
Abstract
Objective:
Community treatment orders (CTOs) have been used in the treatment of some individuals with serious mental illness who fail to adhere to their psychiatric treatment, leading to frequent hospitalization. This article examines perceptions and knowledge of CTOs amongst outpatient service users in Toronto, Canada.
Method:
Service users under a CTO were matched to a comparison control group of voluntary outpatients (n = 69 in each group). Participants were interviewed using a series of questionnaires aimed at assessing instead of evaluating their knowledge and perceptions of CTOs, as well as understanding their views about the utility and impact of CTOs in the treatment of individuals with mental health issues.
Results:
Participants in the CTO group knew significantly more about CTO processes, restrictions, and procedural protections than the control group. Both groups thought that a CTO could improve certain individuals’ mental health. The control group felt more strongly that a CTO could improve a service user’s physical health by providing better access to care and closer monitoring (P = 0.019) while a significant proportion of the CTO group thought that being on a CTO was better than being in the hospital (P = 0.001) and that service users should be able to contest their CTO (P = 0.001). In addition, CTO group participants were significantly more optimistic about the potential positive impact of CTOs on other service users’ quality of life (P = 0.008) and mental health (P = 0.023) compared to themselves.
Conclusions:
In general, both groups viewed CTOs as potentially capable of positively affecting treatment and lives of some individuals with mental illness.
Community treatment orders (CTOs) have been used in various jurisdictions since the 1960s and are currently in use in the United States, many European countries, Canada, Australia, and New Zealand. CTO legislation was introduced in the Canadian province of Ontario in early 2000 with the objective of ensuring public safety as well as providing care to individuals with severe mental illness (SMI). 1,2 In Ontario, CTOs are valid for up to 6 months at a time and are initiated by a physician. Criteria for a CTO include a minimum of 2 psychiatric admissions or a psychiatric admission lasting for at least 30 days within the past 3 years or a prior CTO issued in the past 3 years. A physician cannot impose a CTO unilaterally: the individual or the designated substitute decision maker (SDM) must provide informed consent. The current legislation in Ontario also allows capable individuals who meet the criteria for a CTO to consent to their own CTO, effectively using them as advance directives in their psychiatric care. However, there are limited data available about the number of service users who utilize CTOs in this manner. 3 There are various mechanisms in place for service users to contest a finding of incapacity for psychiatric treatment and/or their CTOs.
Some individuals with SMI fail to adhere to their psychiatric treatment, leading to frequent hospitalizations. This may be due to a number of factors, including lack of adequate community supports, insufficient psychiatric services, illness severity, and/or lack of insight into their own psychiatric illness. 4,5
Three randomized control trials (RCTs) of CTOs 6 –8 have not reached unequivocal conclusions about the efficacy of CTOs, in part due to their significant methodological shortcomings. 5,9 –11 Swartz and colleagues 7 found no difference in inpatient use between treatment and control groups in bivariate analyses but in multivariate secondary analyses found that sustained outpatient commitment (≥180 days) reduced mean admissions and hospital days in patients with nonaffective psychotic diagnoses. By comparison, Steadman and colleagues 6 found no difference in hospital use between CTO and control groups but qualified their findings because no pick-up orders for noncompliant participants in the CTO group were implemented by the police during the study. This, in turn, significantly compromised the fidelity of the outpatient commitment intervention in this study. Both of these RCT studies were conducted in the United States. A UK study 8 found no difference in inpatient use between individuals on a CTO and control subjects; however, control subjects were under a “leave of absence” from hospital under Section 17 of the Mental Health Act, which confers similar powers of hospital readmission following involuntary hospital treatment. In addition, this study only included participants who were able to give informed consent for participating in the study (capable with regards to making decisions about their psychiatric treatment). Therefore, this study does not include individuals who are typically treated under a CTO in many other jurisdictions and may benefit from this intervention.
CTOs are complex interventions involving legal, medical, and social services systems that are unique to each jurisdiction. 12,13 Hence, conducting and interpreting CTO studies are beset by difficulties. Furthermore, the suitability of RCTs in the evaluation of complex interventions such as CTOs has been questioned. 11 Bearing this in mind, a number of pre-post and cohort studies, including a number of large-scale longitudinal studies, have found CTOs reduce the frequency and length of psychiatric hospitalization and improve treatment adherence. 14 –16 For example, in their study in the state of Victoria, Australia that compared 11,424 individuals placed on a CTO for the first time between 2000 and 2010, to a matched comparison group of 16,161 individuals, Segal and colleagues 14 found that placement on a CTO resulted in 4.6 fewer days per inpatient admission over the course of their study and a reduction of 10.4 inpatient days per CTO period. In addition, CTO placement was associated with lower mortality risk (gain of 3.8 years of life for men and 2.4 years for women, compared to the control group) and a modest improvement in quality of life. 17 Similarly, four small-scale Canadian studies have also shown positive outcomes for CTOs on service utilizations. 18 –21 However, these types of studies have their own significant methodological limitations. 22
In addition, position papers by both the Canadian and the American Psychiatric Associations support the use of CTOs. 23,24 Bearing all these factors in mind, the current body of evidence points to a potential positive impact of CTOs in individuals with SMI and poor treatment compliance in some jursiodictions. 5
In addition to quantitative studies on the clinical impacts of CTOs, a number of qualitative studies of patients’ perspectives of CTOs have been undertaken.
