
Abstract
Objectives:
Early intervention programs are effective for improving outcomes in first-episode psychosis; however, less is known about their effectiveness for mood and anxiety disorders. We sought to evaluate the impact of an early intervention program for emerging adults with mood and anxiety disorders in the larger health system context, relative to standard care.
Methods:
Using health administrative data, we constructed a retrospective cohort of cases of mood and anxiety disorders among emerging adults aged 16 to 25 years in the catchment of the First Episode Mood and Anxiety Program (FEMAP) in London, Ontario, between 2009 and 2014. This cohort was linked to primary data from FEMAP to identify service users. We used proportional hazards models to compare indicators of service use between FEMAP users and a propensity score–matched group of nonusers receiving care elsewhere in the health system.
Results:
FEMAP users (n = 490) had more rapid access to a psychiatrist relative to nonusers (hazard ratio [HR], 2.82; 95% confidence interval, 2.45 to 3.26; median time, 16 vs. 71 days). In the year following admission, FEMAP users also had lower rates of emergency department use for mental health reasons (HR, 0.73; 95% CI, 0.53 to 0.99). We did not observe differences in psychiatric hospitalization rates.
Conclusions:
An early intervention model of care for mood and anxiety disorders is associated with better access to psychiatric care and lower use of the emergency department. Our findings suggest that early intervention services for mood and anxiety disorders may be beneficial from a health systems perspective, and further research on the effectiveness of this model of care is warranted.
Background
Nearly 75% of all lifetime mental disorders begin during adolescence and early adulthood. 1 Recognition of this has led to an increased interest in and emphasis on the mental health of emerging adults. Over the past 20 years, mental health systems worldwide have devoted extensive resources toward the development and implementation of early intervention services for a first episode of psychotic disorder. These programs have been shown to be both effective 2 –4 and cost-effective 5 for improving outcomes in first-episode psychosis.
However, the field of mood and anxiety disorders has been slow to follow this lead, despite growing consensus that models of care targeting emerging adults in the early stage of illness are needed. 6 There is emerging evidence that an extended duration of untreated illness is associated with poor outcomes for mood and anxiety disorders. 7 –9 If left untreated, adolescent mental disorders often recur and become chronic, 10,11 potentially leading to impaired social, educational, and career development and poor trajectories into adulthood. 12,13 Furthermore, suicide is the second leading cause of death among emerging adults between the ages of 15 and 24 in North America, 14,15 and more than 75% of youth suicides involve a history of depression. 16 Recent data suggest that all-cause mortality is nearly 3 times higher among emerging adults with depression, relative to matched controls, in the 3-year period after first diagnosis. 17 Early intervention models of care have reduced this early all-cause mortality for psychotic disorders. 4
To our knowledge, there is currently only one established early intervention program for mood and anxiety disorders in Canada—the First Episode Mood and Anxiety Program (FEMAP) in London, Ontario, targets emerging adults between the ages of 16 and 25 years who are experiencing moderate to severe symptoms and who have not yet experienced longstanding functional deterioration. 18 The goal of FEMAP is “to identify youth at critical developmental life stages who are just beginning to depart from their expected developmental trajectory and intervene by providing outpatient treatment before these youth become chronically disabled from mental illness.” 18 This program is based on the early intervention for psychosis model, and its evolution has been described in detail elsewhere. 19 In brief, key components of FEMAP include community outreach and engagement; provision of services in a youth-friendly, nonstigmatizing, community-based setting; an open door self-referral policy; a detailed, in-person intake assessment to determine suitability for the program; treatment regimen and duration based on clinical need and provided by a multidisciplinary team; and linkages with alternative services, if needed. 19
We sought to evaluate the access to and impact of FEMAP within the larger health system context using linked population-based health administrative data from multiple service providers. Our objectives were 1) to describe how users of FEMAP differ from emerging adults with mood and anxiety disorders in the program catchment area who do not use these services, based on sociodemographic, clinical, and service use characteristics, and 2) to evaluate the impact of FEMAP by comparing mental health process and outcome indicators between emerging adults with mood and anxiety disorders using FEMAP services and a matched group of concurrent controls not accessing these services. We compared use of outpatient psychiatry (process indicator), primary care, emergency department (ED) visits, inpatient hospitalizations, and involuntary admissions for the 1-year period following FEMAP admission.
Methods
Study Setting
FEMAP is the only program targeted at emerging adults with mood and anxiety disorders in the area, and the program accepts patients from across the catchment of the local health authority. This covers a wide geographic area with a mix of urban and rural communities. It includes approximately 125,000 emerging adults in the age range served by FEMAP, and the city of London, Ontario, is also home to 1 university, 3 affiliated university-colleges, and 1 community college, which leads to an influx of approximately 40,000 postsecondary students during the academic year.
