
Abstract
Objective:
Opioid self-poisoning is a common suicide method in North America. However, there is limited information about who dies by this method and whether legislation on opioid access has resulted in lower suicide rates by self-poisoning. The primary research question was whether the rate of suicide involving opioids has diminished since the implementation of Ontario’s Narcotics Safety and Awareness Act (NSAA) (1998-2011 vs. 2012-2015).
Methods:
This study examined all suicides by intentional self-poisoning with or without an opioid in Toronto (1998-2015), and tested the mean change after NSAA by one-way ANOVA. Demographic and clinical characteristics as well as details surrounding the suicide were also compared for suicides by opioid and by non-opioid self-poisoning.
Results:
There were 773 suicides in Toronto by self-poisoning where the substance used was known (19.0% of all suicides). Of these, 289 (37.4%) had an opioid present and, in 249 (32.2%) suicides, the opioid was deemed to have been lethal. The mean number of yearly suicides involving opioids was 15.6 before and 17.5 after NSAA implementation (F 1.16, df 1, p = 0.30). Neither the rate per population nor the proportion of suicides by this method has changed between the 2 periods. People who died by suicide using an opioid had higher rates of pain, musculoskeletal, gastrointestinal/liver disorders, and cancer.
Conclusions:
This study confirms that opioids are a major contributor to suicide in Toronto, with no change in the rates after implementation of the NSAA. Physicians who prescribe opioids should monitor patients for elevated suicide risk and intervene where appropriate.
The epidemic of prescription opioid misuse has been described as arguably the most significant current threat to drug safety. 1 Between 2015 and 2016, 1 in 7 Ontarians (14%) filled an opioid prescription. 2 A substantial proportion of opioid misuse involves prescribed opioids 3 and most people who endorse using non-prescription opioids (i.e., heroin) also report previous “nonmedical” use of prescription opioids. 4 Approximately 20% of opioid-related deaths in Ontario occur by suicide. 5 In the US, the involvement of opioids in suicide death has risen over time. 6 Therefore, suicide death by opioid self-poisoning is a significant public health issue and a potentially preventable one, given that most opioids require a physician prescription. However, a focus on restricting access to “high risk” users may not yield the anticipated benefits, since many of those who use opioids for nonmedical purposes appear to obtain them from friends or relatives, most of whom were prescribed the opioid by their own physicians. 7
A major unexplored question in this area is the demographic and clinical profile of those who die by suicide through opioid self-poisoning and how they may differ from people who die by self-poisoning suicide using other substances. Our previous research demonstrates that opioids are frequently identified as the lethal agent in self-poisoning suicides in Toronto; 8 yet, little is known about the characteristics of people who die in this way.
In the US, state prescription drug monitoring programs (PDMPs) were not associated with reductions in opioid deaths. 9 However, in Florida, law enforcement focus on illegal prescriptions at pain clinics as well as policy changes, including placing restrictions on settings in which opioids could be prescribed in addition to a mandatory PDMP were associated with a 27% reduction in opioid-related deaths between 2010 and 2012. 10 In November 2011, the Ontario government implemented the Narcotics Safety and Awareness Act (NSAA), a province-wide strategy for controlling the prescriptions of opioids to “(identify and reduce) the abuse, misuse and diversion of these drugs and (reduce) the risk of addiction and death from the abuse or misuse of these drugs” (Box 1). 11 The NSAA reduced potentially inappropriate opioid prescriptions from 1.6% to 1.0% within the first 18 months; 12 however, the impact of this intervention on suicide is unknown.
Specific regulations under the Narcotics Safety and Awareness Act (NSAA) 10,a
Prescribers must include an identifying number for the patient from government issued identification on a prescription for an NCS. Dispensers must record the name, address, and identifier for people accessing an NCS from a pharmacy. There are certain exemptions allowing prescriptions and dispensing if patients do not have appropriate identification. All opioids are considered monitored drugs in Ontario. The act provides for public notices and disclosures based on data collected.
NCS: Narcotic or Controlled Substance
aNote that prescribers in hospitals and prisons are exempt from the NSAA
This study aims to begin to address these gaps by 1) determining whether rates of suicide by opioid self-poisoning as well as the proportion of suicides by this method have changed over time, and by 2) identifying the characteristics of those who die by suicide using opioids. Evaluating rates over time can inform policy decisions, including whether further legislation may be needed. In addition, characterising the demographic and clinical profiles of those who die by this method may help to inform targeted means for restriction efforts.
