
Abstract
Objective:
No universal definition for treatment-resistant depression (TRD) exists. This lack of consensus reduces the generalizability of study findings and limits the ability to study TRD. In addition, anecdotally, there may be a difference between the definitions of TRD within research and those applied in practice. Thus, the objective of this work was to identify current common definitions of TRD used in both research and clinical practice.
Method:
A systematic review of published literature was conducted to document TRD definitions. Extracted data were grouped based on patient cohort and method of defining TRD. Validation studies were narratively summarized. Interviews with 6 key informants were conducted to understand how definitions are applied in practice.
Results:
In total, 155 definitions for TRD were identified in the published literature, and 48.4% of all definitions specified requirement of at least 2 treatment failures. Key informant interviews indicated the concept of TRD is rarely employed in clinical practice. Instead, concepts like “complex needs,” “struggling with their disease,” and “chronic” are used. When asked directly about how they would define TRD, interview participants said an adequate trial of psychotherapy as well as an adequate trial of at least 2 to 3 antidepressant medications.
Conclusions:
There is no universally accepted definition of TRD, and substantial heterogeneity exists. This study indicates discordance between the use of the term in research and clinical practice, with several key informants emphasizing that the terminology is rarely used in their clinical experience. Development of a shared, common definition across practice and research is required.
Background
Mood disorders, including major depressive disorder (MDD) and bipolar disorder (BD), are among the most common mental disorders in Canada. 1 In a Canadian mental health survey administered in 2012, approximately 13% of the population met the criteria for a mood disorder in their lifetime, with 11.3% of the population experiencing a major depressive episode and 2.6% experiencing BD. 2 Both MDD and BD have significant occupational, medical services, and suicide-related costs. 3,4
In both MDD and BD, a substantial proportion of patients may not respond satisfactorily to first-line antidepressant therapy, commonly termed treatment resistance. 5 Defining treatment-resistant depression (TRD) can be complex, in both MDD and BD, due to the lack of a universally accepted definition. A systematic review from 2012 identified 5 main staging models that are commonly used: the Antidepressant Treatment History Form (ATHF), the Thase and Rush Staging Model (TRSM), the European Staging Model (ESM), the Massachusetts General Hospital Staging Model (MGH), and the Maudsley Staging Model (MSM). 6 However, a 2014 review defines and measures TRD in “medication failure models,” which establish the specific number and/or type of treatment failures required to classify patients as having, or not having, TRD. 7 In addition, a recent narrative review found that no consensus exists on the definition of TRD. 8
As a result, substantial variability may exist in that the practical definitions currently being used result from the lack of consensus on the details of adequate dosage, duration, and specificity. This may, in turn, reduce the generalizability of TRD study findings and limit the ability to study TRD. The objective of this work was to identify current common definitions of TRD used in both research and clinical practice. Furthermore, we sought to understand if there is a difference and, if so, what the difference is between the definitions used in research compared to practice. This work could lead to identification of a common definition within research and practice that could be useful to standardize study populations, cohort selection, and algorithms that could be used in, for example, administrative data to identify patients with TRD.
Methods
Two distinct methods were used to triangulate to a common definition. First, a systematic review of the literature was completed to document the definitions used in research contexts. Second, key informant interviews were completed to understand how definitions were being used in clinical practice. Findings from both methods were synthesized to inform the broader question of appropriate shared common definition across research and practice.
Systematic Review
Search strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRIMSA) guidelines were followed. 9 The PRISMA checklist is available in Supplemental File I. MEDLINE, EMBASE, PsycINFO, the Cochrane CENTRAL Registry of Controlled Trials, and the Cochrane Database of Systematic Reviews were searched from inception until December 6, 2017. Results were limited to English- and French-language studies. The search strategy focused on identifying studies that validated or provided definitions for TRD. Terms such as depressive disorder, treatment resistance, and treatment resistant depression were combined using the Boolean operator or. Full search strategy is provided in Supplemental File II.
