
Abstract
Objectives:
Daily cannabis use can portend problematic use or dependence. We aimed to identify early risk factors for daily cannabis use in young adults.
Methods:
Data were available in a longitudinal investigation of 1294 grade 7 students age 12 to 13 years at inception recruited in 10 secondary schools in Montreal, Canada, in 1999. Data on daily cannabis use were collected in mailed self-report questionnaires from 878 participants (67.9% of 1294) at age 20. The associations between each of 23 potential risk factors measured in grade 7 and daily cannabis use at age 20 were modeled using logistic regression.
Results:
At age 20, 44% of participants reported past-year cannabis use; 10% reported daily use. Older age; male sex; higher levels of family stress and other stress; use of alcohol, cigarettes, and other tobacco products; parent(s), sibling(s), and friend(s) smoke cigarettes; higher body mass index; higher impulsivity and novelty seeking; and lower self-esteem increased the odds of daily cannabis use.
Conclusions:
Children at risk of daily cannabis use as young adults can be identified early. They may benefit from early intervention to prevent problematic cannabis use.
Cannabis is the most widely used illegal substance in North America. 1 In Canada, 45% of persons age 15 years or older have tried cannabis, 1 34% have used it more than once, 2 and 3% report weekly or more frequent use. 1 While use generally declined in the past decade, Canada has one of the highest prevalence rates of cannabis use among youth worldwide. 3,4 Prevalence rates are highest among 18- to 24-year-olds. In 2015, 54%, 30%, and 6% of 18-to 24-year-olds reported ever, past-year, and daily use, respectively, 1 and these prevalence rates have remained relatively stable over the past decade. 1
Although likely dependent on frequency of use, dose, age of initiation, and psychosocial factors, there is no consensus on a definition of problematic cannabis use. 5 Weekly use has been characterized as hazardous or risky, 5 and daily use is often used to identify youth at risk of problematic use, dependence (25%-50% of daily cannabis users report dependence), 6,7 and other negative health effects. 5,7 –9 Problematic cannabis use purportedly peaks in young adulthood. 10 One in 11 lifetime users (9%) develop a cannabis-related disorder, 7,11 although when onset occurs in adolescence, 1 in 6 users (17%) develop a disorder. 4,7,12
Health problems associated with cannabis use in adults include anxiety, depression, psychotic episodes, and impaired cardiovascular and lung health, 13 –17 and frequent users are more likely to experience these adverse consequences. 2,3,8,9,18 However, because of the sensitivity of the developing brain, persons younger than 25 years may be particularly vulnerable to cannabis-related problems. 4,12,19 Cannabinoid receptors, which increase during brain development, are very sensitive to the toxic effects of cannabinoids from cannabis. 20 Use in youth may cause irreversible functional and structural changes to brain areas involved in verbal learning, memory, and attention. 4,19 Use in youth is also associated with substance use disorders, initiation of and sustained cigarette smoking, poor mental health, impaired neurological development, cognitive decline, poor academic performance and lifetime achievement, and cannabis dependence. 4,9,12,21
Numerous studies report risk factors for cannabis use. In a narrative review, previous cannabis use, friend’s cannabis use, cannabis dependence, sensation seeking, and lower socioeconomic status were associated with cannabis use in young adults transitioning from high school. 22 In a review of 13 longitudinal studies, consistent risk factors included male sex, tobacco and alcohol use, problematic relationships with parents, and friends’ cannabis use. 23 Psychiatric disorders, substance use, and negative social circumstances (e.g., family dysfunction, school expulsion, bullying) were associated with problematic cannabis use in American youth 24 while male sex, earlier age at onset, smoking, heavy drinking, illicit drug use, poor mental health, and low socioeconomic status (SES) were associated cross-sectionally with problematic cannabis use in Canadian youth. 25 Other factors positively associated with cannabis use include body mass index (BMI), 26 parental substance use, 27,28 and peer smoking. 27 Sports participation in adolescence may be protective. 29
However, despite an abundant literature on cannabis, risk factors for daily use are rarely studied longitudinally in population-based samples of youth, and few studies investigate a wide range of risk factors early in life so that the relative importance of each can be assessed. Because age of onset, especially in frequent users, occurs early in adolescence, 1 and because frequency of use underpins problematic use, 5,30 identification of early modifiable risk factors for daily use could inform preventive programs and policy. Early prevention of problematic cannabis use is important generally. However, addressing gaps in knowledge in this realm is particularly important given the current context in which many jurisdictions worldwide are considering legalizing cannabis for recreational use. Our objective was to identify early risk factors for daily cannabis use in young adults.