Methods
Data Source and Extraction
Records at the Office of the Chief Coroner of Ontario were examined as part of a larger study of all suicides in Toronto (1998-2015). The full details of this cohort have been previously reported. 13 Deaths by intentional self-poisoning were identified and divided into “opioid” or “non-opioid,” depending on whether an opioid was present at the time of death. The “opioid” group was further subdivided into “lethal” and “present but not lethal”. “Lethal” exposure was deemed to have occurred if the coroner’s and pathologist’s investigations determined that the opioid caused or substantially contributed to the person’s death. The presence of specific substances was generally determined through post-mortem toxicology; although, in some instances, the coroner ruled a cause of death based on other evidence, such as an empty pill bottle found next to the deceased.
Specific data extracted from the charts included substance(s) deemed by the pathologist to be responsible for the death, the number and type of substances detected in the toxicology screen, demographic data (age, sex, marital status and living situation), details surrounding the suicide (place of death and presence of a suicide note), whether there was a reported history of major psychiatric disorder (depressive disorders, bipolar disorders, anxiety disorders, psychotic disorders, substance use disorders), past suicide attempts, and the number and type of medical conditions.
Statistical Analyses
The mean number of suicides by opioid and by non-opioid self-poisoning before and after implementation of Ontario’s NSAA were compared using ANOVA. Rates per 100,000 population were calculated using previously published methods that account for population growth over time. 14 Differences between groups in categorical and continuous variables were compared using χ2 and one-way ANOVA tests. This study was approved by the Sunnybrook Health Sciences Centre research ethics board.
Results
Of 4063 suicide deaths in Toronto from 1998 to 2015, 791 (19.5%) occurred by self-poisoning. Our analysis was for 773 of these deaths, as 18 cases had no information available beyond that the death was by self-poisoning. Of these 773 deaths, 289 (37.4%) had an opioid present, of which fewer than 5 were non-prescription opioids (i.e., heroin). In 249 of these 289 cases, the opioid was deemed by the coroner to have been lethal. In 19 (6.6%) cases, an opioid was the only drug detected. In 16 cases (2.1%), toxicology was not conducted, so it could not be determined if an opioid was present.
Suicides by self-poisoning with and without an opioid present by year are shown in Figure 1. The mean number of opioid suicides per year was 16.1, including 15.6 and 17.5 yearly deaths before and after the NSAA was implemented, respectively (F = 1.16, df = 1, p = 0.30). This equates to 7.1% and 7.2% of all suicides occurring with opioids in each epoch, respectively, as well as an average yearly rate of 0.62 and 0.65 opioid suicides per 100,000 population before and after the legislation. The mean number of suicides with opioids present in lethal amounts were 13.1 and 16.3 yearly before and after the legislation, respectively (F = 3.4, df = 1, p = 0.09). There were 26.9 non-opioid suicides per year, including 27.3 and 25.5 yearly deaths before and after the legislation, respectively (F = 0.19, df = 1, p = 0.67). The proportion of suicides by specific opioids was generally similar for both epochs, with 2 notable exceptions: Codeine was present in 18% of opioid suicides before NSAA and 11% after (χ2 = 5.5, df = 1, p=0.02), whereas fentanyl was present in 1% before and 4% after (χ2 = 9.5, df = 1, p = 0.002).
