
Abstract
Objective:
Housing First is increasingly put forward as an important component of a pragmatic plan to end homelessness. The literature evaluating the impact of Housing First on criminal justice involvement has not yet been systematically examined. The objective of this systematic review is to examine the impact of Housing First on criminal justice outcomes among homeless people with mental illness.
Method:
Five electronic databases (PsycINFO, MEDLINE, Embase, CINAHL, Web of Science) were searched up until July 2018 for randomised and nonrandomised studies of Housing First among homeless people with a serious mental disorder.
Results:
Five studies were included for a total of 7128 participants. Two studies from a randomised controlled trial found no effect of Housing First on arrests compared to treatment as usual. Other studies compared Housing First to other programs or compared configurations of HF and found reductions in criminal justice involvement among Housing First participants.
Conclusions:
This systematic review suggests that Housing First, on average, has little impact on criminal justice involvement. Community services such as Housing First are potentially an important setting to put in place strategies to reduce criminal justice involvement. However, forensic mental health approaches such as risk assessment and management strategies and interventions may need to be integrated into existing services to better address potential underlying individual criminogenic risk factors. Further outcome assessment studies would be necessary.
Housing First (HF) provides immediate access to subsidised housing along with support services to homeless people, including those with mental illness. Because it increases residential stability 1 –6 and results in significant cost offsets, 7 it is put forward by policy makers as an important component of a pragmatic plan to end homelessness. 8
It has been hypothesized that the benefits of HF include a reduction in criminal justice involvement (CJI). 9 CJI is especially prevalent among homeless people with mental illness, with lifetime arrest rates between 63% and 90%, 10 and engenders great costs and consequences. 10 –15 The expectation that HF will reduce CJI reflects the assumption that mental illness and residential instability are main risk factors for CJI among homeless people with mental illness, while other factors may play a more prominent role. These additional risk factors may be understood from a societal perspective, according to which social disadvantage and greater surveillance result in social profiling, 16 and from a clinical perspective, according to which CJI results from individual factors such as substance abuse or antisociality. Although these perspectives are noncompeting, this article focuses on the second.
According to the risk-need-responsivity model, 17 services provided to a justice-involved individual should target specifically criminogenic factors to reduce offending. The dynamic factors that most strongly predict recidivism are the following: antisocial patterns, procriminal associations and attitudes, substance abuse, poor satisfaction in relationships/family and at work/school, and lack of positive involvement in leisure activities. 17 –20 Changes in factors related to antisocial attitudes, satisfaction at school, relationships (including prosocial peers), use of leisure time, and substance abuse are most likely to reduce recidivism. 21
The literature evaluating the impact of HF on CJI among homeless persons with mental illness has not yet been systematically examined. This knowledge gap is an obstacle to the development and implementation of evidence-informed practices to reduce CJI in this population. The objective of this systematic review was to examine the impact of HF on CJI outcomes among this population.
Methods
This systematic review followed the PRISMA guidelines 22 and was registered on Prospero (CRD42018100729).
Eligibility Criteria
We included randomised and nonrandomised studies of interventions that followed the HF model, with any comparison group. We included studies published after 2000 that relied on a sample composed of homeless individuals or precariously housed individuals, of whom at least half had a diagnosis of a ‘serious mental disorder’ (e.g., mood disorder, psychotic disorder). The other inclusion criterion was reporting of at least one outcome related to CJI, including but not limited to arrests, charges, and incarceration. When a particular outcome was reported in several publications of the same study (e.g., subgroup analyses), we selected the paper with the most comprehensive sample.
Search Strategy, Selection, and Data Collection
We identified studies through PsycINFO, MEDLINE, Embase, CINAHL, Web of Science, and manual scan until July 2018. As advised by a librarian, we used a combination of subject headings and keywords around homelessness, CJI, and mental disorders—but not around HF to include interventions that followed the model without labelling it as such.
Two reviewers independently assessed the eligibility and the methodological quality of the studies and extracted the data, resolving disagreements through discussion and consulting protocols, referenced articles, or tool kits, if necessary. 23 –25 We used the Cochrane Collaboration’s tool for assessing risk of bias in randomised trials 26 and the ROBINS-I (Risk of Bias in Non-randomised Studies–of Interventions) 27 to rate randomised and nonrandomised studies on the same scale. Descriptions of the interventions were examined to identify criminogenic factors that they aimed to address.
The online supplement details the complete search strategy, the variables extracted, and the methodological assessment.
Results
Table 1 presents the 5 studies 5,6,28 –30 included (N = 7128 participants; see Suppl. Figure S1 for the selection process). Two studies from a randomised trial of HF compared to treatment as usual (TAU) reported no effect on arrests, with both groups experiencing similar decreases (e.g., 2-year difference in mean change for HF is 95% CI: 1.05 [0.62 to 1.80]). 5,6 Other studies (2 of which were judged to be at serious risk of bias) compared HF to other programs or compared configurations of HF and generally found a reduction in CJI among HF participants. 28 –30
Studies Reporting on the Impact of Housing First on Criminal Justice Outcomes.