Emerging adults with mood or anxiety concerns are admitted to FEMAP if they meet the following eligibility criteria: 1) aged 16 to 25 years; 2) evidence of a primary mood disorder (including bipolar disorder) or anxiety disorder; 3) lifetime duration of psychotropic medication of less than 18 months; 4) absence of developmental delays, major comorbid medical issues (e.g., cancer, cystic fibrosis, uncontrolled epilepsy), or history of serious head injury; 5) absence of a primary substance use problem that preceded the mood or anxiety symptoms based on patient history; and 6) no outstanding legal issues requiring ongoing contact with the criminal justice system. 19
Source of Data
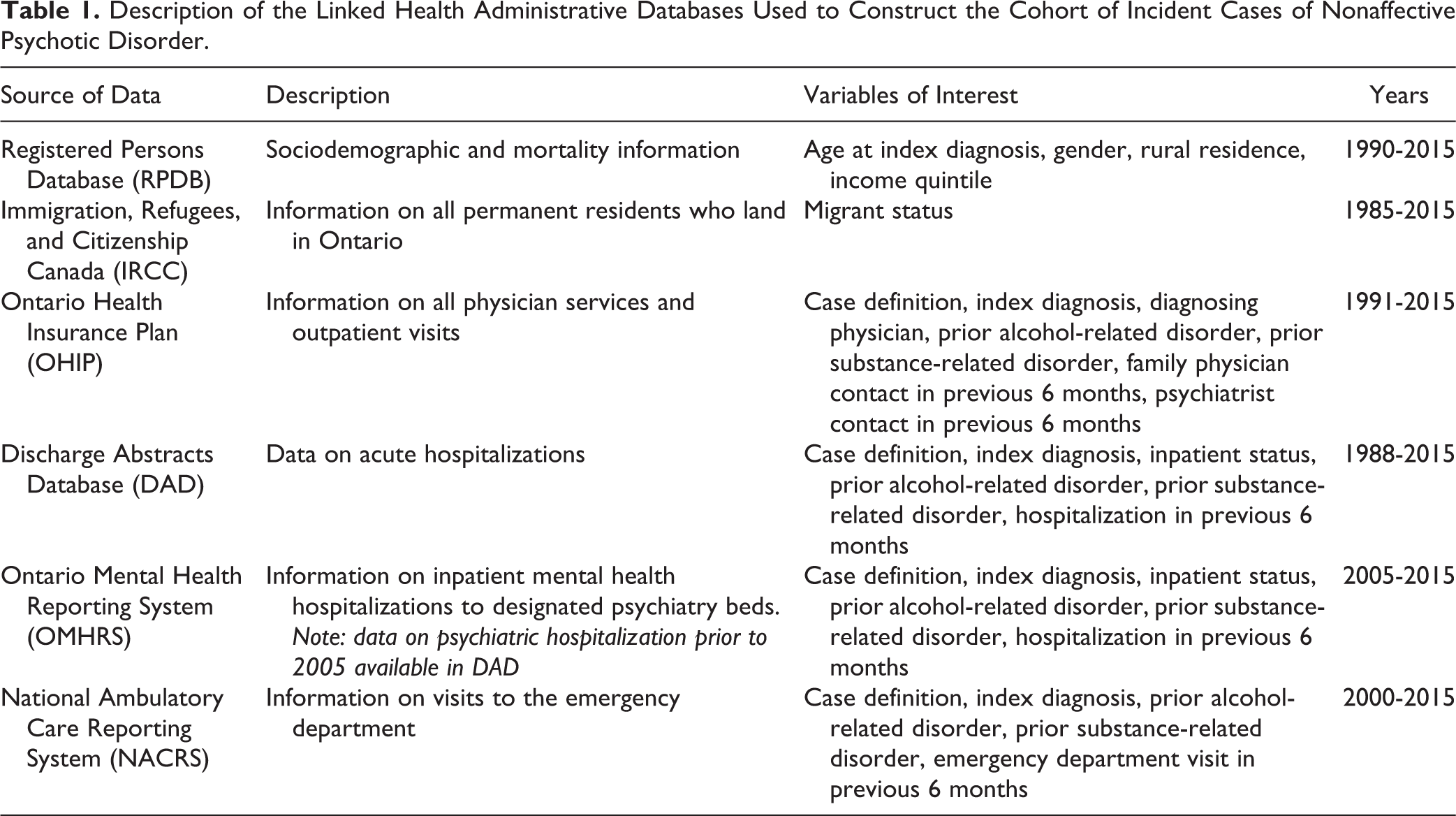
We obtained access to the health administrative data holdings at the Institute for Clinical Evaluative Sciences (ICES), which contains information on all medically necessary services covered by the provincial universal health care system, known as the Ontario Health Insurance Plan (OHIP). These linked databases contain information from physician billings, hospitalizations, and ED visits and include nearly the entire population of Ontario—of exception, we will have missed very recent (<3 months) migrants who are not yet covered by OHIP, as well as students attending postsecondary school from out of province. A description of the databases used in the current study is presented in Table 1.
