
Abstract
Background:
Evidence whether individuals with attention-deficit hyperactivity disorder (ADHD) are at increased risk for traffic violations/collisions is mixed. This study investigated the association between ADHD and traffic violations among youth and young adults; examined whether this association differed by age, sex, or comorbid mental or physical problems; and modelled factors associated with traffic violations among individuals with ADHD.
Methods:
Data come from the 2012 Canadian Community Health Survey–Mental Health (CCHS-MH), a cross-sectional epidemiological study. The sample was restricted to youth and young adults aged 15 to 39 years and categorized into 3 groups: 15 to 19 years (n = 1886), 20 to 29 years (n = 3679), and 30 to 39 years (n = 3659). Lifetime ADHD and past-year contact with police for traffic violations were self-reported. Logistic regression models quantified the association between ADHD and traffic violations, stratified by age. Interactions were included to examine moderating effects.
Results:
No evidence suggested an association between ADHD and past-year traffic violations (odds ratio [OR], 1.07; 95% confidence interval (CI), 0.64 to 1.79), age-specific estimates did not differ across age groups (P = 0.696), and no factors moderated the association. Three factors were found to increase odds for past-year traffic violations among individuals with ADHD: aged 20 to 29 years (OR, 3.84; 95% CI, 1.47 to 10.06), male sex (OR, 3.48; 95% CI, 1.39 to 8.59), and white ethnicity (OR, 5.62; 95% CI, 1.24 to 25.51).
Conclusions:
Individuals with ADHD are not an at-risk group for traffic violations but instead share similar risk factors with individuals in the general population without ADHD—information useful for health professionals. Replication studies are needed to examine the robustness of these findings.
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder commonly diagnosed in childhood 1 but has lifelong consequences. 2 Core features of ADHD—inattention and impulsivity—may predispose individuals to engage in risky behaviour, including unsafe driving practices. 3 Understanding whether ADHD is associated with driving behaviours is relevant given that motor vehicle accidents are a leading cause of mortality throughout life, especially among young people. 4
A meta-analysis found that individuals with ADHD have a 36% increased risk for traffic accidents compared to individuals without ADHD. 5 Researchers have noted that many studies have methodological limitations that blur our understanding of this relationship 5 –8 : small, selective, clinical samples that may bias toward larger effects; focus on specific developmental periods (e.g., adolescence) that ignore sex or age effects; informant reports with long recall periods that result in underreporting; lack of adjustment of confounding factors; experimental designs using driving simulators that do not effectively approximate real-world driving; and studies conducted prior to widespread implementation of graduated licensing systems. Since publication of the meta-analysis, 5 studies addressing some of these limitations have produced findings of higher 6,9,10 or similar 11,12 risk of traffic accidents/violations or unsafe driving behaviour among individuals with ADHD.
No national Canadian study of young people examining ADHD and traffic violations has been conducted. One study of adults ≥18 years in Ontario found that a previous diagnosis of ADHD was not associated with reporting a past-year traffic collision (odds ratio [OR], 1.15; 95% confidence interval (CI), 0.41 to 2.70). 13 Instead, a current positive screen for ADHD was significantly associated with a past-year collision (OR, 2.37; 95% CI, 1.37 to 4.32). This association was attenuated when adjusting for characteristics related to demographics, other psychopathology, and substance use (OR, 0.78; 95% CI, 0.37 to 2.11).
Using data from the Canadian Community Health Survey–Mental Health to overcome the limitations of previous research, this study 1) investigated the association between ADHD and traffic violations among youth and young adults; 2) examined the extent to which age, sex, or comorbid mental (mood disorder or substance use disorder) or physical conditions moderate this association; and 3) modelled factors associated with traffic violations among individuals with ADHD to identify high-risk subgroups.
Methods
Data come from the Canadian Community Health Survey–Mental Health (CCHS-MH), a national study conducted by Statistics Canada to collect information about the prevalence of mental disorder, functional status, and use of health services in a representative sample of respondents ≥15 years (N = 25,113). 14 The study sample was restricted to youth and young adults aged 15 to 39 years (n = 9224), categorized into 3 groups: 15 to 19 years (n = 1886), 20 to 29 years (n = 3679), and 30 to 39 years (n = 3659).