Methods
Data were drawn from the Nicotine Dependence in Teens (NDIT) study, a longitudinal investigation of grade 7 students recruited in a purposive sample of 10 secondary schools in Montreal, Canada, in 1999-2000. 31 A total of 1294 of 2325 eligible students (56%) participated in the baseline data collection. The relatively low response related in part to a labour dispute in Quebec that resulted in several teachers refusing to collect consent forms and to the need for blood samples for genetic analysis. Self-report questionnaires were administered at school every 3 months from grades 7 to 11, for a total of 20 cycles. Participants were contacted in postsecondary school in 2007-2008 (cycle 21) through email/mail/phone calls, and data were collected from 880 participants (73% of the 1208 participants who remained eligible to participate at age 20) 31 in mailed/emailed self-report questionnaires or in office data collection. Parents/guardians provided written informed consent at inception, and participants (who had attained legal age) provided consent post–high school. The study was approved by the ethics review committees at the Montreal Department of Public Health, McGill University, and the Centre de Recherche du Centre Hospitalier de l’Université de Montréal. Baseline characteristics of NDIT participants resembled those of a provincially representative sample of adolescents age 13 years from the 1999 Quebec Child and Adolescent Health and Social Survey. 31
The current analysis uses data on potential risk factors collected in grade 7 when participants were age 12 to 13 years, as well as on past-year cannabis use 7 to 8 years later in cycle 21 when participants were age 20 years on average. Data on past-year cannabis at age 20 were available for 878 participants.
Potential risk factors investigated were selected as associated with cannabis use based on findings of earlier studies, 7,22 –29 as well as the availability of data on the variable in the NDIT study, and included 6 sociodemographic characteristics (i.e., age, sex, mother university educated, language spoken at home, born in Canada, lives with 1 parent only), 7 psychosocial indicators (i.e., depressive symptoms, 32 family stress, 33,34 other stress, 33,34 impulsivity, 35,36 novelty seeking, 37 self-esteem, 38 worry about weight 33 ), 7 lifestyle indicators (i.e., use of alcohol, tobacco products other than cigarettes, smoked cigarettes, 39 number of bouts of participation in moderate and vigorous physical activity [MVPA] in the past week, 40 participation in team sports, computer hours/week, TV hours/week), 3 indicators pertaining to smoking in the social environment (i.e., parent(s) smokes, sibling(s) smoke, friend(s) smoke), and other (i.e., BMI).
We retained the highest value of the potential risk factor observed in grade 7 (cycles 2-4); the value of the variable in cycle 1 was used as a control variable in the modeling because it preceded the risk factor and therefore could not be on the causal pathway. Data on self-esteem, impulsivity, and novelty seeking were available in later cycles only but, because we considered them to be relatively time invariant, 41 –44 we included them in these analyses. The sections below describe the primary study variables. Appendix 1 (available online) describes each potential risk factor, including the item used in the questionnaire, response options, and recoding of response options for analysis. Appendix 2 (available online) describes the number of missing values for each potential risk factor. Analyses included participants with complete data only.
Study Variables
A frequency of cannabis use variable was created based on lifetime cannabis use and frequency of cannabis use in the past year. Lifetime cannabis use (yes/no) was assessed by asking, “Have you ever used marijuana, cannabis, hashish?” Frequency of past-year cannabis use was measured by the following: “In the past 12 months, how often did you use marijuana, cannabis, hashish?” with response choices including never, less than once a month, 1 to 3 times per month, 1 to 6 times per week, and every day. Participants were categorized into 1 of 5 categories based on these 2 items: never users, ever-users but not in the past year, less than weekly users, weekly users, and daily users. For multivariable analyses, participants were categorized according to whether they had used cannabis daily in the past year (yes, no).