Description of the Linked Health Administrative Databases Used to Construct the Cohort of Incident Cases of Nonaffective Psychotic Disorder.
Cohort Creation
Using ICES data, we created a retrospective cohort of cases of mood and anxiety disorders among emerging adults who presented to services between 2009 and 2014 in the FEMAP catchment area, identified by the 6-digit postal code of the service provider. We mirrored the inclusion criteria of the FEMAP program to the extent possible in the health administrative data. Cases were defined as emerging adults between the ages of 16 and 25 years who had at least 2 physician billing claims or ED visits with a diagnostic code for a mood or anxiety disorder in any 12-month period or an inpatient hospitalization with a primary discharge diagnosis of a mood or anxiety disorder (codes presented in Suppl. Table S1). People with a history of a nonaffective psychotic disorder were excluded. Although this algorithm has not been validated in the ICES databases, it has demonstrated a high positive predictive value (>90%) in other health administrative data sets. 20
We linked this cohort to primary data from FEMAP, thereby identifying emerging adults treated by this program. We used a deterministic linkage based on the encrypted OHIP numbers of all patients treated at FEMAP, and the data were subsequently encrypted to protect privacy as per ICES data linkage protocols. Emerging adults within the cohort who were also in the FEMAP data were classified as FEMAP users, and all remaining cohort members were classified as nonusers. A small number of people in the FEMAP database were not captured by our cohort definition (8.5%) due to the requirement for 2 outpatient diagnoses—we considered the presence of a FEMAP diagnosis to supersede the requirement for 2 physician billings for mood or anxiety disorders and included these people in the FEMAP users group to preserve the sample.
The Health Sciences Research Ethics Board at the University of Western Ontario approved the linkage of the primary data to the ICES data holdings. Patient-level data were linked using unique coded identifiers, and the deidentified data sets were analyzed on site at ICES. We followed the RECORD guidelines for observational studies using routinely collected data (Suppl. Table S2), and a description of codes and algorithms used to create the variables is presented in Suppl. Table S1.
Sociodemographic, Clinical, and Service Use Variables
The date of the first diagnosis of mood or anxiety disorder within our study window was set as the index date. We extracted information on sociodemographic, clinical, and service use characteristics for all emerging adults in our cohort from the ICES data holdings. Available sociodemographic variables include age at index diagnosis, gender, migrant status, neighbourhood-level income quintile derived from census data, rural place of residence, and whether the primary place of residence was outside the program catchment area. We also extracted information on several clinical factors, including type of index diagnosis (mood vs. anxiety), source of index diagnosis (inpatient, psychiatrist, other MD), and whether there was evidence of prior contact with services for an alcohol- or substance-related disorder. Binary indicators of mental health service use in the 6-month period preceding the index diagnosis were also constructed, including record of any family physician visit, outpatient psychiatrist visit, ED visit, self-harm attempt, or psychiatric hospitalization. There were minimal missing data (<1%) for covariates of interest, and people with missing data were excluded.
Propensity Score Matching
Process and outcome measures (described below) were compared between FEMAP users and a propensity score–matched comparison group of nonusers. A propensity score uses logistic regression to model the probability that an individual is ‘exposed’ (i.e., FEMAP user/nonuser), conditional on observed covariates. 21 Matching on the propensity score functions to achieve balance between groups on the variables included in the propensity score model 21 but does not achieve balance on unmeasured confounding factors as in a randomized trial.
We computed a propensity score for each person in the study cohort—the model included baseline covariates representing sociodemographic characteristics, clinical factors, and indicators of prior mental health service use at the index date (Suppl. Table S2), and it did not include any data from the follow-up period. We used a greedy matching technique without replacement to match FEMAP users to nonusers based on year of index diagnosis and the propensity score (caliper width = 0.02 standard deviance of the propensity score). 22 We also hard-matched on the source of index diagnosis and residence outside the program catchment area, as these variables were not well balanced on initial matching attempts. The matching was done with a variable ratio of up to 1:2, and each nonuser was assigned the same admission date as the FEMAP user in the matched set.
Process and Outcome Measures
Health system process and outcome measures can be used when evaluating health services—process indicators denote the care that was provided, whereas outcome indicators reflect the health status of the patient. 23 We constructed both process and outcome indicators for the 1-year period following FEMAP admission—this observation window was defined by the date of FEMAP admission, and the nonusers assumed the admission date of their matched FEMAP user. The process indicators included contact with a psychiatrist and time to first psychiatric contact, and the outcome indicators included contact with a family physician or ED for mental health reasons, psychiatric hospitalizations, and involuntary admissions. We had also planned to assess indicators of self-harm, suicide, and all-cause mortality but found too few events for these rare outcomes to allow meaningful comparisons, so they were dropped from further analyses. We obtained data on any use of these services as an indicator of access (binary variable), intensity of service use (count variable), and time between FEMAP admission and first encounter with each service.