Inclusion and exclusion criteria
All abstracts retrieved were screened in duplicate (S.B. and S.C.). Articles proceeded to full-text review if the study defined TRD, was not a single case study design, used TRD patients as their primary study cohort, or assessed the validity of a TRD definition. Abstracts selected for inclusion by either reviewer proceeded to full-text review. This initial screen was intentionally broad to ensure that all relevant literature was captured. At full-text review, the same inclusion criteria were applied. Additional exclusion criteria were as follows: if the study did not report original data, full-text was not available, or the study was not available in English or French. Last, only studies published on or after January 1, 2016, were included. This criterion was identified as the volume of literature was sufficient within the past 2 years and it also ensured the current definition was captured.
Study selection and data extraction
Data from the included studies were extracted in duplicate (S.B. and S.C.). Detailed information on the definition of TRD, study design details, and factors that contributed to misclassification of TRD was extracted. Discrepancies between reviewers during full-text review and data extraction were resolved through consensus.
Data analysis
Extracted data were grouped based on patient cohort and TRD definition used. Four main patient cohorts were identified: unipolar depression, bipolar depression, mixed unipolar and bipolar depression, and MDD patients. Two main methods of defining TRD were identified: use of staging models and use of a minimum number of treatment failures. Studies were further differentiated based on reported specifications for treatment failures.
Key Informant Interviews
Interviews with 6 key informants were conducted via phone following ethics approval from the Conjoint Health Research Ethics Board of the University of Calgary (REB18-0002). A snowball sampling strategy was used to identify health care providers until saturation was reached. An initial key informant was identified and asked to recommend others who may have experience with TRD in their practice. All participants were asked to describe their professional role, experience with patients experiencing depression symptoms, the most common definition of TRD within their practice, their working definition of TRD based on clinical experience, and their experience with TRD misclassification. All interviews were closed with an open-ended question asking if interviewees had anything else they would like to share. All interviews were audiotaped with the informed consent of the participants, and detailed notes were taken. Interview data were analyzed with the goal of identifying key themes emerging in response to the interview questions.
Results
Of the 4581 unique abstracts identified, 224 proceeded to full-text review (Figure 1). At full-text review, 72 were excluded (reasons for exclusions: improper study design, n = 14; TRD definition was not provided, n = 31; non-English and non-French publication, n = 2; full text not available, n = 4; not original data, n = 11; primary study cohort not TRD patients, n = 4; duplicate publication, n = 6). The final data set included 152 studies: 2 validation studies of the definition of TRD and 150 studies that employed a definition of TRD to select a patient cohort.

Study inclusion flowchart. TRD, treatment-resistant depression.
TRD Definitions
Study characteristics
Of the 150 publications included in the TRD definition review, 73 (49%) were published in 2016 and 77 (51%) were published in 2017. Detailed study characteristics are in Supplemental File III. The studies were conducted in 27 countries (Figure 2). The United States produced the greatest number of studies (n = 33), followed by Canada (n = 16). Cohort sizes ranged from 3 to 1546 participants, with 82% of studies having 100 participants or less (Figure 2). Three study designs were used: 1) randomized control trials (30%), 2) observational studies (67%), and 3) case series (3%) (Figure 2).