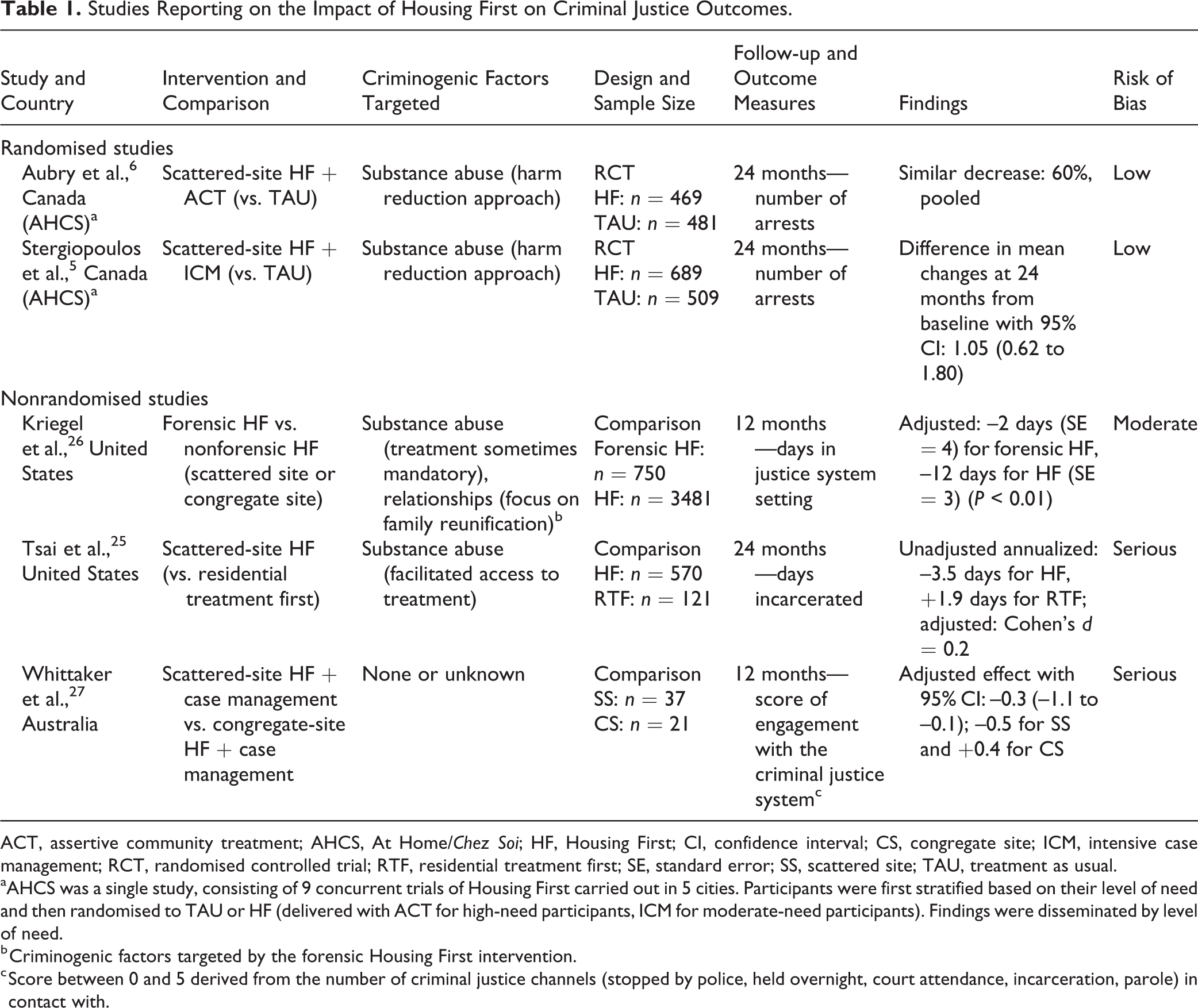
ACT, assertive community treatment; AHCS, At Home/Chez Soi; HF, Housing First; CI, confidence interval; CS, congregate site; ICM, intensive case management; RCT, randomised controlled trial; RTF, residential treatment first; SE, standard error; SS, scattered site; TAU, treatment as usual.
aAHCS was a single study, consisting of 9 concurrent trials of Housing First carried out in 5 cities. Participants were first stratified based on their level of need and then randomised to TAU or HF (delivered with ACT for high-need participants, ICM for moderate-need participants). Findings were disseminated by level of need.
b Criminogenic factors targeted by the forensic Housing First intervention.
c Score between 0 and 5 derived from the number of criminal justice channels (stopped by police, held overnight, court attendance, incarceration, parole) in contact with.
Discussion
This systematic review suggests that HF does not, on average, have much, if any, impact on CJI. The decrease in CJI observed in HF participants of studies comparing configurations is consistent with the phenomenon of regression to the mean. 31 The At Home/Chez Soi randomised trial found no differences between the HF and TAU groups. A review of the cost offsets of HF for individuals with mental illness and/or substance use disorder found that nonrandomised studies reported decreases in justice costs, but not randomised trials. 7 The fact that both reviews yield similar findings suggests that, on average, HF has little impact on CJI.