Statistical Analyses
We compared the baseline characteristics of FEMAP users and nonusers using standardized differences, and values greater than 10% indicated significant between-group differences. 24 We used multivariate logistic regression models to estimate the association between sociodemographic, clinical, and service use factors and odds of admission to FEMAP. For comparison of the process and outcome indicators, we used Cox proportional hazards models with robust variance estimators to account for clustering within matched sets to model indicators of time to access to care (binary), and we used modified Poisson regression to model intensity of service use (counts). Observations were censored at the end of the follow-up period, termination of OHIP eligibility, or death.
Results were consistent across access to care and intensity of service use indicators; therefore, we opted to present results of the access indicators (full results available by request from the authors). All results are presented as odds ratios (ORs) or hazard ratios (HRs) with corresponding 95% confidence intervals (CIs), with the models comparing FEMAP users to a nonuser reference group. All analyses were conducted using SAS Enterprise Guide Version 7.12 (SAS Institute, Cary, NC).
Results
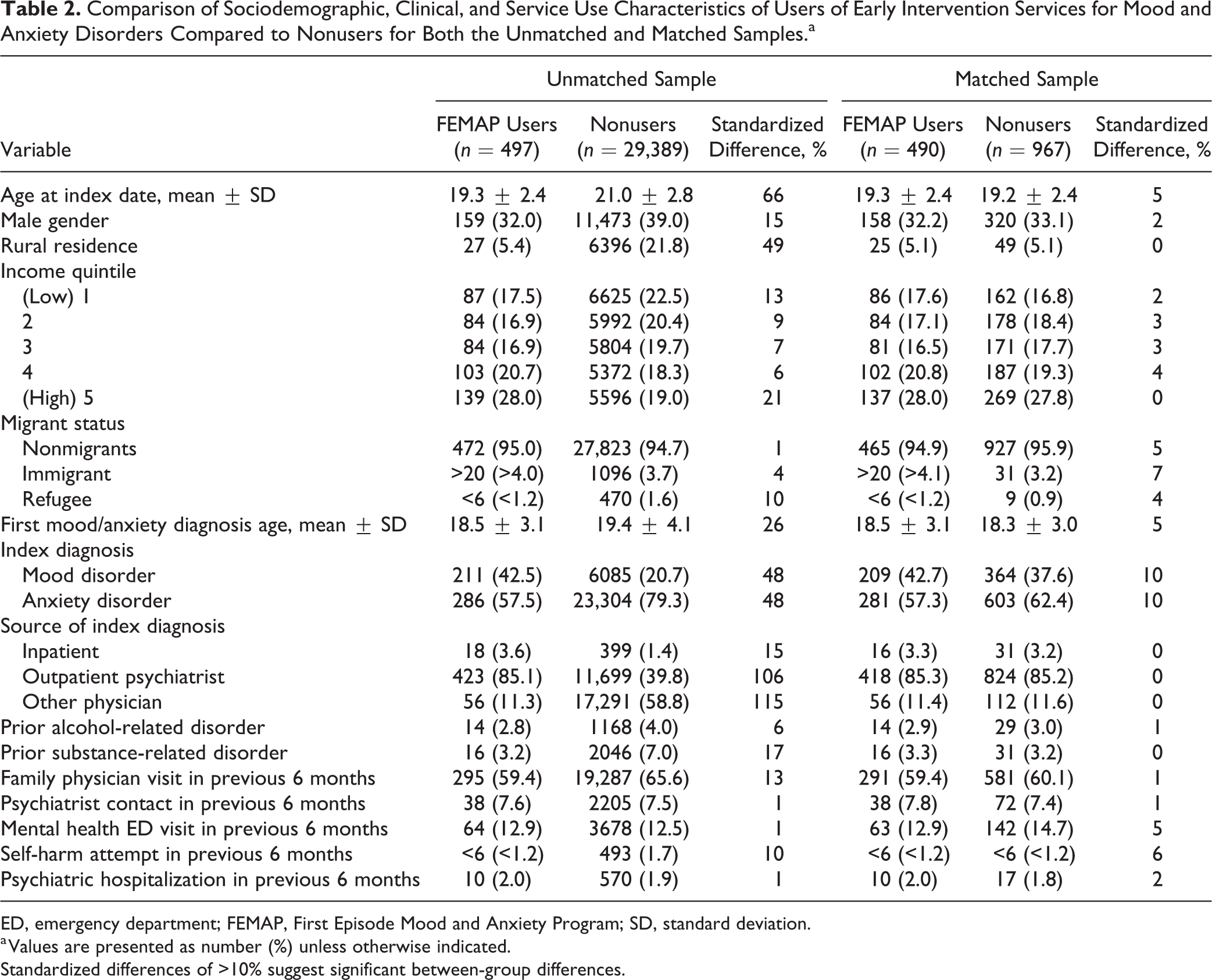
Over the 5-year period between 2009 and 2014, nearly 30,000 emerging adults had contact with mental health services for mood or anxiety disorders in the FEMAP catchment area, representing a treated prevalence of approximately 4%. Of those, 554 were treated by FEMAP, and we linked 89.7% (n = 497) of FEMAP users to health administrative data. The characteristics of the study sample are presented in Table 2, and results of the multivariate logistic regression analysis are presented in Table 3.