ADHD was self-reported. Interviewers informed participants about the following: “We are interested in ‘long-term conditions’ which are expected to last or have already lasted six months or more and that have been diagnosed by a health professional. Do you have attention deficit disorder?” In total, 415 (4.5%) endorsed having ADHD.
Past-year traffic violations were measured in a module examining contact with police. Participants were asked, “During the past 12 months, did you come into contact with the police for a traffic violation?” In total, 1379 (15.0%) endorsed having police contact for a traffic violation (e.g., collisions, driving under the influence of alcohol, speeding).
Sociodemographic and health-related characteristics were included to control for confounding. 5,6,13 These included ethnicity (white/nonwhite), province of residence, residing in a census metropolitan area (yes/no), provincial income decile, number of chronic conditions, using medication for mental health/addiction in the past year, and presence of past-year mood (major depressive, generalized anxiety, or bipolar disorder) or substance use disorder (alcohol/illicit drug) measured using the World Health Organization (WHO) Composite International Diagnostic Interview. 15
ORs were computed from logistic regression models, stratified by age. Product-term interactions were included to examine the moderating effects of age, sex, mood/substance use disorder, or chronic conditions. Analyses were weighted.
Results
The sex distribution of the sample was equal (50.7% male). Most participants lived in urban areas (76.2%), 30.9% identified as nonwhite, and 42.9% had ≥1 chronic condition. Mood and substance use disorder were reported by 7.2% and 7.6% of the sample, respectively. Eight percent had taken medications for mental health/addiction in the past year.
Participants aged 15 to 19 years (6.2%) or 20 to 29 years (5.2%) were more likely to report ADHD compared to those aged 30 to 39 years (3.0%). The proportion of traffic violations was lower in participants aged 15 to 19 years with ADHD compared the group of 20- to 29-year-olds (8.4% vs. 25.8%; P < 0.001). Among those without ADHD, traffic violations were also lower in the 15- to 19-year-old group (8.8%) compared to the group of 20- to 29-year-olds (17.4%) and 30- to 39-year-olds (15.3%; P < 0.001 for both). There was no association between ADHD and past-year traffic violations (OR, 1.07; 95% CI, 0.64 to 1.79; Table 1).
Associations between ADHD and Contact with Police for Traffic Violations.a
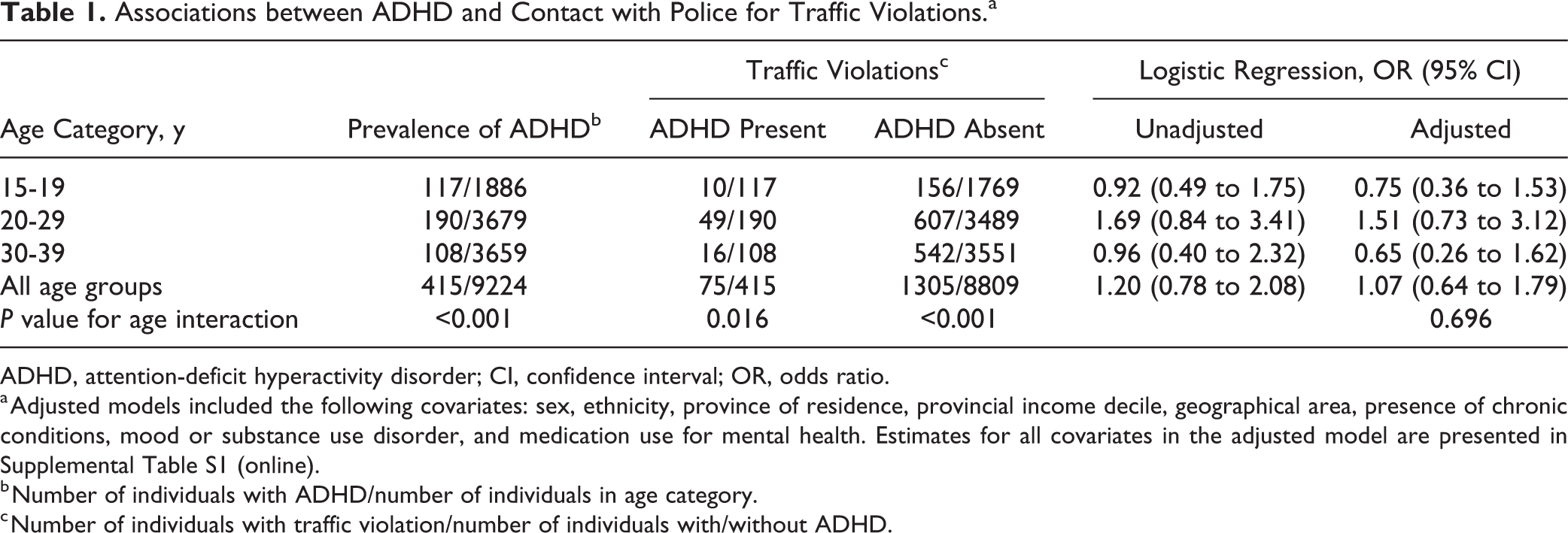
ADHD, attention-deficit hyperactivity disorder; CI, confidence interval; OR, odds ratio.