A recent systemic review of qualitative studies of the views and experiences of individuals treated under CTOs identified a number of common themes across seven different countries, 25 including the following elements: service users view CTOs as coercive, but they prefer them to inpatient psychiatric hospitalization; they viewed CTOs as being able to provide a safety net and valued CTOs due to the services that were provided; and they viewed medication adherence as the primary reason for CTOs. Service users also reported that at times, they experienced lack of respect while being treated under a CTO. They also spoke about their lack of knowledge of CTO processes and legislation. Finally, they expressed a feeling of ambivalence with regards to an improved sense of wellness while being treated under force of a CTO.
Currently, four Canadian qualitative studies conducted in two provinces have examined service users’ perception of CTOs in their care 26 –29 and shown similar findings to studies from other jurisdictions. 25
Multiple studies (both qualitative and quantitative) in various jurisdictions have reported that psychiatric treatment under CTOs may indeed contribute to service users’ sense of coercion, 13 but there is marked variation among studies in the levels of coercion reported. Contextual factors, the presence of additional forms of leverage in patients’ lives, and the process of CTO initiation and enforcement may mitigate or enhance perceptions of coercion. In an earlier study on this current study group, we found that the level of perceived coercion reported by CTO participants was significantly higher than that in a voluntary outpatient comparison group. 30 However, in adjusted analyses, service users’ perception of coercion, irrespective of their CTO status, was positively correlated with their previous experience with probation and inversely correlated with the sense of procedural justice in their treatment.
Despite these studies, there is a limited understanding of service users’ knowledge of CTO legal requirements and processes and how they view CTOs as a psychiatric treatment tool in general versus a treatment intervention in their own care. In addition, very little is known about the opinion of service users with SMI who have never been treated under a CTO up to this point, but who may be subjected to one in the future due to the nature and severity of their illness. This study aims to address some of these unanswered questions.
Method
Study Design
Data for the current analyses were drawn from a study we undertook on patients’ perceptions of coercion and procedural justice in their psychiatric treatment (see Nakhost et al. 30 for details). A cross-sectional matched pairs design was used to examine service users’ knowledge and perceptions of community treatment orders. Patients receiving intensive case management (ICM) or assertive community treatment (ACT) who had been placed on a CTO were individually matched to patients receiving these services but never placed on a CTO. Participants were matched on gender, primary diagnosis, and age (plus or minus 8 years). Matching on self-identified racial/ethnic identity occurred in only 73.9% of the final sample. Structured interviews were conducted by an experienced research assistant, who obtained the participants’ written informed consent prior to the interview. Research ethics approval was obtained from the research ethics boards of St Michael’s Hospital and the Centre for Addiction and Mental Health. Recruitment and data collection occurred between July 2014 and November 2015.
Sample
Participants were drawn from 3 mental health centres in the city of Toronto: a large psychiatric hospital, the mental health service of an urban general hospital, and a community-based mental health agency. All participants were outpatients. Inclusion criteria included age 18 to 65 years and ability to speak English and to give informed consent for participating in a survey. Patients in the CTO group were subjected to a CTO within the past 18 months, and patients in the control arm were never placed on a CTO. Individuals on CTOs were identified through an administrative database of CTO patients. Potential participants were informed by their community mental health teams of the research and offered the contact information of the research coordinator for additional information, or, alternatively, participants gave permission to have their contact information shared with the research coordinator. Participants in the comparison group were selected from the same ICM or ACT service providers based on the matching criteria upon referral by their case managers, who were informed of the selection criteria for the comparison group. To confirm that participants recruited for the comparison group were not subject to a past CTO, they were asked by the research coordinator whether they were ever on a CTO prior to interview.
Survey
Participants were surveyed using a series of fixed-choice and open-ended items. In addition to demographic questions, the survey included items about diagnosis, previous psychiatric hospitalizations, current treatment, and criminal justice involvement. Primary diagnosis was self-reported, and consent was also provided by 125 (81.5%) participants to cross-validate their self-reported diagnosis with their chart diagnosis. Where discrepancies occurred between these two data sources (occurring in 13 cases), the chart diagnosis was used. The Colorado Symptom Index (CSI) was used to query the presence of symptoms of mental illness. Possible scores ranged from 14 to 70, with higher scores representing greater frequency of symptoms. 31 A score of 30 has been proposed as the “clinical cutoff” for CSI, where it can identify individuals who are likely in need of mental health services. 32
Participants in both groups were asked questions that explored their knowledge and understanding of the CTO process and their opinion of the impact of CTOs. Response options for questions about their knowledge of CTO processes included “yes,” “no,” “don’t know,” and “refuse” to answer. Participants were also asked to rate their agreement with statements about the impact of CTOs on a Likert scale from 1 to 5, with 1 as not at all and 5 as absolutely.
If a participant from either group responded no to the first question about CTOs, “I have heard of CTOs before,” they were provided with additional information, including an informational pamphlet about the basic rules and application of CTOs in Ontario, before proceeding. This pamphlet was developed based on a standard community treatment plan (CTP) that is part of every CTO in Ontario and is provided to all individuals placed on a CTO. Interviewers also offered to review this pamphlet with all interested participants before proceeding to the next section. Participants were then asked about their opinion of the potential impact of CTOs in general on individuals who have mental health issues. The CTO group was asked to answer these questions without thinking about their own personal experiences with the CTO/CTO process and rather answer broadly based on how they thought a person with mental illness would respond/react to treatment under a CTO. Responses of the CTO and control groups were compared. Finally, individuals in the CTO group were asked about how they were personally affected by their CTOs using questions similar to those used to solicit their views about the impact of CTOs in general. Responses from the CTO group about the potential impact of CTOs on individuals with mental health issues in general were compared to their responses about the impact of CTOs on them personally.