Comparison of Sociodemographic, Clinical, and Service Use Characteristics of Users of Early Intervention Services for Mood and Anxiety Disorders Compared to Nonusers for Both the Unmatched and Matched Samples.a
ED, emergency department; FEMAP, First Episode Mood and Anxiety Program; SD, standard deviation.
a Values are presented as number (%) unless otherwise indicated.
Standardized differences of >10% suggest significant between-group differences.
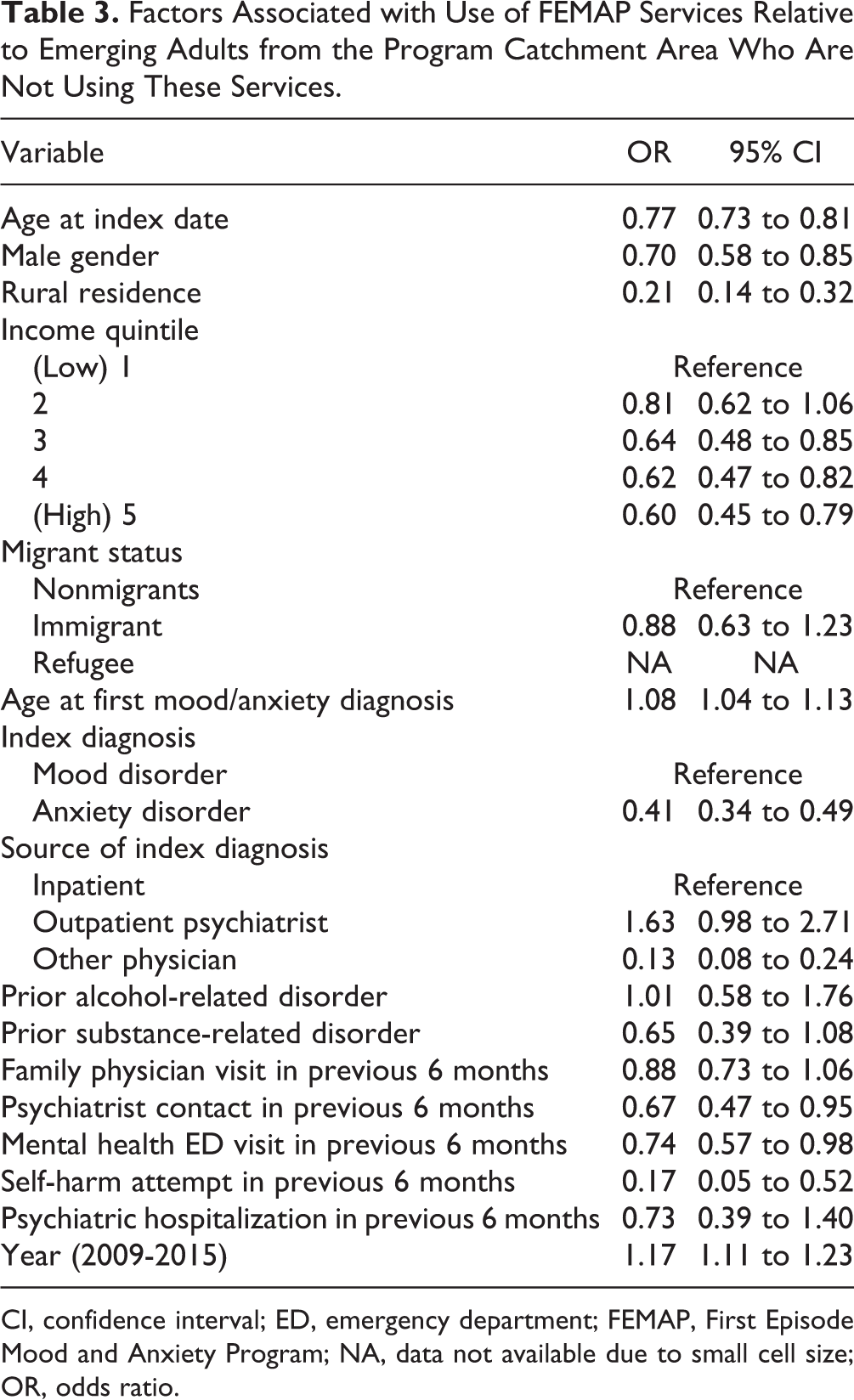
Factors Associated with Use of FEMAP Services Relative to Emerging Adults from the Program Catchment Area Who Are Not Using These Services.
CI, confidence interval; ED, emergency department; FEMAP, First Episode Mood and Anxiety Program; NA, data not available due to small cell size; OR, odds ratio.