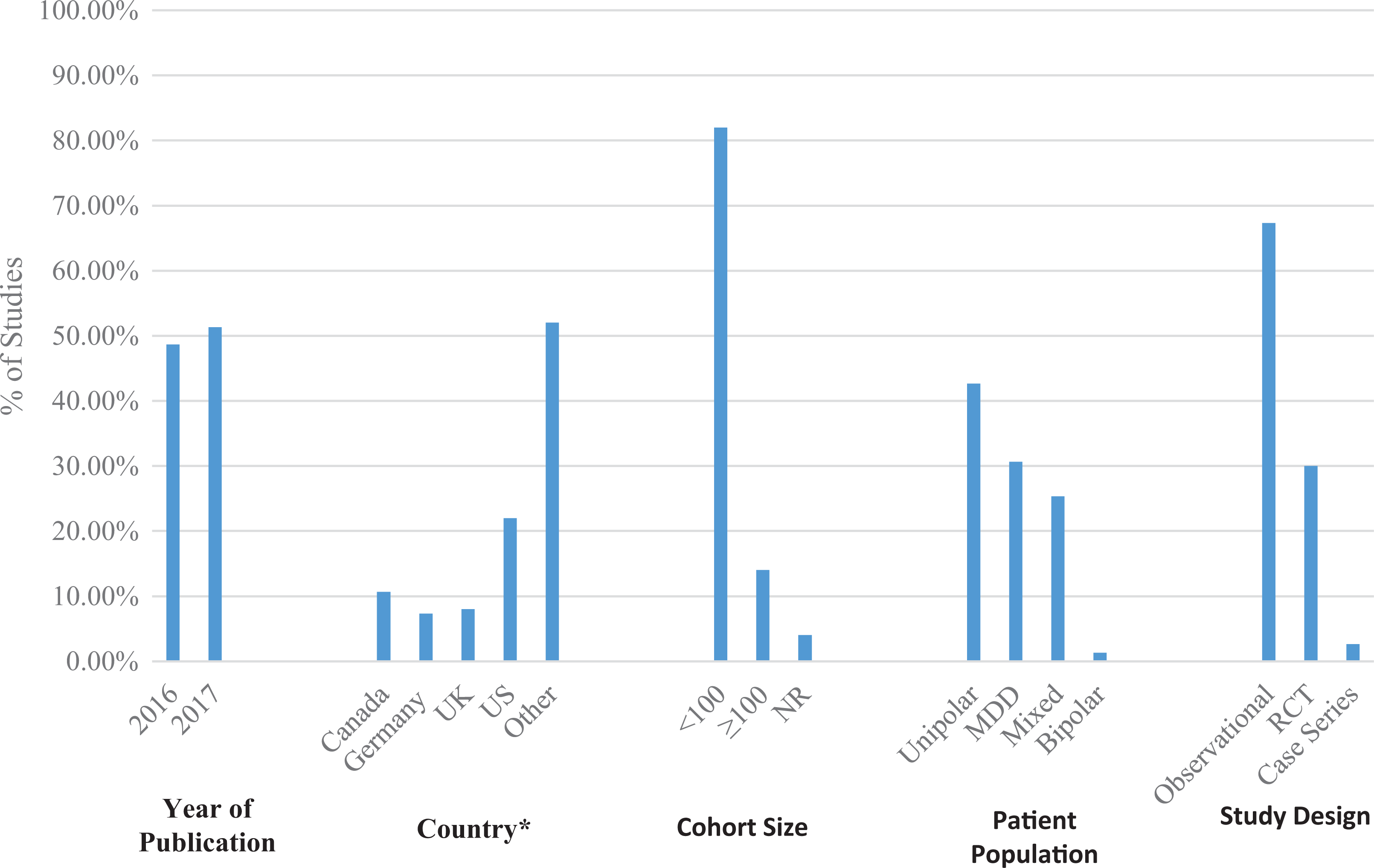
Summary of study characteristics.
Some studies described their MDD population as having unipolar depression while other studies applied the term MDD to include both unipolar and bipolar patients. Thus, studies that described the included patients as “MDD” without further clarification of whether that included unipolar and/or bipolar were grouped separately. Thus, 4 relevant patient populations were identified: 1) treatment-resistant unipolar depressive patients (42.7%), 2) treatment-resistant bipolar depressive patients (1.3%), 3) a mixture of treatment-resistant unipolar and bipolar patients (25.3%), and 4) treatment-resistant MDD patients (30.7%).