Statistical Analysis
Data were analyzed using descriptive statistics conducted in SPSS 24. 33 Comparison of pairs was completed using McNemar’s test for nominal data, Wilcoxon signed rank test for ordinal data, and paired Student’s t test for parametric ratio data. Wilcoxon signed rank tests were also used to compare the CTO group’s views about the impact of CTOs on individuals with mental health issues in general and the impact of CTOs on them personally. Due to multiple comparisons, the Benjamini-Hochberg method of controlling the false discovery rate was used to calculate corrected levels of significance. A q value of 0.05 was used for the false discovery rate. The Benjamini-Hochberg method was applied to a total of 17 comparisons appearing in the tables.
An a priori power analysis was conducted in G*Power. 34 Using an α of 0.05, a power of 0.80, and a medium effect size, 34 subjects were needed in each group to test mean differences.
In the comparison of groups on knowledge of CTOs, response options of “no,” “don’t know,” and “refused to answer” were collapsed together due to small counts for some response options and to meet the assumptions of McNemar’s test. Pairwise deletion was used when a CTO case or its control case had missing responses (i.e., “refuse to answer” response) to questions about the impact of CTOs. Our findings were organized and reported based on the EQUATOR (Enhancing the Quality and Transparency of Health Research) Network’s standards using the STROBE checklist for a cross-sectional study (see online Appendix A). 35
Results
Case managers referred 189 individuals as possible participants. From this group, 13 individuals declined to participate and 3 could not be reached. From the remaining 166 potential participants, 14 did not meet the inclusion criteria. Finally, 152 face-to-face structured interviews were conducted (79 in the CTO group and 73 in the comparison group). Of these, 14 participants were excluded due to withdrawal from the study (n = 2), incorrect identification as a match by their case managers (n = 8), and being matched to participants who withdrew or did not meet study criteria (n = 4). From this group, 138 participants, 69 in each arm, were included in the final analysis.