Age at first cannabis use was measured by asking lifetime cannabis users, “How old were you when you (used cannabis) the first time?” “Number of years since initiation of cannabis use” was computed as the difference between current age in cycle 21 and age first used cannabis.
Data Analysis
We used multivariable logistic regression to estimate the association between the 23 potential risk factors and daily cannabis use. Each risk factor was tested in a separate model with its own distinct set of potential confounders identified as variables correlated with the potential risk factor at r ≥ 0.30. This approach has been used previously in the NDIT. 45 –48 The maximum variance inflation factor value in all models was 1.23 (data not shown). Data on potential confounders were drawn from cycle 1 (so that the value did not lie on the causal pathway between the risk factor tested and cannabis use in young adulthood). However, all models adjusted for sex and age regardless of their correlation with the potential risk factor of interest. Thus, each model addressed a specific hypothesis and consisted of an analysis that included only 2 tests (univariate and multivariate) with carefully selected covariates, including variables that had a high probability of being associated with both exposure and outcome. 49
Two sensitivity analyses were undertaken. First, since weekly cannabis use may also increase the risk of cannabis-related problems, 5,18 we identified risk factors for past-year weekly or daily use. Second, 60 participants (19/60 were daily cannabis users at age 20 years) indicated that they had initiated cannabis use before age 13 years such that it was unclear if onset preceded the exposure. To ensure that values of potential risk factors preceded cannabis initiation, we excluded these participants and reran the multivariate models (n = 818).
Analyses were conducted using SPSS, version 21.0 (SPSS, Inc., an IBM Company, Chicago, IL).