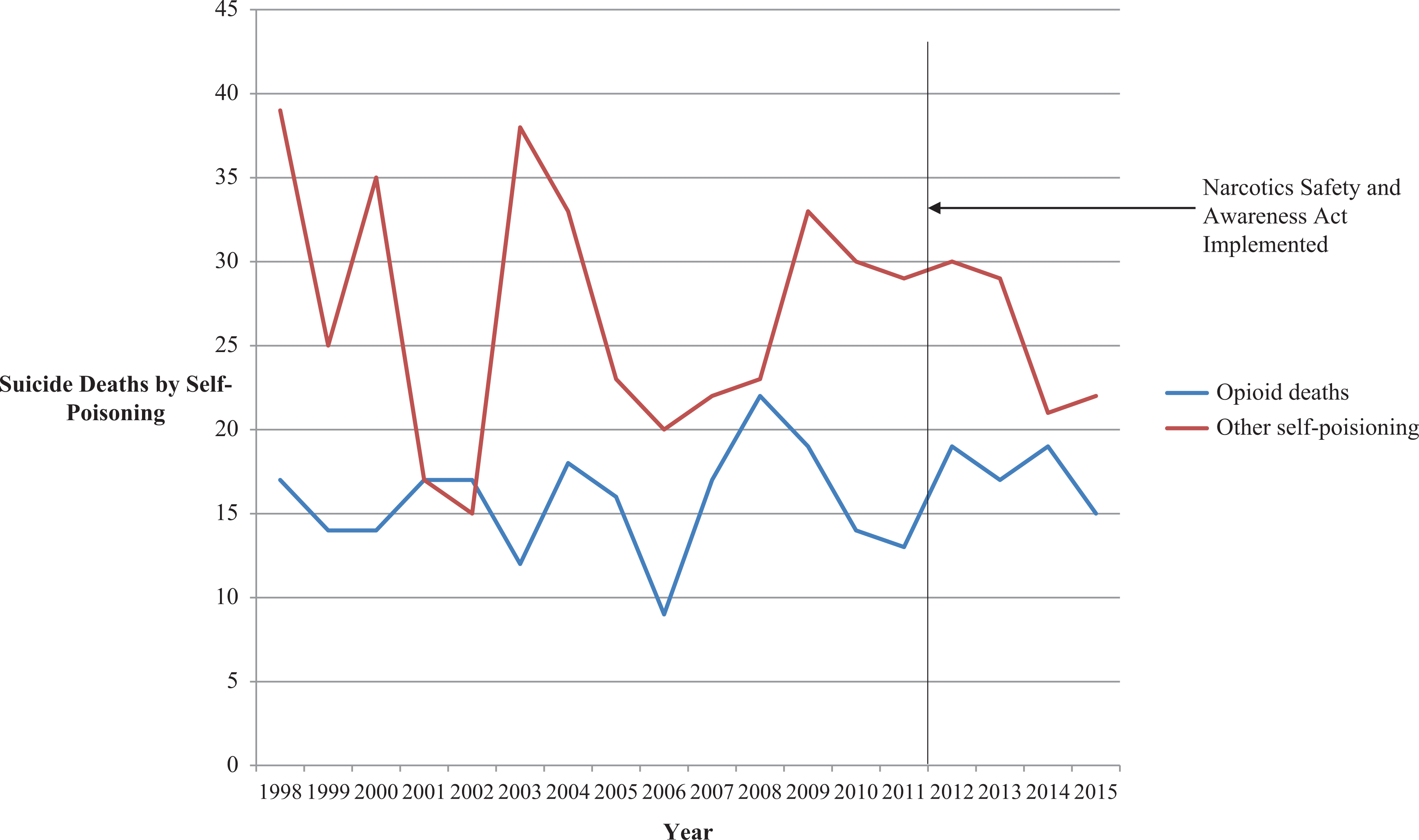
Opioid and non-opioid self-poisoning deaths in Toronto (1998-2015).
The demographic and clinical details identified for people who died by opioid and non-opioid self-poisoning are shown in Table 1. Although there were no significant demographic differences, those who died by opioid self-poisoning were more likely to have a previously diagnosed medical problem (65.1% vs. 49.8%, p < 0.0001) and a history of a substance use disorder (33.9% vs. 29.6%, p = 0.01), and were less likely to have schizophrenia (2.8% vs. 8.7%, p = 0.001). They were also less likely to have a diagnosed mental disorder; although, rates of mental disorders were still high (82.7% vs. 88.2%, p = 0.03). Regarding specific medical disorders, people who died by opioid self-poisoning were more likely to have a pain disorder (29.4% vs. 8.9%, p < 0.001), musculoskeletal disorder (14.9% vs. 6.0%, p < 0.001), gastrointestinal and/or liver condition (10.7 vs. 3.7, p < 0.001), or cancer (8.7% vs. 4.8%, p = 0.03).