a Adjusted models included the following covariates: sex, ethnicity, province of residence, provincial income decile, geographical area, presence of chronic conditions, mood or substance use disorder, and medication use for mental health. Estimates for all covariates in the adjusted model are presented in Supplemental Table S1 (online).
b Number of individuals with ADHD/number of individuals in age category.
c Number of individuals with traffic violation/number of individuals with/without ADHD.
In the presence of each moderator, individuals with ADHD typically had lower odds of reporting past-year traffic violations (OR range, 0.54 to 1.11), whereas in the absence of the moderator, odds were higher compared to those without ADHD (OR range, 1.03 to 1.24; Table 2). None of these associations was significant.
Moderating Effects on the Association between ADHD and Traffic Violations across All Age Groups.a
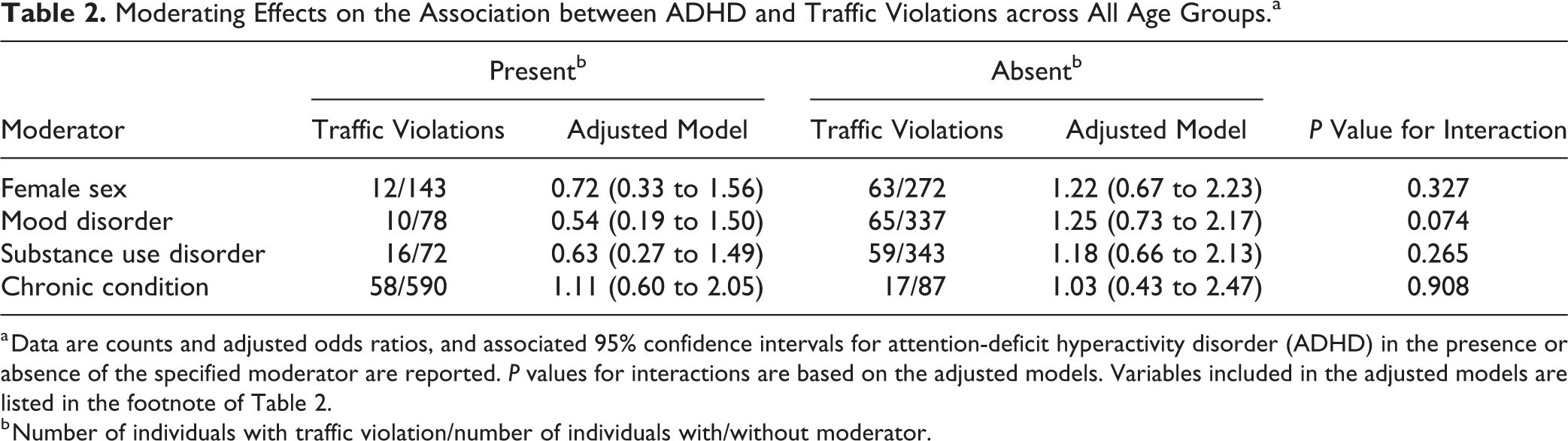
a Data are counts and adjusted odds ratios, and associated 95% confidence intervals for attention-deficit hyperactivity disorder (ADHD) in the presence or absence of the specified moderator are reported. P values for interactions are based on the adjusted models. Variables included in the adjusted models are listed in the footnote of Table 2.
b Number of individuals with traffic violation/number of individuals with/without moderator.