At the time of the interviews, 67 out of 69 participants (97.1%) in the CTO group were being treated under a CTO, of whom 29 individuals (42.0%) had at least experienced 1 CTO, 12 (17.4%) had been treated under 2 CTOs, and the remaining 28 (40.6%) had experienced 3 or more prior CTOs. The control individuals had never been treated under a CTO.
Table 1 presents the sociodemographic and other characteristics of the sample. Participants faced difficult socioeconomic circumstances as over 90% identified disability or social assistance as their primary source of income. A significantly higher number of participants in the CTO group had been involuntary hospitalized over the previous year. The majority of the CTOs were initiated during a period of hospitalization (88.4%). Only 12 individuals in the CTO group (17.4%) could recall having ever been brought to the hospital for not following the terms of their treatment plan, including 8 individuals (11.6%) in the past year.
Demographic and Characteristics of the Study Sample.a
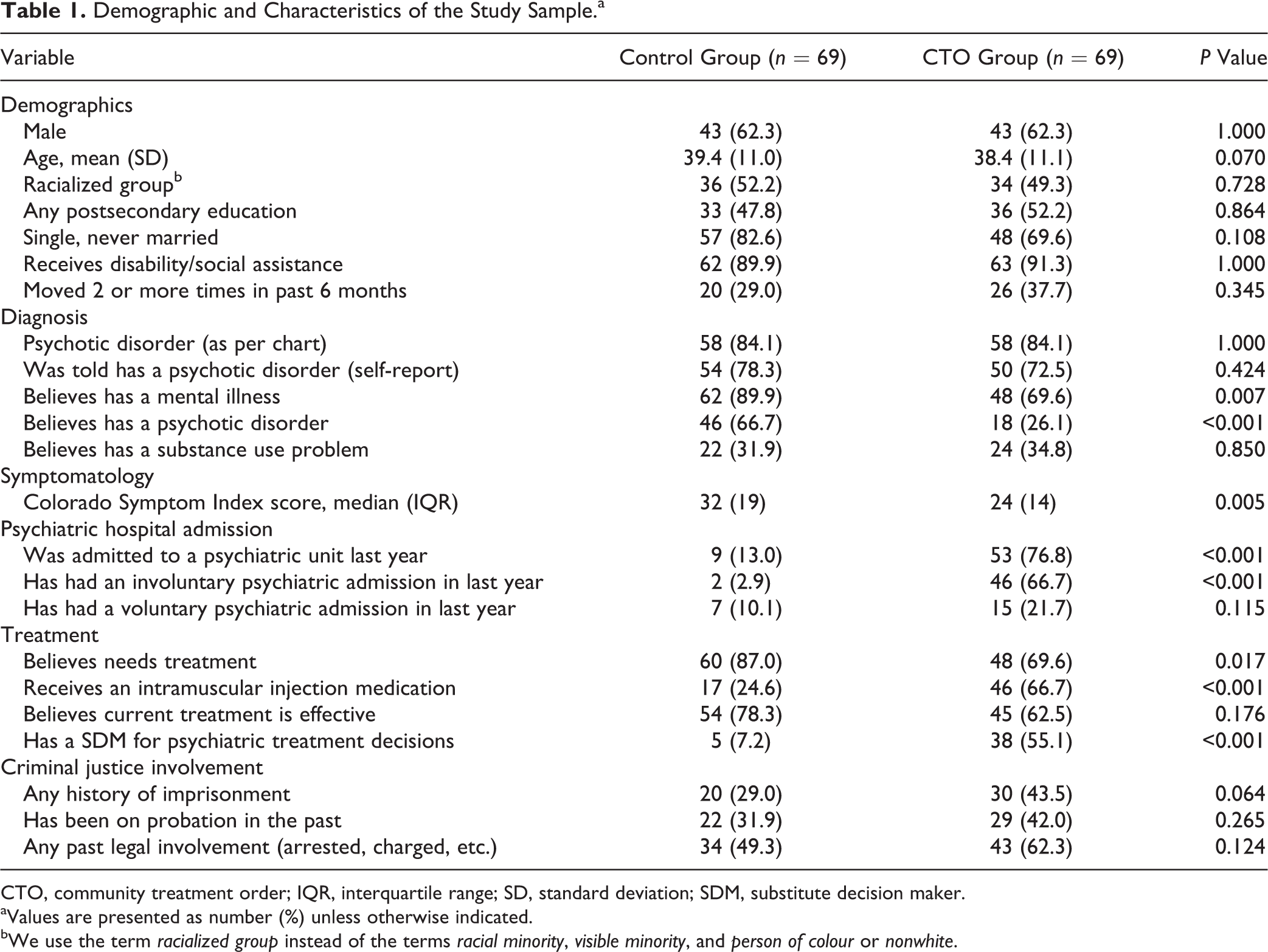
CTO, community treatment order; IQR, interquartile range; SD, standard deviation; SDM, substitute decision maker.
aValues are presented as number (%) unless otherwise indicated.
bWe use the term racialized group instead of the terms racial minority, visible minority, and person of colour or nonwhite.
The knowledge of CTOs of both groups is shown in Table 2. Unsurprisingly, individuals who were treated under a CTO knew significantly more about them compared to the control group. However, more than three-quarters of the comparison group had not even heard of CTOs previously, and 16 (23.2%) of these participants declined to respond to questions about their knowledge of CTOs after being provided with information about the CTO process. By comparison, almost all participants in the CTO group (97.2%) had heard of CTOs prior to their interview. The majority of the CTO group showed an awareness of what a CTO could impose upon a person: 87% knew that CTOs could require a person to attend appointments with the psychiatrist/mental health team, and 97.5% believed that CTOs require people subject to them to take their medications as prescribed.
Comparison of Groups on Knowledge about CTOs.
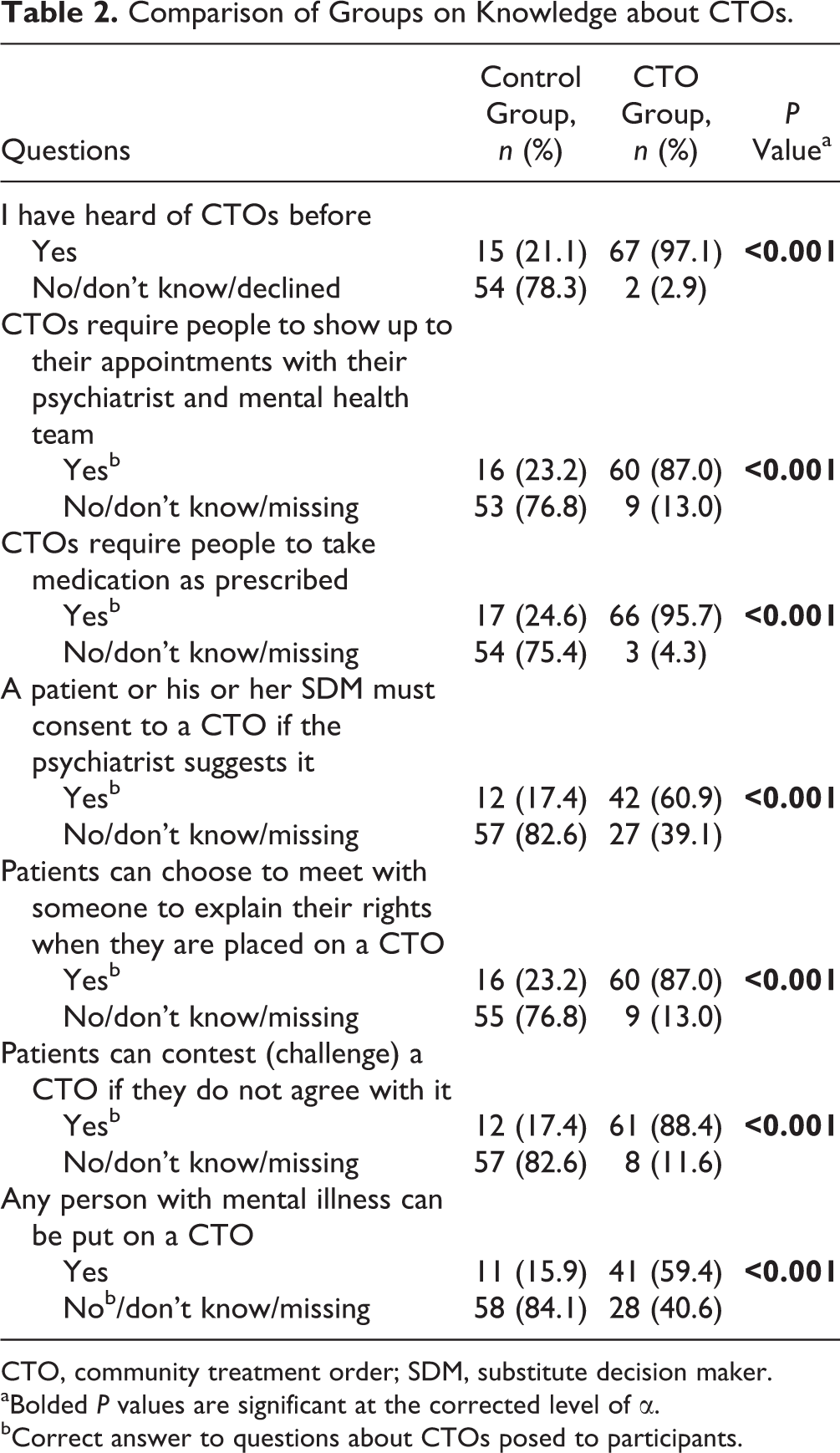
CTO, community treatment order; SDM, substitute decision maker.