Results
Table 1 compares baseline characteristics of 878 participants with data on past-year cannabis use at age 20 with those of the 416 participants without cannabis use data (i.e., participants lost to follow-up or missing data). Participants with cannabis use data were younger on average than those without cannabis use data, higher proportions had university-educated mothers and were born in Canada, and lower proportions were male, smoked cigarettes, and reported alcohol use. There were no differences between groups in language, use of other tobacco products, or depressive symptoms.
Selected Characteristics of Participants with and without Data on Past-Year Cannabis Use in 2007-2008, Nicotine Dependence in Teens Study, 1999-2008.a
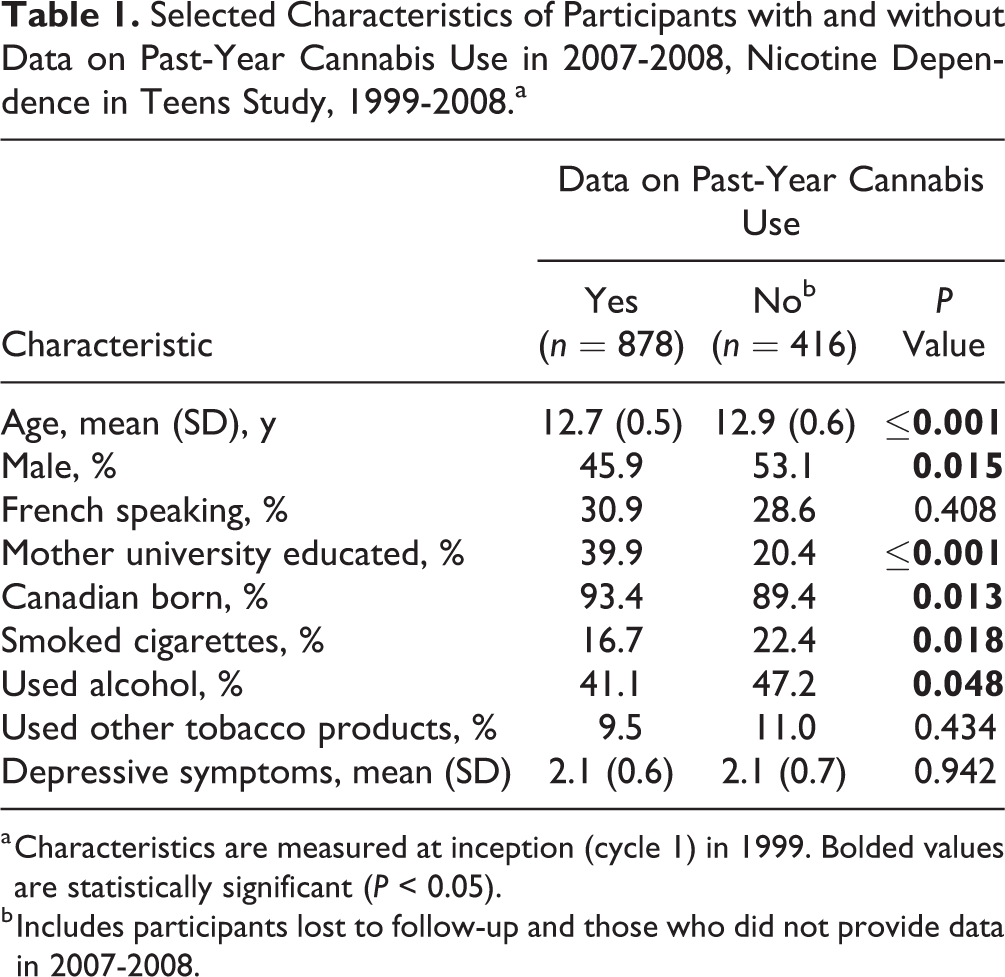
a Characteristics are measured at inception (cycle 1) in 1999. Bolded values are statistically significant (P < 0.05).
b Includes participants lost to follow-up and those who did not provide data in 2007-2008.
Of the 878 participants retained (68% of 1294 participants at inception), 387 (44%) reported past-year cannabis use, 25% had used cannabis but not in the past year, and 31% were never users. Among the 387 past-year users, 43% used cannabis frequently: 21% used cannabis weekly and 22% (10% of 878 participants with data at age 20) used cannabis daily (Appendix 3, available online). Daily cannabis users initiated cannabis use at a mean (SD) age of 14.5 (1.5) years on average compared to 15.4 (1.7), 15.9 (1.9), and 15.3 (1.8) (P ≤ 0.001) among ever users (but not in the past year), less than weekly users, and weekly users, respectively. Mean (SD) number of years using cannabis was 5.0 (1.8), 4.5 (2.0), 5.1 (1.7), and 6.3 (1.5) (P ≤ 0.001) among ever users (but not in the past year), less than weekly users, weekly users, and daily users, respectively.