Definitions used
The 150 studies included 155 definitions for TRD. Sixty-six definitions were for unipolar patient cohorts exclusively, 36 were for mixed unipolar and bipolar cohorts, 5 were for bipolar patient cohorts exclusively, and 48 were for MDD cohorts. Two main methods for defining TRD were used: the medication or treatment failure method and staging models. The majority of definitions (50.3%) required a minimum of 2 treatment failures (Figure 3). Definitions were further split based on treatment failure details. The level of detail provided varied greatly. Some definitions simply indicated they followed the TRSM or required failure of a single antidepressant treatment. Others included further detail pertaining to the minimum duration, dosage, and class and type of treatments required.

Frequency of treatment-resistant depression definition based on number of treatment failures. *Only displayed countries with 10 or more included publications separately in the figure. MDD, major depressive disorder; NR, not reported; RCT, randomized controlled trial.
Overall, staging models were commonly used to define TRD with 59 definitions (38.1%) referencing them. The TRSM was the most commonly referenced, with 22 definitions using this model (14.2%). Of the definitions that did not reference a staging model in their definition of TRD patient cohorts, the most common definition was 2 treatment failures. Fifty-three (34.2%) of all definitions used this requirement. When combined with the definitions using staging models that required 2 treatment failures (22), this rises to a little less than half (48.4%) of all the definitions using the requirement of 2 failed treatments. However, there was significant variability of specified subcriteria within this group, including differences in the classes of pharmacologic treatments (e.g., 2 different classes, at least 1 mood stabilizer, 2 antidepressants), the length of treatment (e.g., trialled for at least 15 days, at least 4 weeks, at least 6 weeks), and timing (e.g., failure within current episode). Supplemental File IV presents the varied definitions and counts of each variation.
Neuromodulation included treatments such as repeated transcranial magnetic stimulation and electroconvulsive therapy (ECT). Only 17 (11%) definitions specify either type of treatment as qualifying treatment failures. Of these definitions, ECT failure was the most common specification, with 8 definitions listing it as a qualifying treatment failure.
Four of the 5 TRD definitions provided for exclusively BD patient cohorts specified failure of mood stabilizers or atypical antipsychotics. All 5 definitions required at least 2 failed drug trials and 3 specified the type of BD being considered. Thirty-six studies provided TRD definitions that applied to both unipolar and bipolar patients in their cohort. Despite including bipolar patients in their study, just 3 of those definitions included required failure of a mood stabilizer or atypical antipsychotic. Supplemental File V presents the detailed definitions used.
TRD Validation Studies
Two validation studies were identified. 10,11 One study looked at the use of a remote structured interview to validate the diagnoses of MDD and TRD patients who had already been deemed eligible for clinical trials. 10 The interview included use of the “SAFER” tool and the Antidepressant Treatment Response Questionnaire (ATRQ), which are clinical trial tools that aim to provide a quality assurance process for qualitative assessments of MDD and TRD. The other study aimed to develop a new measure, the Dutch Measure for Quantifying TRD (DM-TRD), through refining and adding items to the MSM. 11
Key Informant Interviews
Six key informant interviews were conducted with health professionals based in Calgary, Alberta, comprising psychiatrists and clinical researchers, nurses, and coordinators in a tertiary outpatient program and community-based family physicians with a longstanding interest in mental health. The interviews ranged in length from 30 to 60 minutes. Based on the interview data, 4 thematic headings were established (Figure 4).

Key informant interview themes. TRD, treatment-resistant depression.
TRD in clinical practice
The terms treatment resistant and treatment refractory are not commonly used in clinical practice and are rarely, if ever, used in the primary care setting by family physicians. Health professionals working in a tertiary care outpatient mental health program explained that the term TRD is rarely seen on the referrals coming in from the community, and the term TRD is rarely listed as an inclusion criterion for the tertiary outpatient mood disorders clinic. In cases where a patient has not responded to treatment, primary care physicians will most often describe the events that have led them to feel that they can no longer care for the patient in the community, not labelling this TRD. The more common language includes “recurrent or relapsing depression,” “complex depression,” “difficult to treat,” “multiple episodes of depression,” “chronic depression,” and “struggled with depression throughout their lives.” It’s something that I hear about when I go to lectures, but it’s not something that I actually use mentally in my office.…It’s not a term I find helpful in the office…it’s not like if you suddenly cross the threshold to TRD there’s a whole bunch of new drugs you can throw in, because almost from the beginning you are thinking about the best combination…of medication and counseling…for a patient. —Family physician
Defining TRD
When asked how they would define TRD, even if the term was not something they used in practice, most interview participants said an adequate trial of 2 to 3 antidepressant medications and an adequate trial of psychotherapy. An adequate trial of psychotherapy was specified as consisting of at least a 10- to 12-week course of an evidence-based psychotherapy (i.e., cognitive behavioural therapy, behavioural activation, or interpersonal therapy), provided by a qualified practitioner.