aBolded P values are significant at the corrected level of α.
bCorrect answer to questions about CTOs posed to participants.
The majority of the CTO group (60.6%) believed that any person with a mental illness could be put on CTO. Procedural protections were commonly understood. Most CTO patients (87.3%) realized that a person on a CTO could choose to meet with a rights advisor, and most (88.7%) appreciated that a person made subject to a CTO could contest it.
Next, the participants were asked about their perception of the potential impact of a CTO on an individual with mental health issues in general as well as their opinion about the current CTO process in Ontario (Table 3). They were asked to answer the questions in this section without thinking about their own personal experiences with the CTO/CTO process and rather answer broadly based on how they thought a person with mental illness would respond/react to treatment under a CTO. A significantly higher number of individuals in the CTO group thought that being on a CTO was better than being in the hospital and that service users should be able to contest their CTOs if they do not agree with them. A significantly higher number of the participants in the control group thought that CTOs could improve a service user’s physical health by improving access to health services and closer monitoring. Nearly half of individuals in the CTO group and just over half of participants in the control group thought that CTOs could improve a patient’s quality of life. In addition, a majority in both groups thought CTOs could improve a service user’s mental health state.
Comparison of Groups on Opinions of CTOs.
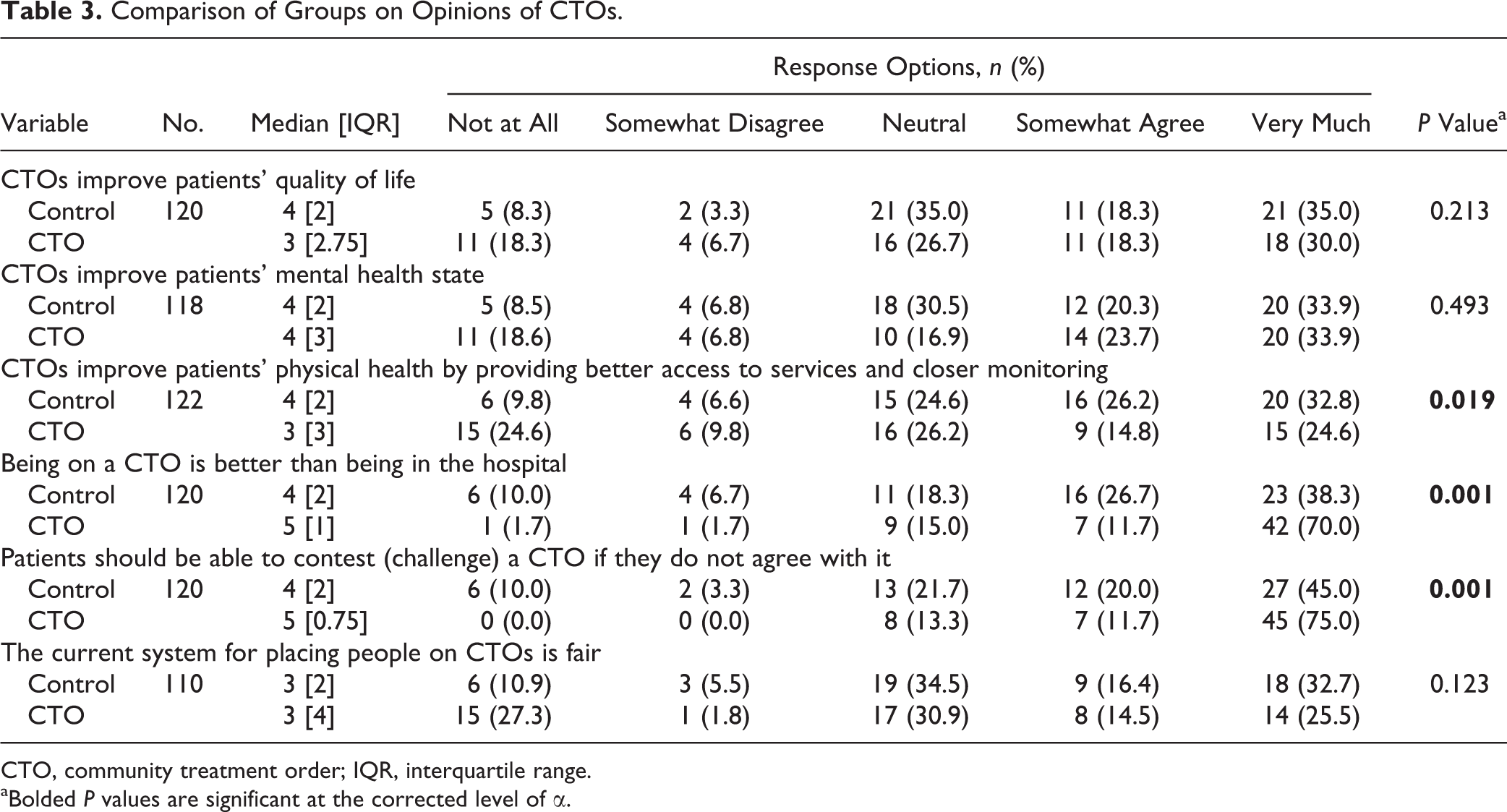
CTO, community treatment order; IQR, interquartile range.