Table 2 describes frequency of cannabis use according to potential risk factors. Among sociodemographic characteristics, a higher proportion of participants who used cannabis daily were male. Never users had the lowest proportion of university-educated mothers and of participants born in Canada. There were no differences across groups in age, language, or living with 1 parent.
Frequency of Past-Year Cannabis Use among Young Adults According to Potential Risk Factors, Nicotine Dependence in Teens Study, 1999-2008 (n = 878).a
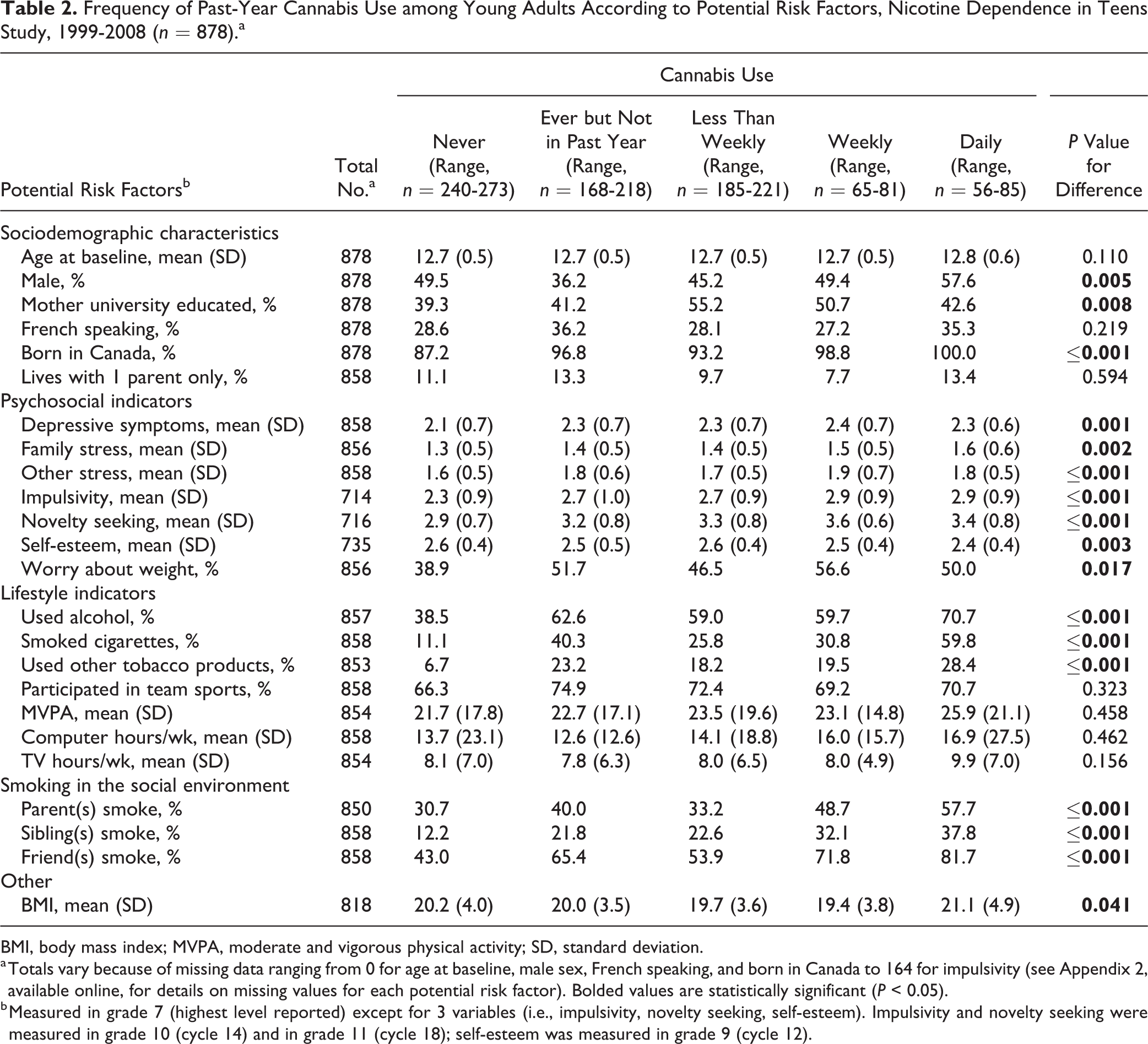
BMI, body mass index; MVPA, moderate and vigorous physical activity; SD, standard deviation.
a Totals vary because of missing data ranging from 0 for age at baseline, male sex, French speaking, and born in Canada to 164 for impulsivity (see Appendix 2, available online, for details on missing values for each potential risk factor). Bolded values are statistically significant (P < 0.05).
b Measured in grade 7 (highest level reported) except for 3 variables (i.e., impulsivity, novelty seeking, self-esteem). Impulsivity and novelty seeking were measured in grade 10 (cycle 14) and in grade 11 (cycle 18); self-esteem was measured in grade 9 (cycle 12).
There were differences across groups in all psychosocial indicators, with a general tendency of mean scores increasing (indicating more distress) from never users to daily users. Mean self-esteem scores declined from never users to daily users, and the proportion of participants who worried about their weight was lowest among never users.
There were no differences across groups for several lifestyle indicators, including team sport participation, MVPA, and computer and TV hours per week. However, the proportion of participants who used alcohol, smoked cigarettes, and used other tobacco products generally increased with increasing frequency of cannabis use. Similarly, smoking in the social environment increased with increasing frequency of cannabis use. BMI at baseline was highest among daily cannabis users.