Challenges with defining TRD
Defining TRD was described as a difficult task for 3 reasons. First, the epidemiology of depression is such that the chance of remission diminishes as the duration of depression increases. TRD definitions are usually built around the idea that there should be a certain number of failed medication trials (usually 2 or 3), but this is confounded by time. Second, the definition of TRD is sensitive to the degree of remission required to categorize an episode of depression as treatment resistant. If the expectation is that any residual symptoms are indicative of an inadequate outcome, then the prevalence of TRD will be very high, whereas more modest expectations would result in lower prevalence. Third, the population of people living with depression is a mixture of people living with MDD and those living with depression as a composite of other mental health presentations. This means that the issue of treatment resistance is made more complex with the impact of comorbidities on prognosis. For example, people with personality disorders, anxiety disorders, and chronic pain very often meet definitions for depression, yet they are not going to respond to strategies for TRD unless those comorbidities are also addressed.
Discussion
This work found no common definition of TRD. In fact, this work highlights that the concept itself is not shared across research and practice. The systematic review of published literature found a large volume of literature assessing TRD and a high level of heterogeneity between the definitions used. More than a third (38.1%) of the definitions referred to a staging model with 8 different staging models being employed. The remaining literature used treatment failures to define TRD specifying required minimum treatment failures ranging from 1 to 6. However, our interview work underlined that TRD is not conceptualized within practice. Rather, more patient-focused concepts are used such as “struggled throughout their life” and “complex needs.” In addition, multiple other patient characteristics are considered when thinking about treatment success, including the duration of depressive symptoms, the definition of remission for a particular individual, and the underlying causes of depression itself (e.g., chronic pain, anxiety).
Lack of a common definition for TRD amongst academics and clinicians limits the application of research findings into practice. A commonly adopted definition of TRD in research literature is failure of response to 2 antidepressants from different pharmacological classes. 12 –14 This systematic review is consistent with the requirement of 2 failed antidepressants, with 50.3% (n = 78) of all identified definitions for TRD requiring 2 prior pharmacologic treatment failures. However, the definition of TRD focusing exclusively on pharmacologic treatment failures does not align with current clinical practice, which includes psychotherapy as a fundamental first-line therapeutic option. Interviewees universally included failure of an adequate trial of psychotherapy (10- to 12-week course of an evidence-based psychotherapy provided by a qualified practitioner) as a condition of defining patients as having TRD (although the language used by interviewees was “complex and in need of more help”). Overcoming this disconnect between research definitions and practice will be challenging. In many research settings, existing administrative data sources may be used to identify cohorts of patients. These data are easy of use, provide historical data, have long periods of follow-up, and are readily availability. 15 However, therapies such as psychotherapy are not commonly captured within these data sets, and thus pharmacologic-based definitions will continue to be applied simply due to the data elements included. Work to understand the bias and limitations resulting from selecting patient cohorts due to pharmacologic failure should be undertaken alongside efforts to enhance capture of therapies such as psychotherapy within routine data sets.