Demographic, Clinical and Suicide-Specific Characteristics of People Who Died by Opioid and by Non-Opioid Self-Poisoning in Toronto, 1998-2015.
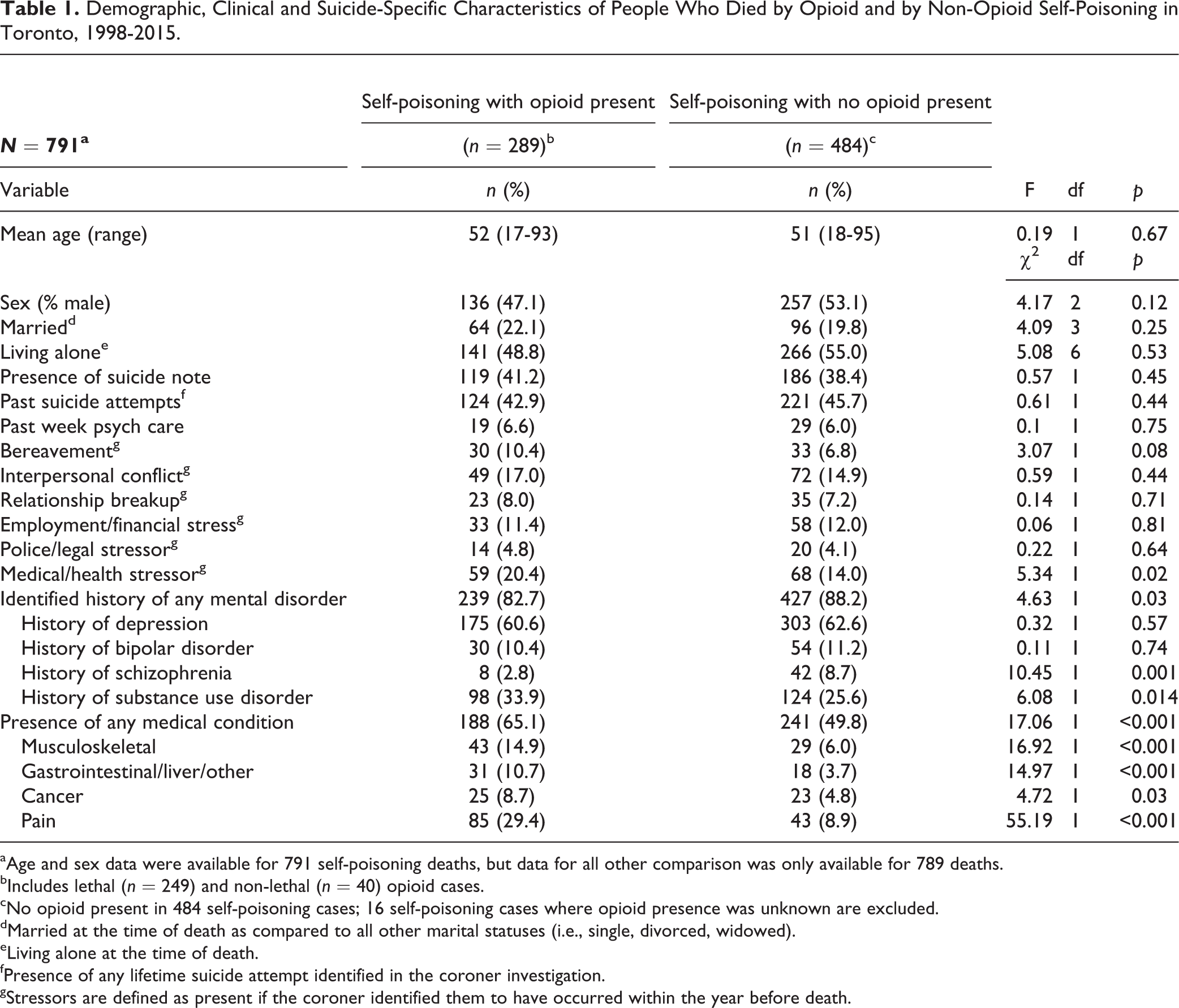
aAge and sex data were available for 791 self-poisoning deaths, but data for all other comparison was only available for 789 deaths.
bIncludes lethal (n = 249) and non-lethal (n = 40) opioid cases.
cNo opioid present in 484 self-poisoning cases; 16 self-poisoning cases where opioid presence was unknown are excluded.
dMarried at the time of death as compared to all other marital statuses (i.e., single, divorced, widowed).
eLiving alone at the time of death.
fPresence of any lifetime suicide attempt identified in the coroner investigation.
gStressors are defined as present if the coroner identified them to have occurred within the year before death.