It also suggests, based on published descriptions, that HF does not systematically address criminogenic factors. HF programs that follow the Pathways model, however, are intended to be recovery oriented and thus support clients in the accomplishments of their own objectives. 32 Case managers may thus indirectly, on a case-by-case basis, address criminogenic factors related to relationships, work/school, or leisure, 33 as highlighted in logic models 34 without conceptualizing them as potential protective factors toward reduction of CJI.
Not recognizing the importance of criminogenic factors among justice-involved individuals with mental illness results in failures to provide them with evidence-based practices. 35,36 Indeed, the policy response to offenders with mental illness has been to use the criminal justice system to divert the individual to mental health services (e.g., forensic mental health services, mental health courts, jail diversion based on case management) 36 –38 with the expectation that recidivism would be reduced. These interventions may successfully improve clinical measures, but they do not improve CJI outcomes. 36,39 While residential stability and symptoms reduction have value in themselves, independent of any reduction in arrests or incarceration they may achieve, integration of forensic knowledge into HF may be needed for it to reduce CJI. 9 Components of forensic assertive community treatment 40,41 could be integrated into regular teams by including professionals trained in risk assessment/management and offender rehabilitation strategies. For example, in addition to addressing use of leisure time and substance abuse, HF could implement voluntary adjunctive interventions such as victim impact intervention to develop empathy 42 and cognitive behavioural therapy to enhance anger management. 43 From a societal perspective, other interventions may be required to address social disadvantage beyond residential instability, as many recently housed participants still live on very low incomes and in disadvantaged neighbourhoods, which increases the odds of CJI. 35,44,45
Community services such as HF are potentially an important setting to put in place strategies to reduce CJI, given the growing number of people receiving HF. However, knowledge about risk assessment/management and crime desistance strategies may need to be integrated into existing services to better address criminogenic factors. Stakeholders at the intersection of mental health and justice in Canada have identified this knowledge transfer as a key priority. 46 Partnerships between forensic and community mental health services must be strengthened to promote the dialogue on and use of evidence-based risk management strategies among those at risk of criminal behaviour.
This systematic review has some limitations. First, the randomised trials identified were conducted in Canada and report only self-reported arrests. Although self-reported outcomes are fairly reliable, 47 future studies may want to validate the findings with a range of outcomes identified from administrative data. Furthermore, participants in the TAU arm may also have received existing services (although not HF, given that it was not otherwise available in Canada at the time of the study). Second, there may be other explanations for the lack of effect of HF on CJI. Increased monitoring of criminal activity or substance use in the HF arm or a heterogenous treatment effect based on subgroups of participants (e.g., chronically homeless or periodically homeless) and/or types of crime could in part account for the lack of effect and should be the subject of future research. Finally, to our knowledge, no studies have examined the specific criminogenic factors of people who are homeless. Because they have been validated in several subpopulations, we expect them to also be important among justice-involved homeless people. However, other factors could also be a criminogenic risk factor for some. Future studies should aim to increase our understanding of criminogenic factors of homeless people with mental illness and the best practices to address them.
Conclusion
This systematic review suggests that HF has little impact on CJI and does not systematically target criminogenic factors beyond substance abuse, although case managers may do so in individual cases. HF could be an important setting to put in place strategies to reduce CJI. However, forensic mental health approaches such as risk assessment and management strategies and interventions may need to be integrated into existing services to better address potential underlying individual criminogenic factors. Further outcome assessment studies would be necessary.
Supplemental Material
CPA815902_onlinesupplement - The Impact of Housing First on Criminal Justice Outcomes among Homeless People with Mental Illness: A Systematic Review: L'effet de « Logement d'abord » sur les résultats de justice pénale chez les personnes en situation d’itinérance vivant avec une maladie mentale : une revue systématique
CPA815902_onlinesupplement for The Impact of Housing First on Criminal Justice Outcomes among Homeless People with Mental Illness: A Systematic Review: L'effet de « Logement d'abord » sur les résultats de justice pénale chez les personnes en situation d’itinérance vivant avec une maladie mentale : une revue systématique by Marichelle C. Leclair, Félicia Deveaux, Laurence Roy, Marie-Hélène Goulet, Eric A. Latimer and Anne G. Crocker in The Canadian Journal of Psychiatry
Footnotes
Data Access
The data collected in the context of this systematic review may be obtained from the first author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Marichelle Leclair would like to acknowledge the financial support of Fonds de recherche Québec–Société et Culture (FRQ-SC) in the form of an MSc fellowship and Équipe Vulnérabilité, intégration sociale et violence (VISEV) as a bursary. Félicia Deveaux is supported by the FRQ-SC in the form of an MSc fellowship. Marie-Hélène Goulet is supported by a postdoctoral fellowship from the Canadian Institutes of Health Research (CIHR). Laurence Roy is supported by a salary award from Fonds de recherche Québec–Santé (FRQ-S; Junior 1).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.