The results of multivariable modeling were generally concordant with the unadjusted findings (Table 3). Older age, male sex, higher family stress, higher levels of other stress, higher impulsivity and novelty seeking, lower self-esteem, alcohol use, cigarette use, other tobacco use, parent(s) smoke, sibling(s) smoke, friend(s) smoke, and higher BMI were associated with daily cannabis use. None of the other characteristics (mother university educated, French speaking, lives with 1 parent only, depressive symptoms, worry about weight, team sports, MVPA, computer hours per week, or TV hours per week) were associated with daily cannabis use. Born in Canada was not included in Table 3 because all daily users were born in Canada, precluding multivariable analyses.
Odds Ratios and 95% Confidence Intervals for the Associations between Potential Risk Factors and Daily Cannabis Use at Age 20, Nicotine Dependence in Teens Study, 1999-2008 (n = 878).a
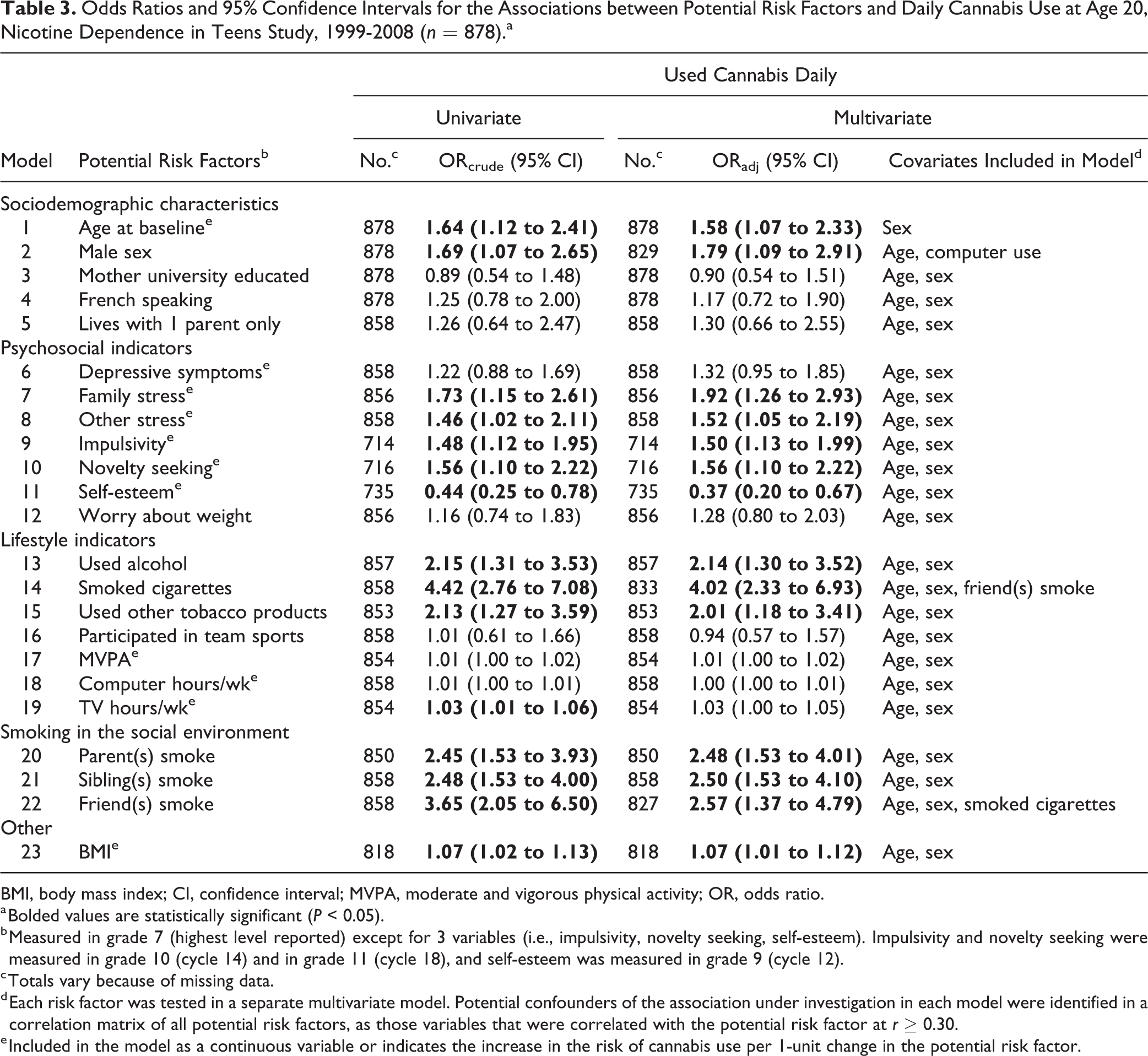
BMI, body mass index; CI, confidence interval; MVPA, moderate and vigorous physical activity; OR, odds ratio.