Access to FEMAP Services—Unmatched Sample
We found that FEMAP users were significantly younger (OR, 0.77; 95% CI, 0.73 to 0.81), less likely to be male (OR, 0.70; 95% CI, 0.58 to 0.85), and less likely to live in rural areas (OR, 0.21; 95% CI, 0.14 to 0.32) compared with other emerging adults with mood and anxiety disorders in our study cohort. We also found differences by neighbourhood-level income quintile, with emerging adults living in the most deprived areas less likely to be a FEMAP user compared to those living in the least deprived areas (OR, 0.60; 95% CI, 0.45 to 0.79). We did not observe differences in access for first-generation migrant groups, although the proportion of migrants in the sample was small (5.3% of total sample).
FEMAP users were much less likely to have a diagnosis of an anxiety disorder, compared with nonusers (OR, 0.41; 95% CI, 0.34 to 0.49). FEMAP users were more likely to receive the first diagnosis from a psychiatrist (OR, 1.63; 95% CI, 0.98 to 2.71) and less likely to be diagnosed by other types of physicians (OR, 0.13; 95% CI, 0.08 to 0.24), relative to nonusers. We did not observe a significant difference between FEMAP users and nonusers on prior diagnosis of alcohol- and substance-related disorders in our multivariate models.
Contact with a family physician for mental health reasons in the 6-month period prior to their first diagnosis of mood or anxiety disorder did not differ between FEMAP users and nonusers (OR, 0.88; 95% CI, 0.73 to 1.06). FEMAP users were significantly less likely to have had prior help-seeking contacts with a psychiatrist (OR, 0.67; 95% CI, 0.47 to 0.95), with the ED for other mental health reasons (OR, 0.74; 95% CI, 0.57 to 0.98), or for self-harm (OR, 0.17; 95% CI, 0.05 to 0.52). Few people in our sample had prior psychiatric hospitalizations, and this did not differ between FEMAP users and nonusers.
Impact of FEMAP Services—Matched Sample
Seven FEMAP users were dropped from this portion of the analysis due to an inability to find a suitable control, for a final matched sample of 490 FEMAP users and 967 controls. The groups were well balanced in sociodemographic, clinical, and prior service use factors (Table 2).
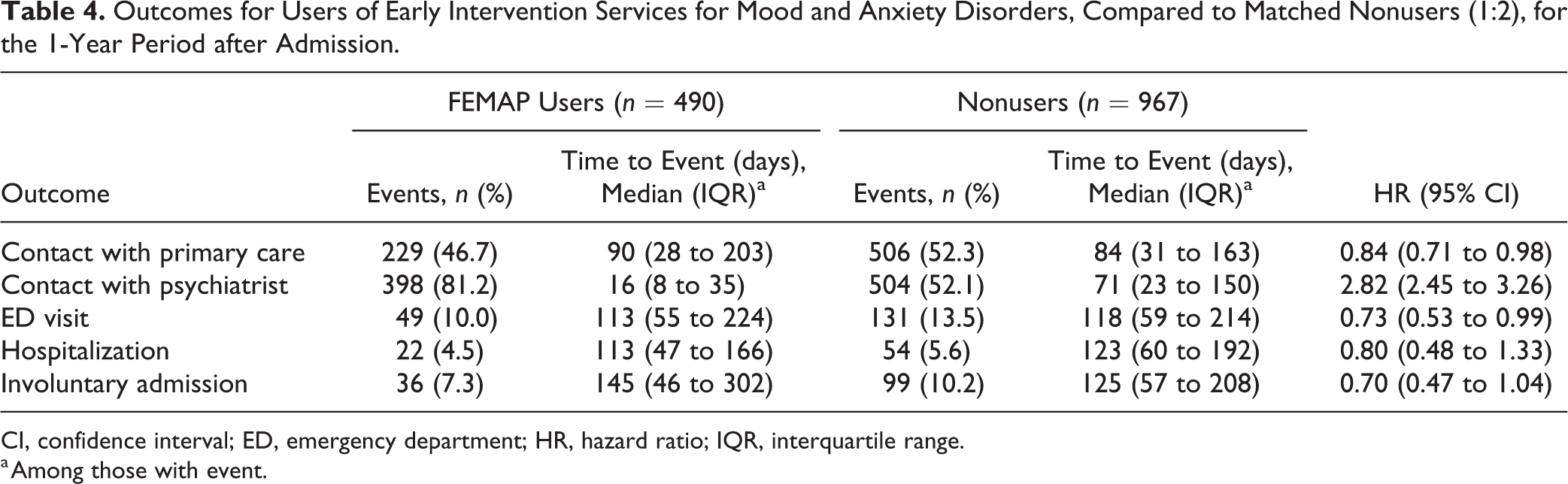
The results of the proportional hazards model comparing process and outcome indicators between FEMAP users and nonusers are presented in Table 4. FEMAP users were nearly 3 times more likely to see a psychiatrist (HR, 2.82; 95% CI, 2.45-3.26), with more rapid access to a psychiatrist (median, 16 days vs. 71 days). They were also less likely to access primary care for mental health reasons (HR, 0.84; 95% CI, 0.71 to 0.98) and had lower use of the ED for mental health reasons (HR, 0.73; 95% CI, 0.53 to 0.99). We did not find a difference in psychiatric hospitalizations between groups (HR, 0.80; 95% CI, 0.48 to 1.33), but the overall event rate was low (FEMAP users = 4.5%, nonusers = 5.6%). There was some evidence that FEMAP users may have lower rates of involuntary admissions (HR, 0.71; 95% CI, 0.47 to 1.04), but larger samples are needed to confirm this.