aBolded P values are significant at the corrected level of α.
Individuals in the CTO group were asked about how they were personally affected by their CTOs. These responses were compared to their responses about the potential impact of a CTO on an individual with mental health issues in general (Table 4). The participants in the CTO group were significantly more likely to positively view the impact of CTOs on someone else’s quality of life and mental health than their own quality of life and mental health.
CTO Group’s Views about the Impact of CTOs on Individuals with Mental Health Issues in General versus the Impact of CTOs on Them Personally.
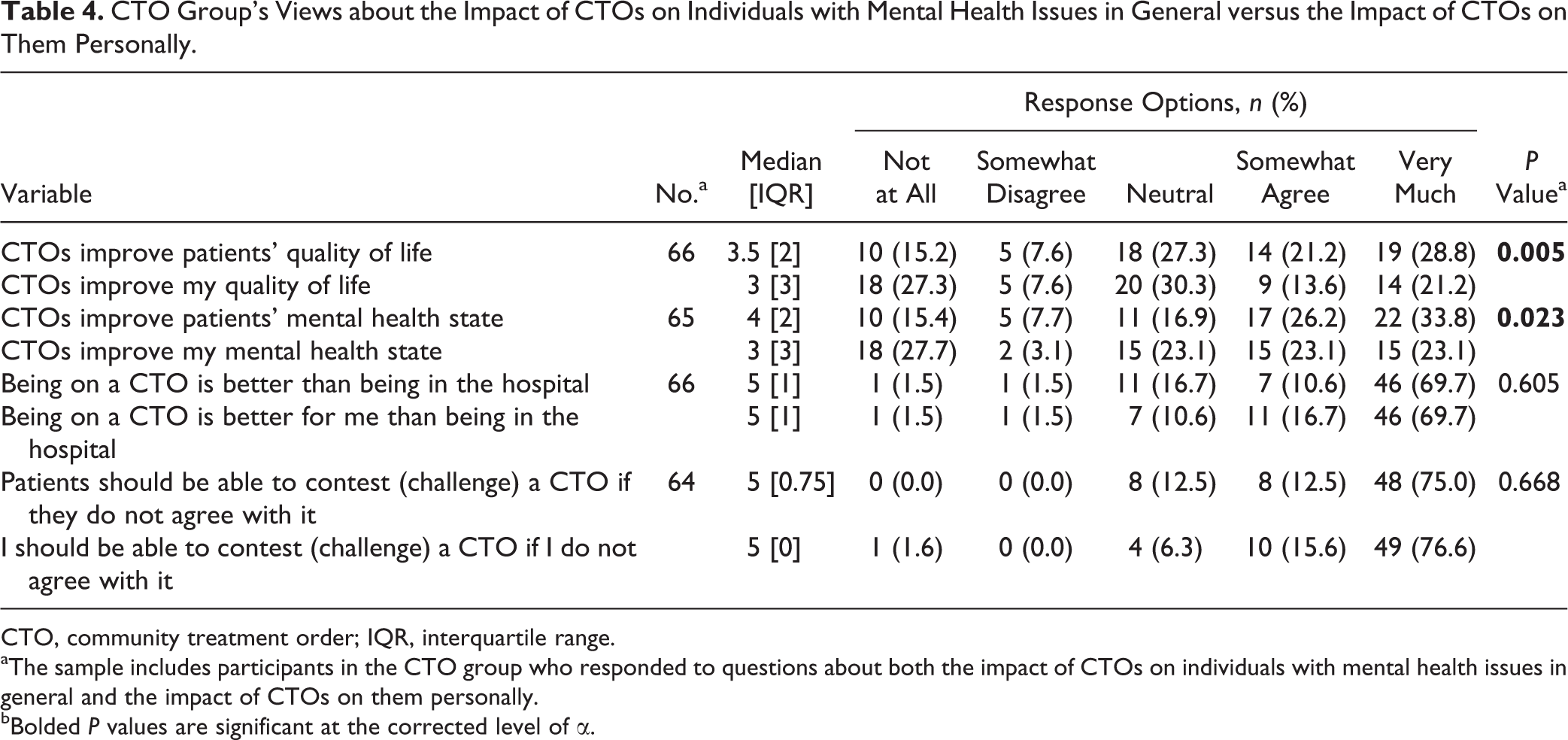
CTO, community treatment order; IQR, interquartile range.
aThe sample includes participants in the CTO group who responded to questions about both the impact of CTOs on individuals with mental health issues in general and the impact of CTOs on them personally.
bBolded P values are significant at the corrected level of α.
