead of covering all of the available literature on internet interventions. This would have required a stricter focus on overlapping papers within the reviews. Also, we did not calculate separate effect sizes controlling for overlap between reviews. In particular, for the reviews on depression, this could have led to a more precise estimate, as the overlap is less than we expected. Second, the included reviews were heterogeneous in terms of comparison conditions. The most common was waitlist controls or treatment as usual, but there were also other more active comparison groups. However, this is unlikely to have led to an overestimation of effects. With regard to the contrast between IBCT and face-to-face, we only considered the review reporting direct comparisons. Third, we only reported the overall results in the reviews and did not consider occasional moderator analyses. We believe that a more detailed umbrella review, perhaps including not only psychiatric conditions, could shed light on the overall effects of ICBT. This could also include reviews on other target groups, such as students and children/adolescents.
In conclusion, we found clear support for ICBT against no treatment control conditions. Although there are many studies, there are still challenges for the future. There are very few studies on the role of ICBT in more severe psychiatric problems like bipolar disorder and schizophrenia, just to give 2 examples. However, given the need for treatment of anxiety and depression, the implementation of ICBT should be considered.
Footnotes
Acknowledgements
This paper was sponsored in part by Linköping University (Professor contract).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.