a Bolded values are statistically significant (P < 0.05).
b Measured in grade 7 (highest level reported) except for 3 variables (i.e., impulsivity, novelty seeking, self-esteem). Impulsivity and novelty seeking were measured in grade 10 (cycle 14) and in grade 11 (cycle 18), and self-esteem was measured in grade 9 (cycle 12).
c Totals vary because of missing data.
d Each risk factor was tested in a separate multivariate model. Potential confounders of the association under investigation in each model were identified in a correlation matrix of all potential risk factors, as those variables that were correlated with the potential risk factor at r ≥ 0.30.
e Included in the model as a continuous variable or indicates the increase in the risk of cannabis use per 1-unit change in the potential risk factor.
In sensitivity analyses, the risk factors for past-year weekly or daily cannabis use mirrored those for daily use with 5 exceptions: age, sex, and BMI were not statistically significant and depressive symptoms and worry about weight were statistically significant in adjusted models. Excluding 60 participants who initiated cannabis use prior to age 13 did not alter the findings.
Discussion
Canada’s Cannabis Act, slated for fall 2018, will legalize recreational use of cannabis in adults. Because of possible normalization and increased availability postlegalization, 1,3,50 perceived harmfulness of cannabis may decrease in youth, and onset 12,51,52 as well as frequency of use 4 could increase. 51
In this study, we identified early risk factors for daily cannabis use in young adults. The finding that those at risk can be identified as early as grade 7 represents an important prevention opportunity; it provides the basis for early screening, informs development of programs and policy, lays the groundwork for developing prognostic clinical tools, and permits optimally matching individuals with appropriate intervention depending on their risk profile. For example, children with family members who smoke cigarettes may require family-targeted intervention, while children with multiple risk factors may need individually tailored intervention that addresses the collective risk.
Consistent with previous reports, 25,53,54 males had a higher risk of daily cannabis use. Several reports suggest that gender differences in youth relate more to opportunity than gender vulnerability. 7,23 Swift et al., 53 however, concluded that opportunity alone could not explain the difference and hypothesized that male propensity for risk taking and stigma associated with female drug use could partially explain gender differences. Alternatively, it is possible that males have a greater need for (immediate) gratification or pleasure obtained by a cannabis high. Despite gender differences, prevention should target both sexes since females increase drug use faster than males, which could signify drug use disorders. 55
Psychological attributes 56 –58 and mental health challenges are both associated with substance use in youth. 24,59 In the NDIT study, high stress levels, impulsivity, novelty seeking, and lower self-esteem were associated with daily cannabis use. These findings may pertain to the self-medication hypothesis, which posits that people with mental health–related vulnerability use substances to alleviate symptoms. 60 Relief from depression and anxiety and the need for a quick euphoric effect are often reported as important motives for cannabis use. 61,62 However, results from longitudinal studies supporting the self-medication theory have been mixed, possibly because the reinforcement pattern associated with the self-medication hypothesis may be short term and not observable in longitudinal studies with data collection time points that are distant. 63 –65 Alternative explanations include common genetic factors such as polymorphisms in the dopamine D2 receptor, which is associated with a lower sensitivity to everyday rewards and can potentially lead individuals to higher levels of sensation seeking in substance use. 63 In addition, adolescents may lack knowledge on coping mechanisms to confront life challenges and therefore turn to seemingly “easy,” available solutions. Depending on symptom severity, education on healthy coping mechanisms, counseling, or treatment may be needed.