When the CTO participants were asked about the potential impact of CTOs on their own treatment engagement and lives (Table 5), many reported improved engagement with their mental health treatment team and better adherence to medications on the CTO. Most did not perceive any negative impact of CTOs on their legal involvement and/or hospitalization rates. However, participants may have concerns about the impact of CTOs in other areas of their lives not currently explored in this study.
CTO Group’s Specific Questions on Perceived Personal Impact of CTOs on Treatment Engagement and Personal Life.
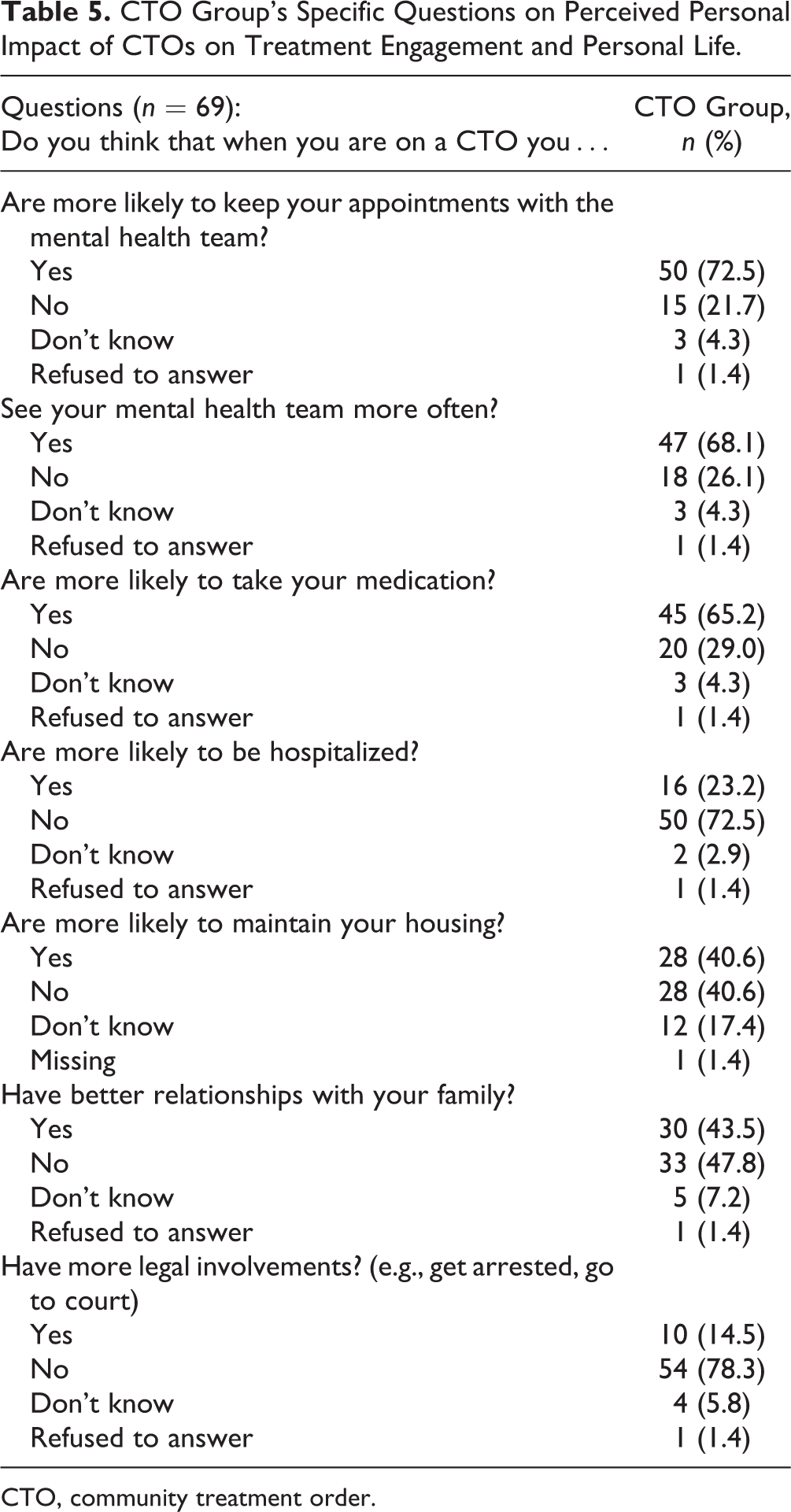
CTO, community treatment order.