The sensitivity analyses examining only “lethal” opioid suicides and comparing epochs are presented in the Appendix.
Discussion
This study confirms that opioids account for a large proportion of self-poisoning suicides in Toronto. Notably, the number, rate, and proportion of suicides by opioids have been stable over time, with no changes associated with the implementation of the NSAA. The characteristics of those who die by suicide using opioids are largely what would be expected; that is, a higher preponderance of people who have substance use disorders and who are medically unwell. Regarding the latter, there are higher rates of people suffering from specific medical conditions that might result in opioid treatment. These results suggest the potential need for changes to public policy and health systems that are more broadly aimed at the safe prescribing in these specific groups and across the entire population.
Pain disorders and serious health conditions, such as cancer, are both risk factors for suicide 6 as well as potential indications for opioid prescriptions, 15 and this confluence provides a rationale for increased suicide surveillance in people with these disorders. 16 Furthermore, restricting access to lethal means is an evidence-based intervention for suicide prevention. 17 Opioids may be particularly amenable to such an approach, since physicians, in large part, control access to them, with the caveat that such efforts would need to be monitored to avoid a negative impact and to encourage the appropriate use of opioid prescriptions in select patients to maintain adequate pain control. The implications for those with substance use disorders would also need to be carefully considered, as restricting access to physician-monitored opioid treatment could lead some to seek opioids through unregulated sources, which carries its own risks. The impact of the NSAA on rates of opioid misuse are currently unknown; however, the findings here suggest that, even an intervention that led to nearly 40% fewer inappropriate opioid prescriptions (1.0% vs. 1.6%) 12 might have been too narrowly targeted, and that broader restriction efforts may be necessary to reduce suicides involving opioids. Potent opioids, such as fentanyl, could be a specific target of interest.
This study has several important limitations. The most important is that many factors may have influenced suicide rates before and after implementation of the NSAA. This study cannot rule out that the NSAA had an impact that is obscured by countervailing forces; for example, an increased prevalence of opioid use disorders or medical conditions. This study did not include a living control group, meaning that we cannot draw conclusions about the relationship between opioid use/prescriptions at a population level and death. Although toxicology was not available in all cases, it was completed for most self-poisoning suicides. Suicide deaths by opioids may also be more likely to be misclassified as an accident, in part because it may be difficult for coroners or medical examiners to determine the deceased’s intent with certainty. 16,18 Given these last 2 limitations, counts and rates presented here should be considered as underestimates. Finally, there is no reason to suspect that a different result would be observed in another Ontario/Canadian city; although, the degree of generalisability to rural communities is uncertain.
The limitations notwithstanding, the results of this study are straightforward. Opioids account for a substantial proportion of suicide deaths by self-poisoning. People who may have access to opioids either for medical conditions or due to substance use disorders are particularly at risk. Finally, the current efforts to better manage access to these medications are not achieving their desired effect from the perspective of suicide prevention and may need to be more broadly focused. These findings have key public health implications given that opioids can be controlled by prescribing physicians who can also monitor opioid-treated patients for elevated suicide risk ideation and intervene where appropriate.
Footnotes
Appendix A – Summary of Sensitivity Analysis Results
A sensitivity analysis examining demographic, clinical, and suicide-specific differences, based on cases of only “lethal” opioid deaths, yielded no differences in any significant findings. A sensitivity analysis examining demographic, clinical, and suicide-specific differences, based on epoch (1998-2011 and 2012-2015), did identify some different results, which are summarised below.
There were no significant differences in the results for mean age, sex, % married, % living alone, presence of suicide note, past suicide attempts, past week psychiatric care, bereavement, interpersonal conflict, relationship breakup, employment/financial stressor, police/legal stressor, history of depression, or history of bipolar disorder before (1998-2011) or after (2012-2015) implementation of the NSAA.