Three factors were found to increase odds for past-year traffic violations among individuals with ADHD (Table 3): aged 20 to 29 years (OR, 3.84; 95% CI, 1.47 to 10.06), male (OR, 3.48; 95% CI, 1.39 to 8.59), and white (OR, 5.62; 95% CI, 1.24 to 25.51).
Risk Factors for Traffic Violations among Individuals with ADHD.a
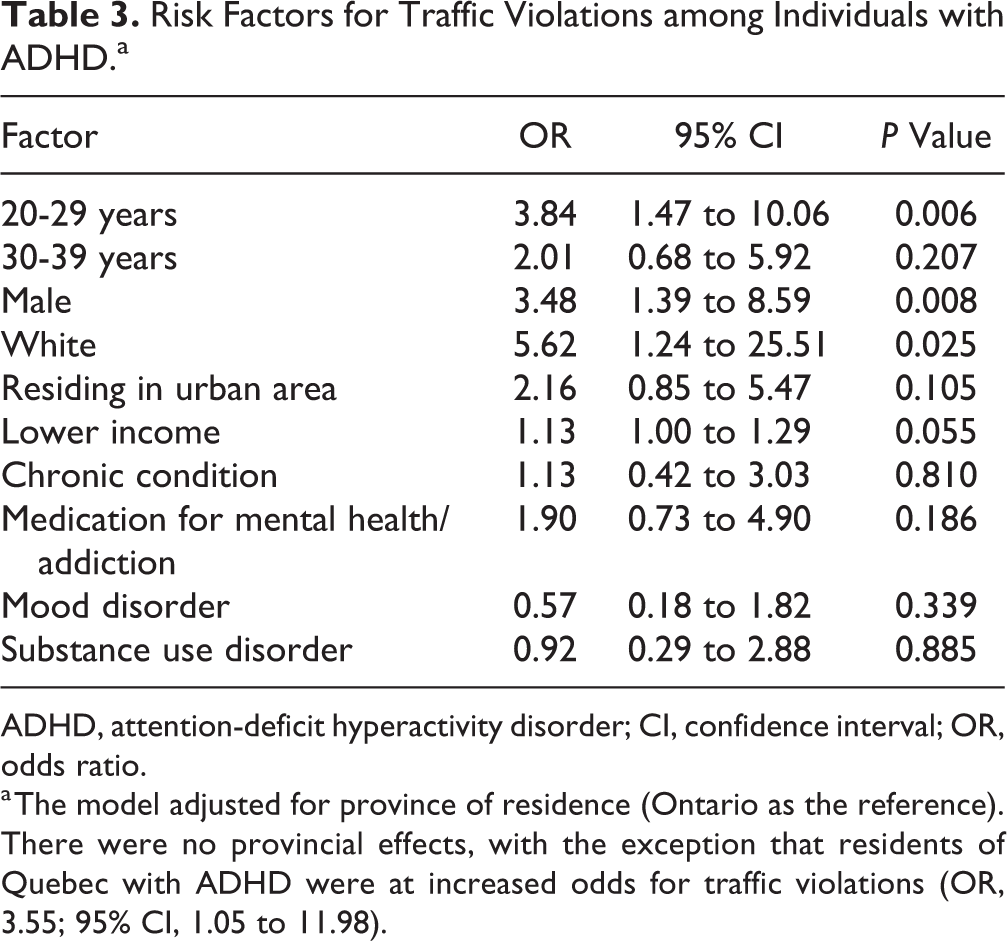
ADHD, attention-deficit hyperactivity disorder; CI, confidence interval; OR, odds ratio.
a The model adjusted for province of residence (Ontario as the reference). There were no provincial effects, with the exception that residents of Quebec with ADHD were at increased odds for traffic violations (OR, 3.55; 95% CI, 1.05 to 11.98).