Discussion
In many ways, the CTO group in our study resembles individuals who are treated under CTOs in other jurisdiction, which typically include men around 40 years old with a diagnosis of psychotic illness and a history of psychiatric hospitalizations and criminal justice involvement. 12 A significantly larger proportion of the participants in the CTO group did not believe that they had a psychotic illness or require treatment compared to the control group, which may explain the higher rate of use of intramuscular antipsychotic medications and prevalence of having a SDM in this group. A significantly higher number of participants in the CTO group were involuntary hospitalized over the previous year, potentially indicating the recent severity of their illness. However, the participants in the CTO group reported to be significantly less symptomatic than the comparison group. It is possible that CTO group participants underreported symptoms or did not believe that their experiences were symptoms of illness. However, it is also possible that CTO group participants were experiencing fewer symptoms due to their mandatory community treatment.
Understanding service users’ knowledge and attitudes toward CTOs is important information that is necessary in understanding how CTOs should be designed and administered. Our results suggest that in general, most participants who have been on CTOs had reasonable knowledge of how CTOs work. Of those who had been made subject to a CTO, almost all appreciated the powers of a CTO and the type of requirements CTOs place on them and the procedural protections available to them. However, some were not fully aware of the exact criteria for placing someone on CTOs in Ontario. This lack of knowledge about CTO legislation and processes is in keeping with the findings from qualitative studies of CTOs. 5 In comparison, the majority of the participants in the control group did not know about CTOs prior to taking part in this study. These findings point to a potential area for further education and training for service users and their SDMs, rights advisors, and care providers. Our findings are similar to results obtained by McKenna et al. 36 when assessing the knowledge of CTOs in voluntary and CTO outpatients in New Zealand. They found that 73% of the CTO group understood that CTOs required people to engage with services compared to 29% in the control group. In addition, 97% of their CTO group knew that CTOs required people to take their medications compared to 38% in their control group. 36
In general, the majority of participants in both groups in our study viewed CTOs as having a positive impact on the physical and mental health of service users with SMI, pointing to a potential place for CTOs in the treatment of certain individuals with mental health issues. Half of the CTO and control groups stated that CTOs could improve the quality of life and the mental state of someone with mental health issues. Participants were split on whether CTOs were fair. The majority of the participants in the CTO group felt more optimistic about the potential positive impact of CTOs on people with SMI in general. In addition, many stated that while treated under a CTO, they were more likely to be better engaged in their own psychiatric care.
These findings align with many of the themes of the systematic review of Corring et al. 25 as well as findings from previous qualitative studies of service users in Canada, 26 –29 where many were able to appreciate the potential positive impact and benefits of CTOs while expressing some concerns about mandated psychiatric treatment in the community.
Limitations
First, some control subjects had little awareness of CTOs and were unsure about the issues surrounding them. Second, our sample size was small and confined to a large Canadian metropolitan area. In addition, data on the number and characteristics of service users who were informed about the study but had declined to participate were not collected. Other methodological issues also include the reduction of complex phenomena to constrictive responses, 36 possible response bias related to CTO participants feeling obliged to respond more positively about a treatment they are receiving, and/or referral of participants with more positive views of CTOs by their case managers. The generalizability of these findings is not clear as services users’ perception of their psychiatric care in general and CTOs in particular is potentially informed by the unique interplay between mental health services, mental health laws/legislation, and social services in each jurisdiction. Therefore, service users in jurisdictions where treatment under a CTO can provide better access to other services (e.g., better access to housing, primary care, and intensive case management) as well as psychosocial interventions may have a different view of CTOs compared to jurisdictions where the only role and benefit of a CTO is in treatment compliance.
Conclusions
Our findings show that the majority of service users in our study thought CTOs could improve the physical and mental health state of certain individuals with mental health issues as well as improve their quality of life and treatment adherence. This points to a potential role for CTOs in treating a subset of individuals with mental health issues to facilitate stability in the community, adherence to treatment, and access to needed psychosocial supports. Identifying who this population is and ensuring that CTOs are delivered in a manner that is therapeutic are vital.
Supplemental Material
Supplemental Material, Appendix_A_STROBE_checklist_v4_case-control-_Nakhost_et_al - Service Users’ Knowledge and Views on Outpatients’ Compulsory Community Treatment Orders: A Cross-Sectional Matched Comparison Study
Supplemental Material, Appendix_A_STROBE_checklist_v4_case-control-_Nakhost_et_al for Service Users’ Knowledge and Views on Outpatients’ Compulsory Community Treatment Orders: A Cross-Sectional Matched Comparison Study by Arash Nakhost, Alexander I. F. Simpson and Frank Sirotich in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
We thank the Psychiatric Associates of St Michael’s Hospital, Toronto, Ontario, Canada, for their support of this project. This project was also greatly aided by Ms. Maria Boada, CTO program manager at Canadian Mental Health Association (CMHA; Toronto Branch); Ms. Kimberly Geller, CTO coordinator at Centre for Addiction and Mental Health (CAMH); and Dr. Justin Geagea, who assisted in patient recruitment. Ms. Katherine M. Francombe Pridham, Ms. Caroline Patterson, and Ms. Camille Arkell helped with patient interviews.
Author Contribution
Drs. Nakhost, Simpson and Sirotich contributed equally to the writing of this manuscript.
Data Access Statement
This study was a multisite study that required data-sharing agreements between 3 different institutions and approval by multiple research ethics boards (REBs). These agreements do not allow sharing of the data set, and data sharing was not covered by the study’s REB approvals.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Ontario Academic Health Science Center Alternate Funding Plan Innovation Funds (SMHAIF-099). The funder had no influence on interpretation, reporting, or the decision to publish this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.