Cigarette smoking by parent(s), sibling(s), and friend(s) was associated with daily cannabis use in the NDIT study. Both access to substances and perceptions of peer substance use predict initiation of tobacco 45 and cannabis use. 23,27,66 Continued monitoring of cannabis use among youth (and their parents) in legalized contexts will be important, because cannabis use in the social and home environment will likely increase and could affect age at cannabis onset and daily use. 52
Concordant with other reports, 22,27,53,67,68 early use of alcohol, tobacco, and other tobacco products was associated with daily cannabis use in the NDIT study. Co-occurrence of multiple substances early in life may signal higher risk because of common genetic or psychosocial vulnerability, greater access or higher exposure to substances, or elevated risks of dependence.
In the NDIT study, higher BMI was associated with daily cannabis use. Although Hayatbakhsh et al. 26 did not detect a longitudinal association, there was an inverse dose-response association between BMI and cannabis use at age 21 cross-sectionally. It is possible that cannabis use and BMI share a common underpinning. Youth with high impulsivity who have not learned self-regulation behaviours, 69 for example, or with higher sensitivity to the reward system may overeat, have higher BMI, 70,71 and also engage in substance use. 72,73 Alternatively, adolescents with overweight or obesity may use substances to cope with negative emotional or social consequences of their weight. Substance use risk may increase through cigarette smoking as a weight control strategy. 74,75 Finally, higher BMI in the NDIT study may relate to early puberty. Adolescents who mature at younger ages may be exposed to substances earlier if they engage with older peers. They may use substances to cope with low self-esteem or higher stress related to earlier puberty, or they may experience weaker parental relationships, which lead to deviant behaviour. 58,76,77
Limitations of this analysis include that self-report data are subject to misclassification. Our cannabis use measure did not incorporate quantity, potency, or method of ingestion, nor were cannabis dependence or use of medicinal cannabis measured. Selection bias related to loss to follow-up may have affected the estimates, and use of a purposive sample could limit generalizability. Past-year cannabis use was reported by 44% of NDIT participants, compared to 33% of Canadians age 20 to 24 years in 2012. 2 However, the higher prevalence in the NDIT study could relate to secular trends, and cannabis use may be underreported in surveillance interviews because of fear of reprisal. 2 Furthermore, the 22% of past-year daily users in the NDIT study is similar to the 18% reported in 2 national surveys, 78,79 and the mean age at cannabis onset in the NDIT study (15.1 years) was similar to that in Canada (i.e., 15.0), 1 suggestive that selection bias and external generalizability may not be important issues.
Conclusions
The risk of daily cannabis use in young adults can be identified as early as grade 7. Parents, teachers, and health care providers may need to monitor at-risk children to ascertain whether they might benefit from intervention to prevent daily cannabis use. Risk profiles may help design tailored preventive intervention for individuals.
Data Access
Data are available on request. To gain access, applicants must complete a data request form available on the NDIT website (www.nditstudy.ca) and return it to the principal investigator (
The procedure to obtain access to NDIT data is described in O’Loughlin et al. 31 The relevant paragraph is described below. This process has been approved by the ethics committee at the CRCHUM.
Access to NDIT data is open to any university-appointed or affiliated investigator upon successful completion of the application process. Masters, doctoral, and postdoctoral students may apply through their primary supervisor. For more information, visit www.nditstudy.ca or contact the principal investigator.
Supplemental Material
Supplemental Material, DS_10.1177_0706743718804541 - Early Risk Factors for Daily Cannabis Use in Young Adults
Supplemental Material, DS_10.1177_0706743718804541 for Early Risk Factors for Daily Cannabis Use in Young Adults by Erika Nicole Dugas, Marie-Pierre Sylvestre, Esthelle Ewusi-Boisvert, Michael Chaiton, Annie Montreuil and Jennifer O’Loughlin in The Canadian Journal of Psychiatry
Footnotes
Acknowledgements
Jennifer O’Loughlin holds a Canada Research Chair in the Early Determinants of Adult Chronic Disease. Marie-Pierre Sylvestre was supported by a Chercheurs-Boursier career award from the Fonds de Recherche du Québec–Santé (FRQS). The authors thank the NDIT study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Cancer Society (grant numbers 010271, 017435). The funders were not involved in the design or conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.