Discussion
In this national study, ADHD was not associated with contact with police for past-year traffic violations. This finding did not differ across demographic or health characteristics. Among individuals with ADHD, those who were male, aged 20 to 29 years, and white were at increased odds for reporting violations, similar to findings from the general population. 16
Findings contrast with other epidemiological studies from the United States and France, which suggested increased risk for traffic collisions among individuals with ADHD. 6,9,10 Whilst many methodological limitations have been addressed, 2 of those studies did not adjust for confounding factors related to disruptive behaviours, including oppositional defiant/conduct disorder or substance use. 9,10 Instead, findings were comparable to a New Zealand study that examined mean number of police contacts for driving violations during the past 3 years among 21-year-olds. 17 That study found no difference in police contacts among individuals who had more attention difficulties at age 13. Our findings also agreed with the previous Canadian study that showed that neither previous diagnosis of ADHD nor current positive screen for ADHD was associated with having a collision. 13 As suggested previously, 5 much of the literature supporting negative driving outcomes for individuals with ADHD may be biased—a function of selective sampling, study design, and inadequate control of error.
Echoing issues raised previously, 13 our findings do not suggest that health professionals should not be concerned about driving outcomes for individuals with ADHD. There is evidence of interventions that can improve driving performance of youth with ADHD. 18,19 In addition to dialogues regarding driving safety, health professionals can offer these interventions broadly and end stigma—perpetuated, in part, to the findings from early studies—associated with ADHD and its influence on driving. In fact, individuals with ADHD are not different from individuals with depression with regards to driving outcomes, including traffic violations, collisions, and injury from collisions. 10 Similarly, meta-analytic evidence shows that individuals with comorbid ADHD and disruptive behaviour problems have an 86% increase in risk for traffic accidents—a 1.4-fold increase compared to ADHD alone. 5 Thus, reported associations between ADHD and driving outcomes may be attributed to the subgroup of individuals with such comorbidities.
Findings must be interpreted in the following context: First, the cross-sectional nature of the CCHS-MH prevents any inferences regarding causality. Second, ADHD and traffic violations were self-reported, single-item questions, which may be influenced by social desirability bias. Third, recall bias is possible given that core symptoms of ADHD relate to inattentiveness, forgetfulness, and difficulty with concentration. 20 Fourth, the CCHS-MH did not collect information on whether participants had a valid driver’s license, driving experience, or violations that did not result in police contact; were the driver during the violation; or, in the case of a collision, were at fault. Individuals with ADHD are less likely to have a driver’s license, which may reduce their probability of having a traffic violation. 6 However, individuals with ADHD are also more likely to engage in risky behaviour and drive more kilometres, which may increase their probability of a violation. 3,5 The extent to which the absence of these data influenced reported associations is unknown. Fifth, we were unable to adjust for disruptive behaviour but instead used presence of substance use disorder. Sixth, in most Canadian provinces, individuals must be ≥16 years of age to obtain a driver’s license. Because the CCHS-MH aggregated participants’ ages, we could not restrict the sample to those ≥16 years of age; instead, we adjusted for provincial effects.
Conclusions
Findings suggested that individuals—regardless of age, sex, or other mental or physical comorbidity—with ADHD were not at increased odds of reporting contact with police for past-year traffic violations. The complex presentation of ADHD and its high proportion of comorbidity with other mental and substance use disorders 20 warrants further study, ideally with representative samples and standardized, objective measures of driving outcomes to contribute methodologically robust information to the knowledge base, particularly within the Canadian context.
Supplemental Material
Supplemental Material, DS_10.1177_0706743718809340 - Traffic Violations among Young People with Attention-Deficit Hyperactivity Disorder
Supplemental Material, DS_10.1177_0706743718809340 for Traffic Violations among Young People with Attention-Deficit Hyperactivity Disorder by Mark A. Ferro and Scott T. Leatherdale in The Canadian Journal of Psychiatry
Footnotes
Data Access
The data used in this study are available to researchers through application to the Canadian Research Data Centre Network.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Although the research and analyses are based on data from Statistics Canada, the opinions expressed do not represent the views of Statistics Canada. Dr. Ferro serves on the editorial board of the Canadian Journal of Psychiatry. Dr. Leatherdale has no conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received no funding. Dr. Ferro holds the Canada Research Chair in Youth Mental Health and is the recipient of an Early Researcher Award from the Ontario Ministry of Research, Innovation and Science. Dr. Leatherdale holds a Canadian Institutes of Health Research and Public Health Agency of Canada Chair in Applied Health Research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.