Fewer opioid decedents had identified mental disorders compared with non-opioid decedents after implementation of the NSAA (74.3% vs. 89.2%; χ2 = 6.60, df = 1, p = 0.01) but not before (85.4 vs. 88.0%; χ2 = 0.81, df = 1; p = 0.37). Fewer had schizophrenia before (1.8% vs. 8.9%; χ2 = 11.8, df = 1, p = 0.001) than after (5.7% vs. 7.8%; χ2 = 11.8, df = 1, p = 0.001). It is uncertain whether this change reflects a true increase in use by people with mental disorders and/or schizophrenia or, rather, possible ascertainment bias. Further research would be required to investigate this finding.
There was a trend toward more opioid decedents with an identified history of substance use disorder compared with non-opioid decedents both before (32.9% vs. 25.9%; χ2 = 3.31, df = 1; p = 0.07) and after (37.1% vs. 24.5%; χ2 = 3.18, df = 1; p = 0.08) the NSAA; although, neither met the threshold for significance. The trend is similar between epochs and only rises to statistical significance with the increased power of the combined sample.
More opioid decedents had an identified history of a medical condition compared with non-opioid decedents before the NSAA (62.6% vs. 46.3%; χ2 = 14.7, df = 1; p < 0.001), with a non-significant trend in that direction after the NSAA (72.9% vs. 62.7%; χ2 = 1.92, df = 1; p = 0.17). Similarly, more opioid decedents had a recent medical stressor compared with non-opioid decedents before the NSAA (21.9% vs. 12.3%; χ2 = 9.67, df = 1; p = 0.02), with no significant difference after its implementation (15.7% vs. 20.6%; χ2 = 0.65, df = 1; p = 0.42). As with the finding for mental disorders/schizophrenia above, it is possible that rising rates of detected medical disorders in suicide decedents over time reflect improved detection by the coroner rather than a true increase.
This finding is also reflected in data from specific medical disorders, where more opioid decedents had pain disorders (29.2% vs. 8.9%; χ2 = 42.1, df = 1; p < 0.001), cancer (9.1% vs. 4.5%; χ2 = 5.28, df = 1; p = 0.02), musculoskeletal disorders (14.6% vs. 5.8%; χ2 = 13.3, df = 1; p < 0.001) and gastrointestinal or hepatic disorders (9.6% vs. 1.6%; χ2 = 20.9, df = 1; p < 0.001) before the NSAA. After implementation of the NSAA, only pain remained significant (30.0% vs. 8.8%; χ2 = 12.9, df = 1; p < 0.001), whereas there were only numeric, non-significant differences for cancer (7.1% vs. 5.9%; χ2 = 0.11, df = 1; p = 0.74), musculoskeletal disorders (15.7% vs. 6.9%; χ2 3.47, df, 1; p = 0.06) and gastrointestinal or hepatic disorders (14.3% vs. 11.8%; χ2 = 0.23, df = 1; p = 0.63). These findings must be interpreted with caution, as the epoch after the NSAA includes fewer years/deaths and therefore has less statistical power to detect differences. It is notable that the directionality of numerical differences was maintained in each case.
Acknowledgments
We thank the entire staff at the Office of the Chief Coroner of Ontario, including Andrew Stephen, for making this research possible. Data access statement: The investigators do not have permission to share the data used in this study as it is the property of the Office of the Chief Coroner of Ontario and keeping it confidential is a requirement of the research ethics approval.
Author Contributions
Conception and design of the study: MS, MW, SG, AS; acquisition of study data: MW; analysis and interpretation of study data: MS, MW, SG, AS; wrote first draft of the paper: MS, SM, SG; critiqued the output for important intellectual content: AS
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Sunnybrook Health Sciences Centre research ethics board (ID# 199-2012).
Financial Disclosure
All authors report no financial relationships with commercial interests of relevance to this study. MS has received grant support from the American Foundation for Suicide Prevention, the Ontario Ministry of Research and Innovation, the Innovation Fund of the Alternative Funding Plan from the Academic Health Sciences Centres of Ontario, the University of Toronto Department of Psychiatry Excellence Fund and the Dr Brenda Smith Bipolar Fund.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by an Academic Scholars Award from the Department of Psychiatry, University of Toronto.