Outcomes for Users of Early Intervention Services for Mood and Anxiety Disorders, Compared to Matched Nonusers (1:2), for the 1-Year Period after Admission.
CI, confidence interval; ED, emergency department; HR, hazard ratio; IQR, interquartile range.
a Among those with event.
Discussion
Our analysis of health administrative data suggests that adoption of an early intervention model of service delivery aimed at emerging adults with mood and anxiety disorders may have an impact at a health system level—specifically, more rapid access to a psychiatrist and reduced number of mental health–related ED visits. These findings are consistent with the FEMAP logic model, which identifies direct access to mental health services and lower use of emergency services for psychiatric care as short-term outcomes. 19 The FEMAP logic model identifies reduced use of inpatient hospitalizations as a long-term program outcome, 19 which we did not find in the current study; however, our sample size and follow-up period may have been insufficient for detecting a difference. These findings suggest that further research on the effectiveness of this model of care for the treatment of mood and anxiety disorder among emerging adults is warranted.
Our findings suggest that FEMAP users relied less on primary care services for mental health needs, with greater use of specialized psychiatric services. Importantly, clinical data from FEMAP confirm that this is an appropriate use of specialized care, as FEMAP users are a population in urgent need of specialized services. Previous reports showed that nearly three-quarters of patients had received some form of mental health care prior to FEMAP, and symptom levels remained moderate to severe despite this. 18 In addition, over 50% of FEMAP patients were found to be at moderate to high risk of a substance use problem, 25 and over two-thirds endorsed suicidal ideation, with 15% of those expressing serious intent. 18 FEMAP patients reported missing an average of 2.6 days per week of work or school and being underproductive an average of 4.2 days per week. 18 Data from FEMAP also showed that emerging adults treated by the program showed reductions in mood and anxiety symptoms, improved levels of functioning, and high levels of patient satisfaction at both short- and intermediate-term follow-up. 25,26
Although it is unlikely that all emerging adults identified in our study cohort were in need of the specialized care provided by FEMAP, the program treated less than 2% of identified cases over the study time period. Furthermore, it has been estimated that up to half of emerging adults with mental disorders do not seek help for their symptoms 27 and therefore will not have been captured in our study cohort, suggesting a huge amount of potential unmet need in this population. Research from other jurisdictions suggests that emerging adults with depressive symptoms who do not access mental health services at age 14 are over 7 times more likely to have a depressive disorder at age 17, relative to emerging adults who did access services. 27 FEMAP is currently functioning at full capacity, with growing demand for its services and increasingly lengthy wait times. 19 To meet the needs of the population, we need to expand access to youth-friendly treatment options for people with mood and anxiety disorders, and consequences for the social, educational, and career trajectories could be dire should the status quo persist.
Importantly, we demonstrated that FEMAP services provide access to mental health care in more appropriate settings by diverting emerging adults with mental health needs from the ED, a finding that has also been demonstrated for early intervention services for psychosis. 4 This is particularly important given that mental health–related ED visits among emerging adults have increased in North America. 28 –30 In Ontario, this increase has occurred at more than double the rate of corresponding increases in outpatient mental health visits, with anxiety disorders being the most common reason for ED presentations. 28 Furthermore, research suggests that more than half of emerging adults who present to the ED for mental health reasons have not previously sought mental health care from outpatient providers, 31 suggesting that early intervention models that provide timely access to mental health services could reduce inappropriate use of the ED.
Strengths and Limitations
These findings demonstrate the health system potential of a novel treatment program aimed at emerging adults with mood and anxiety disorders—to our knowledge, this is the first evaluation of an early intervention model of care for these disorders. Data were linked to a population-based health administrative database including multiple service providers that allowed for a comprehensive examination of the impact of FEMAP services on important health system indicators. We used propensity score matching to select a comparison group with a similar distribution of confounding factors. Finally, we used concurrent controls matched on year of first diagnosis to ensure equivalent temporal and contextual factors between groups. 32
It is important to note the inherent limitations associated with the observational study design that we employed. Although propensity score methods attempt to mimic some of the characteristics of a randomized trial, 21 we are only able to achieve balance on the confounding factors included in the propensity score model, unlike a randomized trial that also balances unmeasured confounding factors. In addition, these methods allow for the estimation of the average treatment effect among the treated, that is, people who have a similar probability of admission to FEMAP services. 21 Given that there were significant differences between FEMAP users and nonusers prior to matching, we are not able to infer the effect of an early intervention model of care on emerging adults who have a low probability of encountering these services. Randomized trials using standardized diagnoses and clinically relevant outcome measures are needed to fully evaluate the effectiveness of an early intervention model of care for mood and anxiety disorders.