Despite the heterogeneity in identified definitions, complexity resulting from the various facets of depression, such as functional impairment, depression subtype, comorbidities, and psychosocial stressors, is not well captured in staging or treatment failure methods. The Dutch model discussed in the second validation study identified 11 shows the benefits of a more detailed diagnosis of treatment resistance in predicting future depressive symptoms and remission. Although these approaches capture more granular detail of each individual’s depressive episode, the range of possible factors involved makes it harder to compare across patients. Inclusion of these more individual-level considerations are echoed within the interviews. A patient-focused approach tailored to the individual’s needs and presentation was noted as a major challenge to a common definition of TRD. To be relevant to practice, a definition that includes duration of symptoms and a functionally focused definition of remission may be required.
Our work reports similar findings to the recently completed narrative review completed by the Agency for Healthcare Research and Quality. 8 While only one focus on the broader report, the Agency for Healthcare Research and Quality reports that among the 18 systematic reviews, 6 nonsystematic reviews, and 13 guidelines reviewed, no consensus definition emerged. Our findings, which result from a systematic review (as opposed to narrative review) focused on primary studies of TRD populations, found the same result. We extend this finding by quantifying the frequency of each definition and providing details of the definitions used stratified by unipolar and bipolar depression.
Limitations
The search strategy was limited to keywords associated with TRD; terms that appear to indicate overlapping constructs of treatment resistance were excluded based on these criteria. This may have excluded some relevant studies. However, it is unlikely that these missed studies would have changed our findings; these studies would only further highlight the heterogeneity of definitions. In addition, this review is limited to studies published from January 1, 2016. While this captures the most recent literature and employment of TRD definitions, it precludes review of earlier studies, which does not allow us to comment on the change in definition over time. Furthermore, key informant interviews were all conducted within 1 provincial health care system, potentially limiting the generalizability of the qualitative findings.
Conclusions
There is no universal agreement on TRD definition. There is a disconnect between the concept and definition across research and practice. The concept of TRD is not described in practice or defined with a simple count of pharmacologic failures as it is in the peer-reviewed literature. In practice, individual-level and patient-focused language is used such as “complex” and “struggled throughout their life,” and nonpharmacologic therapies, such as psychotherapy, are required to be adequately trialled before these terms are applied. Significantly more complex and nuanced definitions must be applied within research to ensure that findings are relevant to practice. In addition, future work should consider the duration, achieved response, and other comorbid diseases when studying the concept of TRD.
Supplemental Material
Supplemental Material, TRDManuscript-SupplementaryFile1 - Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews
Supplemental Material, TRDManuscript-SupplementaryFile1 for Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews by Sage Brown, Katherine Rittenbach, Sarah Cheung, Gail McKean, Frank P. MacMaster and Fiona Clement in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, TRDManuscript-SupplementaryFile2 - Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews
Supplemental Material, TRDManuscript-SupplementaryFile2 for Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews by Sage Brown, Katherine Rittenbach, Sarah Cheung, Gail McKean, Frank P. MacMaster and Fiona Clement in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, TRDManuscript-SupplementaryFile3 - Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews
Supplemental Material, TRDManuscript-SupplementaryFile3 for Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews by Sage Brown, Katherine Rittenbach, Sarah Cheung, Gail McKean, Frank P. MacMaster and Fiona Clement in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, TRDManuscript-SupplementaryFile4 - Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews
Supplemental Material, TRDManuscript-SupplementaryFile4 for Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews by Sage Brown, Katherine Rittenbach, Sarah Cheung, Gail McKean, Frank P. MacMaster and Fiona Clement in The Canadian Journal of Psychiatry
Supplemental Material
Supplemental Material, TRDManuscript-SupplementaryFile5 - Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews
Supplemental Material, TRDManuscript-SupplementaryFile5 for Current and Common Definitions of Treatment-Resistant Depression: Findings from a Systematic Review and Qualitative Interviews by Sage Brown, Katherine Rittenbach, Sarah Cheung, Gail McKean, Frank P. MacMaster and Fiona Clement in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
The authors gratefully acknowledge the valuable contributions of the interviewees.
Data Access
All relevant data are available through the figures and supplementary materials.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Addiction and Mental Health Strategic Clinical Network and funded by grants with the University Hospital Foundation and Johnson & Johnson Health Innovation Partnership.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.