In addition, our data do not contain information on emerging adults with mood and anxiety disorders who were not presenting to the public health care system and may instead have received assessment and treatment from private psychologists, social workers, or other community mental health care providers not covered by OHIP. However, if we assume that this would occur more frequently in the nonusers group, it would function to underestimate the impact of FEMAP. Furthermore, we included a small proportion of cases (8.5%) in the FEMAP group who were not captured by our algorithm for defining the larger cohort. Although this was done to maximize the available data on FEMAP users, it may have introduced bias if these emerging adults differed in some distinct way from the larger cohort. However, we believe the potential impact of this bias on our findings is mitigated by the propensity score matching procedure that we used, combined with hard matching on the source of index diagnosis (outpatient psychiatrist), and should therefore have only a minimal impact on our findings.
Finally, we are limited by the availability of information in the health administrative data holdings, and our findings may be due to residual confounding by factors that we did not have data for, such as severity of illness. On one hand, our algorithm may have identified mild or self-remitting cases of mood and anxiety disorder that would not require more specialized treatment, which would result in nonusers having a less severe illness profile. On the other hand, we do not know how many emerging adults in our nonusers group would be eligible for admission to FEMAP—we attempted to mirror the program criterion as closely as possible but were unable to assess factors such as duration of prior medication use and contact with the criminal justice system, and our data on alcohol and substance use were restricted to diagnosed disorders. This could result in FEMAP users having a less severe illness profile. We have attempted to mitigate the impact of these potential differences by including sociodemographic, clinical, and service use factors in our propensity score model, and the groups were well balanced on all available indicators.
Conclusions
Mood and anxiety disorders are highly prevalent among emerging adults and represent a significant public health burden that calls for an increased focus on the early detection and intervention among emerging adults experiencing them. Our findings suggest that adopting an early intervention model of care for mood and anxiety disorders may lead to more rapid access to effective psychiatric services and diversion of mental health–related help seeking from the ED. Further research on the effectiveness of this model of care is warranted.
Supplementary Materials
Supplemental Material, DS_10.11770706743718809347 - Access and Health System Impact of an Early Intervention Treatment Program for Emerging Adults with Mood and Anxiety Disorders
Supplemental Material, DS_10.11770706743718809347 for Access and Health System Impact of an Early Intervention Treatment Program for Emerging Adults with Mood and Anxiety Disorders by Kelly K. Anderson, Ava John-Baptiste, Arlene G. MacDougall, Lihua Li, Paul Kurdyak and Elizabeth A. Osuch in The Canadian Journal of Psychiatry
Supplementary Materials
Supplemental Material, Online_Supplement_#1 - Access and Health System Impact of an Early Intervention Treatment Program for Emerging Adults with Mood and Anxiety Disorders
Supplemental Material, Online_Supplement_#1 for Access and Health System Impact of an Early Intervention Treatment Program for Emerging Adults with Mood and Anxiety Disorders by Kelly K. Anderson, Ava John-Baptiste, Arlene G. MacDougall, Lihua Li, Paul Kurdyak and Elizabeth A. Osuch in The Canadian Journal of Psychiatry
Supplementary Materials
Supplemental Material, Online_Supplement_#2 - Access and Health System Impact of an Early Intervention Treatment Program for Emerging Adults with Mood and Anxiety Disorders
Supplemental Material, Online_Supplement_#2 for Access and Health System Impact of an Early Intervention Treatment Program for Emerging Adults with Mood and Anxiety Disorders by Kelly K. Anderson, Ava John-Baptiste, Arlene G. MacDougall, Lihua Li, Paul Kurdyak and Elizabeth A. Osuch in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
The authors gratefully acknowledge the contributions of Dr. Salimah Shariff to the cohort creation and analysis plan. The opinions, results, and conclusions reported in this article are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario Ministry of Health and Long-Term Care (MOHLTC) is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are those of the author and not necessarily those of CIHI.
Data Access
This study was conducted at the ICES, which is funded by an annual grant from the Ontario MOHLTC. The data set from this study is held securely in coded form at the ICES, and the ICES analyst (L.L.) had full access to study data. While data-sharing agreements prohibit the ICES from making the data set publicly available, access can be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full data set creation plan is available from the authors upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
KKA is supported by a New Investigator Fellowship from the Ontario Mental Health Association. This study was funded by the Lawson Health Research Institute and the Department of Psychiatry at The University of Western Ontario.
Supplementary Materials
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.